
Climate Change and Health Preparedness in Africa: Analysing Trends in Six African Countries



Abstract
1. Introduction
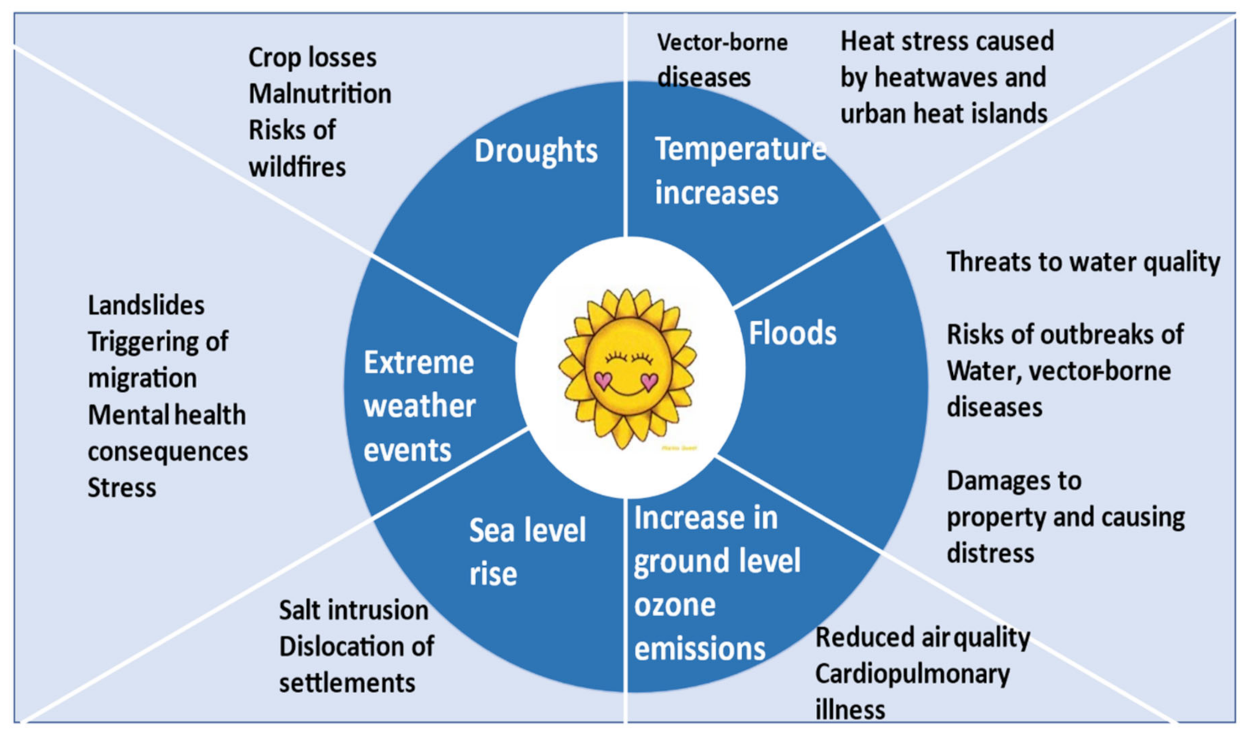
Health Impacts of Climate Change in Africa
2. Methodology
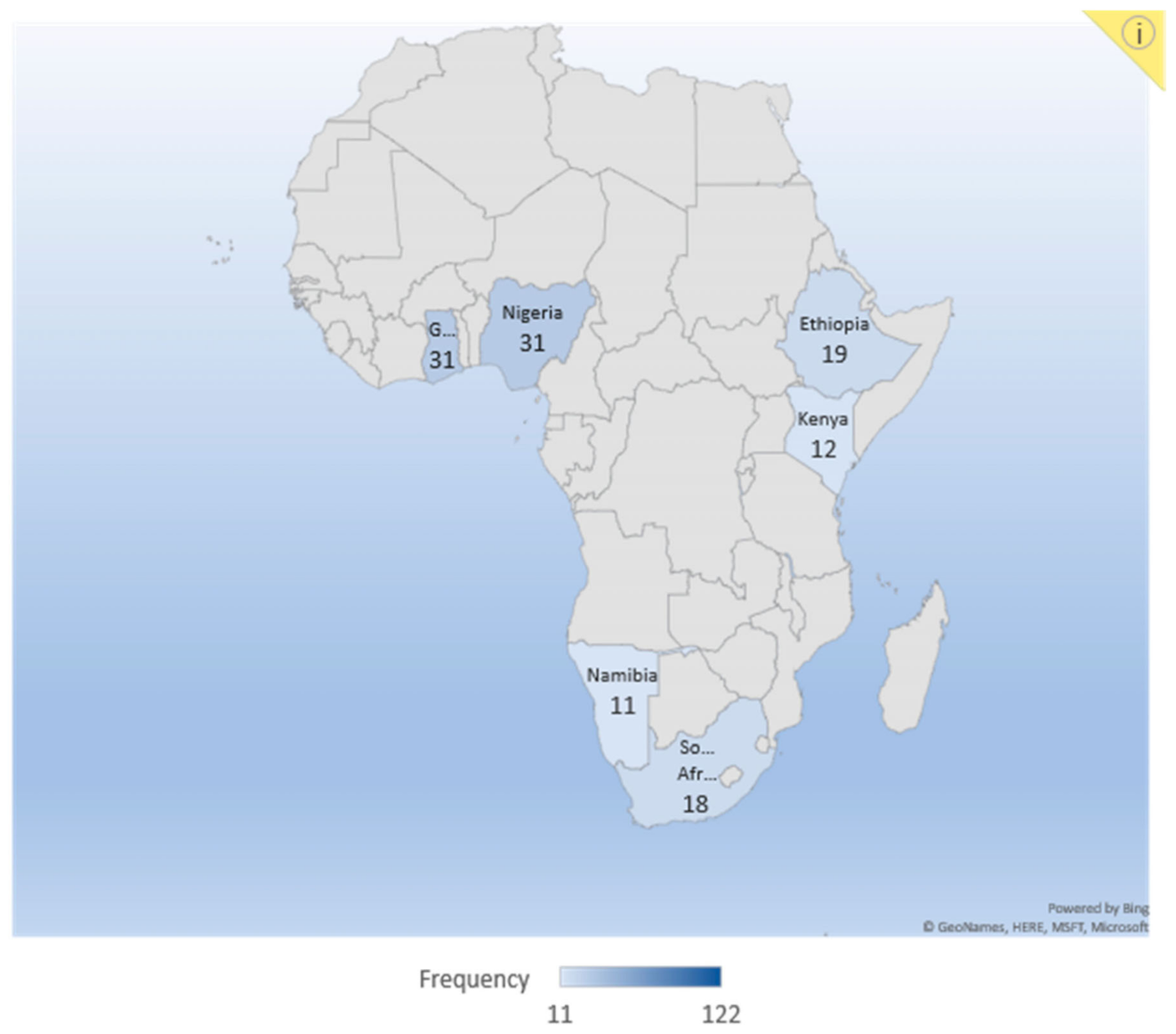
2.1. Data and Sample
2.1.1. Secondary Data
2.1.2. Primary Data Collection
3. Results
3.1. Respondents Background Information
3.2. Respondents Knowledge and Perception of Climate Change and Health Impacts
- Infectious diseases related to changes in vector biology, water, and food contamination.
- Injuries and fatalities related to extreme weather events and heatwaves.
- Allergic symptoms related to increased allergen production.
- Mental health consequences, civil conflicts, and population dislocation.
3.3. Public Health’ Vulnerability to Climate Change Impacts as Perceived by Respondents in Sampled Countries
3.4. The Health Systems’ Preparedness in Dealing with the Health Impacts of Climate Change as Perceived by Respondents
3.5. Available Interventions in Sampled Countries as Perceived by Respondents in Dealing with Health Problems of Climate Change Impacts
3.6. Resources Availability in the Sampled African Countries and Those Needed to Deal with Climate Change Impacts as Perceived by Respondents
4. Discussion
4.1. Vulnerability to Climate Change Impacts on Human Health and the Health Systems’ Perception
4.2. Health System’s Preparedness
4.3. Available Interventions
4.4. Effectiveness of the Available Resources
4.5. Policy Application
- Improve policy frameworks to better consider the many health problems associated with climate change.
- Improve training provisions to raise awareness among professionals in the health sector about the connections between climate change and health.
- Improve frameworks for information exchange and the dissemination of best practice across Africa so that successful initiatives dealing with the nexus of climate change and health may be replicated.
Advantage and Limitations of the Methodology
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Climate Impacts | Most Frequent | More Frequent | Frequent | Less Frequent | Least Frequent |
| Floods | |||||
| Drought | |||||
| Wildfires | |||||
| Extreme temperature | |||||
| Sea level rise | |||||
| Change in Precipitation | |||||
| Increase carbon dioxide | |||||
| Other |
| Most Prevalent | More prevalent | Prevalent | Less Prevalent | Least Prevalent | |
| Malaria and other vector-borne diseases | |||||
| Diarrhoea, water-borne diseases, and sanitation | |||||
| Malnutrition, food-borne and food insecurity | |||||
| Climate-induced mental health consequences | |||||
| Extreme weather events |
| Intervention programs | Yes, and Effective | Yes, but not Effective | No, they do not Exist |
| Water availability, sanitation, and water-borne diseases control | |||
| Vector control | |||
| Nutrition, food safety and distribution during a famine | |||
| Extreme events adaptation |
References
- Halim, S.A.; Dasgupta, P.; Hayward, B.; Kanninen, M. Chapter 5: Sustainable Development, Poverty Eradication 2 and Reducing Inequalities 2017. Available online: https://www.ipcc.ch/site/assets/uploads/sites/2/2019/03/SR15_FOD_Chapter5.pdf (accessed on 25 January 2021).
- Pachauri, D.R.K.; Reisinger, A. IPCC Fourth Assessment Report 2007; Synthesis Report. Contribution of Working Groups I II and III to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2007; p. 17. [Google Scholar]
- Stocker, T.F.; Qin, D.; Plattner, G.-K.; Tignor, M.M.B.; Allen, S.K.; Boschung, J. Working Group I Contribution to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change 2014; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2007; p. 14. [Google Scholar]
- Falkner, R. The Paris agreement and the new logic of international climate politics. Int. Aff. 2016, 92, 1107–1125. [Google Scholar] [CrossRef]
- Tchilibou, M.; Delcroix, T.; Alory, G.; Arnault, S.; Reverdin, G. Variations of the tropical Atlantic and Pacific, S.S.S. minimum zones and their relations to the ITCZ and SPCZ rain bands (1979–2009). J. Geophys. Res. Ocean. 2015, 120, 5090–5100. [Google Scholar] [CrossRef]
- Mpelasoka, F.; Awange, J.L.; Zerihun, A. Influence of coupled ocean-atmosphere phenomena on the Greater Horn of Africa droughts and their implications. Sci. Total. Environ. 2018, 610–611, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Erickson, L.E. Reducing greenhouse gas emissions and improving air quality: Two global challenges. Environ. Prog. Sustain. Energy 2017, 36, 982–988. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases: Key Facts. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 26 October 2020).
- Ritchie, H.; Roser, M. Causes of Death; Published online at OurWorldInData.og. 2018. Available online: https://ourworldindata.org/causes-of-death (accessed on 25 January 2021).
- Siderius, C.; Gannon, K.E.; Ndiyoi, M.; Opere, A.; Batisani, N.; Olago, D.; Pardoe, J.; Conway, D. Hydrological response and complex impact pathways of the 2015/2016 El Niño in eastern and southern Africa. Earth’s Future 2018, 6, 2–22. [Google Scholar] [CrossRef]
- Dessalegn, O.G.; Akalu, D.S. The impacts of climate change on African continent and the way forward. J. Ecol. Nat. Environ. 2015, 7, 256–262. [Google Scholar] [CrossRef]
- Singh, V.P. Impact of climate change on the hydrologic cycle and implications for society. Environ. Soc. Psychol. 2015, 1, 36–49. [Google Scholar] [CrossRef]
- Ramin, B.M.; McMichael, A.J. Climate change and health in Sub-Saharan Africa: A case-based perspective. EcoHealth 2009, 6, 52–57. [Google Scholar] [CrossRef]
- De Souza, D.; Kelly-Hope, L.; Lawson, B.; Wilson, M.; Boakye, D. Environmental factors associated with the distribution of Anopheles Gambiae s.s in Ghana; an important vector of lymphatic filariasis and malaria. PLoS ONE 2010, 5, e9927. [Google Scholar] [CrossRef]
- De Souza, K.; Kituyi, E.; Harvey, B.; Leone, M.; Murali, K.S.; Ford, J.D. Vulnerability to climate change in three hot spots in Africa and Asia: Key issues for policy-relevant adaptation and resilience-building research. Reg. Environ. Chang. 2015, 15, 747–753. [Google Scholar] [CrossRef]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Stern, D.I.; Kaufmann, R.K. Anthropogenic and natural causes of climate change. Clim. Chang. 2014, 122, 257–269. [Google Scholar] [CrossRef]
- Szulejko, J.E.; Kumar, P.; Deep, A.; Kim, K.-H. Global warming projections to 2100 using simple CO2 greenhouse gas modeling and comments on CO2 climate sensitivity factor. Atmospheric Pollut. Res. 2017, 8, 136–140. [Google Scholar] [CrossRef]
- Campbell-Lendrum, D.; Manga, L.; Bagayoko, M.; Sommerfeld, J. Climate change and vector-borne diseases: What are the implications for public health research and policy? Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20130552. [Google Scholar] [CrossRef]
- Abaya, S.W.; Mandere, N.M.; Winqvist, N. Health officials’ perceptions of and preparedness for the impacts of climate variability on human health in the Somali region of Ethiopia. Mitig. Adapt. Strat. Glob. Chang. 2011, 16, 585–596. [Google Scholar] [CrossRef]
- Chersich, M.F.; Wright, C.Y.; Venter, F.; Rees, H.; Scorgie, F.; Erasmus, B. Impacts of climate change on health and wellbeing in South Africa. Int. J. Environ. Res. Public Health 2018, 15, 1884. [Google Scholar] [CrossRef]
- Brousse, O.; Georganos, S.; Demuzere, M.; Vanhuysse, S.; Wouters, H.; Wolff, E.; Linard, C.; van Lipzig, N.P.-M.; Dujardin, S. Using local climate zones in Sub-Saharan Africa to tackle urban health issues. Urban Clim. 2019, 27, 227–242. [Google Scholar] [CrossRef]
- Schulte-Uebbing LHansen, G.; Hernández, A.M.; Winter, M. Chapter scientists in the IPCC AR5—experience and lessons learned. Curr. Opin. Environ. Sustain. 2015, 14, 250–256. [Google Scholar] [CrossRef]
- Frumkin, H.; Hess, J.; Luber, G.; Malilay, J.; McGeehin, M. Climate change: The public health response. Am. J. Public Health 2008, 98, 435–445. [Google Scholar] [CrossRef]
- Hathaway, J.; Maibach, E.W. Health implications of climate change: A review of the literature about the perception of the public and health professionals. Curr. Environ. Health Rep. 2018, 5, 197–204. [Google Scholar] [CrossRef]
- Rahman, M.S.; Bin Mohamad, O.; Bin Abu Zarim, Z. Climate change: A review of its health impact and perceived awareness by the young citizens. Glob. J. Health Sci. 2014, 6, 196–204. [Google Scholar] [CrossRef]
- Byass, P. Climate change and population health in Africa: Where are the scientists? Glob. Health Action 2009, 2, 2065. [Google Scholar] [CrossRef]
- Trtanj, J.; Jantarasami, L.; Brunkard, J.; Collier, T.; Jacobs, J.; Lipp, E.; McLellan, S.; Moore, S.; Paerl, H.; Ravenscroft, J.; et al. 6: Climate Impacts on Water-Related Illness. The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; U.S. Global Change Research Program: Washington, DC, USA, 2016. [Google Scholar]
- De Magny, G.C.; Cazelles, B.; Guégan, J.-F. Cholera threat to humans in Ghana is influenced by both global and regional climatic variability. EcoHealth 2007, 3, 223–231. [Google Scholar] [CrossRef]
- Leckebusch, G.C.; Abdussalam, A.F. Climate and socioeconomic influences on interannual variability of cholera in Nigeria. Health Place 2015, 34, 107–117. [Google Scholar] [CrossRef]
- Nkoko, D.B.; Giraudoux, P.; Plisnier, P.-D.; Tinda, A.M.; Piarroux, M.; Sudre, B.; Horion, S.; Tamfum, J.-J.M.; Ilunga, B.K.; Piarroux, R. Dynamics of cholera outbreaks in great lakes region of Africa, 1978–2008. Emerg. Infect. Dis. 2011, 17, 2026–2034. [Google Scholar] [CrossRef]
- Abu, M.; Codjoe, S.N.A. Experience and future perceived risk of floods and diarrheal disease in urban poor communities in Accra, Ghana. Int. J. Environ. Res. Public Health 2018, 15, 2830. [Google Scholar] [CrossRef]
- Musengimana, G.; Mukinda, F.K.; Machekano, R.; Mahomed, H. Temperature variability and occurrence of diarrhoea in children under five-years-old in cape town metropolitan sub-districts. Int. J. Environ. Res. Public Health 2016, 13, 859. [Google Scholar] [CrossRef]
- Azage, M.; Kumie, A.; Worku, A.; Bagtzoglou, A.C.; Anagnostou, E. Effect of climatic variability on childhood diarrhea and its high risk periods in northwestern parts of Ethiopia. PLoS ONE 2017, 12, e0186933. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, H.; Sanseovic, A.-M. Possible Linkages Between Algae Toxins in Drinking Water and Related illnesses in Windhoek, Namibia 2001; p. 34. Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:hkr:diva-4761 (accessed on 25 January 2021).
- Tschakert, P.; Ricciardi, V.; Smithwick, E.; Machado, M.; Ferring, D.; Hausermann, H.; Bug, L. Situated knowledge of pathogenic landscapes in Ghana: Understanding the emergence of Buruli ulcer through qualitative analysis. Soc. Sci. Med. 2016, 150, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Ekpo, U.F.; Mafiana, C.F.; O Adeofun, C.; Solarin, A.R.; Idowu, A.B. Geographical information system and predictive risk maps of urinary schistosomiasis in Ogun State, Nigeria. BMC Infect. Dis. 2008, 8, 74–111. [Google Scholar] [CrossRef]
- Adu-Prah, S.; Tetteh, E.K. Spatiotemporal analysis of climate variability impacts on malaria prevalence in Ghana. Appl. Geogr. 2015, 60, 266–273. [Google Scholar] [CrossRef]
- Weli, V.E.; Efe, S.I. Climate and epidemiology of malaria in port Harcourt region, Nigeria. Am. J. Clim. Chang. 2015, 4, 40–47. [Google Scholar] [CrossRef]
- Adeola, A.M.; Botai, J.O.; Rautenbach, H.; Adisa, O.M.; Ncongwane, K.P.; Botai, C.M.; Adebayo-Ojo, T.C. Climatic variables and malaria morbidity in Mutale local municipality, South Africa: A 19-year data analysis. Int. J. Environ. Res. Public Health 2017, 14, 1360. [Google Scholar] [CrossRef] [PubMed]
- Komen, K.; Olwoch, J.; Rautenbach, H.; Botai, J.; Adebayo, A. Long-run relative importance of temperature as the main driver to Malaria transmission in Limpopo province, South Africa: A simple econometric approach. EcoHealth 2014, 12, 131–143. [Google Scholar] [CrossRef]
- Codjoe, S.N.A.; Nabie, V.A. Climate change and Cerebrospinal Meningitis in the Ghanaian Meningitis Belt. Int. J. Environ. Res. Public Health 2014, 11, 6923–6939. [Google Scholar] [CrossRef]
- Bauer, J.M.; Mburu, S. Effects of drought on child health in Marsabit district, northern Kenya. Econ. Hum. Biol. 2017, 24, 74–79. [Google Scholar] [CrossRef]
- Grace, K.; Davenport, F.; Funk, C.; Lerner, A.M. Child malnutrition and climate in Sub-Saharan Africa: An analysis of recent trends in Kenya. Appl. Geogr. 2012, 35, 405–413. [Google Scholar] [CrossRef]
- Hagos, S.; Lunde, T.; Mariam, D.H.; Woldehanna, T.; Lindtjørn, B. Climate change, crop production and child under nutrition in Ethiopia; a longitudinal panel study. BMC Public Health 2014, 14, 884. [Google Scholar] [CrossRef]
- Atitsogbey, P. The impact of climate change on food and nutrition security in the Bongo district of the upper east region of Ghana. Bachelor’s Thesis, University of Ghana, Accra, Ghana, 2016; p. 153. [Google Scholar]
- Codjoe, S.N.A.; Owusu, G. Climate change/variability and food systems: Evidence from the Afram Plains, Ghana. Reg. Environ. Chang. 2011, 11, 753–765. [Google Scholar] [CrossRef]
- Achaglinkame, M.A.; Opoku, N.; Amagloh, F.K. Aflatoxin contamination in cereals and legumes to reconsider usage as complementary food ingredients for Ghanaian infants: A review. J. Nutr. Intermed. Metab. 2017, 10, 1–7. [Google Scholar] [CrossRef]
- Armah, F.A.; Odoi, J.O.; Yengoh, G.T.; Obiri, S.; Yawson, D.O.; Afrifa, E.K.A. Food security and climate change in drought-sensitive savanna zones of Ghana. Mitig. Adapt. Strat. Glob. Chang. 2010, 16, 291–306. [Google Scholar] [CrossRef]
- Onafeso, O.D.; Akanni, C.O.; Badejo, B.A. Climate change dynamics and imperatives for food security in Nigeria. Indones. J. Geogr. 2016, 47, 151. [Google Scholar] [CrossRef]
- Idoko, I.D. An impact assessment of flooding on food security among rural farmers in dagiri community, of Gwagwalada area council, Abuja, Nigeria. Agric. Dev. 2016, 1, 6–13. [Google Scholar] [CrossRef]
- Masipa, T.S. The impact of climate change on food security in South Africa: Current realities and challenges ahead. Jàmbá J. Disaster Risk Stud. 2017, 9, 7. [Google Scholar] [CrossRef]
- Akudugu, M.A.; Alhassan, A.-R. Climate change menace, food security, livelihoods, and social safety in northern Ghana. Int. J. Sustain. Dev. 2012, 1, 80–95. [Google Scholar]
- Endalew, B.; Muche, M.; Tadesse, S. Assessment of food security situation in Ethiopia: A review. Asian J. Agric. Res. 2015, 9, 55–68. [Google Scholar] [CrossRef]
- Hooli, L.J. Resilience of the poorest: Coping strategies and indigenous knowledge of living with the floods in northern Namibia. Reg. Environ. Chang. 2015, 16, 695–707. [Google Scholar] [CrossRef]
- Anthonj, C.; Nkongolo, O.T.; Schmitz, P.; Hango, J.N.; Kistemann, T. The impact of flooding on people living with HIV: A case study from the Ohangwena region, Namibia. Glob. Health Action 2015, 8, 26441. [Google Scholar] [CrossRef]
- Shifidi, V.T.; Tuwilika, S.V. Impact of flooding on rural livelihoods of the Cuvelai Basin in northern Namibia. J. Geogr. Reg. Plan. 2016, 9, 104–121. [Google Scholar] [CrossRef]
- Angula, M.N.; Kaundjua, M.B. The changing climate and human vulnerability in north-central Namibia. Jàmbá: J. Disaster Risk Stud. 2016, 8, 7. [Google Scholar] [CrossRef]
- Addo, I.Y.; Danso, S. Sociocultural factors and perceptions associated with voluntary and permanent relocation of flood victims: A case study of Sekondi-Takoradi Metropolis in Ghana. Jàmbá J. Disaster Risk Stud. 2017, 9, 157. [Google Scholar] [CrossRef]
- Dziwornu, E.; Kugbey, N. Mental health problems and coping among flood victims in Ghana: A comparative study of victims and non-victims. Curr. Res. Psychol. 2015, 6, 15–21. [Google Scholar] [CrossRef]
- Shabu, T.; Adaaku, E.M. Natural disaster and household vulnerability to crime in flood-prone areas of urban centres in Nigeria. Ph.D. Thesis, Benue State University, Makurdi, Nigeria, 2018; p. 16. [Google Scholar]
- Acharibasam, J.W.; Anuga, S.W. Psychological distance of climate change and mental health risks assessment of smallholder farmers in northern Ghana: Is habituation a threat to climate change? Clim. Risk Manag. 2018, 21, 16–25. [Google Scholar] [CrossRef]
- Ajibade, I.; McBean, G.; Bezner-Kerr, R. Urban flooding in Lagos, Nigeria: Patterns of vulnerability and resilience among women. Glob. Environ. Chang. 2013, 23, 1714–1725. [Google Scholar] [CrossRef]
- Eludoyin, O.M.; Adelekan, I.O.; Webster, R.; Eludoyin, A.O. Air temperature, relative humidity, climate regionalization and thermal comfort of Nigeria. Int. J. Clim. 2013, 34, 2000–2018. [Google Scholar] [CrossRef]
- Daniel, O.A. Urban extreme weather: A challenge for a healthy living environment in Akure, Ondo State, Nigeria. Climate 2015, 3, 775–791. [Google Scholar] [CrossRef]
- Wichmann, J. Heat effects of ambient apparent temperature on all-cause mortality in Cape Town, Durban and Johannesburg, South Africa: 2006–2010. Sci. Total. Environ. 2017, 587–588, 266–272. [Google Scholar] [CrossRef]
- Frimpong, K.; MPHIL development studies; Van Etten, E.J.E.; Oosthuzien, J.; Nunfam, V.F. Heat exposure on farmers in northeast Ghana. Int. J. Biometeorol. 2016, 61, 397–406. [Google Scholar] [CrossRef]
- Ngwenya, B.; Oosthuizen, J.; Cross, M.; Frimpong, K.; Chaibva, C.N. A review of heat stress policies in the context of climate change and its impacts on outdoor workers. Int. J. Soc. Ecol. Sustain. Dev. 2018, 9, 1–11. [Google Scholar] [CrossRef]
- Mathee, A.; Oba, J.; Rose, A. Climate change impacts on working people (the HOTHAPS initiative): Findings of the South African pilot study. Glob. Health Action 2010, 3, 5612. [Google Scholar] [CrossRef]
- Oa, O.V.A.O. A review of the future of tourism in coastal Kenya: The challenges and opportunities posed by climate change. J. Earth Sci. Clim. Chang. 2014, 5. [Google Scholar] [CrossRef]
- United Nations. African Countries by Population (2021)—Worldometer 2019. Available online: https://www.worldometers.info/population/countries-in-africa-by-population/ (accessed on 25 January 2021).
- Saidi, S.M.; Lijima, Y.; Sang, W.K.; Mwangudza, A.K.; Oundo, J.O.; Taga, K.; Aihara, M.; Nagayama, K.; Yamamoto, H.; Waiyaki, P.G.; et al. Epidemiological study on infectious diarrheal diseases in children in a coastal rural area of Kenya. Microbiol. Immunol. 1997, 41, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Tsegaw, T.; Gadisa, E.; Seid, A.; Abera, A.; Teshome, A.; Mulugeta, A.; Herrero, M.; Argaw, D.; Jorge, A.; Aseffa, A. Identification of environmental parameters and risk mapping of visceral leishmaniasis in Ethiopia by using geographical information systems and a statistical approach. Geospat. Health 2013, 7, 299. [Google Scholar] [CrossRef] [PubMed]
- Kipruto, E.K.; Ochieng, A.O.; Anyona, D.N.; Mbalanya, M.; Mutua, E.N.; Onguru, D.; Nyamongo, I.K.; Estambale, B.B.A. Effect of climatic variability on malaria trends in Baringo county, Kenya. Malar. J. 2017, 16, 220. [Google Scholar] [CrossRef]
- Delbiso, T.D.; Altare, C.; Rodriguez-Llanes, J.M.; Doocy, S.; Guha-Sapir, D. Drought and child mortality: A meta-analysis of small-scale surveys from Ethiopia. Sci. Rep. 2017, 7, 2212. [Google Scholar] [CrossRef]
- Hendriks, S.L.; Van Der Merwe, C.; Ngidi, M.S.; Manyamba, C.; Mbele, M.; McIntyre, A.M.; Mkandawire, E.; Molefe, Q.N.; Mphephu, M.Q.; Ngwane, L. What are we measuring? Comparison of household food security indicators in the eastern cape province, South Africa. Ecol. Food Nutr. 2016, 55, 141–162. [Google Scholar] [CrossRef]
- Filho, W.L.; Balogun, A.-L.; Ayal, D.Y.; Bethurem, E.M.; Murambadoro, M.; Mambo, J.; Taddese, H.; Tefera, G.W.; Nagy, G.J.; Fudjumdjum, H.; et al. Strengthening climate change adaptation capacity in Africa—Case studies from six major African cities and policy implications. Environ. Sci. Policy 2018, 86, 29–37. [Google Scholar] [CrossRef]
- Watkins, K.; Ugaz, C.; Gaye, A.; Ha, W.; Johansson, C.; Kennedy, A. Human Development Report 2007–2008: Fighting Climate Change: Human Solidarity in a Divided World; United Nations Development Programme (UNDP): New York, NY, USA, 2007. [Google Scholar]
- Keim, M.E. Building human resilience. Am. J. Prev. Med. 2008, 35, 508–516. [Google Scholar] [CrossRef]
- Newman, L.; Dale, A. Network structure, diversity, and proactive resilience building: A response to Tompkins and Adger. Ecol. Soc. 2005, 10, 10. [Google Scholar] [CrossRef]
- Hughes, T.P.; Baird, A.H.; Bellwood, D.R.; Card, M.; Connolly, S.R.; Folke, C.; Grosberg, R.; Hoegh-Guldberg, O.; Jackson, J.B.C.; Kleypas, J.; et al. Climate change, human impacts, and the resilience of coral reefs. Science 2003, 301, 929–933. [Google Scholar] [CrossRef]
- Ulhøi, J.P.; Ulhøi, B.P. Beyond climate focus and disciplinary myopia. The roles and responsibilities of hospitals and healthcare professionals. Int. J. Environ. Res. Public Health 2009, 6, 1204–1214. [Google Scholar] [CrossRef]
- Bell, J.; Herring, S.; Jantarasami, L.; Adrianopoli, C.; Benedict, K.; Conlon, K.; Escobar, V.; Hess, J.; Luvall, J.; Garcia-Pando, C.; et al. 4: Impacts of Extreme Events on Human Health. The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment; U.S. Global Change Research Program: Washington, DC, USA, 2016. [Google Scholar]
- Nichols, M.; Sarfo, F.S.; Singh, A.; Qanungo, S.; Treiber, F.; Ovbiagele, B.; Saulson, R.; Patel, S.; Jenkins, C.; Stephen, S.F. Assessing mobile health capacity and task shifting strategies to improve hypertension among Ghanaian stroke survivors. Am. J. Med. Sci. 2017, 354, 573–580. [Google Scholar] [CrossRef]
- McDermott-Levy, R.; Jackman-Murphy, K.P.; Leffers, J.M.; Jordan, L. Integrating climate change into nursing curricula. Nurse Educ. 2019, 44, 43–47. [Google Scholar] [CrossRef]
- Leffers, J.; Levy, R.M.; Nicholas, P.K.; Sweeney, C.F. Mandate for the nursing profession to address climate change through nursing education. J. Nurs. Sch. 2017, 49, 679–687. [Google Scholar] [CrossRef]
- Finkel, M.L. A call for action: Integrating climate change into the medical school curriculum. Perspect. Med. Educ. 2019, 8, 265–266. [Google Scholar] [CrossRef]
- Wellbery, C.; Sheffield, P.; Timmireddy, K.; Sarfaty, M.; Teherani, A.; Fallar, R. It’s time for medical schools to introduce climate change into their curricula. Acad. Med. 2018, 93, 1774–1777. [Google Scholar] [CrossRef]
- Saltzman, H.M. Medical school curricula should highlight environmental health. Acad. Med. 2019, 94, 1406. [Google Scholar] [CrossRef]
- Hayes, K.; Blashki, G.; Wiseman, J.; Burke, S.; Reifels, L. Climate change and mental health: Risks, impacts and priority actions. Int. J. Ment. Health Syst. 2018, 12, 28. [Google Scholar] [CrossRef]
- Burke, S.E.L.; Sanson, A.V.; Van Hoorn, J. The psychological effects of climate change on children. Curr. Psychiatry Rep. 2018, 20, 35. [Google Scholar] [CrossRef]
- Hess, J.J.; McDowell, J.Z.; Luber, G. Integrating climate change adaptation into public health practice: Using adaptive management to increase adaptive capacity and build resilience. Environ. Health Perspect. 2012, 120, 171–179. [Google Scholar] [CrossRef]
- Shezi, B.; Mathee, A.; Siziba, W.; Street, R.A.; Naicker, N.; Kunene, Z.; Wright, C.Y. Environmental health practitioners potentially play a key role in helping communities adapt to climate change. BMC Public Health 2019, 19, 54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Impacts | Author (Year) | Study Period (Year) | City/Country | Study Population | Study Design/Statistical Model | Exposure | Outcome |
|---|---|---|---|---|---|---|---|
| Water, sanitation, and water-borne diseases | [32] | 2012 | Jamestown/Agbogbloshie (Ghana) | 401 Households | Cross-sectional Descriptive, bivariate, and Multivariate | Floods | Reported cases of diarrheal diseases. A strong correlation between flooding and diarrheal disease. |
| [30] | 1990–2011 | North-West (Nigeria) | Morbidity and mortality dataset on cholera cases | Ecological. Stepwise multiple regression, G.A.M. | Min/Max temp, annual Temp and RH | A significant correlation between cholera and annual min/max temperature and rainfall with 1716 deaths from 41,784 cases in 2010 in 18 states. | |
| [33] | 2012–2014 | Cape Town (South Africa) | Surveillance database on 58,617 children under five years. | Poisson regression | Min and Max temp | A 32% to 40% increase in diarrhoea incidence at 5 oC increase in Min and Max Temp. | |
| [34] | 2013–2015 | Amhara region (Ethiopia) | Retrospective data on children under five years | Ecological Negative Binomial | Average monthly Temp and rainfall | A monthly incidence rate of childhood diarrhoea at 11.4 per 1000 (95% Cl) was significantly associated with mean average temperature and rainfall. | |
| [72] | 1991–1993 | Hospital-Based (Malindi). (Kenya). | 862 children under five years old | Case-control Binary logistic regression | Rainfall and Temperature | A strong positive correlation between rainfall, temperature, and childhood bloody diarrhoea. | |
| Vector-borne diseases. | [38] | 1995–2006 | National (Ghana) | Reported cases of malaria ranging from 5054 to 347,000 per 100,000 | Ecological GLLMM and Local Moran’s I | Rainfall, temperature, and humidity | A statistically significant correlation between temperature, humidity, and malaria incidence with a less significant association with rainfall as it only predicted malaria prevalence. |
| [39] | 1998–2008 | Ondo state (Nigeria) | Data on weather variability; cases of malaria in 18 government hospitals | Ecological Poisson multiple regression | Air and sea surface temp. | The occurrence of monthly malaria of 53.4% and 29% at 1 oC increase in air and sea surface temp. | |
| [40] | 1998–2017 | Mutale (Limpopo province) (South Africa) | Malaria and climate data | Ecological Spearman correlation SARIMA | Temp. Rainfall RH | A positive significant association malaria incidence and total monthly rainfall, min and max temp., average temp., and mean relative humidity. | |
| [73] | 1989–2009 | Amhara, SNNPR, Tigray, Oromia (Ethiopia) | Data on cases of visceral leishmaniasis cases and meteorological data | Ecological Binary and multivariate regression | Annual average Temp. and rainfall | 94.7% of Vl cases occurred between 20–37 °C of annual average Temp, with fewer cases with increasing rainfall. | |
| [74] | 2004–2014 | Baringo county. (Kenya) | Malaria data from 10 health facilities; meteorological data | Ecological Negative binomial regression | Rainfall and Temp. | Rainfall increased malaria transmission across four zones at a time lag of 2 months while temp. increased cases of malaria in riverine and highland zones at time lad of 0 and one month. | |
| Extreme weather events | [59] | Secondi-Takoradi (Ghana) | 207 heads of households | Mixed cross-sectional Descriptive analysis | Floods | Report of psychological, environmental, and economic problems; disease outbreaks (malaria, cholera, and dysentery). | |
| (Eludoyin et al., 2013 [65] | 1951–2009; 2003–2012 | National Akure (Nigeria) | Secondary data Data on the incidence of heat rash. | Ecological Descriptive and correlation analysis | Extreme temperature | Population experience of thermal stress since year 2000 and a significant heat rash among the population between September and December from 2003 to 2012. | |
| [55] | 2011–2012 | Ohangwena, Oshana, Omusata (Namibia) | 282 households | Cross-sectional | Floods | A remarkable but unspecified number of deaths, injuries, illness from resulting floods. | |
| [66] | 2006–2010 | Cape Town, Durban, J’berg (South Africa) | Ambient temperature-all-cause mortality | Case-cross over epidemiological design G.A.M. | Ambient Temp. | Increased temperature above the city-specific threshold significantly increased the general population risk of death (number not specified). | |
| [75] | 2009–2014 | National survey (Ethiopia) | 55,219 children under five years old | Meta-analysis Bayesian Poisson | Drought | Minimal food-insecure areas showed elevated U5DR compared to stressed food-insecure areas as death rate increases as the prevalence of acute malnutrition increases. | |
| Nutrition, food security and distribution | [46] | 2016 | Bongo District (Ghana) | 246 Mother–child pairs (children under 5 years) | Mixed-method cross-sectional Descriptive statistics | Drought | Malnutrition and food insecurity resulted from drought impact, 97.2% being food insecure; children stunting (42.3%), underweight (24.4%) and wasting (17.5%). |
| [50] | 2015 | National data (Nigeria) | Food and crop production index, population density, annual average temp, and rainfall. | Ecological Bivariate correlation and multiple regression | Floods, drought, land use and cover change. | Country’s food deficit due to low agricultural production; hence the country’s dependence on food import. Malnutrition resulting from food insecurity. | |
| [76] | 2013–2014 | Dubana and Kwathehle (South Africa) | Children between 24 and 59 months and their caregivers | Cross-sectional Spearman correlation | Summer and winter season | Hunger due to food insecurity was reported in the summer rather than in the winter though their difference in food consumption score was not statistically significant. | |
| [54] | 2014 | All regions (Ethiopia) | National F.A.O. dataset | Ecological study | Drought | A frequent drought increased population food insecurity from 10% to 15%. | |
| [43] | 2009–2013 | Marsabit district (Kenya) | Children under five years old; 924 households | Panel study Descriptive z-score | Drought | Approximately 20% of the children under study were malnourished. | |
| Mental health and wellbeing | [60] | 2015 | Kwaebibrim (History of a flood), West Akyem (no history of a flood) (Ghana) | 400 respondents; 200 from each district | Retrospective cohort study Descriptive | Floods | Flood victims more likely to experience symptoms of mental health problems than the non-victims. Reports of significantly higher levels of obsessive compulsion, depression, anxiety, and other global severity indexes. |
| [61] | 2012 | Urban areas affected by floods. (Nigeria) | 100 victims of flood-induced crime | Cross-sectional Descriptive analysis | Flooding | Flood-induced crime harms human health and wellbeing with possible effects of anxiety, depression, social dysfunction, and loss of confidence. | |
| [21] | 2018 | National (South Africa) | Whole population | Systematic review | Extreme weather events | Population affected by multiple health and social stressors. |
| Country | Number of Respondents | % of the Total |
|---|---|---|
| Ghana | 31 | 25.4% |
| Nigeria | 31 | 25.4% |
| South Africa | 18 | 14.8% |
| Namibia | 11 | 9.0% |
| Ethiopia | 19 | 15.6% |
| Kenya | 12 | 9.8% |
| Total | 122 | 100% |
| Country | Government Agencies | Higher Institutions | Non-Governmental Agencies | Research Institutions | Total within the Country |
|---|---|---|---|---|---|
| Ethiopia | 21.0% | 47.4% | 31.6% | 0.0% | 100.0% |
| Ghana | 46.6% | 26.7% | 6.7% | 20.0% | 100.0% |
| Kenya | 27.2% | 36.4% | 0.0% | 36.4% | 100.0% |
| Namibia | 45.4% | 27.3% | 27.3% | 0.0% | 100.0% |
| Nigeria | 21.2% | 45.5% | 21.2% | 12.1% | 100.0% |
| South Africa | 22.2% | 44.4% | 5.6% | 27.8% | 100.0% |
| % of the total | 30.3% | 38.5% | 15.6% | 15.6% | 100.0% |
| Country | Yes, a Lot | Yes, Some | Yes, Little | Total within the Country |
|---|---|---|---|---|
| Ghana | 19.4% | 61.3% | 19.3% | 100% |
| Nigeria | 42.0% | 54.8% | 3.2% | 100% |
| South Africa | 22.2% | 44.5% | 33.3% | 100% |
| Namibia | 0.0 | 72.7% | 27.3% | 100% |
| Ethiopia | 52.6% | 42.1% | 5.3% | 100% |
| Kenya | 16.7% | 75.0% | 8.3% | 100% |
| % of Total | 28.7% | 56.6% | 14.7% | 100% |
| Country | Increased | No Changes | Decreased | I Do Not Know | Total within the Country |
|---|---|---|---|---|---|
| Ghana | 71.0% | 16.1% | 9.7% | 3.2% | 100% |
| Nigeria | 80.6% | 19.4% | 0.0% | 0.0% | 100% |
| South Africa | 66.7% | 16.7% | 5.5% | 11.1% | 100% |
| Namibia | 81.8% | 9.1% | 9.1% | 0.0% | 100% |
| Ethiopia | 68.5% | 10.5% | 10.5% | 10.5% | 100% |
| Kenya | 75.0% | 0% | 16.7% | 8.3% | 100% |
| % of Total | 73.8% | 13.9% | 7.4% | 4.9% | 100% |
| Country | 1. Preparedness a Priority in the Country 2. Experts to Deal with Climate Impacts (CI) 3. Healthcare Delivery Systems to Address CI. 4. Addressing Mental Illness Caused by Extreme Events. 5. Enough Training of Health Professionals 6. Enough Healthcare Personnel | Yes, but a Little | No, Not at All |
|---|---|---|---|
| 7. Preparedness to Respond to Extreme Events | Fairly Well Prepared | Not so Much Prepared | |
| Ghana | 1. | 58.1% | 22.6% |
| 2. | 61.3% | 22.6% | |
| 3. | 77.4% | 6.5% | |
| 4. | 83.9% | 12.9% | |
| 5. | 67.7% | 16.1% | |
| 6. | 83.9% | 12.9% | |
| 7. | 45.2% | 48.4% | |
| Nigeria | 1. | 58.1% | 25.8% |
| 2. | 51.6% | 22.6% | |
| 3. | 64.5% | 29.0% | |
| 4. | 67.7% | 19.4% | |
| 5. | 67.7% | 22.6% | |
| 6. | 61.3% | 25.8% | |
| 7. | 25.8% | 71.0% | |
| South Africa | 1. | 33.3% | 16.7% |
| 2. | 66.7% | 5.6% | |
| 3. | 55.6% | 27.8% | |
| 4. | 50.0% | 27.8% | |
| 5. | 72.2% | 16.7% | |
| 6. | 55.6% | 16.7% | |
| 7. | 44.4% | 44.4% | |
| Namibia | 1. | 45.5% | 27.3% |
| 2. | 45.5% | 27.3% | |
| 3. | 54.5% | 9.1% | |
| 4. | 63.6% | 27.3% | |
| 5. | 36.4% | 45.5% | |
| 6. | 45.5% | 45.5% | |
| 7. | 19.2% | 72.7% | |
| Ethiopia | 1. | 57.9% | 10.5% |
| 2. | 78.9% | 0.0% | |
| 3. | 94.7% | 0.0% | |
| 4. | 73.7% | 21.1% | |
| 5. | 52.6% | 42.1% | |
| 6. | 52.6% | 36.8% | |
| 7. | 47.4% | 47.4% | |
| Kenya | 1. | 41.7% | 41.7% |
| 2. | 66.7% | 16.7% | |
| 3. | 75.0% | 8.3% | |
| 4. | 66.7% | 25.0% | |
| 5. | 50.0% | 33.3% | |
| 6. | 50.0% | 25.0% | |
| 7. | 50.0% | 47.1% |
| Country | Control of Climate Impacts 1. Water-Borne Diseases Control 2. Vector-Borne Diseases and Vector Control 3. Nutrition, Food Security and Distribution Organisations 4. Extreme Events Adaptation | Available, but Not Effective | Not Available |
|---|---|---|---|
| Ghana | 1. 2. 3. 4. | 77.4% 54.8% 74.2% 58.1% | 3.2% 9.7% 9.7% 22.6% |
| Nigeria | 1. 2. 3. 4. | 45.2% 48.4% 64.5% 54.8% | 16.1% 16.1% 12.9% 22.6% |
| South Africa | 1. 2. 3. 4. | 66.7% 27.8% 55.6% 38.9 | 0.0% 27.8% 0.0% 27.8% |
| Namibia | 1. 2. 3. 4. | 63.6% 18.2% 54.5% 81.8% | 0.00% 9.1% 9.1% 0.0% |
| Ethiopia | 1. 2. 3. 4. | 52.6% 36.8% 36.8% 52.6% | 00% 10.5% 10.5% 5.3% |
| Kenya | 1. 2. 3. 4. | 58.3% 50.0% 50.0% 50.0% | 16.7% 8.3% 25.0% 25.0% |
| Country | Percentages of ‘Not Enough’ as Reported by Respondents |
|---|---|
| Ghana | 77.4% |
| Nigeria | 64.5% |
| South Africa | 50.0% |
| Namibia | 81.8% |
| Ethiopia | 78.9% |
| Kenya | 58.3% |
| Country | 1. Climate Change Incorporated into Public Health Interventions | Yes, but a Little | No, Not at All |
|---|---|---|---|
| 2. Technical Support from the Government | |||
| 3. Budget/Funding Needed | Perceived Percentage Funding/Budget Needed | ||
| Ghana | 83.9% | 12.9% | |
| 1. | 77.4% | 16.1% | |
| 2. | 90.3% | ||
| Nigeria | 1. | 41.9% | 32.3% |
| 2. | 64.5% | 22.6% | |
| 3. | 96.8% | ||
| South Africa | 1. | 38.9% | 22.2% |
| 2. | 22.2% | 44.4% | |
| 3. | 77.8% | ||
| Namibia | 1. | 54.5% | 27.3% |
| 2. | 27.3% | 27.3% | |
| 3. | 90.9% | ||
| Ethiopia | 1. | 63.2% | 21.1% |
| 2. | 47.4% | 42.1% | |
| 3. | 89.5% | ||
| Kenya | 1. | 58.3% | 25.0% |
| 2. | 50.0% | 25.0% | |
| 3. | 91.7% | ||
| Country | 1. Available Resources to Deal with Health Impact of CC | Limited Availability (%) |
|---|---|---|
| 2. Expand and Construct More Hospital and Health Centres. 3. Additional Staffs Needed. 4. Staff Training 5. Medical Equipment Needed. 6. Good Surveillance System 7. Emergency Response Unit/Resources Needed | Needed Resources Perceived (% within a Country) | |
| Ghana | 1. | 61.9% |
| 2. | 83.9% | |
| 3. | 74.2% | |
| 4. | 83.9% | |
| 5. | 83.9% | |
| 6. | 77.4% | |
| 7. | 90.3% | |
| Nigeria | 1. | 61.3% |
| 2. | 80.6% | |
| 3. | 77.4% | |
| 4. | 90.3% | |
| 5. | 90.3% | |
| 6. | 87.1% | |
| 7. | 93.5% | |
| South Africa | 1. | 66.7% |
| 2. | 61.1% | |
| 3. | 55.6% | |
| 4. | 94.4% | |
| 5. | 55.5% | |
| 6. | 44.4% | |
| 7. | 66.7% | |
| Namibia | 1. | 90.9% |
| 2. | 66.6% | |
| 3. | 72.7% | |
| 4. | 81.8% | |
| 5. | 81.8% | |
| 6. | 72.7% | |
| 7. | 63.6% | |
| Ethiopia | 1. | 68.4% |
| 2. | 78.9% | |
| 3. | 89.5% | |
| 4. | 94.7% | |
| 5. | 84.2% | |
| 6. | 78.9% | |
| 7. | 84.4% | |
| Kenya | 1. | 75.0% |
| 2. | 75.0% | |
| 3. | 66.7% | |
| 4. | 91.7% | |
| 5. | 75.0% | |
| 6. | 75.0% | |
| 7. | 66.7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Opoku, S.K.; Filho, W.L.; Hubert, F.; Adejumo, O. Climate Change and Health Preparedness in Africa: Analysing Trends in Six African Countries. Int. J. Environ. Res. Public Health 2021, 18, 4672. https://doi.org/10.3390/ijerph18094672
Opoku SK, Filho WL, Hubert F, Adejumo O. Climate Change and Health Preparedness in Africa: Analysing Trends in Six African Countries. International Journal of Environmental Research and Public Health. 2021; 18(9):4672. https://doi.org/10.3390/ijerph18094672
Chicago/Turabian StyleOpoku, Samuel Kwasi, Walter Leal Filho, Fudjumdjum Hubert, and Oluwabunmi Adejumo. 2021. "Climate Change and Health Preparedness in Africa: Analysing Trends in Six African Countries" International Journal of Environmental Research and Public Health 18, no. 9: 4672. https://doi.org/10.3390/ijerph18094672
APA StyleOpoku, S. K., Filho, W. L., Hubert, F., & Adejumo, O. (2021). Climate Change and Health Preparedness in Africa: Analysing Trends in Six African Countries. International Journal of Environmental Research and Public Health, 18(9), 4672. https://doi.org/10.3390/ijerph18094672