
The Effect of Regimen Frequency Simplification on Provider Order Generation: A Quasi-Experimental Study in a Korean Hospital


Abstract
1. Introduction
2. Materials and Methods
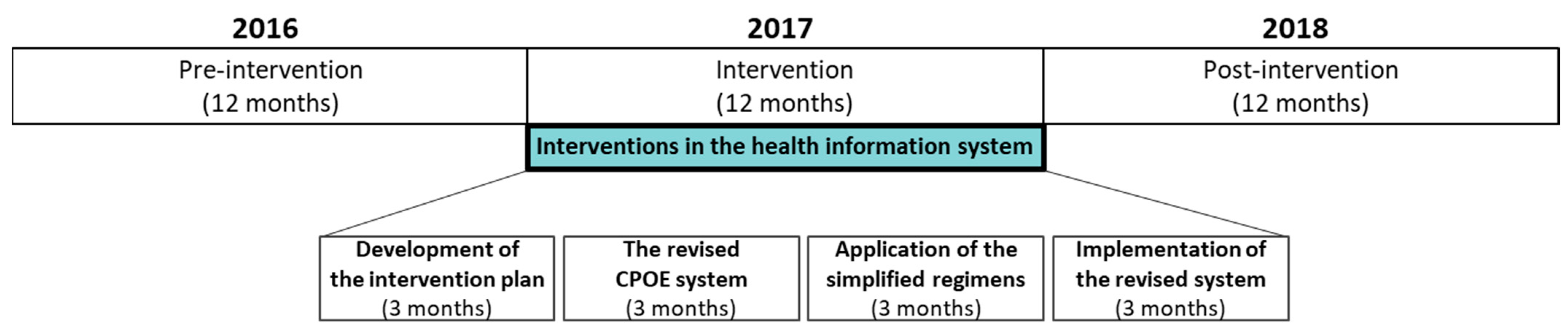
2.1. Study Design and Period
2.2. Study Site
2.3. Study Process
2.4. Interventions
2.4.1. Intervention 1: Standardization of the Default Regimens
2.4.2. Intervention 2: Prioritization of Prevalent Regimens
2.5. Outcomes
2.6. Statistical Analysis
2.7. Ethics Approval and Consent to Participate
3. Results
3.1. Characteristics of the Study Population
3.2. Prioritization of Prevalent Regimens by Dosing Frequency
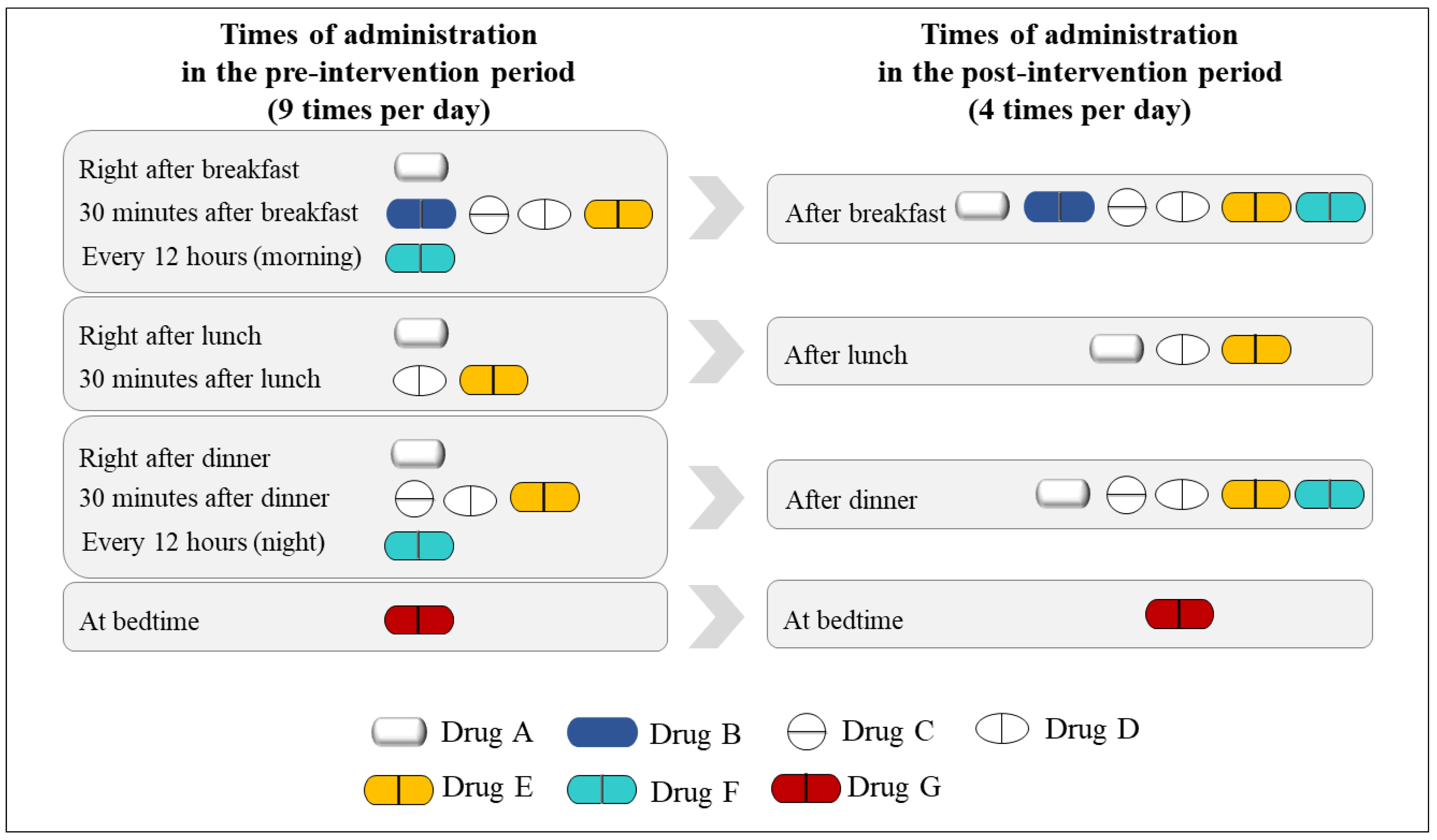
3.3. Dosing Frequency per Day
3.4. Proportion of Patients Taking Medications with High Frequencies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Simpson, S.H.; Eurich, D.T.; Majumdar, S.R.; Padwal, R.S.; Tsuyuki, R.T.; Varney, J.; Johnson, J.A. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 2006, 333, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Dent, E.; Visvanathan, R.; Wiese, M.D.; Johnell, K.; Chapman, I.; Bell, J.S. Polypharmacy and medication regimen complexity as factors associated with hospital discharge destination among older people: A prospective cohort study. Drugs Aging 2014, 31, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Vlasnik, J.J.; Aliotta, S.L.; DeLor, B. Medication adherence: Factors influencing compliance with prescribed medication plans. Case Manag. 2005, 16, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Benner, J.S.; Chapman, R.H.; Petrilla, A.A.; Tang, S.S.; Rosenberg, N.; Schwartz, J.S. Association between prescription burden and medication adherence in patients initiating antihypertensive and lipid-lowering therapy. Am. J. Health Syst. Pharm. 2009, 66, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Stange, D.; Kriston, L.; von Wolff, A.; Baehr, M.; Dartsch, D.C. Medication complexity, prescription behaviour and patient adherence at the interface between ambulatory and stationary medical care. Eur. J. Clin. Pharmacol. 2013, 69, 573–580. [Google Scholar] [CrossRef]
- Richter, A.; Anton, S.F.; Koch, P.; Dennett, S.L. The impact of reducing dose frequency on health outcomes. Clin. Ther. 2003, 25, 2307–2335. [Google Scholar] [CrossRef]
- Chen, E.Y.; Sluggett, J.K.; Ilomäki, J.; Hilmer, S.N.; Corlis, M.; Picton, L.J.; Dean, L.; Alderman, C.P.; Farinola, N.; Gailer, J.; et al. Development and validation of the Medication Regimen Simplification Guide for Residential Aged CarE (MRS GRACE). Clin. Interv. Aging 2018, 18, 975–986. [Google Scholar] [CrossRef]
- Sluggett, J.K.; Stasinopoulos, J.; Bell, J.S. Medication management by informal caregivers—Under-recognized and under-supported. Res. Social Adm. Pharm. 2018, 14, 215–217. [Google Scholar] [CrossRef]
- Maeil Business Newspaper. Available online: https://www.mk.co.kr/news/it/view/2017/09/649580/ (accessed on 10 February 2021).
- Wolf, M.S.; Davis, T.C.; Tilson, H.H.; Bass, P.F., III; Parker, R.M. Misunderstanding of prescription drug warning labels among patients with low literacy. Am. J. Health Syst. Pharm. 2006, 63, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.C.; Wolf, M.S.; Bass, P.F., III; Thompson, J.A.; Tilson, H.H.; Neuberger, M.; Parker, R.M. Literacy and misunderstanding prescription drug labels. Ann. Intern. Med. 2006, 145, 887–894. [Google Scholar] [CrossRef] [PubMed]
- List of Error-Prone Abbreviations. Available online: https://www.ismp.org/recommendations/error-prone-abbreviations-list/ (accessed on 7 February 2021).
- Hanlon, J.T.; Schmader, K.E.; Samsa, G.P.; Weinberger, M.; Uttech, K.M.; Lewis, I.K.; Cohen, H.J.; Feussner, J.R. A method for assessing drug therapy appropriateness. J. Clin. Epidemiol. 1992, 45, 1045–1051. [Google Scholar] [CrossRef]
- Kroenke, K.; Pinholt, E.M. Reducing polypharmacy in the elderly. A controlled trial of physician feedback. J. Am. Geriatr. Soc. 1990, 38, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Meyer, T.J.; Van Kooten, D.; Marsh, S.; Prochazka, A.V. Reduction of polypharmacy by feedback to clinicians. J. Gen. Intern. Med. 1991, 6, 133–136. [Google Scholar] [CrossRef]
- Jeetu, G.; Girish, T. Prescription Drug Labeling Medication Errors: A Big Deal for Pharmacists. J. Young Pharm. 2010, 2, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Tan Edwin, C.K.; Sluggett, J.K.; Johnell, K.; Onder, G.; Elseviers, M.; Morin, L.; Vetrano, D.L.; Wastresson, J.W.; Fastbom, J.; Taipale, H.; et al. Research Priorities for Optimizing Geriatric Pharmacotherapy: An International Consensus. J. Am. Med. Dir. Assoc. 2018, 19, 193–199. [Google Scholar] [CrossRef]
- Sluggett, J.K.; Chen Esa, Y.H.; Ilomäki, J.; Megan, C.; Hilmer, S.N.; Emden, J.V.; Ooi, C.E.; Nguyen, K.-H.; Comans, T.; Hogan, M. SImplification of Medications Prescribed to Long-tErm Care Residents (SIMPLER): Study Protocol for a Cluster Randomised Controlled Trial. Trials 2018, 19, 37–39. [Google Scholar] [CrossRef]
- Muir, A.J.; Sanders, L.L.; Wilkinson, W.E.; Schmader, K. Reducing medication regimen complexity: A controlled trial. J. Gen. Intern. Med. 2001, 16, 77–82. [Google Scholar] [CrossRef]
- Allen, C.M.; Becker, P.M.; McVey, L.J.; Saltz, C.; Feussner, J.R.; Cohen, H.J. A randomized, controlled clinical trial of a geriatric consultation team. Compliance with recommendations. JAMA 1986, 255, 2617–2621. [Google Scholar] [CrossRef]
- Hanlon, J.T.; Weinberger, M.; Samsa, G.P.; Schmader, K.E.; Uttech, K.M.; Lewis, I.K.; Cowper, P.A.; Landsman, P.B.; Cohen, H.J.; Feussner, J.R. A randomized, controlled trial of a clinical pharmacist intervention to improve inappropriate prescribing in elderly outpatients with polypharmacy. Am. J. Med. 1996, 100, 428–437. [Google Scholar] [CrossRef]
- Hamdy, R.C.; Moore, S.W.; Whalen, K.; Donnelly, J.P.; Compton, R.; Testerman, F.; Haulsee, P.; Hughes, J. Reducing polypharmacy in extended care. South. Med. J. 1995, 88, 534–538. [Google Scholar] [CrossRef]
- Archer, J.C. State of the science in health professional education: Effective feedback. Med. Educ. 2010, 44, 101–108. [Google Scholar] [CrossRef]
- The Pharmaceutical Journal-How to Give and Receive Constructive Feedback. Available online: https://www.pharmaceutical-journal.com/cpd-and-learning/learning-article/how-to-give-and-receive-constructive-feedback/20200756.article?firstPass=false#fn_8/ (accessed on 13 February 2021).
- Elliott, R.A.; O’Callaghan, C.J. Impact of Hospitalisation on the Complexity of Older Patients’ Medication Regimens and Potential for Regimen Simplification. J. Pharm. Pract. Res. 2011, 41, 21–25. [Google Scholar] [CrossRef]
- Pauly, A.; Wolr, C.; Mayr, A.; Lenz, B.; Kornhuber, J.; Friedland, K. Effect of a Multi-Dimensional and Inter-Sectoral Intervention on the Adherence of Psychiatric Patients. PLoS ONE 2015, 10, e0139302. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Hopkins, R.E.; Chen Esa, Y.H.; Ilomäki, J.; Corlis, M.; Emden, J.V.; Hogan, M.; Caporale, T.; Ooi, C.E.; Himer, S.N.; et al. Impact of Medication Regimen Simplification on Medication Administration Times and Health Outcomes in Residential Aged Care: 12 Month Follow Up of the SIMPLER Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1053. [Google Scholar] [CrossRef]
- Stange, D.; Kriston, L.; von-Wolff, A.; Baehr, M.; Dartsch, D.C. Reducing cardiovascular medication complexity in a German university hospital: Effects of a structured pharmaceutical management intervention on adherence. J. Manag. Care Pharm. 2013, 19, 396–407. [Google Scholar] [CrossRef] [PubMed]
- Schneider, P.J.; Pedersen, C.A.; Scheckelhoff, D.J. ASHP national survey of pharmacy practice in hospital settings: Dispensing and administration-2017. Am. J. Health Syst. Pharm. 2018, 75, 1203–1226. [Google Scholar] [CrossRef]
- Van Dort, B.A.; Zheng, W.Y.; Baysari, M.T. Prescriber perceptions of medication-related computerized decision support systems in hospitals: A synthesis of qualitative research. Int. J. Med. Inform. 2019, 129, 285–295. [Google Scholar] [CrossRef]
- Schiff, G.D.; Amato, M.G.; Eguale, T.; Boehne, J.J.; Wright, A.; Koppel, R.; Rashidee, A.H.; Elson, R.B.; Whitney, D.L.; Thach, T.T.; et al. Computerised physician order entry-related medication errors: Analysis of reported errors and vulnerability testing of current systems. BMJ Qual. Saf. 2015, 24, 264–271. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Changes | n | Examples |
|---|---|---|
| Right after meal → after meal | 123 | Azathioprine |
| 30 min after meal → after meal | 1261 | Amlodipine besylate |
| One tablet every eight hours → one tablet three times a day | 10 | Acetaminophen |
| One tablet every 12 h → one tablet twice a day | 48 | Cefuroxime axetil |
| One tablet every 24 h → one tablet once a day | 7 | Moxifloxacin |
| Characteristics | Pre-Intervention 1 n = 40,716 (%) | Post-Intervention 2 n = 44,328 (%) | p-Value |
|---|---|---|---|
| Sex | |||
| Female | 20,480 (50.3) | 22,541 (50.9) | 0.11 a |
| Male | 20,236 (49.7) | 21,787 (49.1) | |
| Age, mean ± SD (years) | 57.9 ± 16.9 | 58.6 ± 16.8 | <0.001 b |
| 18–65 years | 25,302 (62.1) | 27,403 (61.8) | 0.33 a |
| Over 65 years | 15,414 (37.9) | 16,925 (38.2) | |
| Length of stay, mean ± SD (days) | 10.8 ± 30.6 | 9.9 ± 25.8 | <0.001 b |
| Department at discharge | <0.001 a | ||
| Internal medicine | 13,565 (33.3) | 14,767 (33.3) | |
| Surgery | 9503 (23.3) | 10,644 (24.0) | |
| Obstetrics and gynecology | 3865 (9.5) | 4725 (10.7) | |
| Orthopedics | 3466 (8.5) | 3529 (8.0) | |
| Urology | 3061 (7.5) | 2928 (6.6) | |
| Neurology | 1576 (3.9) | 1607 (3.6) | |
| Neuropsychiatry | 935 (2.3) | 865 (2.0) | |
| Pediatrics | 72 (0.2) | 120 (0.3) | |
| Others | 4673 (11.5) | 5143 (11.6) |
| Dosing Frequency | Regimens | Pull-Down Options’ Order | ||
|---|---|---|---|---|
| Post | Pre | Rank Change | ||
| QD | 30 min after breakfast | 1 | 9 | 8↑ |
| Right after breakfast | 2 | 8 | 6↑ | |
| Before sleep | 3 | 36 | 33↑ | |
| BID | 30 min after breakfast and dinner | 1 | 8 | 7↑ |
| Right after breakfast and dinner | 2 | 6 | 4↑ | |
| 30 min after breakfast and before sleep | 3 | 14 | 11↑ | |
| TID | 30 min after each meal | 1 | 9 | 8↑ |
| Right after each meal | 2 | 7 | 5↑ | |
| Every 8 h | 3 | 14 | 11↑ | |
| QID | 30 min after each meal and before sleep | 1 | 6 | 5↑ |
| Right after each meal and before sleep | 2 | 5 | 3↑ | |
| Every 6 h | 3 | 10 | 7↑ | |
| Outcomes | Pre-Intervention 1 n = 40,716 (%) | Post-Intervention 2 n = 44,328 (%) | p-Value |
|---|---|---|---|
| Mean dosing frequency per day, count (SD) | 4.3 (2.2) | 3.5 (1.8) | <0.001 |
| Proportion of patients taking medications with high frequencies, n (%) | 16,619 (40.8) | 9196 (20.7) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; Shin, S.; Jeong, Y.M.; Lee, E.; Lee, E. The Effect of Regimen Frequency Simplification on Provider Order Generation: A Quasi-Experimental Study in a Korean Hospital. Int. J. Environ. Res. Public Health 2021, 18, 4086. https://doi.org/10.3390/ijerph18084086
Cho J, Shin S, Jeong YM, Lee E, Lee E. The Effect of Regimen Frequency Simplification on Provider Order Generation: A Quasi-Experimental Study in a Korean Hospital. International Journal of Environmental Research and Public Health. 2021; 18(8):4086. https://doi.org/10.3390/ijerph18084086
Chicago/Turabian StyleCho, Jungwon, Sangmi Shin, Young Mi Jeong, Eunsook Lee, and Euni Lee. 2021. "The Effect of Regimen Frequency Simplification on Provider Order Generation: A Quasi-Experimental Study in a Korean Hospital" International Journal of Environmental Research and Public Health 18, no. 8: 4086. https://doi.org/10.3390/ijerph18084086
APA StyleCho, J., Shin, S., Jeong, Y. M., Lee, E., & Lee, E. (2021). The Effect of Regimen Frequency Simplification on Provider Order Generation: A Quasi-Experimental Study in a Korean Hospital. International Journal of Environmental Research and Public Health, 18(8), 4086. https://doi.org/10.3390/ijerph18084086