
Association of Gender, Painkiller Use, and Experienced Pain with Pain-Related Fear and Anxiety among University Students According to the Fear of Pain Questionnaire-9

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
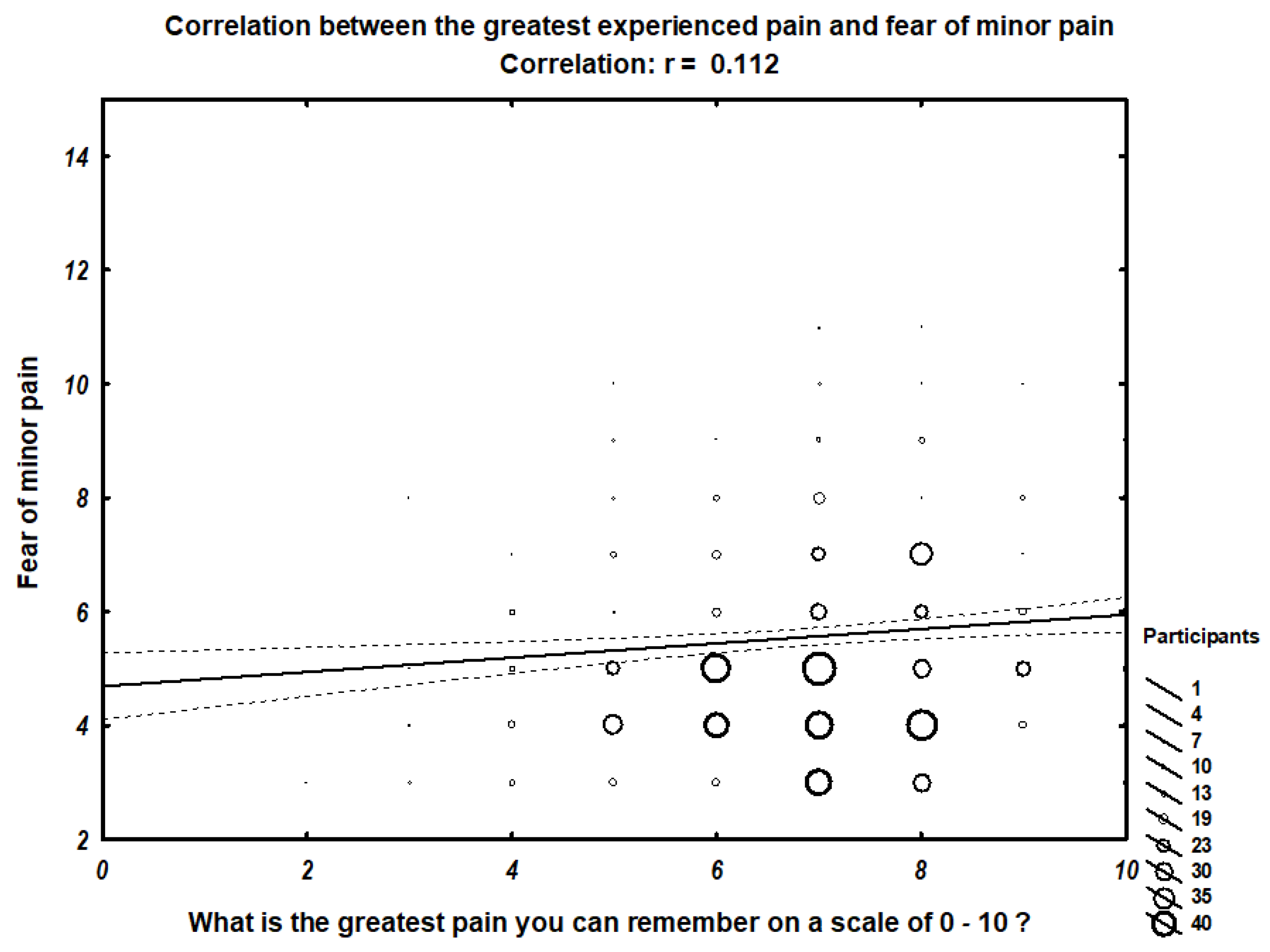
- fear of minor pain, which was calculated by summing the values of the items: 3, 5, 7 from the survey;
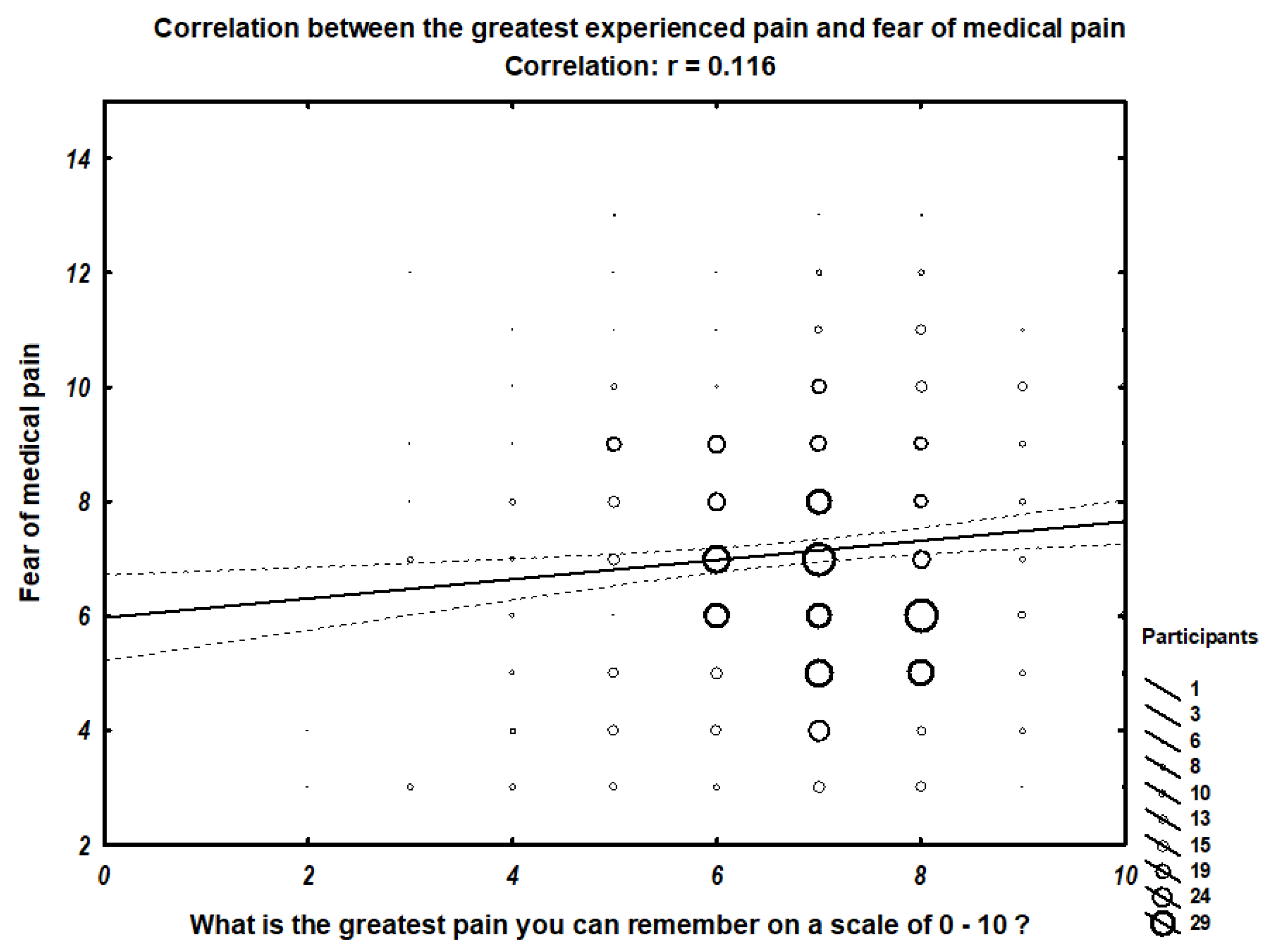
- fear of medical pain, which was calculated by summing the values of the items: 2, 4, 8 from the survey;
- fear of severe pain, which was calculated by summing the values of the items: 1, 6, 9 from the survey;
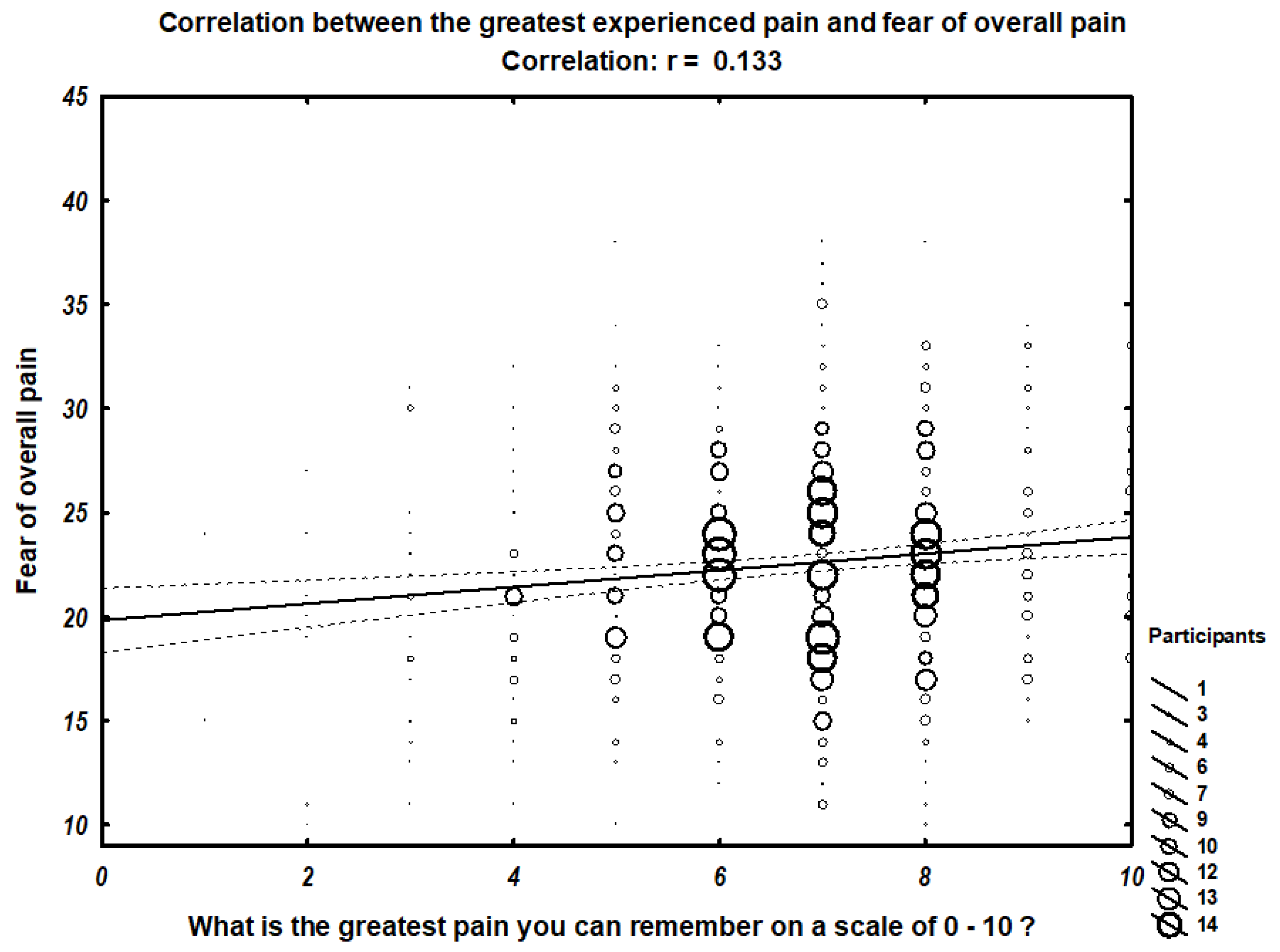
- overall fear of pain, which was calculated by summing values of all nine items from the survey (Appendix B).
3. Results
4. Discussion
4.1. Association between Gender and Fear of Pain
4.2. Association between Painkiller Use and Fear of Pain
4.3. Association between the Extent of Experienced Pain and Fear of Pain
4.4. Differences in Fear of Pain According to the Type and Year of Academic Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. FEAR of PAIN Questionnaire-9
| I FEAR the PAIN Associated with: | Not at All | A Little | A Fair Amount | Very Much | Extreme |
| 1. Breaking your arm | 1 | 2 | 3 | 4 | 5 |
| 2. Having a foot doctor remove a wart from your foot with a sharp instrument | 1 | 2 | 3 | 4 | 5 |
| 3. Getting a papercut on your finger | 1 | 2 | 3 | 4 | 5 |
| 4. Receiving an injection in your mouth | 1 | 2 | 3 | 4 | 5 |
| 5. Getting strong soap in both your eyes while bathing or showering | 1 | 2 | 3 | 4 | 5 |
| 6. Having someone slam a heavy car door on your hand | 1 | 2 | 3 | 4 | 5 |
| 7. Gulping a hot drink before it has cooled | 1 | 2 | 3 | 4 | 5 |
| 8. Receiving an injection in your hip/buttocks | 1 | 2 | 3 | 4 | 5 |
| 9. Falling down a flight of concrete stairs | 1 | 2 | 3 | 4 | 5 |
Appendix B
- (1)
- Score the Fear of Severe Pain subscale by summing values for the following items: 1, 6, 9
- (2)
- Score the Fear of Minor Pain subscale by summing values for the following items: 3, 5, 7
- (3)
- Score the Fear of Medical/Dental Pain subscale by summing values for the following items: 2, 4, 8
- (4)
- Calculate the Total Score by summing the three subscale values, or simply sum all 9 items.
References
- Institute of Medicine (US) Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Hasselström, J.; Liu-Palmgren, J.; Rasjö-Wrååk, G. Prevalence of pain in general practice. Eur. J. Pain 2002, 6, 375–385. [Google Scholar] [CrossRef]
- Romano, J.M.; Turner, J.A. Chronic pain and depression: Does the evidence support a relationship? Psychol. Bull. 1985, 97, 18–34. [Google Scholar] [CrossRef] [PubMed]
- Hursey, K.G.; Jacks, S.D. Fear of pain in recurrent headache sufferers. Headache J. Head Face Pain 1992, 32, 283–286. [Google Scholar] [CrossRef]
- McCracken, L.M.; Zayfert, C.; Gross, R.T. The Pain Anxiety Symptoms Scale: Development and validation of a scale to measure fear of pain. Pain 1992, 50, 67–73. [Google Scholar] [CrossRef]
- Geisser, M.E.; Robinson, M.E.; Keefe, F.J.; Weiner, M.L. Catastrophizing, depression and the sensory, affective and evaluative aspects of chronic pain. Pain 1994, 59, 79–83. [Google Scholar] [CrossRef]
- Hirsh, A.T.; George, S.Z.; Bialosky, J.E.; Robinson, M.E. Fear of pain, pain catastrophizing, and acute pain perception: Relative prediction and timing of assessment. J. Pain 2008, 9, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Van Hecke, O.; Torrance, N.; Smith, B.H. Chronic pain epidemiology and its clinical relevance. Br. J. Anaesth. 2013, 111, 13–18. [Google Scholar] [CrossRef]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef]
- Fayaz, A.; Croft, P.; Langford, R.M.; Donaldson, L.J.; Jones, G.T. Prevalence of chronic pain in the UK: A systematic review and meta-analysis of population studies. BMJ Open 2016, 6, e010364. [Google Scholar] [CrossRef]
- Arntz, A.; Dreessen, L.; De Jong, P. The influence of anxiety on pain: Attentional and attributional mediators. Pain 1994, 56, 307–314. [Google Scholar] [CrossRef]
- Turk, D.C.; Robinson, J.P.; Burwinkle, T. Prevalence of fear of pain and activity in patients with fibromyalgia syndrome. J. Pain 2004, 5, 483–490. [Google Scholar] [CrossRef]
- Parr, J.J.; Borsa, P.A.; Fillingim, R.B.; Tillman, M.D.; Manini, T.M.; Gregory, C.M.; George, S.Z. Pain-related fear and catastrophizing predict pain intensity and disability independently using an induced muscle injury model. J. Pain 2012, 13, 370–378. [Google Scholar]
- van Wijk, A.J.; Hoogstraten, J. Anxiety and pain during dental injections. J. Dent. 2009, 37, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Tran, U.E.; Kircher, J.; Jaggi, P.; Lai, H.; Hillier, T.; Ali, S. Medical students’ perspectives of their clinical comfort and curriculum for acute pain management. J. Pain Res. 2018, 11, 1479–1488. [Google Scholar]
- Guivarc’h, M.; Saliba-Serre, B.; Jacquot, B.; Le Coz, P.; Bukiet, F. Dental students’ attitudes towards management of pain and anxiety during a dental emergency: Educational issues. Int. Dent. J. 2017, 67, 384–390. [Google Scholar] [CrossRef] [PubMed]
- McNeil, D.W.; Kennedy, S.G.; Randall, C.L.; Addicks, S.H.; Wright, C.D.; Hursey, K.G.; Vaglienti, R. Fear of Pain Questionnaire-9: Brief assessment of pain-related fear and anxiety. Eur. J. Pain 2018, 22, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Okie, S. The evolving primary care physician. N. Engl. J. Med. 2012, 366, 1849–1853. [Google Scholar] [CrossRef]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L., 3rd. Sex, gender, and pain: A review of recent clinical and experimental findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef]
- Robinson, M.E.; Riley, J.L., 3rd; Brown, F.F.; Gremillion, H. Sex differences in response to cutaneous anesthesia: A double blind randomized study. Pain 1998, 77, 143–149. [Google Scholar] [CrossRef]
- Kindler, L.L.; Valencia, C.; Fillingim, R.B.; George, S.Z. Sex differences in experimental and clinical pain sensitivity for patients with shoulder pain. Eur. J. Pain 2011, 15, 118–123. [Google Scholar] [CrossRef]
- Bingefors, K.; Isacson, D. Epidemiology, co-morbidity, and impact on health-related quality of life of self-reported headache and musculoskeletal pain—A gender perspective. Eur. J. Pain 2004, 8, 435–450. [Google Scholar] [CrossRef]
- George, S.Z.; Wittmer, V.T.; Fillingim, R.B.; Robinson, M.E. Sex and pain-related psychological variables are associated with thermal pain sensitivity for patients with chronic low back pain. J. Pain 2007, 8, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Dannecker, E.A.; George, S.Z.; Otis, J.; Atchison, J.W.; Fillingim, R.B. Sex differences in the associations among psychological factors and pain report: A novel psychophysical study of patients with chronic low back pain. J. Pain 2005, 6, 463–470. [Google Scholar] [CrossRef] [PubMed]
- George, S.Z.; Fritz, J.M.; Childs, J.D.; Brennan, G.P. Sex differences in predictors of outcome in selected physical therapy interventions for acute low back pain. J. Orthop. Sports Phys. Ther. 2006, 36, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Riley, J.L., 3rd; Myers, C.D.; Papas, R.K.; Wise, E.A.; Waxenberg, L.B.; Fillingim, R.B. Gender role expectations of pain: Relationship to sex differences in pain. J. Pain 2001, 2, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Robinson, M.E.; Wise, E.A.; Gagnon, C.; Fillingim, R.B.; Price, D.D. Influences of gender role and anxiety on sex differences in temporal summation of pain. J. Pain 2004, 5, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Heima, M.; Heaton, L.J.; Ng, H.H.; Roccoforte, E.C. Dental fear among transgender individuals—A cross-sectional survey. Spec. Care Dent. 2017, 37, 212–222. [Google Scholar] [CrossRef]
- Samuelsen, P.J.; Nielsen, C.S.; Wilsgaard, T.; Stubhaug, A.; Svendsen, K.; Eggen, A.E. Pain sensitivity and analgesic use among 10,486 adults: The Tromsø study. BMC Pharmacol. Toxicol. 2017, 18, 45. [Google Scholar] [CrossRef]
- Fredheim, O.M.S.; Mahic, M.; Skurtveit, S.; Dale, O.; Romundstad, P.; Borchgrevink, P.C. Chronic pain and use of opioids: A population-based pharmacoepidemiological study from the Norwegian prescription database and the Nord-Trøndelag health study. Pain 2014, 155, 1213–1221. [Google Scholar] [CrossRef]
- Edwards, R.R. Individual differences in endogenous pain modulation as a risk factor for chronic pain. Neurology 2005, 65, 437–443. [Google Scholar] [CrossRef]
- Stoicea, N.; Russell, D.; Weidner, G.; Durda, M.; Joseph, N.C.; Yu, J.; Bergese, S.D. Opioid-induced hyperalgesia in chronic pain patients and the mitigating effects of gabapentin. Front. Pharmacol. 2015, 6, 104. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krebs, E.E.; Gravely, A.; Nugent, S.; Jensen, A.C.; DeRonne, B.; Goldsmith, E.S.; Kroenke, K.; Bair, M.J.; Noorbaloochi, S. Effect of Opioid vs. Nonopioid Medications on Pain-Related Function in Patients With Chronic Back Pain or Hip or Knee Osteoarthritis Pain: The SPACE Randomized Clinical Trial. JAMA 2018, 319, 872–882. [Google Scholar] [CrossRef] [PubMed]
- Nayyer, N.V.; Byers, J.; Marney, C. Identifying adults at risk of paracetamol toxicity in the acute dental setting: Development of a clinical algorithm. Br. Dent. J. 2014, 216, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.M.; Gooberman-Hill, R.; Hanks, G.W. Opioid analgesics for cancer pain: Symptom control for the living or comfort for the dying? A qualitative study to investigate the factors influencing the decision to accept morphine for pain caused by cancer. Ann. Oncol. 2008, 19, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Graczyk, M.; Borkowska, A.; Krajnik, M. Why patients are afraid of opioid analgesics: A study on opioid perception in patients with chronic pain. Pol. Arch. Intern. Med. 2017, 128, 89–97. [Google Scholar] [CrossRef]
- George, S.Z.; Hirsh, A.T. Psychologic influence on experimental pain sensitivity and clinical pain intensity for patients with shoulder pain. J. Pain 2009, 10, 293–299. [Google Scholar] [CrossRef]
- Keogh, E.; Book, K.; Thomas, J.; Giddins, G.; Eccleston, C. Predicting pain and disability in patients with hand fractures: Comparing pain anxiety, anxiety sensitivity and pain catastrophizing. Eur. J. Pain 2010, 14, 446–451. [Google Scholar] [CrossRef]
- Dimova, V.; Horn, C.; Parthum, A.; Kunz, M.; Schöfer, D.; Carbon, R.; Griessinger, N.; Sittl, R.; Lautenbacher, S. Does severe acute pain provoke lasting changes in attentional and emotional mechanisms of pain-related processing? A longitudinal study. Pain 2013, 154, 2737–2744. [Google Scholar] [CrossRef]
- Cohen, M.J.; Naliboff, B.D.; Schandler, S.L.; Heinrich, R.L. Signal detection and threshold measures to loud tones and radiant heat in chronic low back pain patients and cohort controls. Pain 1983, 16, 245–252. [Google Scholar] [CrossRef]
- Cohen, M.J.; Song, Z.K.; Schandler, S.L.; Ho, W.H.; Vulpe, M. Sensory detection and pain thresholds in spinal cord injury patients with and without dysesthetic pain, and in chronic low back pain patients. Somatosens. Mot. Res. 1996, 13, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Dar, R.; Ariely, D.; Frenk, H. The effect of past-injury on pain threshold and tolerance. Pain 1995, 60, 189–193. [Google Scholar] [CrossRef]
- Hapidou, E.G.; De Catanzaro, D. Responsiveness to laboratory pain in women as a function of age and childbirth pain experience. Pain 1992, 48, 177–181. [Google Scholar] [CrossRef]
- Naliboff, B.D.; Cohen, M.J.; Schandler, S.L.; Heinrich, R.L. Signal detection and threshold measures for chronic back pain patients, chronic illness patients, and cohort controls to radiant heat stimuli. J. Abnorm. Psychol. 1981, 90, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.L.; Schmidt, A.J. Differences in pain perception and sensory discrimination between chronic low back pain patients and healthy controls. J. Psychosom. Res. 1992, 36, 47–53. [Google Scholar] [CrossRef]
- Kleinböhl, D.; Hölzl, R.; Möltner, A.; Rommel, C.; Weber, C.; Osswald, P.M. Psychophysical measures of sensitization to tonic heat discriminate chronic pain patients. Pain 1999, 81, 35–43. [Google Scholar] [CrossRef]
- O’Neill, S.; Manniche, C.; Graven-Nielsen, T.; Arendt-Nielsen, L. Generalized deep-tissue hyperalgesia in patients with chronic low-back pain. Eur. J. Pain 2007, 11, 415–420. [Google Scholar] [CrossRef]
- Smith, B.W.; Tooley, E.M.; Montague, E.Q.; Robinson, A.E.; Cosper, C.J.; Mullins, P.G. Habituation and sensitization to heat and cold pain in women with fibromyalgia and healthy controls. Pain 2008, 140, 420–428. [Google Scholar] [CrossRef]
- Hohmeister, J.; Demirakça, S.; Zohsel, K.; Flor, H.; Hermann, C. Responses to pain in school-aged children with experience in a neonatal intensive care unit: Cognitive aspects and maternal influences. Eur. J. Pain 2009, 13, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Hagenaars, M.A.; Fisch, I.; van Minnen, A. The effect of trauma onset and frequency on PTSD-associated symptoms. J. Affect. Disord. 2011, 132, 192–199. [Google Scholar] [CrossRef]
- Goubert, L.; Crombez, G.; Van Damme, S. The role of neuroticism, pain catastrophizing and pain-related fear in vigilance to pain: A structural equations approach. Pain 2004, 107, 234–241. [Google Scholar] [CrossRef]
- Vangronsveld, K.L.H.; Peters, M.; Goossens, M.; Vlaeyen, J. The influence of fear of movement and pain catastrophizing on daily pain and disability in individuals with acute whiplash injury: A daily diary study. Pain 2008, 139, 449–457. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef]
- Carleton, R.N.; Asmundson, G.J.G.; Korol, S.L.; LeBouthillier, D.M.; Hozempa, K.; Katz, J.D.; Vlaeyen, J.W.S.; Crombez, G. Evaluating the efficacy of an attention modification program for patients with fibromyalgia: A randomized controlled trial. Pain 2020, 161, 584–594. [Google Scholar] [CrossRef]
- Friesen, L.N.; Hadjistavropoulos, H.D.; Schneider, L.H.; Alberts, N.M.; Titov, N.; Dear, B.F. Examination of an Internet-Delivered Cognitive Behavioural Pain Management Course for Adults with Fibromyalgia: A Randomized Controlled Trial. Pain 2017, 158, 593–604. [Google Scholar] [CrossRef]
- Van Oosterwijck, J.; Meeus, M.; Paul, L.; De Schryver, M.; Pascal, A.; Lambrecht, L.; Nijs, J. Pain physiology education improves health status and endogenous pain inhibition in fibromyalgia: A double-blind randomized controlled trial. Clin. J. Pain 2013, 29, 873–882. [Google Scholar] [CrossRef]
- Simister, H.D.; Tkachuk, G.A.; Shay, B.L.; Vincent, N.; Pear, J.J.; Skrabek, R.Q. Randomized Controlled Trial of Online Acceptance and Commitment Therapy for Fibromyalgia. J. Pain 2018, 19, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Amer-Cuenca, J.J.; Pecos-Martín, D.; Martínez-Merinero, P.; Lluch Girbés, E.; Nijs, J.; Meeus, M.; Ferrer Peña, R.; Fernández-Carnero, J. How Much Is Needed? Comparison of the Effectiveness of Different Pain Education Dosages in Patients with Fibromyalgia. Pain Med. 2020, 21, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Luque-Suarez, A. Intervention Therapies to Reduce Pain-Related Fear in Fibromyalgia Syndrome: A Systematic Review of Randomized Clinical Trials. Pain Med. 2021, 22, 481–498. [Google Scholar] [CrossRef] [PubMed]
- Trenado, C.; Pedroarena-Leal, N.; Cif, L.; Nitsche, M.; Ruge, D. Neural Oscillatory Correlates for Conditioning and Extinction of Fear. Biomedicines 2018, 6, 49. [Google Scholar] [CrossRef]
- Deyo, R.A.; Dworkin, S.F.; Amtmann, D.; Andersson, G.; Borenstein, D.; Carragee, E.; Carrino, J.; Chou, R.; Cook, K.; Delitto, A.; et al. Report of the NIH Task Force on research standards for chronic low back pain. Phys. Ther. 2015, 95, e1–e18. [Google Scholar] [CrossRef] [PubMed]
- Tick, H.; Nielsen, A.; Pelletier, K.R.; Bonakdar, R.; Simmons, S.; Glick, R.; Ratner, E.; Lemmon, R.L.; Wayne, P.; Zador, V. Pain Task Force of the Academic Consortium for Integrative Medicine and Health. Evidence-Based Nonpharmacologic Strategies for Comprehensive Pain Care: The Consortium Pain Task Force White Paper. Explore 2018, 14, 177–211. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographics’ Features | Number of Patients (N = 717) |
|---|---|
| Gender n, (%) | |
| Female | 547 (76.3) |
| Male | 162 (22.6) |
| Prefer not to say | 7 (1) |
| Living n, (%) | |
| Village | 196 (27.3) |
| City less than 50,000 inhabitants | 185 (25.7) |
| City less than 150,000 inhabitants | 89 (12.4) |
| City more than 150,000 inhabitants | 248 (34.6) |
| Type of study n, (%) | |
| Medicine | 412 (57.5) |
| Stomatology | 71 (10) |
| Public Health | 234 (32.5) |
| Year of study n, (%) | |
| 1 | 173 (24.1) |
| 2 | 142 (19.8) |
| 3 | 156 (21.8) |
| 4 | 131 (18.3) |
| 5 | 67 (9.3) |
| 6 | 48 (6.7) |
| Greatest pain you can remember on a scale of 0–10 n, (%) | |
| 0 | 2 (0.3) |
| 1 | 2 (0.3) |
| 2 | 8 (1.1) |
| 3 | 23 (3.2) |
| 4 | 41 (5.7) |
| 5 | 84 (11.7) |
| 6 | 117 (16.3) |
| 7 | 177 (24.7) |
| 8 | 146 (20.4) |
| 9 | 58 (8.1) |
| 10 | 58 (8.1) |
| Suffering from chronic illness n, (%) | |
| Yes | 112 (15.6) |
| No | 605 (84.4) |
| Mental illness present or in past n, (%) | |
| Yes | 161 (22.5) |
| No | 556 (77.5) |
| Hospitalization in the past n, (%) | |
| Yes | 422 (58.9) |
| No | 295 (41.1) |
| Use of painkillers n, (%) | |
| Hardly ever | 301 (42) |
| Once a month | 301 (42) |
| Once a week | 101 (14.1) |
| Once a day | 14 (1.9) |
| Fear of: Median (Interquartile range) | Study population (N = 717) |
| Breaking arm | 3 (2–4) |
| Having a foot doctor remove a wart from a foot with a sharp instrument | 3 (2–4) |
| Getting a papercut on a finger | 1 (1–2) |
| Receiving an injection in mouth | 2 (1–3) |
| Getting strong soap in both eyes while bathing or showering | 1 (1–2) |
| Having someone slam a heavy car door on a hand | 4 (3–4) |
| Gulping a hot drink before it has cooled | 2 (1–3) |
| Receiving an injection in hip/buttocks | 2 (1–3) |
| Falling down a flight of concrete stairs | 3 (2–4) |
| Minor pain 3 + 5 + 7 | 5 (4–7) |
| Medical pain 2 + 4 + 8 | 7 (5–9) |
| Severe pain 1 + 6 + 9 | 10 (8–12) |
| Demographics’ Features | Study Population (N = 717) Median (Interquartile Range) | p-Value |
|---|---|---|
| Gender | 0.87 | |
| Female | 5 (4–7) | |
| Male | 5 (4–7) | |
| Living | 0.20 | |
| Village | 5 (4–7) | |
| City less than 50,000 inhabitants | 5 (4–7) | |
| City less than 150,000 inhabitants | 5 (4–6) | |
| City more than 150,000 inhabitants | 5 (4–7) | |
| Type of study | 0.003 | |
| Medicine | 5 (4–6) | |
| Stomatology | 5 (4–7) | |
| Public Health | 5 (4–7) | |
| Year of study | 0.44 | |
| 1 | 5 (4–7) | |
| 2 | 5 (4–7) | |
| 3 | 5 (4–7) | |
| 4 | 5 (4–7) | |
| 5 | 5 (4–7) | |
| 6 | 5 (4–6) | |
| Greatest pain you can remember on a scale of 0–10 | 0.19 | |
| 0 | 7 (4–10) | |
| 1 | 6.5 (4–9) | |
| 2 | 4 (3–6) | |
| 3 | 5 (3–7) | |
| 4 | 5 (4–6) | |
| 5 | 5 (4–7) | |
| 6 | 5 (4–6) | |
| 7 | 5 (4–7) | |
| 8 | 5 (4–7) | |
| 9 | 5 (5–7) | |
| 10 | 6 (4–8) | |
| Suffering from chronic illness | 0.72 | |
| Yes | 5 (4–7) | |
| No | 5 (4–7) | |
| Mental illness present or in past | 0.47 | |
| Yes | 5 (4–7) | |
| No | 5 (4–7) | |
| Hospitalization in the past | 0.14 | |
| Yes | 5 (4–7) | |
| No | 5 (4–7) | |
| Use of painkillers | 0.003 | |
| Hardly ever | 5 (4–6) | |
| Once a month | 5 (4–7) | |
| Once a week | 6 (5–7) | |
| Once a day | 6.5 (5–8) |
| Demographics’ Features | Study Population (N = 717) Median (Interquartile Range) | p-Value |
|---|---|---|
| Gender | 0.002 | |
| Female | 7 (5–9) | |
| Male | 6 (5–8) | |
| Living | 0.25 | |
| Village | 7 (5–9) | |
| City less than 50,000 inhabitants | 7 (5–9) | |
| City less than 150,000 inhabitants | 7 (5–8) | |
| City more than 150,000 inhabitants | 7 (5–9) | |
| Type of study | 0.003 | |
| Medicine | 7 (5–9) | |
| Stomatology | 7 (5–8) | |
| Public Health | 7 (6–10) | |
| Year of study | 0.008 | |
| 1 | 7 (5–9) | |
| 2 | 7 (6–9) | |
| 3 | 7 (5–9) | |
| 4 | 7 (5–9) | |
| 5 | 7 (5–8) | |
| 6 | 5 (4–7.5) | |
| Greatest pain you can remember on a scale of 0–10 | 0.05 | |
| 0 | 7 (5–9) | |
| 1 | 7 (6–8) | |
| 2 | 4 (3–5.5) | |
| 3 | 7 (3–8) | |
| 4 | 6 (4–8) | |
| 5 | 7.5 (5–9) | |
| 6 | 7 (6–8) | |
| 7 | 7 (5–9) | |
| 8 | 7 (5–9) | |
| 9 | 7 (5–10) | |
| 10 | 7.5 (5–10) | |
| Suffering from chronic illness | 0.77 | |
| Yes | 7 (5–9) | |
| No | 7 (5–9) | |
| Mental illness present or in past | 0.24 | |
| Yes | 7 (5–9) | |
| No | 7 (5–9) | |
| Hospitalization in the past | 0.66 | |
| Yes | 7 (5–9) | |
| No | 7 (5–9) | |
| Use of painkillers | 0.004 | |
| Hardly ever | 6 (5–8) | |
| Once a month | 7 (5–9) | |
| Once a week | 7 (5–9) | |
| Once a day | 8.5 (6–10) |
| Demographics’ Features | Study Population (N = 717) Median (Interquartile Range) | p-Value |
|---|---|---|
| Gender | 0.0007 | |
| Female | 10 (8–12) | |
| Male | 10 (8–11) | |
| Living | 0.92 | |
| Village | 10 (8–12) | |
| City less than 50,000 inhabitants | 10 (8–12) | |
| City less than 150,000 inhabitants | 10 (8–12) | |
| City more than 150,000 inhibitants | 10 (8–12) | |
| Type of study | 0.28 | |
| Medicine | 10 (8–12) | |
| Stomatology | 10 (9–12) | |
| Public Health | 10 (8–12) | |
| Year of study | 0.61 | |
| 1 | 10 (8–12) | |
| 2 | 10 (8–12) | |
| 3 | 10 (8–11.5) | |
| 4 | 10 (8–12) | |
| 5 | 10 (8–12) | |
| 6 | 9 (8–11.5) | |
| Greatest pain you can remember on a scale of 0–10 | 0.07 | |
| 0 | 8 (6–10) | |
| 1 | 6 (5–7) | |
| 2 | 9.5 (5–12) | |
| 3 | 9 (7–10) | |
| 4 | 9 (8–11) | |
| 5 | 10 (8–12) | |
| 6 | 11 (9–12) | |
| 7 | 10 (8–12) | |
| 8 | 10 (8–12) | |
| 9 | 10 (8–11) | |
| 10 | 10.5 (9–12) | |
| Suffering from chronic illness | 0.35 | |
| Yes | 10 (8–12) | |
| No | 10 (8–12) | |
| Mental illness present or in past | 0.39 | |
| Yes | 10 (8–12) | |
| No | 10 (8–12) | |
| Hospitalization in the past | 0.66 | |
| Yes | 10 (8–12) | |
| No | 10 (8–12) | |
| Use of painkillers | 0.17 | |
| Hardly ever | 10 (8–12) | |
| Once a month | 10 (8–12) | |
| Once a week | 10 (9–12) | |
| Once a day | 11.5 (9–12) |
| Demographics’ Features | Study Population (N = 717) Median (Interquartile Range) | p-Value |
|---|---|---|
| Gender | 0.003 | |
| Female | 23 (19–27) | |
| Male | 21 (17–25) | |
| Living | 0.20 | |
| Village | 23 (19.5–27) | |
| City less than 50,000 inhabitants | 23 (18–26) | |
| City less than 150,000 inhabitants | 21 (18–25) | |
| City more than 150,000 inhabitants | 22 (18–26) | |
| Type of study | 0.06 | |
| Medicine | 22 (18–26) | |
| Stomatology | 22 (20–25) | |
| Public Health | 23 (19–27) | |
| Year of study | 0.07 | |
| 1 | 23 (19–27) | |
| 2 | 23 (19–27) | |
| 3 | 22 (18–25.5) | |
| 4 | 23 (19–27) | |
| 5 | 23 (18–26) | |
| 6 | 21 (17–24) | |
| Greatest pain you can remember on a scale of 0–10 | 0.04 | |
| 0 | 22 (19–25) | |
| 1 | 19.5 (15–24) | |
| 2 | 19.5 (11–22.5) | |
| 3 | 21 (15–24) | |
| 4 | 21 (17–23) | |
| 5 | 23 (19–27) | |
| 6 | 23 (20–25) | |
| 7 | 22 (18–26) | |
| 8 | 23 (19–26) | |
| 9 | 22.5 (19–26) | |
| 10 | 24.5 (20–29) | |
| Suffering from chronic illness | 0.62 | |
| Yes | 23 (19–26) | |
| No | 22 (19–26) | |
| Mental illness present or in past | 0.66 | |
| Yes | 22 (19–26) | |
| No | 22 (19–26) | |
| Hospitalization in the past | 0.73 | |
| Yes | 22 (19–26) | |
| No | 23 (18–27) | |
| Use of painkillers | 0.002 | |
| Hardly ever | 22 (18–25) | |
| Once a month | 23 (19–26) | |
| Once a week | 24 (20–28) | |
| Once a day | 26.5 (20–31) |
| Type of Study | Fear of Minor Pain Median (Interquartile Range) | p-Value | Fear of Severe Pain Median (Interquartile Range) | p-Value | Fear of Medical Pain Median (Interquartile Range) | p-Value | Overall Fear of Pain Median (Interquartile Range) | p-Value |
|---|---|---|---|---|---|---|---|---|
| Medicine | 5 (4–6) | 0.003 | 10 (8–12) | 0.28 | 7 (5–9) | 0.003 | 22 (18–26) | 0.06 |
| Stomatology | 5 (4–7) | 10 (9–12) | 7 (5–8) | 22 (20–25) | ||||
| Public Health | 5 (4–7) | 10 (8–12) | 7 (6–10) | 23 (19–27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piwowarczyk, P.; Kaczmarska, A.; Kutnik, P.; Hap, A.; Chajec, J.; Myśliwiec, U.; Czuczwar, M.; Borys, M. Association of Gender, Painkiller Use, and Experienced Pain with Pain-Related Fear and Anxiety among University Students According to the Fear of Pain Questionnaire-9. Int. J. Environ. Res. Public Health 2021, 18, 4098. https://doi.org/10.3390/ijerph18084098
Piwowarczyk P, Kaczmarska A, Kutnik P, Hap A, Chajec J, Myśliwiec U, Czuczwar M, Borys M. Association of Gender, Painkiller Use, and Experienced Pain with Pain-Related Fear and Anxiety among University Students According to the Fear of Pain Questionnaire-9. International Journal of Environmental Research and Public Health. 2021; 18(8):4098. https://doi.org/10.3390/ijerph18084098
Chicago/Turabian StylePiwowarczyk, Paweł, Agnieszka Kaczmarska, Paweł Kutnik, Aleksandra Hap, Joanna Chajec, Urszula Myśliwiec, Mirosław Czuczwar, and Michał Borys. 2021. "Association of Gender, Painkiller Use, and Experienced Pain with Pain-Related Fear and Anxiety among University Students According to the Fear of Pain Questionnaire-9" International Journal of Environmental Research and Public Health 18, no. 8: 4098. https://doi.org/10.3390/ijerph18084098
APA StylePiwowarczyk, P., Kaczmarska, A., Kutnik, P., Hap, A., Chajec, J., Myśliwiec, U., Czuczwar, M., & Borys, M. (2021). Association of Gender, Painkiller Use, and Experienced Pain with Pain-Related Fear and Anxiety among University Students According to the Fear of Pain Questionnaire-9. International Journal of Environmental Research and Public Health, 18(8), 4098. https://doi.org/10.3390/ijerph18084098