
Assessment of Gait after Treatment of Tibial Nonunion with the Ilizarov Method

 , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Evaluation of Gait Parameters
2.2. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yin, P.; Ji, Q.; Li, T.; Li, J.; Li, Z.; Liu, J.; Wang, G.; Wang, S.; Zhang, L.; Mao, Z.; et al. A systematic review and meta-analysis of Ilizarov methods in the treatment of infected nonunion of tibia and femur. PLoS ONE 2015, 10, e0141973. [Google Scholar] [CrossRef]
- Peng, J.; Min, L.; Xiang, Z.; Huang, F.; Tu, C.; Zhang, H. Ilizarov bone transport combined with antibiotic cement spacer for infected tibial nonunion. Int. J. Clin. Exp. Med. 2015, 8, 10058–10065. [Google Scholar] [PubMed]
- Schoenleber, S.J.; Hutson, J.J. Treatment of hypertrophic distal tibia nonunion and early malunion with callus distraction. Foot Ankle Int. 2015, 36, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xue, F.; Jun Xiao, H. Ilizarov method in combination with autologous mesenchymal stem cells from iliac crest shows improved outcome in tibial non-union. Saudi J. Biol. Sci. 2018, 25, 819–825. [Google Scholar] [CrossRef]
- Meleppuram, J.J.; Ibrahim, S. Experience in fixation of infected non-union tibia by Ilizarov technique-a retrospective study of 42 cases. Rev. Bras. Ortop. 2017, 52, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Wani, N.B.; Syed, B. Ilizarov ring fixator in the management of infected non-unions of tibia. SICOT-J 2015, 1, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Abuomira, I.E.A.; Sala, F.; Elbatrawy, Y.; Lovisetti, G.; Alati, S.; Capitani, D. Distraction osteogenesis for tibial nonunion with bone loss using combined Ilizarov and Taylor spatial frames versus a conventional circular frame. Strateg. Trauma Limb Reconstr. 2016, 11, 153–159. [Google Scholar] [CrossRef]
- Baruah, R.K. Ilizarov methodology for infected nonunion of the tibia: Classic circular transfixion wire assembly vs. hybrid assembly. Indian J. Orthop. 2007, 41, 198–203. [Google Scholar] [CrossRef]
- Eralp, I.L.; Kocaoğlu, M.; Dikmen, G.; Azam, M.E.; Balci, H.I.; Bilen, F.E. Treatment of infected nonunion of the juxta-articular region of the distal tibia. Acta Orthop. Traumatol. Turc. 2016, 50, 139–146. [Google Scholar] [CrossRef]
- Hosny, G.; Shawky, M.S. The treatment of infected non-union of the tibia by compression-distraction techniques using the Ilizarov external fixator. Int. Orthop. 1998, 22, 298–302. [Google Scholar] [CrossRef]
- Khan, M.S.; Rashid, H.; Umer, M.; Qadir, I.; Hafeez, K.; Iqbal, A. Salvage of infected non-union of the tibia with an Ilizarov ring fixator. J. Orthop. Surg. 2015, 23, 52–55. [Google Scholar] [CrossRef]
- Madhusudhan, T.R.; Ramesh, B.; Manjunath, K.; Shah, H.M.; Sundaresh, D.C.; Krishnappa, N. Outcomes of Ilizarov ring fixation in recalcitrant infected tibial non-unions-a prospective study. J. Trauma Manag. Outcomes 2008, 2. [Google Scholar] [CrossRef] [PubMed]
- Magadum, M.P.; Basavaraj Yadav, C.M.; Phaneesha, M.S.; Ramesh, L.J. Acute compression and lengthening by the Ilizarov technique for infected nonunion of the tibia with large bone defects. J. Orthop. Surg. 2006, 14, 273–279. [Google Scholar] [CrossRef]
- Sahu, R.; Ranjan, R. Treatment of complex nonunion of the shaft of the tibia using Ilizarov technique and its functional outcome. Niger. Med. J. 2016, 57, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.W.; Galpin, R.D.; Hosseini, M.; MacLeod, M.D. Morbidity resulting from the treatment of tibial nonunion with the Ilizarov frame. Can. J. Surg. 2002, 45, 196–200. [Google Scholar] [PubMed]
- Shahid, M.; Hussain, A.; Bridgeman, P.; Bose, D. Clinical outcomes of the Ilizarov method after an infected tibialnon union. Arch. Trauma Res. 2013, 2, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wei, X.; Liu, P.; Fu, Y.H.; Wang, P.F.; Cong, Y.X.; Zhang, B.F.; Li, Z.; Lei, J.L.; Zhang, K.; et al. Quality of life and complications at the different stages of bone transport for treatment infected nonunion of the tibia. Medicine 2017, 96, e8569. [Google Scholar] [CrossRef]
- Yin, P.; Zhang, L.; Li, T.; Zhang, L.; Wang, G.; Li, J.; Liu, J.; Zhou, J.; Zhang, Q.; Tang, P. Infected nonunion of tibia and femur treated by bone transport. J. Orthop. Surg. Res. 2015, 10. [Google Scholar] [CrossRef]
- McNally, M.; Ferguson, J.; Kugan, R.; Stubbs, D. Ilizarov treatment protocols in the management of infected nonunion of the tibia. J. Orthop. Trauma 2017, 31, 47–54. [Google Scholar] [CrossRef]
- Aiona, M.; Do, K.P.; Emara, K.; Dorociak, R.; Pierce, R. Gait patterns in children with limb length discrepancy. J. Pediatr. Orthop. 2015, 35, 280–284. [Google Scholar] [CrossRef]
- Klöpfer-Krämer, I.; Brand, A.; Wackerle, H.; Müßig, J.; Kröger, I.; Augat, P. Gait analysis-available platforms for outcome assessment. Injury 2020, 51, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Goh, J.C.H.; Bose, K.; Khoo, B.C.C. Gait analysis study on patients with varusosteoarthrosis of the knee. Clin. Orthop. Relat. Res. 1993, 294, 223–231. [Google Scholar] [CrossRef]
- Koczewski, P.; Urban, F.; Jóźwiak, M. Analysis of some gait parameters at different stages of leg lengthening using the Ilizarov technique. Chir. Narzadow Ruchu Ortop. Pol. 2004, 69, 393–397. [Google Scholar] [PubMed]
- Wu, W.L.; Su, F.C.; Cheng, Y.M.; Huang, P.J.; Chou, Y.L.; Chou, C.K. Gait analysis after ankle arthrodesis. Gait Posture 2000, 11, 54–61. [Google Scholar] [CrossRef]
- Tenenbaum, S.; Coleman, S.C.; Brodsky, J.W. Improvement in gait following combined ankle and subtalar arthrodesis. J. Bone Jt. Surg. Am. Vol. 2014, 96, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Braito, M.; Dammerer, D.; Kaufmann, G.; Fischler, S.; Carollo, J.; Reinthaler, A.; Huber, D.; Biedermann, R. Are our expectations bigger than the results we achieve? A comparative study analysing potential advantages of ankle arthroplasty over arthrodesis. Int. Orthop. 2014, 38, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Katsenis, D.; Bhave, A.; Paley, D.; Herzenberg, J.E. Treatment of malunion and nonunion at the site of an ankle fusion with the Ilizarov apparatus. J. Bone Jt. Surg. Ser. A 2005, 87, 302–309. [Google Scholar] [CrossRef]
- Bhave, A.; Paley, D.; Herzenberg, J.E. Improvement in gait parameters after lengthening for the treatment of limb-length discrepancy. J. Bone Jt. Surg. Ser. A 1999, 81, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Song, K.M.; Halliday, S.E.; Little, D.G. The Effect of limb-length discrepancy on gait. J. Bone Jt. Surg. Ser. A 1997, 79, 1690–1698. [Google Scholar] [CrossRef]
- Suciu, O.; Onofrei, R.R.; Totorean, A.D.; Suciu, S.C.; Amaricai, E.C. Gait analysis and functional outcomes after twelve-week rehabilitation in patients with surgically treated ankle fractures. Gait Posture 2016, 49, 184–189. [Google Scholar] [CrossRef]
- Morasiewicz, M.; Koprowski, P.; Wrzosek, Z.; Dragan, S. Gait analysis in patients after lengthening and correction of tibia with Ilizarov technique. Physiother. Q. 2010, 18, 9–18. [Google Scholar] [CrossRef]
- Manjra, M.A.; Naude, J.; Birkholtz, F.; Glatt, V.; Tetsworth, K.; Hohmann, E. The relationship between gait and functional outcomes in patients treated with circular external fixation for malunitedtibial fractures. Gait Posture 2019, 68, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Fenwick, A.; Kröger, N.; Jovic, S.; Hölscher-Doht, S.; Meffert, R.; Jansen, H. Pedobarography shows no differences in gait after talar fractures. Technol. Health Care 2020, 28, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Genc, Y.; Gultekin, A.; Duymus, T.M.; Mutlu, S.; Mutlu, H.; Komur, B. Pedobarography in the assessment of postoperative calcaneal fracture pressure with gait. J. Foot Ankle Surg. 2016, 55, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, O.S.; Teo, S.H.; Lee, Y.S. Change in gait after high tibial osteotomy: A systematic review and meta-analysis. Gait Posture 2017, 57, 57–68. [Google Scholar] [CrossRef]
- Cichy, B.; Wilk, M. Gait analysis in osteoarthritis of the hip. Med. Sci. Monit. 2006, 12, 507–513. [Google Scholar]
- Saraph, V.; Zwick, E.B.; Steinwender, G.; Auner, C.; Schneider, F.; Linhart, W. Leg lengthening as part of gait improvement surgery in cerebral palsy: An evaluation using gait analysis. Gait Posture 2006, 23, 83–90. [Google Scholar] [CrossRef]
- Shrader, M.W.; Draganich, L.F.; Pottenger, L.A.; Piotrowski, G.A. Effects of knee pain relief in osteoarthritis on gait and stair-stepping. Clin. Orthop. Relat. Res. 2004, 421, 188–193. [Google Scholar] [CrossRef]
- Karol, L.A.; Haideri, N.F.; Halliday, S.E.; Smitherman, T.B.; Johnston, C.E. Gait analysis and muscle strength in children with congenital pseudarthrosis of the tibia: The effect of treatment. J. Pediatr. Orthop. 1998, 18, 381–386. [Google Scholar] [CrossRef]
- Morasiewicz, P.; Konieczny, G.; Dejnek, M.; Urbański, W.; Dragan, S.Ł.; Kulej, M.; Dragan, S.F.; Pawik, Ł. Assessment of the distribution of load on the lower limbs and balance before and after ankle arthrodesis with the Ilizarov method. Sci. Rep. 2018, 8, 15693. [Google Scholar] [CrossRef] [PubMed]
- Morasiewicz, P.; Konieczny, G.; Dejnek, M.; Morasiewicz, L.; Urbański, W.; Kulej, M.; Dragan, S.Ł.; Dragan, S.F.; Pawik, Ł. Pedobarographic analysis of body weight distribution on the lower limbs and balance after ankle arthrodesis with Ilizarov fixation and internal fixation. Biomed. Eng. Online 2018, 17, 174. [Google Scholar] [CrossRef] [PubMed]
- Morasiewicz, P.; Urbański, W.; Kulej, M.; Dragan, S.Ł.; Dragan, S.F.; Pawik, Ł. Balance and lower limb loads distribution after Ilizarovcorticotomy. Injury 2018, 49, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Morasiewicz, P.; Dragan, S.; Dragan, S.Ł.; Wrzosek, Z.; Pawik, Ł. Pedobarographic analysis of body weight distribution on the lower limbs and balance after Ilizarovcorticotomies. Clin. Biomech. 2016, 31, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.P.; Chapman, L.J.; Allen, J.J. The measurement of foot preference. Neuropsychologia 1987, 25, 579–584. [Google Scholar] [CrossRef]
- Coren, S. The lateral preference inventory for measurement of handedness, footedness, eyedness, and earedness: Norms for young adults. Bull. Psychon. Soc. 1993, 31, 1–3. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 32) | Patients after Surgery (n = 24) | p | |
|---|---|---|---|
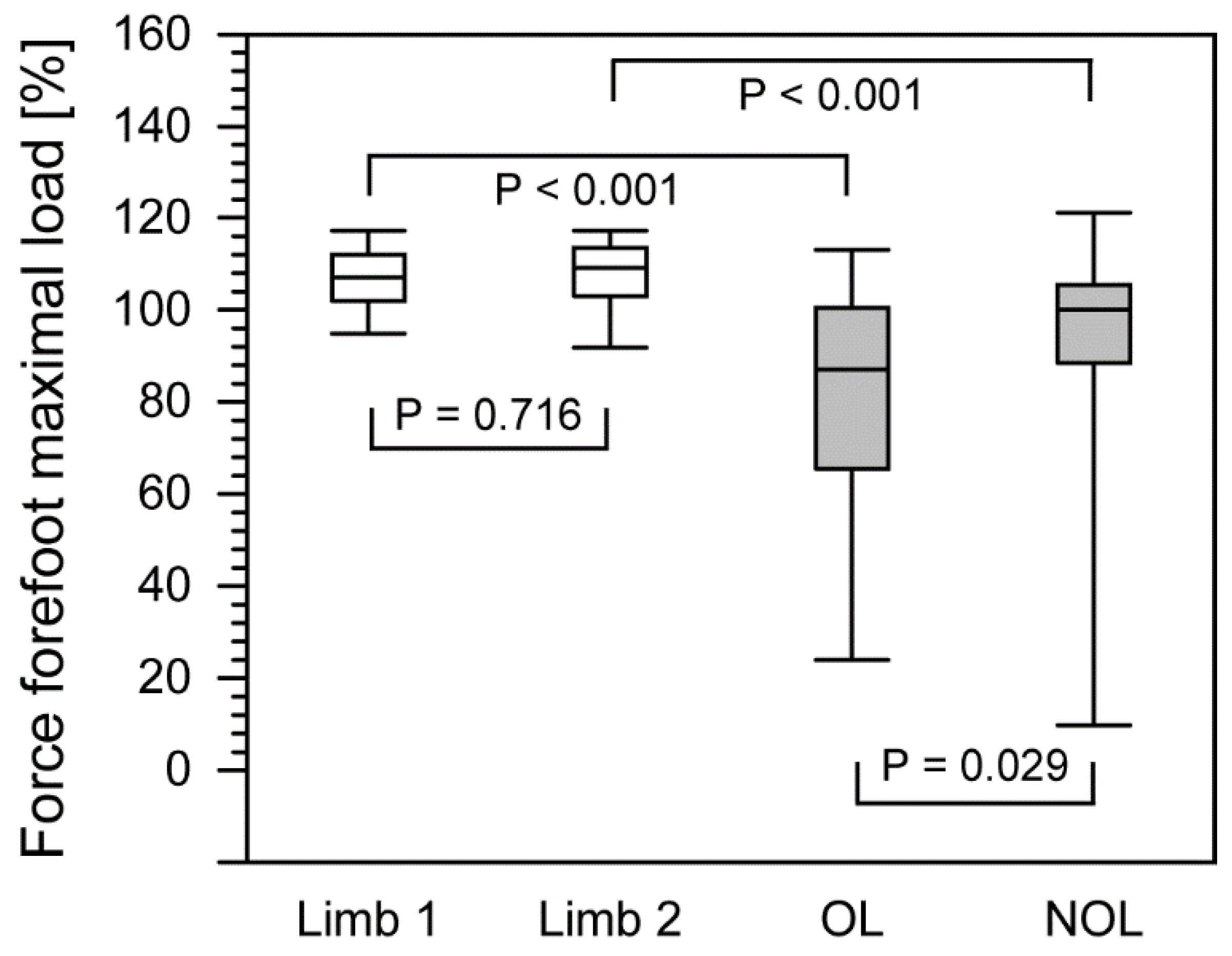
| Force Forefoot max load OL (%) | 107.0 (95.6–117.0) | 87.0 (26.0–110.5) | <0.001 |
| Force Forefoot max load NOL (%) | 108.5 (93.9–117.0) | 100.0 (19.7–118.0) | <0.001 |
| p | 0.716 | 0.029 | |
| Force Backfoot max load OL (%) | 79.5 (67.6–89.3) | 73.0 (35.5–87.7) | 0.021 |
| Force Backfoot max load NOL (%) | 77.5 (70.0–89.4) | 71.0 (57.2–82.7) | <0.001 |
| p | 0.396 | 0.256 | |
| Step length OP (cm) | 55.0 (47.2–69.1) | 47.5 (15.2–60.0) | <0.001 |
| Step length NOP (cm) | 56.5 (52.0–70.3) | 43.0 (12.5–68.7) | <0.001 |
| p | 0.309 | 0.628 | |
| Stance phase OL (%) | 63.9 (57.7–71.8) | 65.7 (60.6–77.2) | 0.047 |
| Stance phase NOL (%) | 65.2 (57.5–68.4) | 68.6 (60.5–78.4) | 0.006 |
| p | 0.151 | 0.140 | |
| Swing phase OL (%) | 35.9 (30.7–42.5) | 34.3 (22.8–39.4) | 0.023 |
| Swing phase NOL (%) | 24.9 (31.5–42.3) | 31.3 (21.6–39.5) | 0.002 |
| p | 0.655 | 0.130 | |
| Step time OL (s) | 0.585 (0.460–0.703) | 0.720 (0.490–0.907) | <0.001 |
| Step time NOL (s) | 0.580 (0.460–0.703) | 0.635 (0.495–0.795) | 0.010 |
| p | 0.660 | 0.045 |
| Gait Parameters | Control Group (n = 32) | Patients after Surgery (n = 24) | p |
|---|---|---|---|
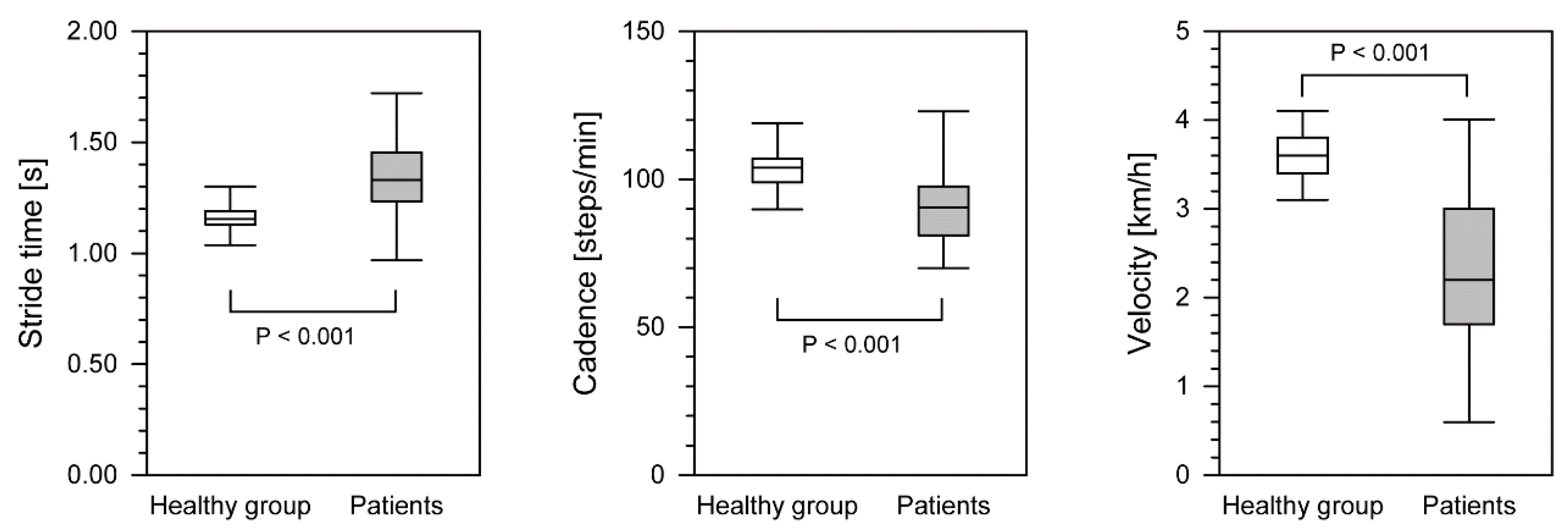
| Stride time (s) | 1.15 (1.06–1.27) | 1.33 (1.00–1.68) | <0.001 |
| Cadence steps/min | 104.0 (90.0–112.5) | 90.5 (71.0–119.7) | <0.001 |
| Velocity (km/h) | 3.60 (3.16–3.97) | 2.20 (0.75–3.87) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawik, Ł.; Fink-Lwow, F.; Pajchert Kozłowska, A.; Szelerski, Ł.; Żarek, S.; Górski, R.; Pawik, M.; Urbanski, W.; Reichert, P.; Morasiewicz, P. Assessment of Gait after Treatment of Tibial Nonunion with the Ilizarov Method. Int. J. Environ. Res. Public Health 2021, 18, 4217. https://doi.org/10.3390/ijerph18084217
Pawik Ł, Fink-Lwow F, Pajchert Kozłowska A, Szelerski Ł, Żarek S, Górski R, Pawik M, Urbanski W, Reichert P, Morasiewicz P. Assessment of Gait after Treatment of Tibial Nonunion with the Ilizarov Method. International Journal of Environmental Research and Public Health. 2021; 18(8):4217. https://doi.org/10.3390/ijerph18084217
Chicago/Turabian StylePawik, Łukasz, Felicja Fink-Lwow, Andżelika Pajchert Kozłowska, Łukasz Szelerski, Sławomir Żarek, Radosław Górski, Malwina Pawik, Wiktor Urbanski, Paweł Reichert, and Piotr Morasiewicz. 2021. "Assessment of Gait after Treatment of Tibial Nonunion with the Ilizarov Method" International Journal of Environmental Research and Public Health 18, no. 8: 4217. https://doi.org/10.3390/ijerph18084217
APA StylePawik, Ł., Fink-Lwow, F., Pajchert Kozłowska, A., Szelerski, Ł., Żarek, S., Górski, R., Pawik, M., Urbanski, W., Reichert, P., & Morasiewicz, P. (2021). Assessment of Gait after Treatment of Tibial Nonunion with the Ilizarov Method. International Journal of Environmental Research and Public Health, 18(8), 4217. https://doi.org/10.3390/ijerph18084217