
Child Marriage and Sexual Autonomy among Women in Sub-Saharan Africa: Evidence from 31 Demographic and Health Surveys

 , ,
, ,  , , ,
, , , 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Data Collection Procedure
2.3. Sampling Procedure and Size
2.4. Definition of Variables
2.4.1. Outcome Variable
2.4.2. Independent Variables
2.5. Statistical Analyses
2.6. Ethical Approval
3. Results
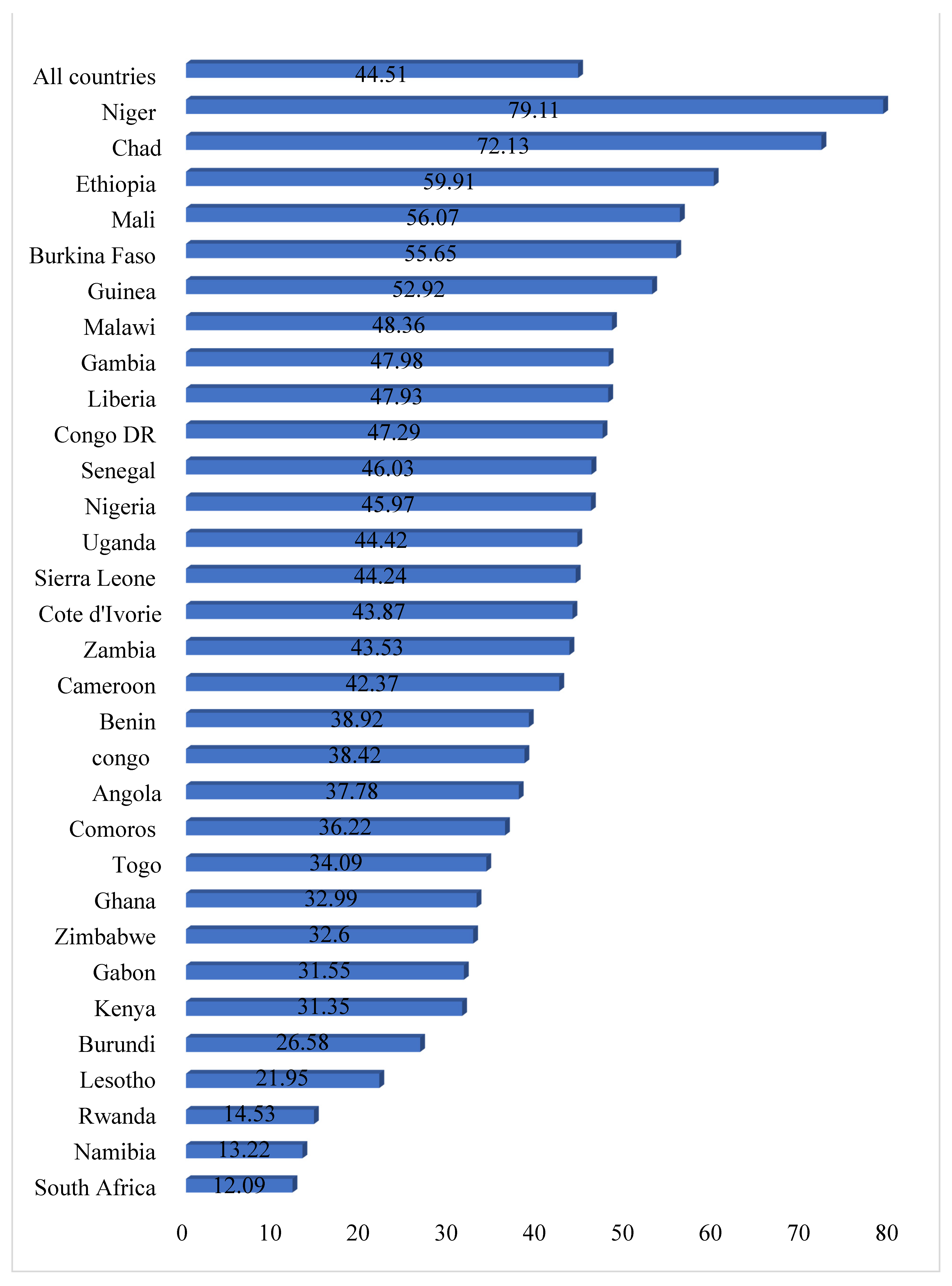
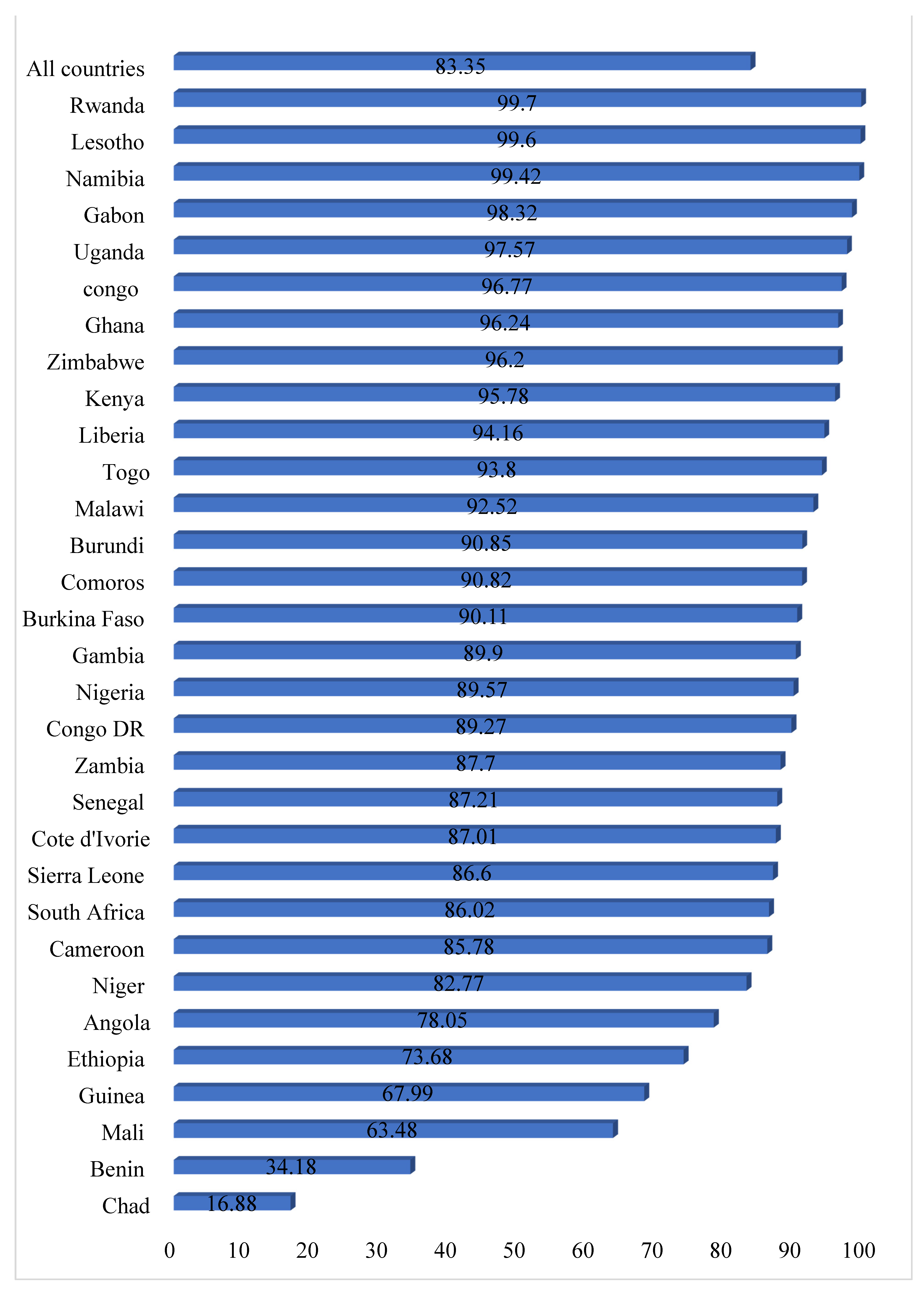
3.1. Prevalence of Child Marriage and Sexual Autonomy in Sub-Saharan Africa
3.2. Distribution of Sexual Autonomy across Age at First Marriage and Other Socio-Demographic Characteristics of Women
3.3. Association between Age at First Marriage and Sexual Autonomy in Sub-Saharan Africa
4. Discussion
4.1. Limitations
4.2. Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- UNICEF. Child Marriage–UNICEF DATA. 2020. Available online: https://data.unicef.org/topic/child-protection/child-marriage/ (accessed on 9 February 2021).
- De Groot, R.; Kuunyem, M.Y.; Palermo, T.; Osei-Akoto, I.; Adamba, C.; Darko, J.K.; Caparello, A. Child marriage and associated outcomes in northern Ghana: A cross-sectional study. BMC Public Health 2018, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sarfo, E.A.; Salifu Yendork, J.; Naidoo, A.V. Understanding Child Marriage in Ghana: The Constructions of Gender and Sexuality and Implications for Married Girls. Child. Care Pract. 2020, 1–14. [Google Scholar] [CrossRef]
- United Nations Children’s Fund, Ending Child Marriage: Progress and Prospects; UNICEF: New York, NY, USA, 2014.
- McCleary-Sills, J.; Hanmer, L.; Parsons, J.; Klugman, J. Child Marriage: A Critical Barrier to Girls’ Schooling and Gender Equality in Education. Rev. Faith Int. Aff. 2015, 13, 69–80. [Google Scholar] [CrossRef]
- Brown, E.N. Against Sexual Autonomy: Why Sex Law’s Lodestar Should Be Self-Possession. 2014. The Philosophical Principles Underpinning Rape Law Have Changed Over Time. What’s the Next Step in our Understanding of the Issue Website. Available online: https://www.libertarianism.org/columns/against-sexual-autonomy-why-sex-laws-lodestar-should-be-self-possession (accessed on 11 February 2021).
- UNICEF. Child Marriage: Latest Trends and Future Prospects; UNICEF: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Girls Not Brides. Ending Child Marriage in Africa: A brief by Girls Not. Brides. 2014. Available online: https://www.girlsnotbrides.org/wp-content/uploads/2015/02/Child-marriage-in-Africa-A-brief-by-Girls-Not-Brides.pdf (accessed on 12 February 2021).
- United Nations Children’s Fund. A Profile of Child Marriage in Africa; UNICEF: New York, NY, USA, 2015. [Google Scholar]
- NICEF. Child Marriage and Sexual and Reproductive Health and Rights. In The Global Partnership to End Child Marriage; UNICEF: New York, NY, USA, 2018; pp. 1–8. [Google Scholar]
- Lazarus, S.I.; Rush, M.; Dibiana, E.T.; Monks, C.P. Gendered penalties of divorce on remarriage in Nigeria: A qualitative study. J. Comp. Fam. Stud. 2017, 48, 351–366. [Google Scholar] [CrossRef]
- Delprato, M.; Akyeampong, K.; Sabates, R.; Hernandez-Fernandez, J. On the Impact of Early Marriage on Schooling Outcomes in Sub-Saharan Africa and South West Asia. Int. J. Educ. Dev. 2015, 44, 42–55. [Google Scholar] [CrossRef]
- Erulkar, A. Very early marriage, marital relations and intimate partner violence in Ethiopia. Int. Perspect. Sex. Reprod. Health 2013, 39, 6–13. [Google Scholar] [CrossRef]
- Montazeri, S.; Gharacheh, M.; Mohammadi, N.; Alaghband Rad, J.; Eftekhar Ardabili, H. Determinants of Early Marriage from Married Girls’ Perspectives in Iranian Setting: A Qualitative Study. J. Environ. Public Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Mathew, L.A. Right to sexual autonomy of children—implications of the UNCRC upon the Indian law on the age of consent. Int. J. Crime Justice Soc. Democr. 2019, 8, 121–134. [Google Scholar] [CrossRef]
- Hindi, M.J.; Fatusi, A.O. Adolescent Sexual and Reproductive Health in Developing Countries: An Overview of Trends and Interventions. Acad. Psychiatry 2010, 34, 381–385. [Google Scholar] [CrossRef]
- Yaya, S.; Odusina, E.K.; Bishwajit, G. Prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. BMC Int. Health Hum. Rights 2019, 19, 1–11. [Google Scholar] [CrossRef]
- Ahmed, S.; Creanga, A.A.; Gillespie, D.G.; Tsui, A.O. Economic status, education and empowerment: Implications for maternal health service utilization in developing countries. PLoS ONE 2010, 5, e11190. [Google Scholar] [CrossRef] [PubMed]
- Deb, S.; Kabir, A.; Kawsar, L.A. Women’s empowerment and regional variation of contraceptive norms in Bangladesh. Int. Q. Community Health Educ. 2010, 31, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Ung, M.; Boateng, G.O.; Armah, F.A.; Amoyaw, J.A.; Luginaah, I.; Kuuire, V. Negotiation for safer sex among married women in Cambodia: The role of women’s autonomy. J. Biosoc. Sci. 2014, 46, 90–106. [Google Scholar] [CrossRef] [PubMed]
- Viswan, S.P.; Ravindran, T.S.; Kandala, N.B.; Petzold, M.G.; Fonn, S. Sexual autonomy and contraceptive use among women in Nigeria: Findings from the demographic and health survey data. Int. J. Women’s Health 2017, 9, 581. [Google Scholar] [CrossRef]
- Ibrahim, S. A Binary Model of Broken Home: Parental Death-Divorce Hypothesis of Male Juvenile Delinquency in Nigeria and Ghana. In Contemporary Perspectives in Family Research; Royo Maxwell, S., Lee Blair, S., Eds.; Emerald Group Publishing: Bingley, UK, 2015; Volume 9, pp. 311–340. [Google Scholar]
- Abada, T.; Tenkorang, E.Y. Women’s autonomy and unintended pregnancies in the Philippines. J. Biosoc. Sci. 2012, 44, 703–718. [Google Scholar] [CrossRef]
- Crissman, H.P.; Adanu, R.M.; Harlow, S.D. Women’s sexual empowerment and contraceptive use in Ghana. Stud. Fam. Plann. 2012, 43, 201–212. [Google Scholar] [CrossRef]
- Speizer, I.S.; Pearson, E. Association between early marriage and intimate partner violence in india: A focus on youth from Bihar and Rajasthan. J. Interpers. Violence 2011, 26, 1963–1981. [Google Scholar] [CrossRef]
- Corsi, D.J.; Neuman, M.; Finlay, J.E.; Subramanian, S.V. Demographic and health surveys: A profile. Int. J. Epidemiol. 2012, 41, 1602–1613. [Google Scholar] [CrossRef]
- Aliaga, A.; Ruilin, R. Cluster optimal sample size for demographic and health surveys. In Proceedings of the 7th International Conference on Teaching Statistics–ICOTS, Bahia, Brazil, 2–7 July 2006; Volume 7, pp. 2–7. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Memiah, P.; Opanga, Y.; Bond, T.; Cook, C.; Mwangi, M.; Fried, J.; Machira, Y.W. Is sexual autonomy a protective factor for neonatal, child, and infant mortality? A multi-country analysis. PLoS ONE 2019, 14, e0212413. [Google Scholar] [CrossRef]
- Hossain, M.G.; Mahumud, R.A.; Saw, A. Prevalence of child marriage among Bangladeshi women and trend of change over time. J. Biosoc Sci. 2016, 48, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Skafte, I.; Silberschmidt, M. Female gratification, sexual power and safer sex: Female sexuality as an empowering resource among women in Rwanda. Cult. Health Sex. 2014, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Darteh, E.K.M.; Doku, D.T.; Esia-Donkoh, K. Reproductive health decision making among Ghanaian women. Reprod. Health 2014, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Darteh, E.K.M.; Dickson, K.S.; Doku, D.T. Women’s reproductive health decision-making: A multi-country analysis of demographic and health surveys in sub-Saharan Africa. PLoS ONE 2019, 14, e0209985. [Google Scholar] [CrossRef] [PubMed]
- Hameed, W.; Azmat, S.K.; Ali, M.; Sheikh, M.I.; Abbas, G.; Temmerman, M.; Avan, B.I. Women’s empowerment and contraceptive use: The role of independent versus couples’ decision-making, from a lower middle income country perspective. PLoS ONE 2014, 9, e104633. [Google Scholar] [CrossRef] [PubMed]
- Santhya, K.G.; Ram, U.; Acharya, R.; Jejeebhoy, S.J.; Ram, F.; Singh, A. Associations between early marriage and young women’s marital and reproductive health outcomes: Evidence from India. Int. Perspect. Sex. Reprod. Health 2010, 132–139. [Google Scholar] [CrossRef]
- Schlecht, J.; Rowley, E.; Babirye, J. Early relationships and marriage in conflict and post-conflict settings: Vulnerability of youth in Uganda. Reprod. Health Matters 2013, 21, 234–242. [Google Scholar] [CrossRef]
- Acharya, D.R.; Bell, J.S.; Simkhada, P.; Van Teijlingen, E.R.; Regmi, P.R. Women’s Autonomy in Household Decision-Making: A Demographic Study in Nepal. Reprod. Health 2010, 7, 1–2. [Google Scholar] [CrossRef] [PubMed]
- UN. Open Working Group Proposal for Sustainable Development Goals. 2015. Available online: https://sustainabledevelopment.un.org/ (accessed on 12 February 2021).



{kind=link}
{kind=link}
| Countries | Survey Year | Weighted N | Weighted % |
|---|---|---|---|
| Angola | 2015–16 | 5788 | 2.65 |
| Burkina Faso | 2010 | 12,015 | 5.50 |
| Benin | 2018–19 | 9572 | 4.38 |
| Burundi | 2016–17 | 9266 | 4.38 |
| Congo DR | 2013–14 | 9723 | 4.45 |
| Congo | 2011–12 | 5347 | 2.45 |
| Côte d’Ivoire | 2011–12 | 4997 | 2.29 |
| Cameroon | 2018 | 6874 | 3.14 |
| Ethiopia | 2016 | 8320 | 3.81 |
| Gabon | 2012 | 3590 | 1.64 |
| Ghana | 2014 | 4816 | 2.40 |
| Gambia | 2013 | 5252 | 2.40 |
| Guinea | 2018 | 5280 | 2.42 |
| Kenya | 2014 | 7762 | 3.55 |
| Comoros | 2012 | 2254 | 1.03 |
| Liberia | 2013 | 4781 | 2.19 |
| Lesotho | 2014 | 1368 | 0.63 |
| Mali | 2018 | 6813 | 3.12 |
| Malawi | 2015–16 | 14,322 | 6.55 |
| Nigeria | 2018 | 19.293 | 8.83 |
| Niger | 2012 | 7130 | 3.26 |
| Namibia | 2013 | 2304 | 1.05 |
| Rwanda | 2014–15 | 6698 | 3.06 |
| Sierra Leone | 2019 | 8381 | 3.83 |
| Senegal | 2010–11 | 7908 | 3.62 |
| Chad | 2014–15 | 9109 | 4.17 |
| Togo | 2013–14 | 5408 | 2.47 |
| Uganda | 2016 | 9673 | 4.42 |
| South Africa | 2016 | 2265 | 1.04 |
| Zambia | 2018–19 | 6806 | 3.11 |
| Zimbabwe | 2015 | 5481 | 2.51 |
| Total | 218,578 | 100 |
| Variables | Weighted N | Weighted % | Sexual Autonomy | p Value |
|---|---|---|---|---|
| Age at First Marriage | <0.0001 | |||
| Less than 18 years | 97,287 | 44.5 | 79.2 | |
| 18 years and more | 121,291 | 55.5 | 86.7 | |
| Mother’s Age | <0.001 | |||
| 20–24 | 39,675 | 18.2 | 83.0 | |
| 25–29 | 50,806 | 23.24 | 83.3 | |
| 30–34 | 44,274 | 20.26 | 83.9 | |
| 35–39 | 37,336 | 17.08 | 84.0 | |
| 40–44 | 26,124 | 12.0 | 83.5 | |
| 45–49 | 20,363 | 9.3 | 81.4 | |
| Educational Level | <0.0001 | |||
| No education | 89,929 | 41.1 | 72.7 | |
| Primary | 65,178 | 29.8 | 88.4 | |
| Secondary/higher | 63,471 | 29.0 | 93.3 | |
| Employment Status | <0.0001 | |||
| Not working | 55,761 | 25.5 | 77.5 | |
| Working | 162,817 | 74.5 | 85.4 | |
| Mass Media Exposure | <0.0001 | |||
| No | 75,782 | 35.1 | 74.6 | |
| Yes | 141,796 | 64.9 | 88.1 | |
| Partner’s Educational Level | <0.0001 | |||
| No education | 75,791 | 34.7 | 72.1 | |
| Primary education | 57,357 | 26.2 | 86.7 | |
| Secondary/higher education | 85,429 | 39.1 | 92.1 | |
| Partner’s Occupational Status | <0.0001 | |||
| Not working | 7842 | 3.6 | 79.6 | |
| Working | 210,736 | 96.4 | 83.5 | |
| Type of Place of Residence | <0.0001 | |||
| Urban | 77,470 | 35.4 | 88.9 | |
| Rural | 141,108 | 64.6 | 80.3 | |
| Wealth Quintile | <0.0001 | |||
| Poorest | 40,315 | 18.4 | 77.7 | |
| Poorer | 43,168 | 19.8 | 80.4 | |
| Middle | 43,511 | 19.9 | 82.5 | |
| Richer | 45,222 | 20.7 | 85.4 | |
| Richest | 46,362 | 21.2 | 89.8 | |
| Sex of Head of Household | <0.0001 | |||
| Male | 185,236 | 84.7 | 82.8 | |
| Female | 33,342 | 15.3 | 86.4 | |
| Variable | Model I cOR (95% CI) | Model II aOR (95% CI) |
|---|---|---|
| Age at First Marriage | ||
| Less than 18 years | 0.58 *** (0.56–0.60) | 0.86 *** (0.83–0.89) |
| 18 years and more | Ref | Ref |
| Mother’s Age | ||
| 20–24 | 0.98 (0.94–1.03) | 0.98 (0.93–1.02) |
| 25–29 | Ref | Ref |
| 30–34 | 1.05 (1.00–1.09) | 1.07 ** (1.02–1.12) |
| 35–39 | 1.06 * (1.01–1.11) | 1.14 *** (1.08–1.19) |
| 40–44 | 1.02 (0.97–1.07) | 1.13 *** (1.07–1.20) |
| 45–49 | 0.89 *** (0.85–0.94) | 1.05 (0.99-1.11) |
| Educational Level | ||
| No education | 0.34 *** (0.32-0.36) | 0.50 *** (0.47–0.53) |
| Primary | Ref | Ref |
| Secondary/higher | 1.72 *** (1.61–1.84) | 1.39 *** (1.30–1.48) |
| Employment Status | ||
| Not working | 0.55 *** (0.53–0.58) | 0.62 *** (0.59–0.65) |
| Working | Ref | Ref |
| Exposure to Mass Media | ||
| No | 0.39 *** (0.37–0.41) | 0.53 *** (0.50–0.55) |
| Yes | Ref | Ref |
| Partner’s Educational Level | ||
| No education | 0.25 *** (0.24–0.27) | 0.56 *** (0.53–0.60) |
| Primary education | 0.68 *** (0.65–0.72) | 0.97 (0.92–1.02) |
| Secondary/higher education | Ref | Ref |
| Partner’s Occupational Status | ||
| Not working | 0.81 *** (0.74–0.89) | 0.95 (0.87–1.04) |
| Working | Ref | Ref |
| Type of Place of Residence | ||
| Urban | 1.77 *** (1.63–1.92) | 0.98 (0.89–1.07) |
| Rural | Ref | Ref |
| Wealth Quintile | ||
| Poorest | 0.85 *** (0.81–0.90) | 1.04 (0.98–1.10) |
| Poorer | Ref | Ref |
| Middle | 1.14 *** (1.09–1.20) | 0.97 (0.92–1.02) |
| Richer | 1.41 *** (1.32–1.51) | 0.97 (0.90–1.04) |
| Richest | 2.12 *** (1.93–2.32) | 0.93 (0.85–1.03) |
| Sex of Head of Household | ||
| Male | Ref | Ref |
| Female | 1.30 *** (1.23–1.37) | 1.13 *** (1.07–1.19) |
| Countries | Model I cOR (95% CI) | Model II aOR (95% CI) |
|---|---|---|
| Angola | 0.96 (0.85–1.09) | 1.14 (0.99–1.30) |
| Burkina Faso | 0.82 *** (0.73–0.93) | 0.93 (0.82–1.05) |
| Benin | 0.86 *** (0.79–0.94) | 0.93 (0.85–1.02) |
| Burundi | 0.74 *** (0.63–0.86) | 0.78 *** (0.67–0.92) |
| Congo DR | 0.77 *** (0.68-.87) | 0.86 ** (0.76–0.97) |
| Congo | 0.71 ** (0.54–0.94) | 0.77 (0.58–1.05) |
| Côte d’Ivoire | 0.66 *** (0.56–0.78) | 0.85 (0.71–1.01) |
| Cameroon | 0.61 *** (0.53–0.70) | 0.98 (0.84–1.14) |
| Ethiopia | 0.78 *** (0.70–0.86) | 1.05 (0.93–1.7) |
| Gabon | 0.78 (0.46–1.30) | 1.25 (0.72–2.18) |
| Ghana | 0.73 ** (0.55–0.98) | 1.01 (0.75–1.35) |
| Gambia | 0.78 *** (0.67–0.92) | 1.00 (0.84–1.19) |
| Guinea | 0.93 (0.83–1.04) | 1.04 (0.92–1.17) |
| Kenya | 0.55 *** (0.47–0.66) | 1.03 (0.85–1.26) |
| Comoros | 0.91 (0.68–1.22) | 1.11 (0.81–1.52) |
| Liberia | 0.77 ** (0.62–0.97) | 0.85 (0.67–1.07) |
| Lesotho | 1.06 (0.22–5.13) | 1.59 (0.29–8.79) |
| Mali | 0.90 ** (0.81–0.99) | 0.96 (0.86–1.07) |
| Malawi | 0.97 (0.85–1.10) | 1.15 (0.99–1.31) |
| Nigeria | 0.41 *** (0.37–0.45) | 0.85 *** (0.76–0.95) |
| Niger | 0.62 *** (0.53–0.72) | 0.75 *** (0.64–0.89) |
| Namibia | 1.65 (0.38–7.09) | 2.76 (0.60–12.81) |
| Rwanda | 0.38 * (0.15–1.00) | 0.43 (0.16–1.16) |
| Sierra Leone | 1.07 (0.95–1.22) | 1.12 (0.99–1.27) |
| Senegal | 0.78 *** (0.69–0.88) | 1.06 (0.93–1.20) |
| Chad | 1.00 (0.88–1.13) | 1.10 (0.96–1.36) |
| Togo | 0.60 *** (0.49–0.74) | 0.84 (0.68–1.04) |
| Uganda | 0.79 * (0.61–1.01) | 1.00 (0.77–1.29) |
| South Africa | 0.72 * (0.51–1.01) | 0.76 (0.53–1.08) |
| Zambia | 0.89 (0.77–1.02) | 1.10 (0.94–1.27) |
| Zimbabwe | 0.64 *** (0.49–0.84) | 0.96 (0.72–1.29) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budu, E.; Ahinkorah, B.O.; Seidu, A.-A.; Hagan, J.E., Jr.; Agbemavi, W.; Frimpong, J.B.; Adu, C.; Dickson, K.S.; Yaya, S. Child Marriage and Sexual Autonomy among Women in Sub-Saharan Africa: Evidence from 31 Demographic and Health Surveys. Int. J. Environ. Res. Public Health 2021, 18, 3754. https://doi.org/10.3390/ijerph18073754
Budu E, Ahinkorah BO, Seidu A-A, Hagan JE Jr., Agbemavi W, Frimpong JB, Adu C, Dickson KS, Yaya S. Child Marriage and Sexual Autonomy among Women in Sub-Saharan Africa: Evidence from 31 Demographic and Health Surveys. International Journal of Environmental Research and Public Health. 2021; 18(7):3754. https://doi.org/10.3390/ijerph18073754
Chicago/Turabian StyleBudu, Eugene, Bright Opoku Ahinkorah, Abdul-Aziz Seidu, John Elvis Hagan, Jr., Wonder Agbemavi, James Boadu Frimpong, Collins Adu, Kwamena Sekyi Dickson, and Sanni Yaya. 2021. "Child Marriage and Sexual Autonomy among Women in Sub-Saharan Africa: Evidence from 31 Demographic and Health Surveys" International Journal of Environmental Research and Public Health 18, no. 7: 3754. https://doi.org/10.3390/ijerph18073754
APA StyleBudu, E., Ahinkorah, B. O., Seidu, A.-A., Hagan, J. E., Jr., Agbemavi, W., Frimpong, J. B., Adu, C., Dickson, K. S., & Yaya, S. (2021). Child Marriage and Sexual Autonomy among Women in Sub-Saharan Africa: Evidence from 31 Demographic and Health Surveys. International Journal of Environmental Research and Public Health, 18(7), 3754. https://doi.org/10.3390/ijerph18073754