
Depressive Symptom Trajectories and Early Adult Education and Employment: Comparing Longitudinal Cohorts in Canada and the United States

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Sample Characteristics
2.2. Measures
2.2.1. Education and Employment Outcomes
2.2.2. Depressive Symptoms
2.2.3. Confounders
2.3. Data Handling and Analyses
3. Results
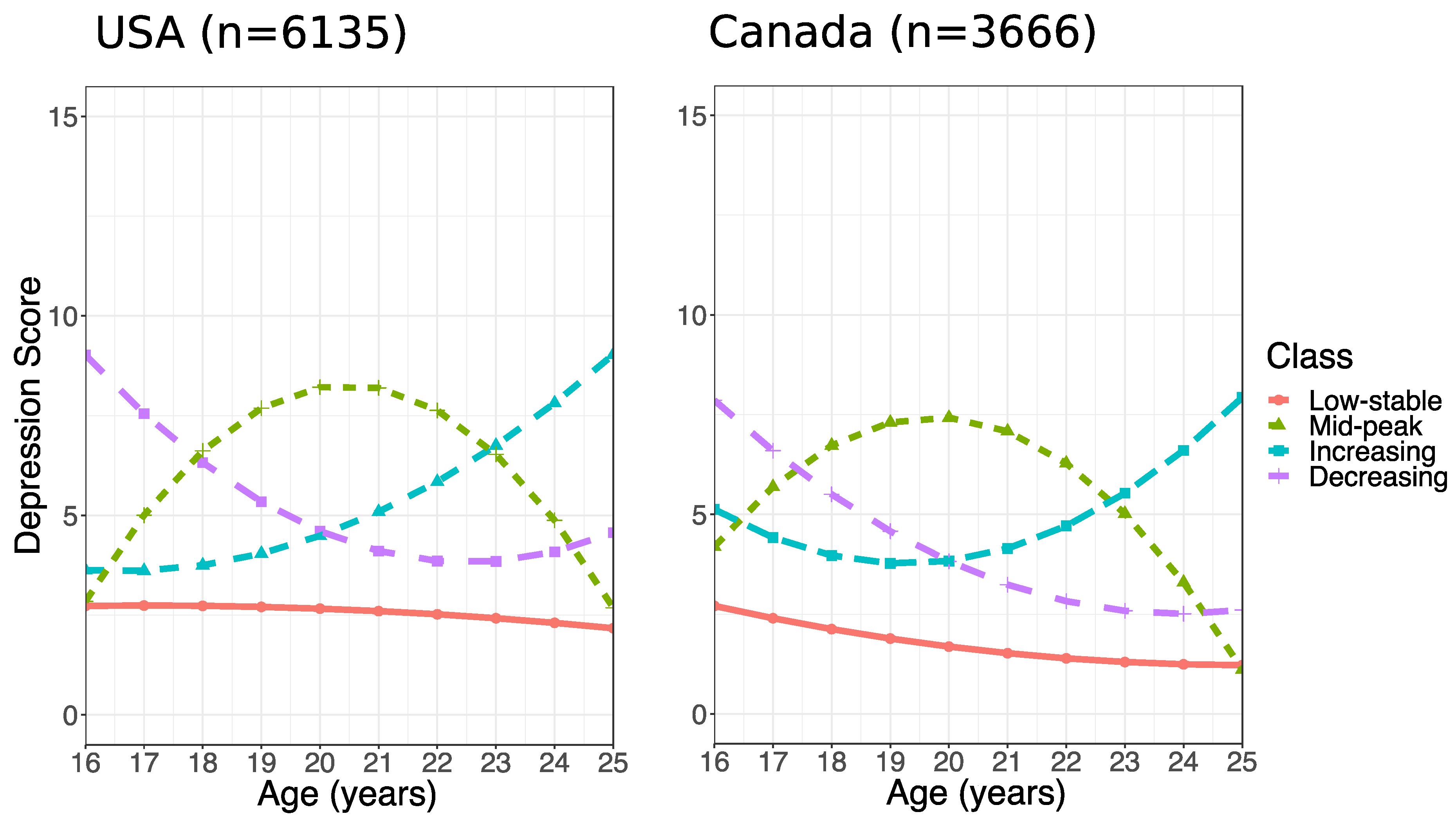
3.1. Distribution of Depressive Symptom Trajectories and Early Adult Education and Employment in Canada and the USA
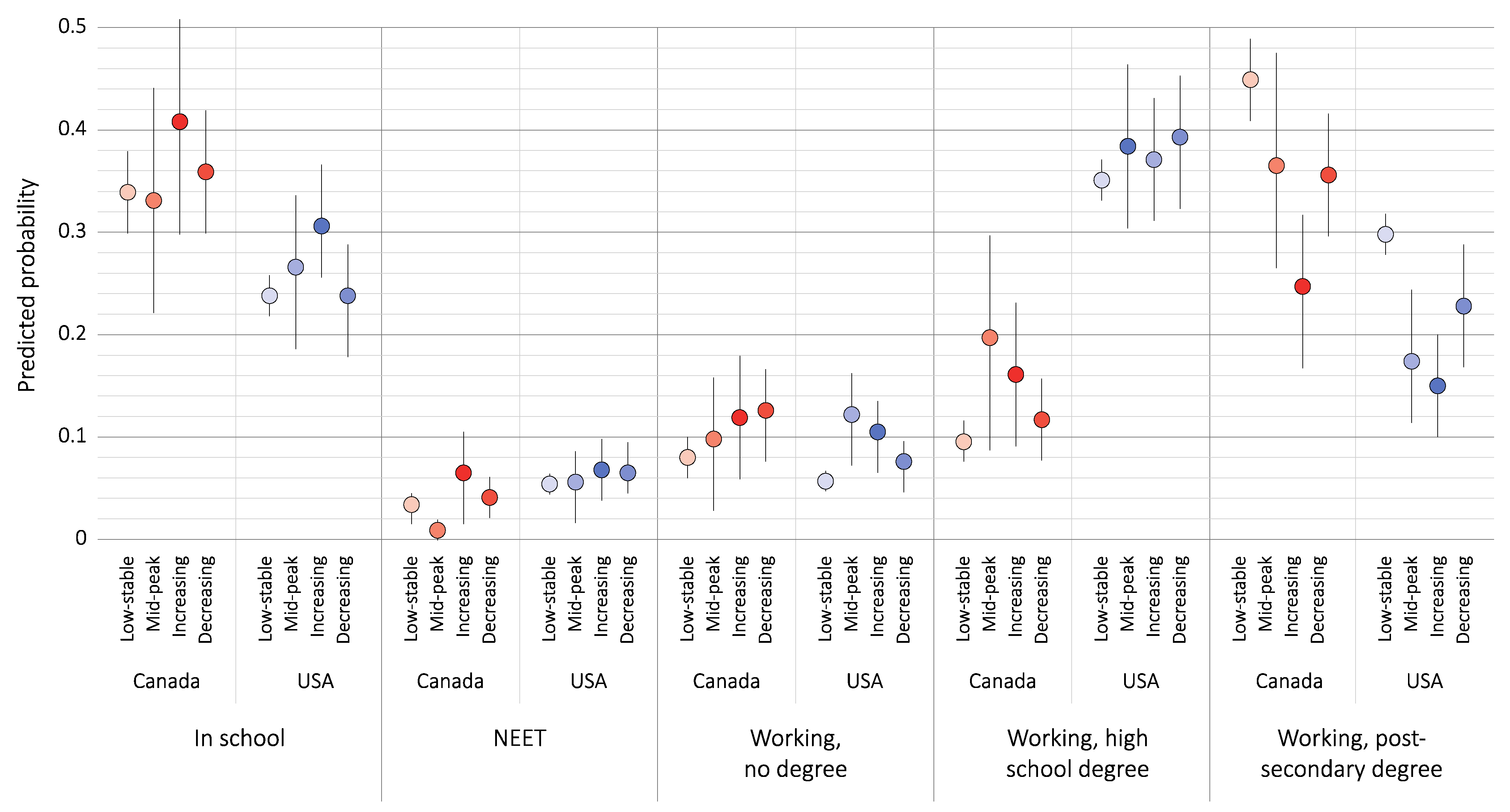
3.2. Association between Depressive Symptom Trajectories and Early Adult Education and Employment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davidson, J.; Arim, R. A Profile of Youth Not in Employment, Education or Training (NEET) in Canada, 2015 to 2017; Analytical Studies Branch Research Paper Series; Statistics Canada: Ottawa, ON, Canada, 2019.
- United Nations. Sustainable Development Goal 8; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Barham, C.; Walling, A.; Clancy, G.; Hicks, S.; Conn, S. Young people and the labour market. Econ. Labour Market Rev. 2009, 3, 17–29. [Google Scholar] [CrossRef]
- Roberts, S. Beyond ‘NEET’ and ‘tidy’ pathways: Considering the ‘missing middle’ of youth transition studies. J. Youth Stud. 2011, 14, 21–39. [Google Scholar] [CrossRef]
- Carnevale, A.P.; Jayasundera, T.; Gulish, A. America’s Divided Recovery: College Haves and Have-Nots; Georgetown University Center on Education and the Workforce: Washington, DC, USA, 2016. [Google Scholar]
- Carnevale, A.P.; Rose, S.J. The undereducated American; Georgetown University Center on Education and the Workforce: Washington, DC, USA, 2011. [Google Scholar]
- Fletcher, J. Adolescent Depression and Adult Labor Market Outcomes. South Econ. J. 2013, 80, 26–49. [Google Scholar] [CrossRef]
- Baggio, S.; Iglesias, K.; Deline, S.; Studer, J.; Henchoz, Y.; Mohler-Kuo, M.; Gmel, G. Not in Education, Employment, or Training status among young Swiss men. Longitudinal associations with mental health and substance use. J. Adolesc. Health 2015, 56, 238–243. [Google Scholar] [CrossRef]
- Zajacova, A.; Lawrence, E.M. The Relationship Between Education and Health: Reducing Disparities Through a Contextual Approach. Annu. Rev. Publ. Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, M.; Normandeau, S. Share of Population by Education and Labour Force Status; OECD Statistics: Paris, France, 2019. [Google Scholar]
- Hale, D.R.; Bevilacqua, L.; Viner, R.M. Adolescent Health and Adult Education and Employment: A Systematic Review. Pediatrics 2015, 136, 128–140. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Maughan, B.; Collishaw, S.; Stringaris, A. Depression in childhood and adolescence. J. Can. Acad. Child. Adolesc. Psychiatry 2013, 22, 35–40. [Google Scholar]
- Gariepy, G.; Iyer, S. The Mental Health of Young Canadians Who Are Not Working or in School. Can. J. Psychiatry 2019, 64, 338–344. [Google Scholar] [CrossRef]
- Minh, A.; O’Campo, P.; Guhn, M.; McLeod, C.B. Out of the labour force and out of school: A population-representative study of youth labour force attachment and mental health. J. Youth Stud. 2020, 23, 853–868. [Google Scholar] [CrossRef]
- Rodwell, L.; Romaniuk, H.; Nilsen, W.; Carlin, J.B.; Lee, K.; Patton, G.C. Adolescent mental health and behavioural predictors of being NEET: A prospective study of young adults not in employment, education, or training. Psychol. Med. 2018, 48, 861–871. [Google Scholar] [CrossRef]
- Salmela-Aro, K.; Savolainen, H.; Holopainen, L. Depressive symptoms and school burnout during adolescence: Evidence from two cross-lagged longitudinal studies. J. Youth Adolesc. 2009, 38, 1316–1327. [Google Scholar] [CrossRef] [PubMed]
- Tuominen-Soini, H.; Salmela-Aro, K. Schoolwork engagement and burnout among Finnish high school students and young adults: Profiles, progressions, and educational outcomes. Dev. Psychol. 2014, 50, 649–662. [Google Scholar] [CrossRef] [PubMed]
- McLeod, J.D.; Fettes, D.L. Trajectories of Failure: The Educational Careers of Children with Mental Health Problems. AJS 2007, 113, 653–701. [Google Scholar] [CrossRef]
- Veldman, K.; Reijneveld, S.A.; Ortiz, J.A.; Verhulst, F.C.; Bültmann, U. Mental health trajectories from childhood to young adulthood affect the educational and employment status of young adults: Results from the TRAILS study. J. Epidemiol. Commun. Health 2015, 69, 588–593. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Lopez, J.A.; Kwong, A.S.F.; Washbrook, E.; Pearson, R.M.; Tilling, K.; Fazel, M.S.; Kidger, J.; Hammerton, G. Trajectories of depressive symptoms and adult educational and employment outcomes. Bjpsych Open 2020, 6, e6. [Google Scholar] [CrossRef]
- Walker, J. Stratification and Vocationalization in Canadian Higher Education. In Higher Education, Stratification, and Workforce Development: Competitive Advantage in Europe, the US, and Canada; Slaughter, S., Taylor, B.J., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 251–269. [Google Scholar]
- Weis, L. Positioning for Elite and Quasi-Elite Colleges and Universities in the United States: Parent and Student Strategies for “Maintaining Advantage” in New Economic and Postsecondary Context. In Higher Education, Stratification, and Workforce Development: Competitive Advantage in Europe, the US, and Canada; Slaughter, S., Taylor, B.J., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 271–288. [Google Scholar]
- Frenette, M.; Frank, K. Are Canadian Jobs More or Less Skilled than American Jobs? Analytical Studies Branch Research Paper Series; Social Analysis and Modelling Division, Statistics Canada: Ottawa, ON, Canada, 2018.
- Davies, S.; Zarifa, D. The stratification of universities: Structural inequality in Canada and the United States. Res. Soc. Strat. Mobil. 2012, 30, 143–158. [Google Scholar] [CrossRef]
- Belley, P.; Frenette, M.; Lochner, L. Post-secondary attendance by parental income in the US and Canada: Do financial aid policies explain the differences? Can. J. Econ./Rev. Can. d’Écon. 2014, 47, 664–696. [Google Scholar]
- Statistics Canada. National Longitudinal Survey of Children and Youth, Cycles 4-8—Longitudinal Cohort. In Using University of British Columbia Inter-University Research Data Centres; Statistics Canada: Ottawa, ON, Canada, 2000–2009. [Google Scholar]
- Bureau of Labor Statistics. U.S. Department of Labor, National Institute for Child Health and Human Development. In Children of the NLSY79, 1979–2014; The Center for Human Resource Research TOSU: Columbus, OH, USA, 2017. [Google Scholar]
- Minh, A.; Bültmann, U.; Reijneveld, S.A.; van Zon, S.K.; McLeod, C.B. Childhood Socioeconomic Status and Depressive Symptom Trajectories in the Transition to Adulthood in the United States and Canada. J. Adolesc. Health 2021, 68, 161–168. [Google Scholar] [CrossRef]
- Radloff, L.S. The Use of the Center for Epidemiologic Studies Depression Scale in Adolescents and Young-Adults. J. Youth Adolesc. 1991, 20, 149–166. [Google Scholar] [CrossRef]
- Poulin, C.; Hand, D.; Boudreau, B. Validity of a 12-item version of the CES-D used in the National Longitudinal Study of Children and Youth. Chronic Dis. Can. 2005, 26, 65–72. [Google Scholar]
- Gardner, P.L. Measuring attitudes to science: Unidimensionality and internal consistency revisited. Res. Sci. Educ. 1995, 25, 283–289. [Google Scholar] [CrossRef]
- Dall’Oglio, A.M.; Rossiello, B.; Coletti, M.F.; Caselli, M.C.; Ravà, L.; Di Ciommo, V.; Orzalesi, M.; Giannantoni, P.; Pasqualetti, P. Developmental evaluation at age 4: Validity of an Italian parental questionnaire. J. Paediatr. Child Health 2010, 46, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Berlin, K.S.; Parra, G.R.; Williams, N.A. An introduction to latent variable mixture modeling (part 2): Longitudinal latent class growth analysis and growth mixture models. J. Pediatr. Psychol. 2014, 39, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.J.; MacLehose, R.F. Estimating predicted probabilities from logistic regression: Different methods correspond to different target populations. Int. J. Epidemiol. 2014, 43, 962–970. [Google Scholar] [CrossRef]
- Statistics Canada. National Longitudinal Survey of Children and Youth (NLSCY); Statistics Canada: Ottawa, ON, Canada, 2007.
- Arim, R.; Frenette, M. Are Mental Health and Neurodevelopmental Conditions Barriers to Postsecondary Access? The Analytic Studies Branch Research Paper Series; Social Analysis and Modelling Division Statistics Canada: Ottawa, ON, Canada, 2019.
- Rebok, G.W.; Bradshaw, C.P.; Volk, H.E.; Mendelson, T.; Eaton, W.W.; Letourneau, E.J.; Kellam, S.G. Models of Stress and Adapting to Risk: A Life Course, Developmental Perspective. In Public Mental Health; Oxford University Press: New York, NY, USA, 2019. [Google Scholar]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout–depression overlap: A review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef]
- Giaconia, R.M.; Reinherz, H.Z.; Silverman, A.B.; Pakiz, B.; Frost, A.K.; Cohen, E. Traumas and Posttraumatic-Stress-Disorder in a Community Population of Older Adolescents. J. Am. Acad. Child. Psychiatry 1995, 34, 1369–1380. [Google Scholar] [CrossRef]
- Fletcher, J.M. Adolescent Depression and Educational Attainment: Results Using Sibling Fixed Effects. Health Econ. 2010, 19, 855–871. [Google Scholar] [CrossRef]
- Butterworth, P.; Leach, L.S.; McManus, S.; Stansfeld, S.A. Common mental disorders, unemployment and psychosocial job quality: Is a poor job better than no job at all? Psychol. Med. 2013, 43, 1763–1772. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Amick, B.C.; McLeod, C.B.; Bultmann, U. Labor markets and health: An integrated life course perspective. Scand. J. Work Environ. Health 2016, 42, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Eng, K.; Feeny, D. Comparing the health of low income and less well educated groups in the United States and Canada. Popul. Health Metr. 2007, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Frenette, M. Is Post-secondary Access More Equitable in Canadaor the United States? Analytical Studies Branch Research Paper Series; Statistics Canada: Ottawa, ON, Canada, 2005.
- The Conference Board of Canada. Return on investment in tertiary education. In Education and Skills Indicators; The Conference Board of Canada: Ottawa, ON, Canada, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Canada Total (n = 2348) | Working, Post-Secondary Degree | Working, High School Degree | Working, No Degree a | NEET a,b | In School | p | USA Total (n = 3961) | Working, Post-Secondary Degree | Working, High School Degree | Working, No Degree | NEET | In School | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 39.8 | 11.4 | 9.5 | 4.0 | 35.3 | 27.5 | 35.6 | 6.8 | 5.7 | 24.4 | |||||
| Depressive symptom trajectory | * | *** | ||||||||||||
| Low-stable | 63.5 | 70.4 | 55.3 | 55.3 | 61.3 | 77.5 | 87.2 | 75.2 | 60.9 | 70.7 | 78.4 | |||
| Mid-peak | 6.2 | 5.4 | 9.9 | 5.2 | 6.3 | 5.2 | 3.1 | 5.6 | 10.7 | 5.8 | 4.5 | |||
| Decreasing | 10.5 | 6.3 | 15.0 | 16.0 | 11.9 | 7.9 | 5.6 | 9.4 | 11.7 | 11.3 | 6.8 | |||
| Increasing | 19.7 | 17.9 | 19.8 | 23.5 | 20.4 | 9.3 | 4.1 | 9.8 | 16.7 | 12.3 | 10.2 | |||
| Gender | ** | ** | ||||||||||||
| Male | 49.6 | 48.4 | 62.7 | 62.0 | 32.5 | 45.4 | 51.5 | 45.4 | 52.7 | 61.6 | 44.7 | 47.8 | ||
| Female | 50.4 | 51.6 | 37.3 | 38.0 | 67.5 | 54.6 | 48.5 | 54.6 | 47.3 | 38.4 | 55.3 | 52.2 | ||
| Childhood income quartile | *** | *** | ||||||||||||
| Lowest | 13.6 | 11.5 | 22.0 | 22.9 | 20.5 | 9.9 | 18.3 | 8.5 | 20.3 | 42.1 | 30.0 | 14.9 | ||
| Second | 21.9 | 21.6 | 24.3 | 29.4 | 33.8 | 18.0 | 24.0 | 14.7 | 28.6 | 29.3 | 28.6 | 21.6 | ||
| Third | 27.0 | 27.7 | 28.8 | 19.7 | 23.8 | 28.1 | 28.7 | 34.3 | 27.8 | 19.2 | 23.2 | 26.2 | ||
| Highest | 37.5 | 39.2 | 24.9 | 28.0 | 21.9 | 43.9 | 29.0 | 42.5 | 23.3 | 9.4 | 18.2 | 37.3 | ||
| Parental education | *** | *** | ||||||||||||
| Less than high school | 6.1 | 5.6 | 8.5 | 10.3 | 13.8 | 3.8 | 8.6 | 2.7 | 7.5 | 26.3 | 16.2 | 4.6 | ||
| High school graduation | 10.9 | 13.9 | 14.1 | 12.2 | 3.0 | 7.1 | 43.4 | 32.2 | 51.3 | 54.9 | 45.9 | 35.9 | ||
| More than high school | 83.0 | 80.5 | 77.4 | 77.5 | 83.2 | 89.1 | 48.0 | 64.1 | 41.2 | 18.8 | 37.9 | 59.5 | ||
| Parental unemployment in childhood | * | *** | ||||||||||||
| No | 78.6 | 77.6 | 75.0 | 73.3 | 61.7 | 84.4 | 77.2 | 81.2 | 79.1 | 65.0 | 71.1 | 78.0 | ||
| Yes | 21.4 | 22.4 | 25.0 | 26.7 | 38.3 | 15.6 | 22.8 | 18.8 | 20.9 | 35.0 | 28.9 | 22.0 | ||
| Mother born in the US/Canada | ||||||||||||||
| No | 15.0 | 13.5 | 10.8 | 14.0 | 19.8 | 17.8 | 4.2 | 4.3 | 3.7 | 5.2 | 2.8 | 5.3 | ||
| Yes | 85.0 | 86.5 | 89.2 | 86.0 | 80.2 | 82.2 | 95.8 | 95.7 | 96.3 | 94.8 | 97.2 | 94.7 | ||
| Single parent status | * | *** | ||||||||||||
| No | 87.0 | 89.2 | 82.9 | 76.9 | 86.6 | 88.7 | 74.7 | 84.0 | 70.6 | 59.0 | 65.3 | 78.5 | ||
| Yes | 13.0 | 10.8 | 17.1 | 23.1 | 13.4 | 11.3 | 25.3 | 16.0 | 29.4 | 41.0 | 34.7 | 21.5 | ||
| Residence in rural area | * | |||||||||||||
| No | 83.2 | 80.7 | 80.7 | 81.9 | 77.8 | 87.8 | 76.2 | 76.5 | 74.4 | 78.2 | 75.4 | 78.6 | ||
| Yes | 16.8 | 19.3 | 19.3 | 18.1 | 22.2 | 12.2 | 23.8 | 23.5 | 25.6 | 21.8 | 24.6 | 21.4 | ||
| Model 1 a | Model 2 | |||||||
|---|---|---|---|---|---|---|---|---|
| Working, High School Degree | Working, No Degree | NEET b | In School | Working, High School Degree | Working, No Degree | NEET | In School | |
| Canada (n = 2348) | ||||||||
| Low-stable (ref) | 1.00 | 1.00 | ||||||
| Mid-peak | 2.18 (0.97–2.90) | 1.33 (0.59–3.01) | 0.62 (0.17–2.26) | 1.27 (0.66–2.45) | 2.74 (1.22–6.12) * | 1.61 (0.68–3.84) | 0.29 (0.06–1.41) | 1.23 (0.68–2.23) |
| Increasing | 3.39 (1.59–3.25) ** | 2.67 (1.28–5.57) * | 5.71 (2.00–16.34) * | 2.44 (1.47–4.06) * | 3.36 (1.74–6.47) ** | 2.94 (1.42–6.06) ** | 3.88 (1.44–10.44) * | 2.30 (1.34–3.93) * |
| Decreasing | 1.57 (0.96–2.54) | 1.76 (1.03–3.04) * | 1.92 (0.98–3.74) | 1.45 (1.00–2.13) | 1.60 (0.96–2.70) | 2.10 (1.22–3.61) * | 1.54 (0.78–3.03) | 1.37 (0.92–2.02) |
| USA (n = 3961) | ||||||||
| Low-stable (ref) | 1.00 | 1.00 | ||||||
| Mid-peak | 1.99 (1.20–3.32) * | 4.58 (2.45–8.56) ** | 2.15 (0.99–4.67) ** | 1.71 (0.96–3.05) | 2.14 (1.26–3.62) * | 4.88 (2.52–9.47) ** | 2.09 (0.95–4.62) | 1.97 (1.10–3.51) * |
| Increasing | 2.67 (1.73–4.12) ** | 5.62 (3.29–9.62) ** | 3.55 (1.98–6.47) ** | 2.88 (1.83–4.55) ** | 2.36 (1.49–3.73) ** | 4.68 (2.60–8.41) ** | 2.91 (1.56–5.42) ** | 2.65 (1.66–4.24) ** |
| Decreasing | 1.78 (1.17–2.69) * | 2.56 (1.45–4.49) ** | 2.21 (1.23–3.98) * | 1.43 (0.90–2.26) | 1.59 (1.01–2.49) * | 2.03 (1.06–3.87) * | 1.73 (0.91–3.28) | 1.32 (0.83–2.10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minh, A.; Bültmann, U.; Reijneveld, S.A.; van Zon, S.K.R.; McLeod, C.B. Depressive Symptom Trajectories and Early Adult Education and Employment: Comparing Longitudinal Cohorts in Canada and the United States. Int. J. Environ. Res. Public Health 2021, 18, 4279. https://doi.org/10.3390/ijerph18084279
Minh A, Bültmann U, Reijneveld SA, van Zon SKR, McLeod CB. Depressive Symptom Trajectories and Early Adult Education and Employment: Comparing Longitudinal Cohorts in Canada and the United States. International Journal of Environmental Research and Public Health. 2021; 18(8):4279. https://doi.org/10.3390/ijerph18084279
Chicago/Turabian StyleMinh, Anita, Ute Bültmann, Sijmen A. Reijneveld, Sander K. R. van Zon, and Christopher B. McLeod. 2021. "Depressive Symptom Trajectories and Early Adult Education and Employment: Comparing Longitudinal Cohorts in Canada and the United States" International Journal of Environmental Research and Public Health 18, no. 8: 4279. https://doi.org/10.3390/ijerph18084279
APA StyleMinh, A., Bültmann, U., Reijneveld, S. A., van Zon, S. K. R., & McLeod, C. B. (2021). Depressive Symptom Trajectories and Early Adult Education and Employment: Comparing Longitudinal Cohorts in Canada and the United States. International Journal of Environmental Research and Public Health, 18(8), 4279. https://doi.org/10.3390/ijerph18084279