
Measuring Neighborhood Landscapes: Associations between a Neighborhood’s Landscape Characteristics and Colon Cancer Survival

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Residential Histories
2.3. Socio-Economic Variables
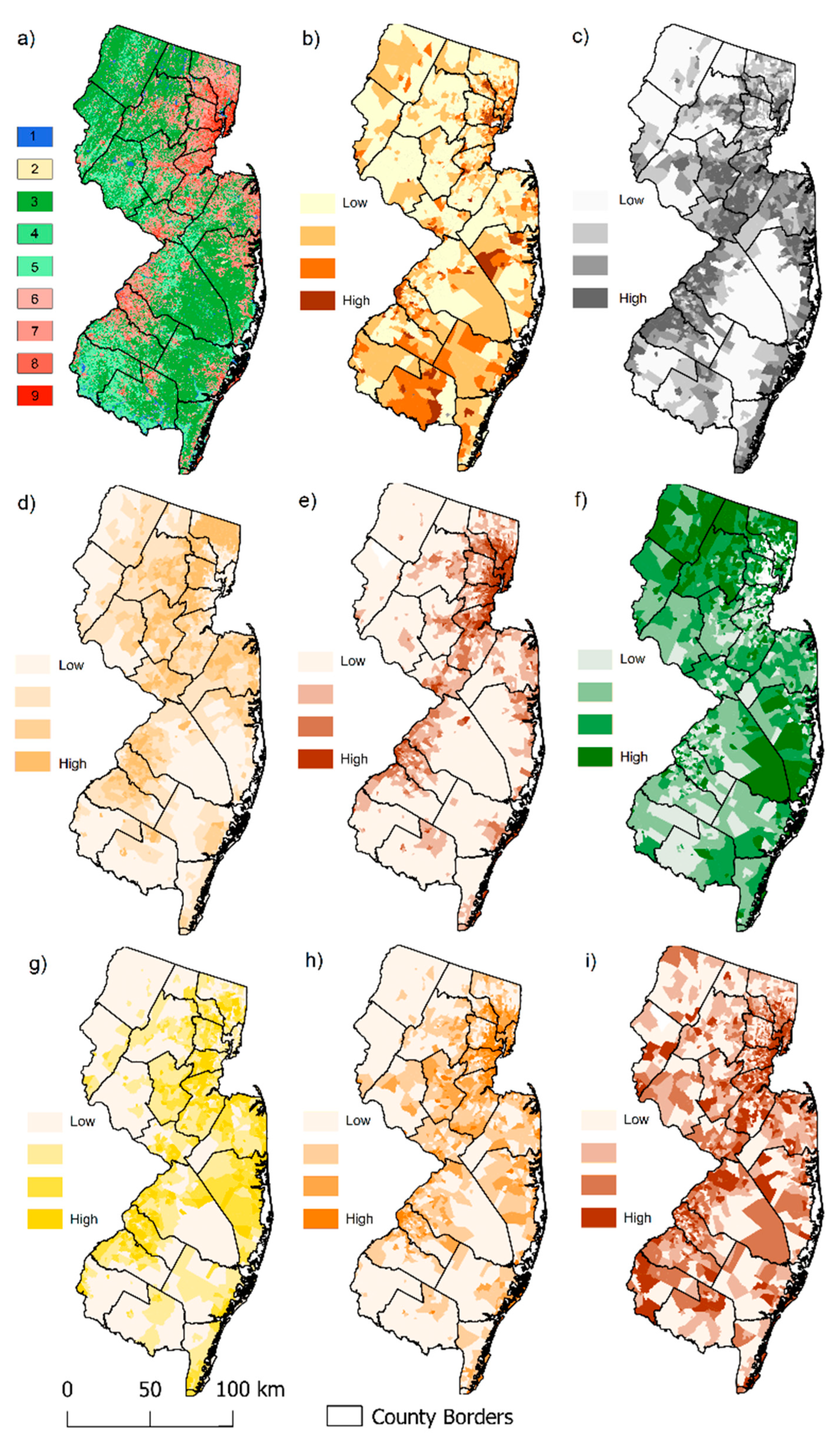
2.4. Environmental Variables
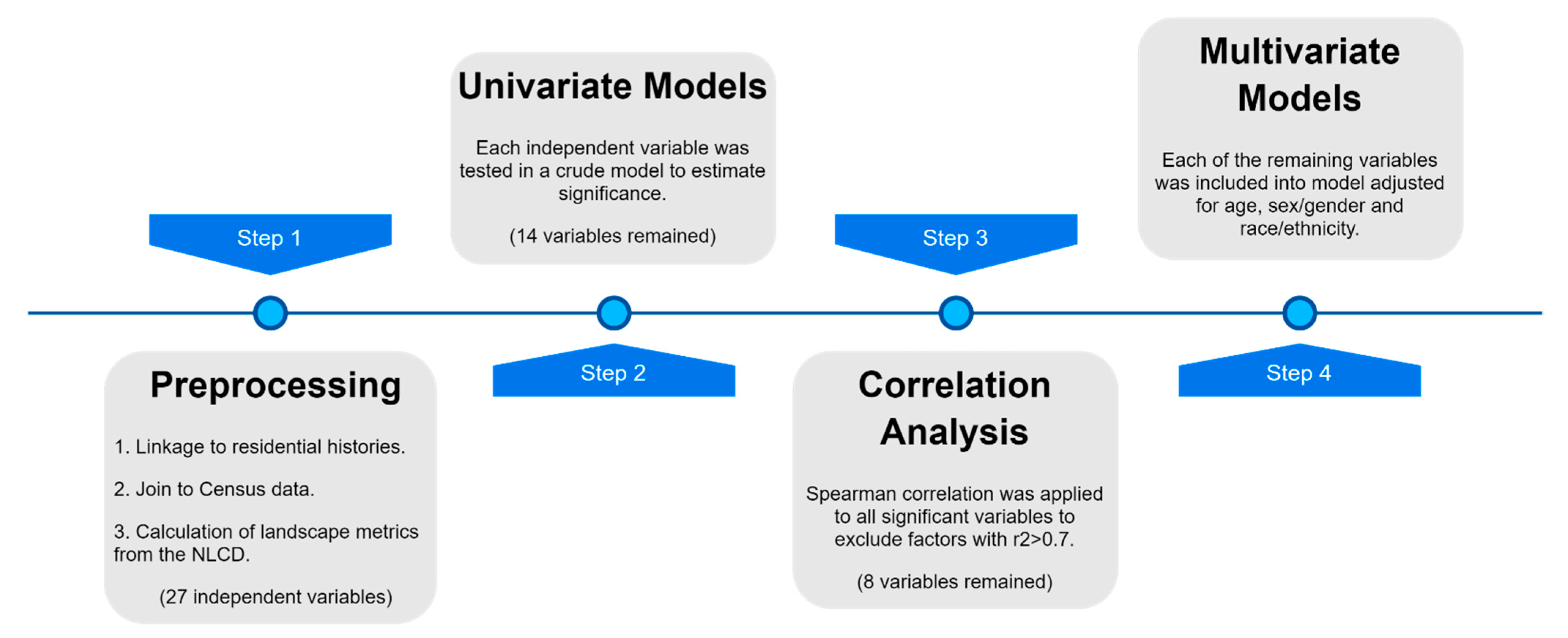
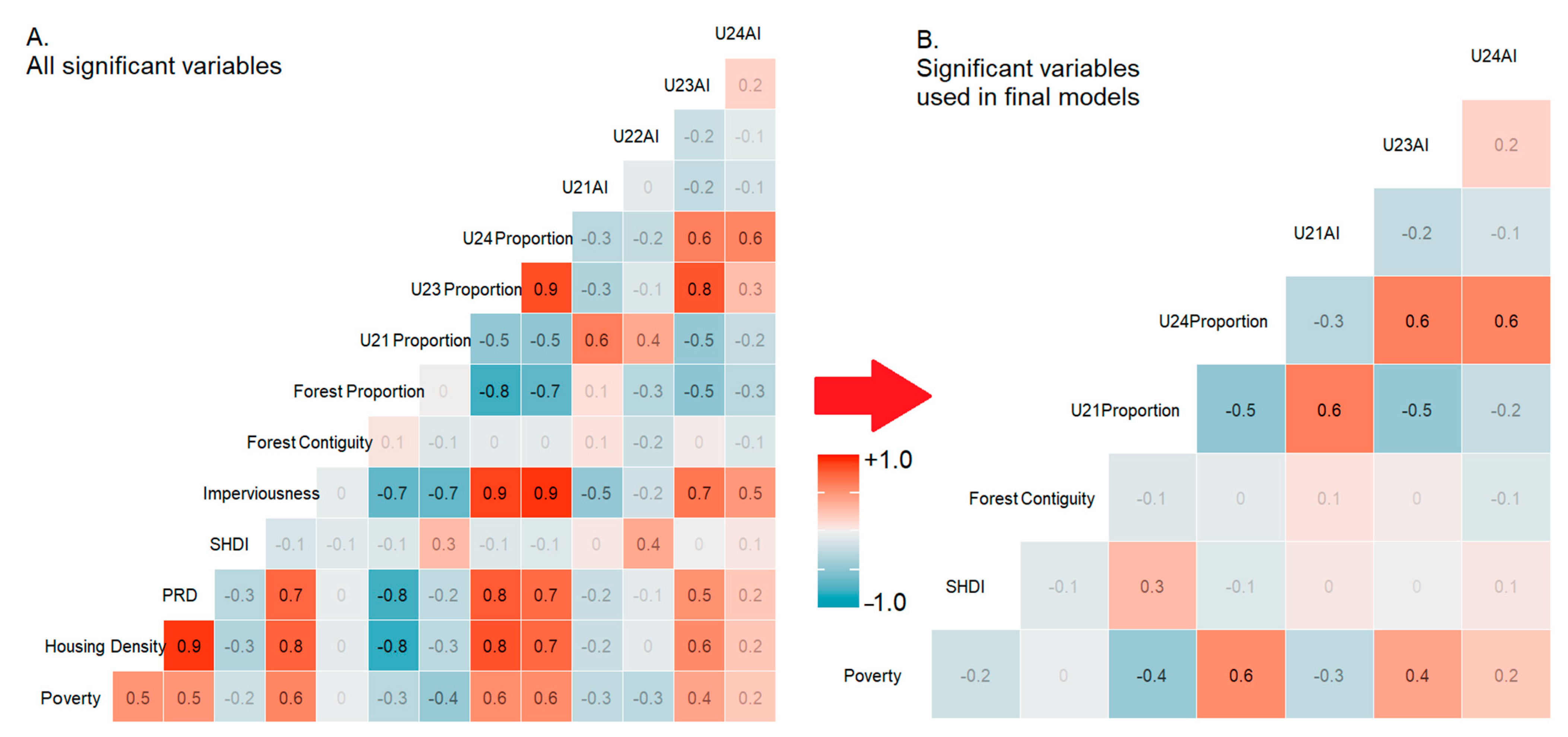
2.5. Statistical Analysis
3. Results
3.1. Study Population
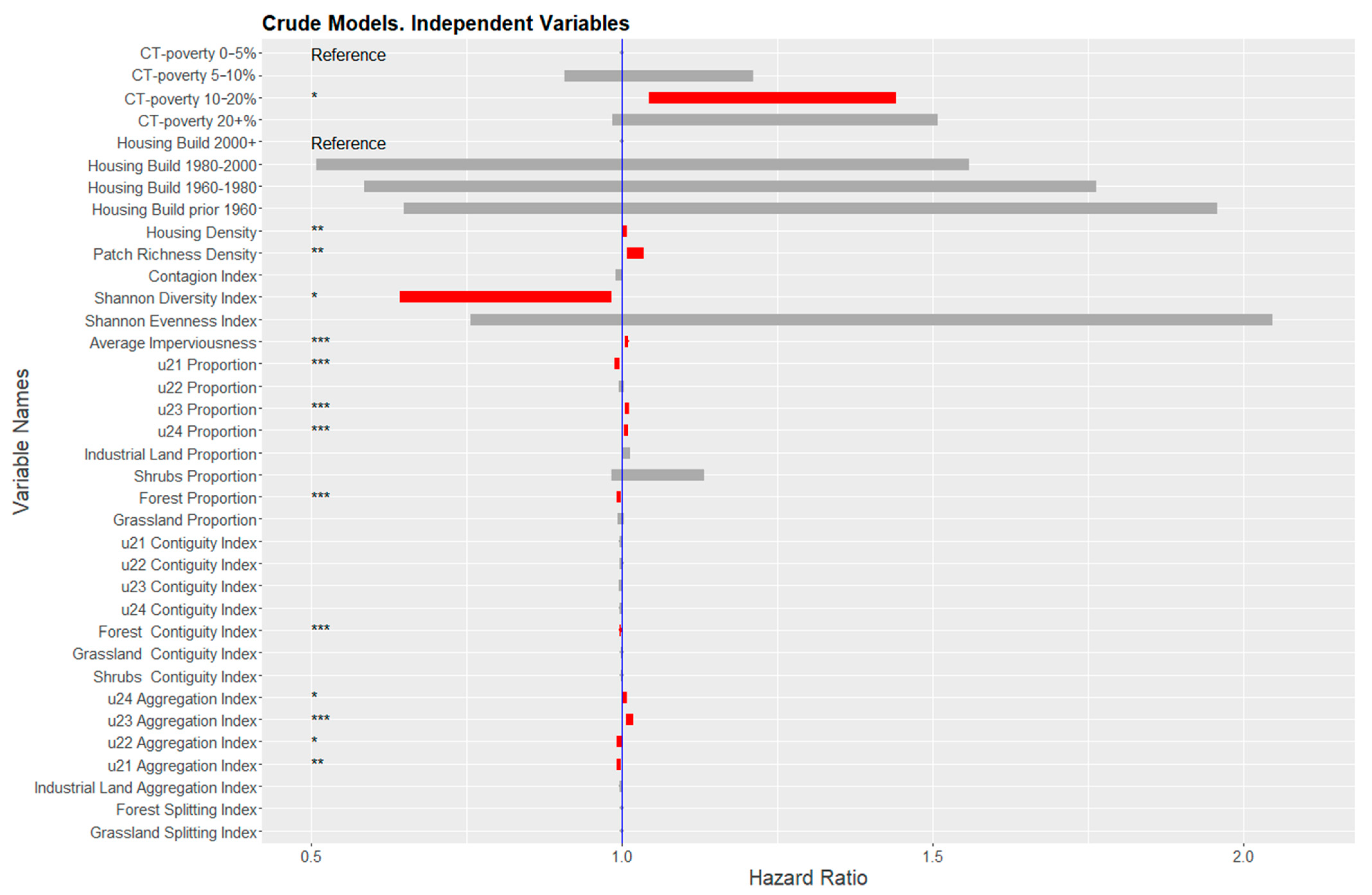
3.2. Univariate Models
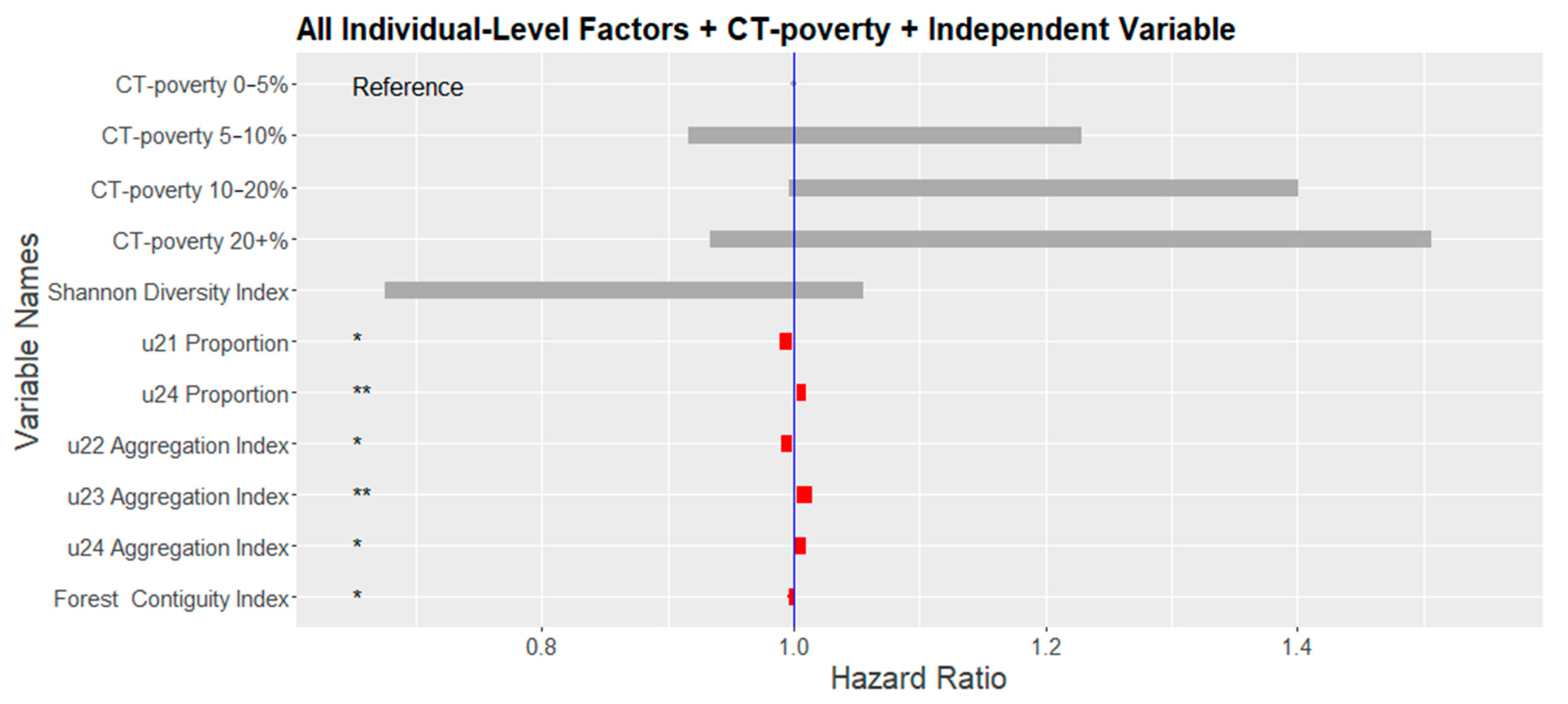
3.3. Multivariate Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diez Roux, A.V. Investigating neighborhood and area effects on health. Am. J. Public Health 2001, 91, 1783–1789. [Google Scholar] [CrossRef]
- Northridge, M.E.; Sclar, E.D.; Biswas, P. Sorting out the connections between the built environment and health: A conceptual framework for navigating pathways and planning healthy cities. J. Urban Health 2003, 80, 556–568. [Google Scholar] [CrossRef]
- Link, B.G.; Phelan, J. Social Conditions As Fundamental Causes of Disease. J. Health Soc. Behav. 1995, 80–94. [Google Scholar] [CrossRef]
- Rapoport, A. The Mutual Interaction of People and Their Built Environment; De Gruyter Mouton: Berlin, Germany, 2011. [Google Scholar]
- Renalds, A.; Smith, T.H.; Hale, P.J. A systematic review of built environment and health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef]
- Gesler, W.M. Therapeutic landscapes: Medical issues in light of the new cultural geography. Soc. Sci. Med. 1992, 34, 735–746. [Google Scholar] [CrossRef]
- Matsuoka, R.; Sullivan, W. Human Psychological Community Health. In The Routledge Handbook of Urban Ecology; Douglas, I., Goode, D., Houck, M.C., Maddox, D., Eds.; Taylor & Francis Group: London, UK, 2011. [Google Scholar]
- Dramstad, W.E.; Tveit, M.S.; Fjellstad, W.; Fry, G.L. Relationships between visual landscape preferences and map-based indicators of landscape structure. Landsc. Urban Plan. 2006, 78, 465–474. [Google Scholar] [CrossRef]
- Palmer, J.F. Using spatial metrics to predict scenic perception in a changing landscape: Dennis, Massachusetts. Landsc. Urban Plan. 2004, 69, 201–218. [Google Scholar] [CrossRef]
- Staats, H.; Kieviet, A.; Hartig, T. Where to recover from attentional fatigue: An expectancy-value analysis of environmental preference. J. Environ. Psychol. 2003, 23, 147–157. [Google Scholar] [CrossRef]
- van den Berg, A.E.; Koole, S.L.; van der Wulp, N.Y. Environmental preference and restoration: (How) are they related? J. Environ. Psychol. 2003, 23, 135–146. [Google Scholar] [CrossRef]
- Lee, S.-W.; Ellis, C.D.; Kweon, B.-S.; Hong, S.-K. Relationship between landscape structure and neighborhood satisfaction in urbanized areas. Landsc. Urban Plan. 2008, 85, 60–70. [Google Scholar] [CrossRef]
- Kaplan, S. Aesthetics, Affect, and Cognition:Environmental Preference from an Evolutionary Perspective. Environ. Behav. 1987, 19, 3–32. [Google Scholar] [CrossRef]
- Ittelson, W.H. Environmental Perception and Urban Experience. Environ. Behav. 1978, 10, 193–213. [Google Scholar] [CrossRef]
- Zube, E.H.; Sell, J.L.; Taylor, J.G. Landscape perception: Research, application and theory. Landsc. Plan. 1982, 9, 1–33. [Google Scholar] [CrossRef]
- Iverson Nassauer, J. Culture and changing landscape structure. Landsc. Ecol. 1995, 10, 229–237. [Google Scholar] [CrossRef]
- Jackson, L.E. The relationship of urban design to human health and condition. Landsc. Urban Plan. 2003, 64, 191–200. [Google Scholar] [CrossRef]
- Singh, G.K. Area Deprivation and Widening Inequalities in US Mortality, 1969–1998. Am. J. Public Health 2003, 93, 1137–1143. [Google Scholar] [CrossRef]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 19. [Google Scholar] [CrossRef]
- Singh, G.K.; Williams, S.D.; Siahpush, M.; Mulhollen, A. Socioeconomic, Rural-Urban, and Racial Inequalities in US Cancer Mortality: Part I-All Cancers and Lung Cancer and Part II-Colorectal, Prostate, Breast, and Cervical Cancers. J. Cancer Epidemiol. 2011, 2011, 107497. [Google Scholar] [CrossRef]
- Henry, K.A.; Niu, X.; Boscoe, F.P. Geographic disparities in colorectal cancer survival. Int. J. Health Geogr. 2009, 8, 48. [Google Scholar] [CrossRef]
- Henry, K.A.; Sherman, R.L.; McDonald, K.; Johnson, C.J.; Lin, G.; Stroup, A.M.; Boscoe, F.P. Associations of census-tract poverty with subsite-specific colorectal cancer incidence rates and stage of disease at diagnosis in the United States. J. Cancer Epidemiol. 2014, 2014, 823484. [Google Scholar] [CrossRef] [PubMed]
- Lian, M.; Schootman, M.; Doubeni, C.A.; Park, Y.; Major, J.M.; Stone, R.A.; Laiyemo, A.O.; Hollenbeck, A.R.; Graubard, B.I.; Schatzkin, A. Geographic variation in colorectal cancer survival and the role of small-area socioeconomic deprivation: A multilevel survival analysis of the NIH-AARP Diet and Health Study Cohort. Am. J. Epidemiol. 2011, 174, 828–838. [Google Scholar] [CrossRef] [PubMed]
- Wiese, D.; Stroup, A.M.; Maiti, A.; Harris, G.; Lynch, S.M.; Vucetic, S.; Henry, K.A. Socioeconomic Disparities in Colon Cancer Survival: Revisiting Neighborhood Poverty using Residential Histories. Epidemiology 2020, 31, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Wiese, D.; Stroup, A.M.; Maiti, A.; Harris, G.; Lynch, S.M.; Vucetic, S.; Henry, K.A. Residential mobility and geospatial disparities in colon cancer survival. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2119–2125. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Pawlish, K.S.; Roche, L.M. Cancer survival disparities by race/ethnicity and socioeconomic status in New Jersey. J. Health Care Poor Underserved 2010, 21, 144–160. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Quesenberry, C.; Peng, T.; Horn-Ross, P.; Stewart, S.; Brown, S.; Swallen, K.; Guillermo, T.; Suh, D.; Alvarez-Martinez, L. Social class, race/ethnicity, and incidence of breast, cervix, colon, lung, and prostate cancer among Asian, Black, Hispanic, and White residents of the San Francisco Bay Area, 1988–1992 (United States). Cancer Cause Control 1999, 10, 525–537. [Google Scholar] [CrossRef]
- Wang, L.; Wilson, S.E.; Stewart, D.B.; Hollenbeak, C.S. Marital status and colon cancer outcomes in US Surveillance, Epidemiology and End Results registries: Does marriage affect cancer survival by gender and stage? Cancer Epidemiol. 2011, 35, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-C.; Cheng, L.-C.; Lin, Y.-W.; Wang, S.-C.; Ke, T.-M.; Huang, C.-I.; Su, Y.-C.; Tai, M.-H. The impact of marital status on survival in patients with surgically treated colon cancer. Medicine 2019, 98, e14856. [Google Scholar] [CrossRef]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to greenness and mortality in a nationwide prospective cohort study of women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Richardson, E.; Pearce, J.; Mitchell, R.; Day, P.; Kingham, S. The association between green space and cause-specific mortality in urban New Zealand: An ecological analysis of green space utility. BMC Public Health 2010, 10, 240. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R. Gender differences in relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R.; Hartig, T.; De Vries, S.; Astell-Burt, T.; Frumkin, H. Green cities and health: A question of scale? J. Epidemiol. Community Health 2012, 66, 160–165. [Google Scholar] [CrossRef]
- Keegan, T.H.M.; Shariff-Marco, S.; Sangaramoorthy, M.; Koo, J.; Hertz, A.; Schupp, C.W.; Yang, J.; John, E.M.; Gomez, S.L. Neighborhood influences on recreational physical activity and survival after breast cancer. Cancer Cause Control 2014, 25, 1295–1308. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P.; Jorgensen, A.; Maheswaran, R. Population-level linkages between urban greenspace and health inequality: The case for using multiple indicators of neighbourhood greenspace. Health Place 2020, 62, 102284. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; De Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T. Nature and mental health: An ecosystem service perspective. Sci. Adv. 2019, 5, eaax0903. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [PubMed]
- Mears, M.; Brindley, P.; Jorgensen, A.; Ersoy, E.; Maheswaran, R. Greenspace spatial characteristics and human health in an urban environment: An epidemiological study using landscape metrics in Sheffield, UK. Ecol. Indic. 2019, 106, 105464. [Google Scholar] [CrossRef]
- Sugiyama, T.; Carver, A.; Koohsari, M.J.; Veitch, J. Advantages of public green spaces in enhancing population health. Landsc. Urban Plan. 2018, 178, 12–17. [Google Scholar] [CrossRef]
- Van Dillen, S.M.; de Vries, S.; Groenewegen, P.P.; Spreeuwenberg, P. Greenspace in urban neighbourhoods and residents’ health: Adding quality to quantity. J. Epidemiol. Community Health 2012, 66, e8. [Google Scholar] [CrossRef]
- Mears, M.; Brindley, P. Measuring urban greenspace distribution equity: The importance of appropriate methodological approaches. ISPRS Int. J. Geo-Inf. 2019, 8, 286. [Google Scholar] [CrossRef]
- Hunter, M.C.R.; Brown, D.G. Spatial contagion: Gardening along the street in residential neighborhoods. Landsc. Urban Plan. 2012, 105, 407–416. [Google Scholar] [CrossRef]
- Gomez, S.L.; Shariff-Marco, S.; DeRouen, M.; Keegan, T.H.M.; Yen, I.H.; Mujahid, M.; Satariano, W.A.; Glaser, S.L. The impact of neighborhood social and built environment factors across the cancer continuum: Current research, methodological considerations, and future directions. Cancer 2015, 121, 2314–2330. [Google Scholar] [CrossRef] [PubMed]
- Demoury, C.; Thierry, B.; Richard, H.; Sigler, B.; Kestens, Y.; Parent, M.-E. Residential greenness and risk of prostate cancer: A case-control study in Montreal, Canada. Environ. Int. 2017, 98, 129–136. [Google Scholar] [CrossRef]
- Ashing-Giwa, K.T.; Lim, J.-W.; Tang, J. Surviving cervical cancer: Does health-related quality of life influence survival? Gynecol. Oncol. 2010, 118, 35–42. [Google Scholar] [CrossRef]
- Cunningham, R.; Sarfati, D.; Stanley, J.; Peterson, D.; Collings, S. Cancer survival in the context of mental illness: A national cohort study. Gen. Hosp. Psychiatry 2015, 37, 501–506. [Google Scholar] [CrossRef]
- McCormack, G.R.; Cabaj, J.; Orpana, H.; Lukic, R.; Blackstaffe, A.; Goopy, S.; Hagel, B.; Keough, N.; Martinson, R.; Chapman, J. Evidence synthesis A scoping review on the relations between urban form and health: A focus on Canadian quantitative evidence. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2019, 39, 187. [Google Scholar] [CrossRef]
- Plascak, J.J.; Rundle, A.G.; Babel, R.A.; Llanos, A.A.; LaBelle, C.M.; Stroup, A.M.; Mooney, S.J. Drop-and-spin virtual neighborhood auditing: Assessing built environment for linkage to health studies. Am. J. Prev. Med. 2020, 58, 152–160. [Google Scholar] [CrossRef]
- Rzotkiewicz, A.; Pearson, A.L.; Dougherty, B.V.; Shortridge, A.; Wilson, N. Systematic review of the use of Google Street View in health research: Major themes, strengths, weaknesses and possibilities for future research. Health Place 2018, 52, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Maharana, A.; Nsoesie, E.O. Use of Deep Learning to Examine the Association of the Built Environment With Prevalence of Neighborhood Adult ObesityDeep Learning to Examine the Built Environment and Neighborhood Adult Obesity PrevalenceDeep Learning to Examine the Built Environment and Neighborhood Adult Obesity Prevalence. JAMA Netw. Open 2018, 1, e181535. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe-Nelson, C.; Kelly, S.; Kennedy, M.; Cherrie, J.W. A scoping review mapping research on green space and associated mental health benefits. Int. J. Environ. Res. Public Health 2019, 16, 2081. [Google Scholar] [CrossRef]
- Turner, M.G.; Gardner, R.H.; O’neill, R.V.; O’Neill, R.V. Landscape Ecology in Theory and Practice; Springer: Berlin/Heidelberg, Germany, 2001; Volume 401. [Google Scholar]
- Uuemaa, E.; Antrop, M.; Roosaare, J.; Marja, R.; Mander, Ü. Landscape metrics and indices: An overview of their use in landscape research. Living Rev. Landsc. Res. 2009, 3, 1–28. [Google Scholar] [CrossRef]
- Uuemaa, E.; Mander, Ü.; Marja, R. Trends in the use of landscape spatial metrics as landscape indicators: A review. Ecol. Indic. 2013, 28, 100–106. [Google Scholar] [CrossRef]
- NJSCR. NJ State Cancer Registry. Available online: https://www.state.nj.us/health/ces/reporting-entities/njscr/ (accessed on 28 April 2021).
- Percy, C.; Holten, V.V.; Muir, C.S. International Classification of Diseases for Oncology; World Health Organization: Geneva, Switzerland, 1990. [Google Scholar]
- Hurley, S.; Hertz, A.; Nelson, D.O.; Layefsky, M.; Von Behren, J.; Bernstein, L.; Deapen, D.; Reynolds, P. Tracing a path to the past: Exploring the use of commercial credit reporting data to construct residential histories for epidemiologic studies of environmental exposures. Am. J. Epidemiol. 2017, 185, 238–246. [Google Scholar] [CrossRef]
- Wheeler, D.C.; Wang, A. Assessment of Residential History Generation Using a Public-Record Database. Int. J. Environ. Res. Public Health 2015, 12, 11670–11682. [Google Scholar] [CrossRef]
- Jacquez, G.M.; Slotnick, M.J.; Meliker, J.R.; AvRuskin, G.; Copeland, G.; Nriagu, J. Accuracy of commercially available residential histories for epidemiologic studies. Am. J. Epidemiol. 2010, 173, 236–243. [Google Scholar] [CrossRef]
- Stinchcomb, D.; Roeser, A. NCI/SEER Residential History Project Technical Report; Westat, Inc.: Rockville, MD, USA, 2016. [Google Scholar]
- Texas A &M University. NAACCR Geocoder Data Dictionary; NAACCR: Springfield, IL, USA, 2016; Available online: http://www.naaccr.org/wp-content/uploads/2016/11/NAACCR-Geocoder-Data-Dictionary.pdf (accessed on 28 April 2021).
- Homer, C.H.; Fry, J.A.; Barnes, C.A. The national land cover database. US Geol. Surv. Fact Sheet 2012, 3020, 1–4. [Google Scholar]
- Hijmans, R.J.; van Etten, J.; Cheng, M.; Mattiuzzi, M.; Sumner, J.A.; Greenberg, O.P.; Lamigueiro, A.; Bevan, E.B. Racine, and A. Shortridge. Package ‘Raster’; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Akpinar, A.; Barbosa-Leiker, C.; Brooks, K.R. Does green space matter? Exploring relationships between green space type and health indicators. Urban For. Urban Green. 2016, 20, 407–418. [Google Scholar] [CrossRef]
- Wu, J.; Jackson, L. Inverse relationship between urban green space and childhood autism in California elementary school districts. Environ. Int. 2017, 107, 140–146. [Google Scholar] [CrossRef]
- Callaghan, C.T.; Bino, G.; Major, R.E.; Martin, J.M.; Lyons, M.B.; Kingsford, R.T. Heterogeneous urban green areas are bird diversity hotspots: Insights using continental-scale citizen science data. Landsc. Ecol. 2019, 34, 1231–1246. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Hesselbarth, M.H.; Sciaini, M.; With, K.A.; Wiegand, K.; Nowosad, J. Landscapemetrics: An open-source R tool to calculate landscape metrics. Ecography 2019, 42, 1648–1657. [Google Scholar] [CrossRef]
- Van Der Wal, J.; Falconi, L.; Januchowski, S.; Shoo, L.; Storlie, C.; Van Der Wal, M.J. Package ‘SDMTools’; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Riitters, K.H.; O’neill, R.; Hunsaker, C.; Wickham, J.D.; Yankee, D.; Timmins, S.; Jones, K.; Jackson, B. A factor analysis of landscape pattern and structure metrics. Landsc. Ecol. 1995, 10, 23–39. [Google Scholar] [CrossRef]
- Li, H.; Reynolds, J. On definition and quantification of heterogeneity. Oikos 1995, 73, 280–284. [Google Scholar] [CrossRef]
- Li, H.; Reynolds, J.F. A simulation experiment to quantify spatial heterogeneity in categorical maps. Ecology 1994, 75, 2446–2455. [Google Scholar] [CrossRef]
- Tsai, W.-L.; McHale, M.R.; Jennings, V.; Marquet, O.; Hipp, J.A.; Leung, Y.-F.; Floyd, M.F. Relationships between characteristics of urban green land cover and mental health in US metropolitan areas. Int. J. Environ. Res. Public Health 2018, 15, 340. [Google Scholar] [CrossRef]
- Greenfield, E.J.; Nowak, D.J.; Walton, J.T. Assessment of 2001 NLCD percent tree and impervious cover estimates. Photogramm. Eng. Remote Sens. 2009, 75, 1279–1286. [Google Scholar] [CrossRef]
- Nowak, D.J.; Greenfield, E.J. Evaluating the National Land Cover Database tree canopy and impervious cover estimates across the conterminous United States: A comparison with photo-interpreted estimates. Environ. Manag. 2010, 46, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Howden-Chapman, P. Housing standards: A glossary of housing and health. J. Epidemiol. Community Health 2004, 58, 162–168. [Google Scholar] [CrossRef]
- Shaw, M. Housing and public health. Annu. Rev. Public Health 2004, 25, 397–418. [Google Scholar] [CrossRef] [PubMed]
- Rauh, V.A.; Landrigan, P.J.; Claudio, L. Housing and health: Intersection of poverty and environmental exposures. Ann. N. Y. Acad. Sci. 2008, 1136, 276–288. [Google Scholar] [CrossRef] [PubMed]
- Lynch, S.M.; Mitra, N.; Ross, M.; Newcomb, C.; Dailey, K.; Jackson, T.; Zeigler-Johnson, C.M.; Riethman, H.; Branas, C.C.; Rebbeck, T.R. A Neighborhood-Wide Association Study (NWAS): Example of prostate cancer aggressiveness. PLoS ONE 2017, 12, e0174548. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Reinikainen, J.; Adeleke, K.A.; Pieterse, M.E.; Groothuis-Oudshoorn, C.G.M. Time-varying covariates and coefficients in Cox regression models. Ann. Transl. Med. 2018, 6, 121. [Google Scholar] [CrossRef]
- Mills, M. Introducing Survival and Event History Analysis; SAGE: London, UK, 2010. [Google Scholar]
- Zwiener, I.; Blettner, M.; Hommel, G. Survival analysis: Part 15 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2011, 108, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Therneau, T.M.; Lumley, T. Package ‘survival’. R Top. Doc. 2015, 128, 112. [Google Scholar]
- Rappaport, J. Moving to nice weather. Reg. Sci. Urban Econ. 2007, 37, 375–398. [Google Scholar] [CrossRef]
- Banzhaf, H.S.; Walsh, R.P. Do people vote with their feet? An empirical test of Tiebout. Am. Econ. Rev. 2008, 98, 843–863. [Google Scholar] [CrossRef]
- Litwak, E.; Longino, C.F., Jr. Migration patterns among the elderly: A developmental perspective. Gerontol. 1987, 27, 266–272. [Google Scholar] [CrossRef]
- Iyer, H.S.; Valeri, L.; James, P.; Chen, J.T.; Hart, J.E.; Laden, F.; Holmes, M.D.; Rebbeck, T.R. The contribution of residential greenness to mortality among men with prostate cancer: A registry-based cohort study of Black and White men. Environ. Epidemiol. 2020, 4, e087. [Google Scholar] [CrossRef]
- O’Callaghan-Gordo, C.; Pollan, M.; Molina de la Torre, A.J.; Dierssen-Sotos, T.; Ardanaz, E.; Fernández-Tardón, G.; Amiano, P.; Capelo, R.; Chirlaque, M.-D.; Nieuwenhuijsen, M. Green Spaces and Colon Cancer Risk: A Case-Control in Spain. In Proceedings of the ISEE Conference Abstracts, Ottawa, ON, Canada, 26–30 August 2018. [Google Scholar]
- Schmitz, K.H.; Stout, N.L.; Maitin-Shepard, M.; Campbell, A.; Schwartz, A.L.; Grimmett, C.; Meyerhardt, J.A.; Sokolof, J.M. Moving through cancer: Setting the agenda to make exercise standard in oncology practice. Cancer 2021, 127, 476–484. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Winters-Stone, K.; Lee, A.; Schmitz, K.H. Cancer, physical activity, and exercise. Compr. Physiol. 2012, 2, 2775–2809. [Google Scholar] [CrossRef]
- Van Blarigan, E.L.; Meyerhardt, J.A. Role of physical activity and diet after colorectal cancer diagnosis. J. Clin. Oncol. 2015, 33, 1825–1834. [Google Scholar] [CrossRef]
- Garvin, E.; Branas, C.; Keddem, S.; Sellman, J.; Cannuscio, C. More Than Just An Eyesore: Local Insights And Solutions on Vacant Land And Urban Health. J. Urban Health 2013, 90, 412–426. [Google Scholar] [CrossRef]
- Chen, Y.; Stephens, M.; Jones, C.A. Does residents’ satisfaction with the neighbourhood environment relate to residents’ self-rated health? Evidence from Beijing. Int. J. Environ. Res. Public Health 2019, 16, 5051. [Google Scholar] [CrossRef]
- Zuniga, T.; Adriana, A. From Neighborhoods to Wellbeing and Conservation: Enhancing the Use of Greenspace through Walkability; The University of Arizona: Tucson, AZ, USA, 2015. [Google Scholar]
- Jennings, V.; Baptiste, A.K.; Jelks, O.; Skeete, R. Urban green space and the pursuit of health equity in parts of the United States. Int. J. Environ. Res. Public Health 2017, 14, 1432. [Google Scholar] [CrossRef]
- Soderstrom, M. The Walkable City: From Haussmann’s Boulevards to Jane Jacobs’ Streets and Beyond; Vehicule Press: Montreal, QC, Canada, 2008. [Google Scholar]
- Doubeni, C.A.; Major, J.M.; Laiyemo, A.O.; Schootman, M.; Zauber, A.G.; Hollenbeck, A.R.; Sinha, R.; Allison, J. Contribution of Behavioral Risk Factors and Obesity to Socioeconomic Differences in Colorectal Cancer Incidence. JNCI J. Natl. Cancer Inst. 2012, 104, 1353–1362. [Google Scholar] [CrossRef]
- Wen, M.; Zhang, X.; Harris, C.D.; Holt, J.B.; Croft, J.B. Spatial Disparities in the Distribution of Parks and Green Spaces in the USA. Ann. Behav. Med. 2013, 45, S18–S27. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The NLCD Code | Reclassification | Commentary |
|---|---|---|
| 21: Developed Open Space | U21: Developed Open Space | Max 20% imperviousness per cell/pixel |
| 22: Developed Low Intensity | U22: Developed Low Intensity | 20–49% imperviousness per cell/pixel |
| 23: Developed Medium Intensity | U23: Developed Medium Intensity | 50–79% imperviousness per cell/pixel |
| 24: Developed High Intensity | U24: Developed High Intensity | 80–100% imperviousness per cell/pixel |
| 41: Deciduous Forest | Forest | Dominated by tree canopy and includes any type of parks and squares |
| 42: Evergreen Forest | ||
| 43: Mixed Forest | ||
| 52: Shrub/Scrub | Shrubs | Dominated by shrubs; present on empty housing parcels |
| 71: Grasslands/Herbaceous | Grassland | In urban areas, may assume a low-quality green space |
| 81: Pasture/Hay | ||
| 82: Cultivated Crops | ||
| 90: Woody Wetland | Forest | Woody wetlands are common in southern New Jersey and have large proportions of deciduous trees |
| 95: Emergent Herbaceous Wetland | Grassland | Herbaceous (also grassy) wetlands are typical for many coastal regions. |
| Variables | Land Covers | Definition | Commentary |
|---|---|---|---|
| Land Cover Class-Level Metrics | |||
| Class Proportion | Forest, Grass, Shrubs, Industrial, Developed Lands (Open, Low, Medium, High Intensities) | Composition metric. Proportional coverage—% of the landscape covered by each type. | Used by [72,73] and recommended by [36] for green and water space; [74] recommended for Forest, Shrubs and Grass |
| Aggregation Index (AI) | Developed Lands (Open, Low, Medium, High Intensities), Industrial Areas | Configuration metric. Computed as an area-weighted mean class aggregation index, where each class is weighted by its proportional area in the landscape. | Redundant with several other metrics of proportion, cohesion, and contiguity and may be a meaningful alternative [53] |
| Splitting Index | Forest, Grass, Shrubs | Configuration metric. A large splitting index, results from land covers being split into many patches with an even size distribution. | Correlated with the aggregation index. Applied for green spaces only in relation to health outcomes [39]. |
| Contiguity Index (CI) | Developed Lands (Open, Low, Medium, High Intensities), Forest, Grass | Configuration metric. Large contiguous patches will result in larger contiguity index values. | CI for green/tree land cover classes associated with health outcomes [39]. |
| Landscape-Level Metrics | |||
| Shannon Diversity Index | Based on all Land Cover Classes | Composition metric. The more classes and the more equally distributed, the higher the index. | Used for measuring the aesthetic value and diversity [8]. Associated with health outcomes [39]. |
| Patch Richness Density (PRD) | Based on all Land Cover Classes | Number of patches per hectare. High values indicate high dispersion | PRD for green areas and recreational lands associated with poor health [39]. |
| Contagion Index | Based on all Land Cover Classes | Composition metric. High values indicate result from landscapes with a few large, contiguous patches and low dispersion and interspersion of patch types | |
| Average Proportion of Imperviousness | Census Tract Average based on NLCD dataset estimating imperviousness proportion per pixel | Composition metric. Highly negatively correlated with Tree Canopy proportions but is more accurate | Highly correlated (negative) with Tree Canopy Cover but more accurate [75,76] |
| Census-Based Variables | |||
| Poverty Level by Category | Percentage of population 18 and older living below federal poverty level. | Socio-economic status | Associated with cancer outcomes including survival and mortality |
| Median Year Structures Built | Median that the areas residential buildings were constructed. | Organized into categories. | Housing age and conditions are associated with health outcomes [17,77] and poverty [78] |
| Housing Density | Number of structures per area unit (acre) | Continuous variable defined by census tract | Potential intermediate factor in health outcomes [79] |
| Overall (n = 3949) | |
|---|---|
| Age | |
| Mean (SD) | 65.8 (13.3) |
| Median [Min, Max] | 68.0 [21.0, 85.0] |
| Gender | |
| Male | 1878 (47.6%) |
| Female | 2071 (52.4%) |
| Race/Ethnicity | |
| NH-White | 2902 (73.5%) |
| NH-Black | 488 (12.3%) |
| Hispanic (any race) | 325 (8.2%) |
| NH-API | 141 (3.6%) |
| Other | 93 (2.4%) |
| Regional Stage Subcategory | |
| Regional, direct extension only | 1339 (33.9%) |
| Regional, lymph nodes only | 1268 (32.1%) |
| Regional, both | 1342 (34.0%) |
| Vital Status | |
| Censored | 2862 (72.5%) |
| Colon Cancer Death | 1087 (27.5%) |
| Survival Time (months) | |
| Mean (SD) | 62.3 (38.0) |
| Median [Min, Max] | 66.0 [1.00, 139] |
| CT Changes (Type of “moves”) | |
| CT at Date of Diagnosis Only | 2587 (65.5%) |
| Change in Residential CT within NJ | 885 (22.4%) |
| Change in Residential CT outside NJ | 477 (12.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiese, D.; Stroup, A.M.; Maiti, A.; Harris, G.; Lynch, S.M.; Vucetic, S.; Gutierrez-Velez, V.H.; Henry, K.A. Measuring Neighborhood Landscapes: Associations between a Neighborhood’s Landscape Characteristics and Colon Cancer Survival. Int. J. Environ. Res. Public Health 2021, 18, 4728. https://doi.org/10.3390/ijerph18094728
Wiese D, Stroup AM, Maiti A, Harris G, Lynch SM, Vucetic S, Gutierrez-Velez VH, Henry KA. Measuring Neighborhood Landscapes: Associations between a Neighborhood’s Landscape Characteristics and Colon Cancer Survival. International Journal of Environmental Research and Public Health. 2021; 18(9):4728. https://doi.org/10.3390/ijerph18094728
Chicago/Turabian StyleWiese, Daniel, Antoinette M. Stroup, Aniruddha Maiti, Gerald Harris, Shannon M. Lynch, Slobodan Vucetic, Victor H. Gutierrez-Velez, and Kevin A. Henry. 2021. "Measuring Neighborhood Landscapes: Associations between a Neighborhood’s Landscape Characteristics and Colon Cancer Survival" International Journal of Environmental Research and Public Health 18, no. 9: 4728. https://doi.org/10.3390/ijerph18094728
APA StyleWiese, D., Stroup, A. M., Maiti, A., Harris, G., Lynch, S. M., Vucetic, S., Gutierrez-Velez, V. H., & Henry, K. A. (2021). Measuring Neighborhood Landscapes: Associations between a Neighborhood’s Landscape Characteristics and Colon Cancer Survival. International Journal of Environmental Research and Public Health, 18(9), 4728. https://doi.org/10.3390/ijerph18094728