
The Therapeutic Relationship in China: A Systematic Review and Meta-Analysis


 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Result
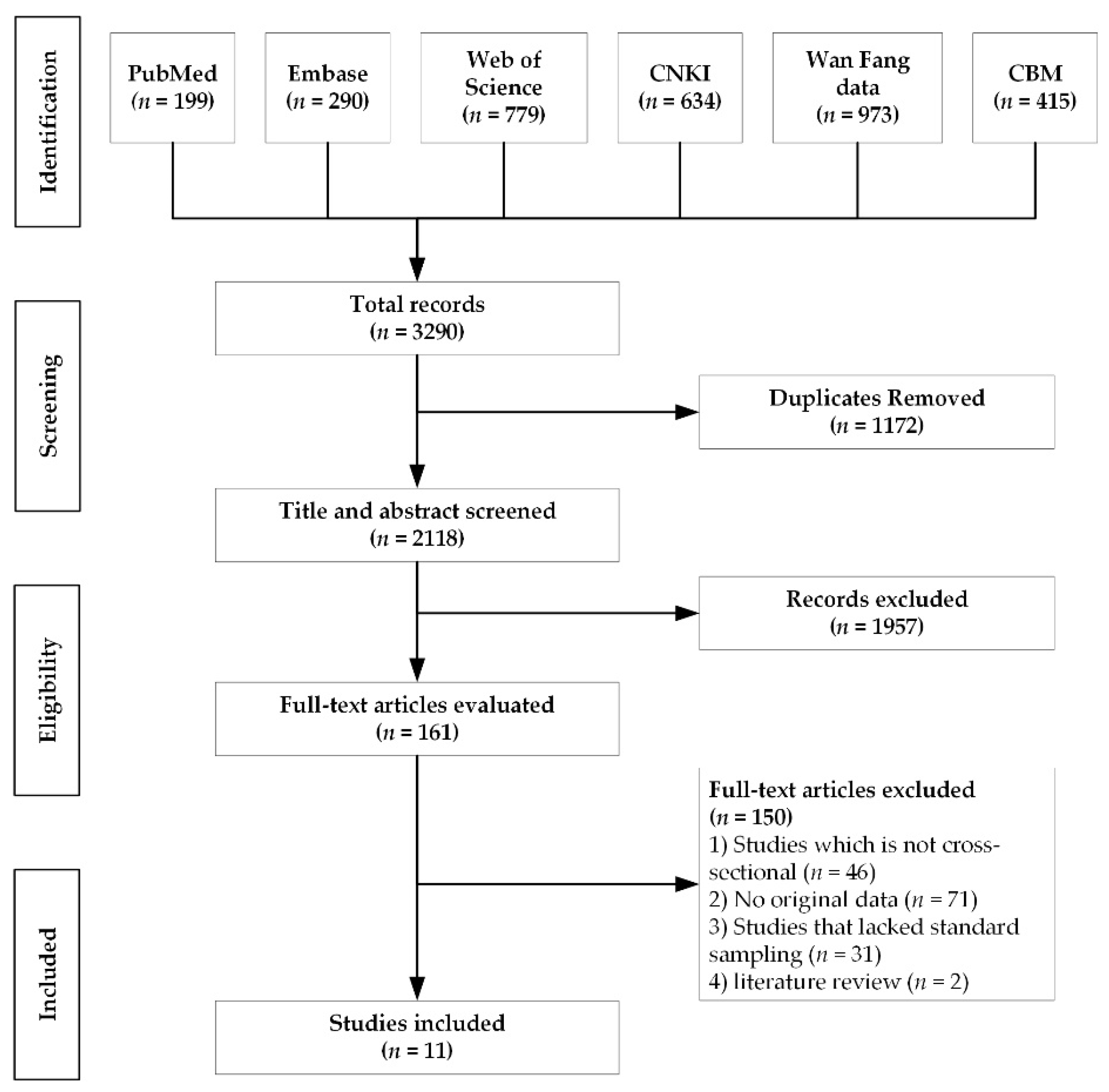
3.1. Search Results
3.2. Analysis of the Included Articles
3.3. Quality of the Included Articles
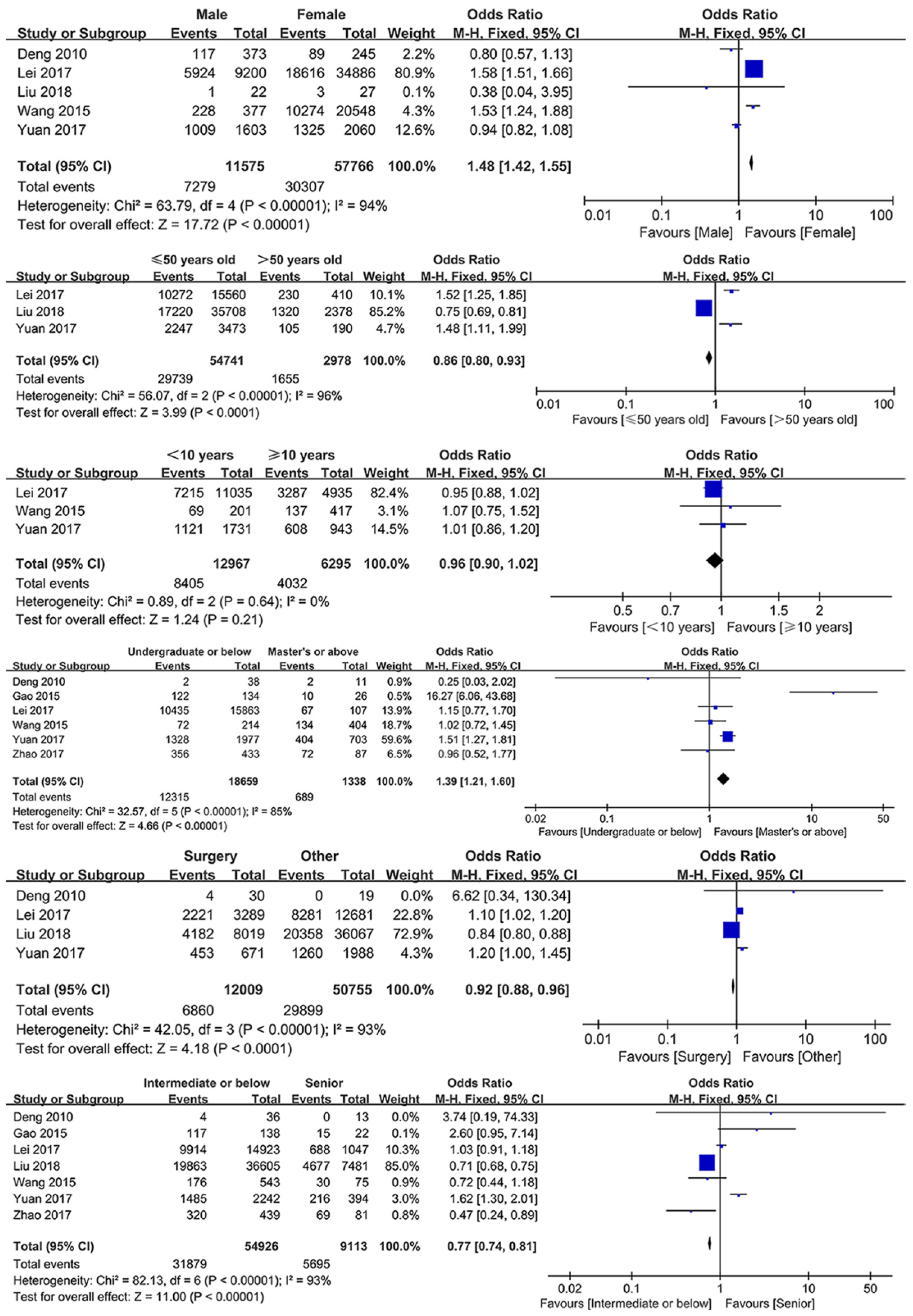
3.4. Analysis of Healthcare Worker-Related Factors
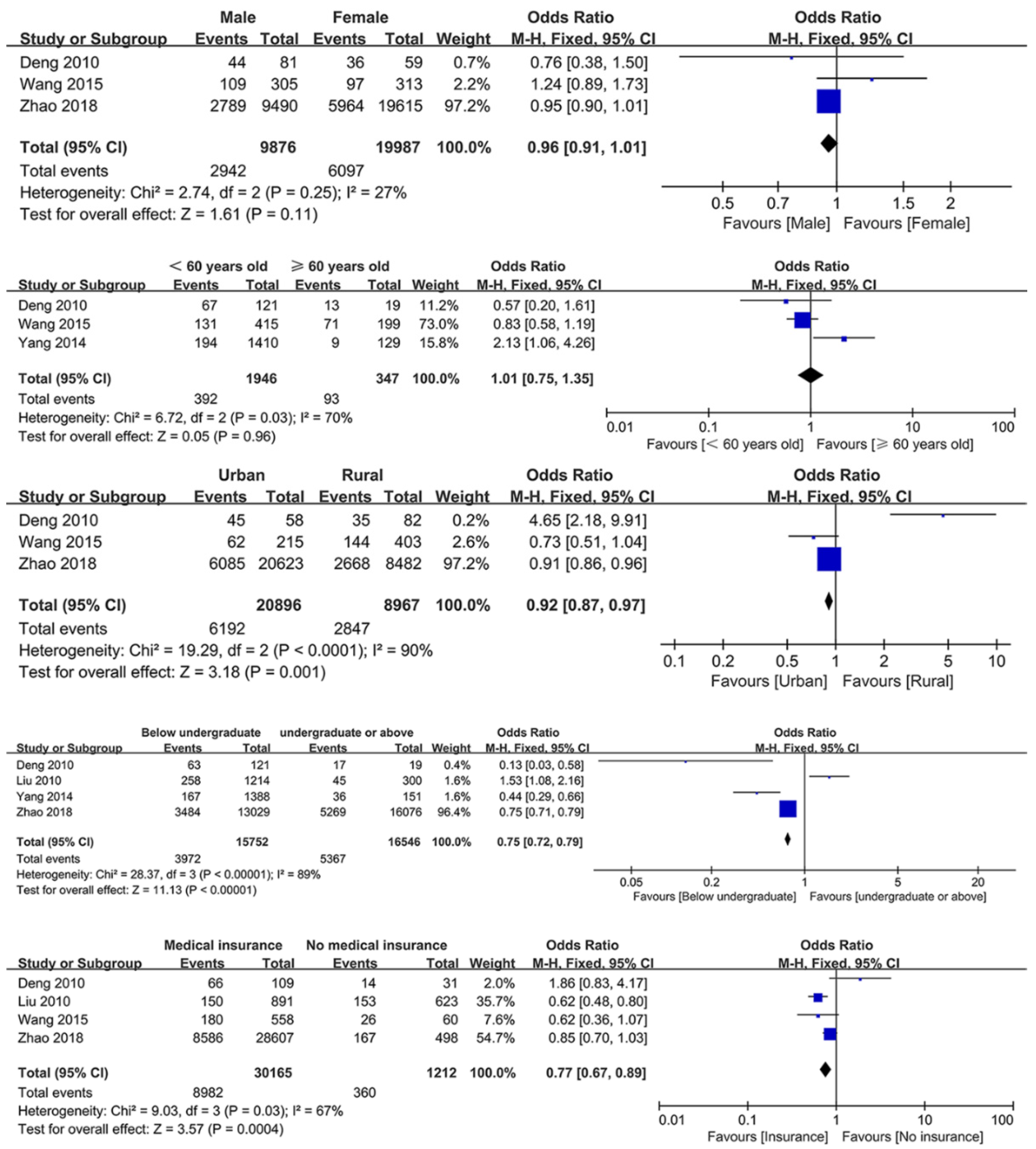
3.5. Analysis of Patient-Related Factors
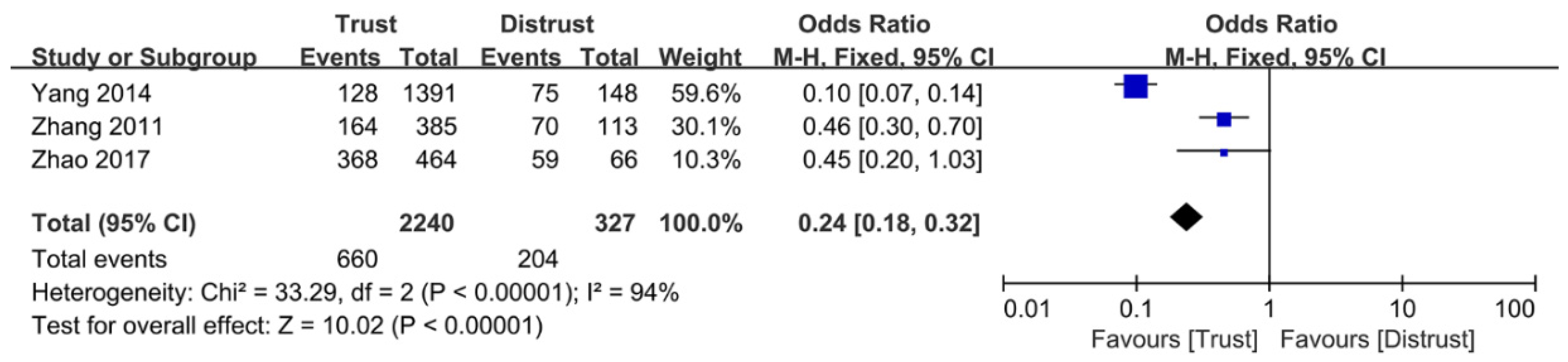
3.6. Analysis of Therapeutic Interaction-Related Factors
4. Discussion
4.1. Impact of Healthcare Worker-Related Factors
4.2. Impact of Patient-Related Factors
4.3. Impact of Therapeutic Interaction-Related Factors
4.4. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TR | Therapeutic Relationship |
| PCC | Person-Centered Care |
| WB | The World Bank |
| WHO | The World Health Organization |
| PCIC | People-Centered and Integrated Health Care |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| CNKI | China National Knowledge Internet Database |
| CBM | China Biology Medicine disc |
| GRADE | The Grading of Recommendations: Assessment, Development, and Evaluation |
| HWP | Healthcare worker Perspective |
| PP | Patient Perspective |
| TIP | Therapeutic Interaction Perspective |
| OR | Odds Ratio |
| PDRQ | Patient-Doctor Relationship Questionnaire |
| DDPRQ | Difficult Doctor-Patient Relationship Questionnaire |
References
- Wang, L.Q. An analysis on the governance of medical disputes and conflicts in china during the social transformation period. Mod. Hosp. 2020, 20, 1753–1756. [Google Scholar]
- Hu, N. Research on the Current Situation, Causes and Countermeasures of Doctor-Patient Disputes in the New Era. China Health Stand. Manag. 2020, 11, 20–23. [Google Scholar]
- Xu, Z.W.; Pan, K.L.; Ye, X.X. Analysis of Causes and Policy Recommendations of Disharmony between Doctors and Patients. Hosp. Manag. Forum 2020, 37, 38–41. [Google Scholar]
- Mao, Y.; Xie, T.; Ning, W. The Influence of Medical Service Quality on Patients’ perception of Doctor-Patient Relationship: Mediating Effect Analysis Based on Patient satisfaction. J. Xi’an Jiaotong Univ. (Soc. Sci.) 2020, 40, 119–127. [Google Scholar]
- Shi, Z.; Liu, J. Fracturing and bridging: Cognitive differences in doctor-patient relationship and improvement of doctor-patient trust: A case study in Inner Mongolia. Mod. Commun. 2019, 23, 92–93. [Google Scholar]
- Kim, S.S.; Cho, D.Y.; Park, B.K.; Hwang, I.K.; Chang, C.L.; Lee, Y.M.; Yune, S.J. Differences in Patients’ Awareness of Doctors’ Communication Styles, Patients’ Satisfaction, and Patients’ Compliance among Patient Social Styles. Korean J. Med. Educ. 2008, 20, 321–331. [Google Scholar] [CrossRef]
- Alkorashy, H.A.; Al, M.F. Workplace violence against nursing staff in a Saudi university hospital. Int. Nurs. Rev. 2016, 63, 226–232. [Google Scholar] [CrossRef]
- Fallahi-Khoshknab, M.; Oskouie, F.; Ghazanfari, N.; Najafi, F.; Tamizi, Z.; Afshani, S.; Azadi, G.; Student, M. The Frequency, Contributing and Preventive Factors of Harassment towards Health Professionals in Iran. Int. J. Community Nurs. Midwifery 2015, 3, 156. [Google Scholar]
- Jena, A.B.; Seabury, S.; Lakdawalla, D.; Chandra, A. Malpractice risk according to physician specialty. N. Engl. J. Med. 2011, 365, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Speroni, K.G.; Fitch, T.; Dawson, E.; Dugan, L.; Atherton, M. Incidence and cost of nurse workplace violence perpetrated by hospital patients or patient visitors. J. Emerg. Nurs. 2014, 40, 218–228, 295. [Google Scholar] [CrossRef] [PubMed]
- China Minutes: German ‘Medical Dispute’: Nearly 40 Percent of Doctors Have Been Beaten. 2018. Available online: http://www.oushinet.com/europe/germany/20180510/290943.html (accessed on 15 February 2020).
- Hiyama, T.; Yoshihara, M.; Tanaka, S.; Chayama, K. Trend in Japanese malpractice litigation involving gastrointestinal endoscopy. Am. J. Gastroenterol. 2009, 104, 251–252. [Google Scholar] [CrossRef]
- Guan Tian, G.S. Don’t rely on government protection for everything. Fancy Grass (Class. Read.) 2015, 5, 16. [Google Scholar]
- Qian, J. Overdependence on the Government to be Guarded against in Improving the People’s Wellbeing. J. Guizhou Univ. Financ. Econ. 2012, 1, 1–5. [Google Scholar]
- Wang, X.Y.; Lei, X.S. The impact of the rapid development of private hospitals on public hospitals and the countermeasures of public hospitals. J. Med. Theory Pract. 2016, 29, 1826–1828. [Google Scholar]
- Song, S.S.; Wang, F.Y. Study on the Causes and Improvement Paths of Disharmonious Doctor-patient Relationship. Mod. Hosp. Manag. 2020, 18, 89–92. [Google Scholar]
- Chen, D.H. Ethical Diagnosis and Treatment of the Tense Relationship between Doctors and Patients: Rationality and Limitation. J. Jiangsu Univ. (Soc. Sci. Ed.) 2020, 22, 52–63. [Google Scholar]
- Zhao, H.L.; Zhong, M. About the predicament and policy improvement of “difficult and expensive to get the medical treatment” in our country. Rural Econ. Sci. Technol. 2019, 30, 149–150. [Google Scholar]
- Ma, S.X.; Li, K.Z.; Zheng, F.Y.; Li, S.N. Discussion on Harmonious Doctor-patient Relationship in the New Era and Under the New Contradictions. Heilongjiang Med. J. 2019, 43, 294–296. [Google Scholar]
- Chinese Medical Doctor Association. White Paper on the Practice of Doctors in China. Chinese Medical Doctor Association. 2017. Available online: http://www.cmda.net/u/cms/www/201807/06181247ffex.pdf (accessed on 15 February 2020).
- Zhao, K.D.; Zhang, W.; Yi, Y.X.; Chen, Y.R.; Cao, J. Exploration on the Reform of Humanistic Quality Education for Medical Students from the Perspective of Improving Doctor-Patient Relationship. J. Jinzhou Med. Univ. (Soc. Sci. Ed.) 2020, 18, 28–30. [Google Scholar]
- Li, Z.X.; Zhang, J.; Zhu, L.Y.; Yin, H.Y.; Liu, G.D.; Ji, C.Y.; Huang, X.H.; Hang, L.; Yu, J.F. Time Attribute of China’s Doctor-patient Conflict and Social Governance Strategies. Chin. Hosp. Manag. 2019, 39, 65–67, 74. [Google Scholar]
- Wang, Z.J.; Zhang, P.W.; Liu, M.C.; Yang, Z.R.; Pei, C.Y.; Sun, J.; Liu, Y.L. Outpatient experiences: Major findings from the third-party evaluation of the China Healthcare Improvement Initiative. J. Chin. Res. Hosp. 2020, 7, 51–56, 167–173. [Google Scholar]
- Yu, H.; Pan, H.W.; Zhang, X. The Analysis on the Agents of Doctor-patient Culture Conflicts in Clinical Diagnosis and Treatment. Med. Philos. B 2015, 36, 88–90. [Google Scholar]
- Bai, N.; Yin, M. Interpretation of the Doctor-patient Conflict in China from the Perspective of Social Culture Comparison between China and Western. Med. Philos. A 2012, 33, 36–38. [Google Scholar]
- The Work Bank; World Health Organization; Ministry of Finance of the People’s Republic of China; National Health Commission of the People’s Republic of China; Ministry of Human Resources and Social Security of the People’s Republic of China. Deepening Health Reform in China: Building High-Quality and Value-Based Service Delivery. 2016. Available online: http://documents1.worldbank.org/curated/zh/707951469159439021/pdf/107176-REVISED-PUBLIC-CHINESE-Health-Reform-In-China-Policy-Summary-Oct-reprint-CHN.pdf (accessed on 14 March 2021).
- Tucker, J.D.; Cheng, Y.; Wong, B.; Gong, N.; Nie, J.; Zhu, W.; McLaughlin, M.M.; Xie, R.; Deng, Y.; Huang, M.; et al. Patient-physician mistrust and violence against physicians in Guangdong Province, China: A qualitative study. BMJ Open 2015, 5, e8221. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Zeng, X.; Wang, Z. Recognition of relationship between doctors and patients among medical staff. Chin. J. Public Health 2013, 29, 1638–1641. [Google Scholar]
- Mo, X.; Xu, L.; Luo, H.; Gai, R. Medical Professional Perceived Doctor-patient Relationship, Job Satisfaction and Turnover Intention. Chin. J. Clin. Psychol. 2015, 23, 141–146. [Google Scholar]
- Sun, J.; Zhang, L.; Mu, P.; Wan, Y.; Liu, J.; He, C. Differences in the cognitive evaluation of the doctor-patient relationship between the medical side and the contracting parties. Chin. Ment. Health J. 2016, 30, 486–491. [Google Scholar]
- WW, L.; HL, W. Assessment of Patient-Doctor Depth-of-Relationship Scale and Influencing Factors for the Depth of Patient-doctor Relationship. Chin. Gen. Pract. 2015, 22, 2705–2708. [Google Scholar]
- Ma, T.; Li, J.; Wang, J.; Zhang, L.; Chen, H. Relationship Among Perceived Physician—Patient Relationship, Job Involvement and Job Satisfaction of Medical Staffs in Jinli Province. Med. Soc. 2018, 31, 62–65. [Google Scholar]
- Zhang, X.; Liu, Y.; Tu, L.; Hu, Y. The Overall Evaluation of the Current Tense Doctor-patient Relationship in China. Mod. Hosp. Manag. 2014, 12, 6–10. [Google Scholar]
- Dickinson, G.E.; Pearson, A.A. Sex-Differences of Physicians in Relation to Dying Patients. J. Am. Med. Womens Assoc. 1979, 34, 45–47. [Google Scholar]
- Yang, H.; Lu, M.; He, L. A comparison and analysis of the present status of doctor—Patient relationship among medical staffs and patients: A meta—analysis. J. Xiangnan Univ. (Med. Sci.) 2015, 17, 7–10. [Google Scholar]
- Gray, J. The effect of the doctor’s sex on the doctor-patient relationship. J. R. Coll. Gen. Pract. 1982, 236, 167–169. [Google Scholar]
- Walton, H.J. Sex differences in ability and outlook of senior medical students. Br. J. Med. Educ. 1968, 2, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.S.; Cartwright, A. Patients and Their Doctors: A Study of General Practice. Am. Soc. Rev. 1968, 33, 997. [Google Scholar] [CrossRef]
- Abiola, T.; Udofia, O.; Abdullahi, A. Patient-doctor relationship: The practice orientation of doctors in Kano. Niger. J. Clin. Pract. 2014, 17, 241. [Google Scholar] [CrossRef]
- Babitsch, B.; Braun, T.; Borde, T.; David, M. Doctor’s perception of doctor-patient relationships in emergency departments: What roles do gender and ethnicity play? BMC Health Serv. Res. 2008, 8, 82. [Google Scholar] [CrossRef]
- Wang, G.; Xu, Y.; Wang, W.; Liu, Q.; Zhao, Y.; Jiang, S.; Luo, J. Differences and Influencing Factors in the Evaluation of the Doctor-patient Relationship between the Medical Side and the Contracting Parties. Chin. J. Soc. Med. 2018, 35, 522–526. [Google Scholar]
- Xing, K.; Zhang, X.; Jiao, M.; Cui, Y.; Lu, Y.; Liu, J.; Zhang, J.; Zhao, Y.; Zhao, Y.; Li, Y.; et al. Concern about Workplace Violence and Its Risk Factors in Chinese Township Hospitals: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2016, 13, 811. [Google Scholar] [CrossRef] [PubMed]
- Roseanne Moody, F.; Marcee, E.; Lisa, B.; Renee, B.; Linda, W.; Marilyn, S.; Louise, A. A qualitative study of continuing education needs of rural nursing unit staff: The nurse administrator’s perspective. Nurs. Educ. Today 2013, 33, 364–369. [Google Scholar]
- Zhang, P.; Wang, F.; Cheng, Y.; Zhang, L.Y.; Ye, B.Z.; Jiang, H.W.; Sun, Y.; Zhu, X.; Liang, Y. Impact of organizational and individual factors on patient-provider relationships: A national survey of doctors, nurses and patients in China. PLoS ONE 2017, 12, e181396. [Google Scholar] [CrossRef] [PubMed]
- Qiao, T.; Fan, Y.; Geater, A.F.; Chongsuvivatwong, V.; McNeil, E.B. Factors associated with the doctor–patient relationship: Doctor and patient perspectives in hospital outpatient clinics of Inner Mongolia Autonomous Region, China. Patient Prefer. Adherence 2019, 13, 1125–1143. [Google Scholar] [CrossRef]
- Yu, Y.; Hao, Y.; Liang, L.; Wu, Q.; Zhang, Y.; Kang, Z.; Jiao, M.; Pan, Q. Analysis of medical staff perspective factors influencing a harmonious doctor-patient relationship: Based on 27 public hospitals of Heilongjiang province. Chin. J. Health Policy 2016, 9, 15–19. [Google Scholar]
- Zeng, Y.; Zhang, L.; Yao, G.; Fang, Y. Analysis of current situation and influencing factor of medical disputes among different levels of medical institutions based on the game theory in Xiamen of China: A cross-sectional survey. Medicine (Baltimore) 2018, 97, e12501. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.; Zeller, A.; Needham, I.; Kok, G.; Dassen, T.; Halfens, R.J.G. Patient and visitor violence in general hospitals: A systematic review of the literature. Aggress. Violent Behav. 2008, 13, 431–441. [Google Scholar] [CrossRef]
- Olsen, D.; Bellass, S.; Stievano, A.; Johnson, M.; Rocco, G.; Sabatino, L. Nursing’s professional respect as experienced by hospital and community nurses. Nurs. Ethics 2018, 25, 665–683. [Google Scholar]
- He, A.J.; Qian, J. Explaining Medical Disputes in Chinese Public Hospitals: The Doctor-Patient Relationship and Its Implications for Health Policy Reforms. Health Econ. Policy Law 2016, 11, 359–378. [Google Scholar] [CrossRef]
- Yang, Q.; Zhang, H.; Yu, M.; Hu, X.; Gu, Y.; Sun, X.; Zhen, X.; Gu, S.; Huang, M.; Wei, J.; et al. Chinese Minority Perceives the Doctor-Patient Relationship Differently: A Cultural and Economic Interpretation. Front. Public Health 2019, 7, 330. [Google Scholar] [CrossRef]
- Zhang, J.; Teng, W.; Tang, M.; Zhu, J.; Cai, W. Comparison Study on Cognition of Doctor-patient Relationship between Doctors and Patients. Med. Philos. 2012, 33, 58–59. [Google Scholar]
- Zhang, J.; Teng, W.; Tang, M.; Zhu, J.; Cai, W. Influencial Factors Analysis and Policy Selection of Physician—Patient Relationship in View of Hospital and Medical staff. Chin. Med. Ethics 2011, 24, 123–125. [Google Scholar]
- Namazi, H.; Aramesh, K.; Larijani, B. The doctor-patient relationship: Toward a conceptual re-examination. J. Med Ethics Hist. Med. 2016, 9, 10. [Google Scholar]
- Benatar, S.R. The changing doctor-patient relationship and the new medical ethics. SA J. Contin. Med. Educ. 1987, 5, 32–34. [Google Scholar]
- Beraldi, A.; Kukk, E.; Heußner, P.; Herschbach, P. Bedarf, Kenntnis, Akzeptanz und Nutzung von psychosozialen Angeboten. Onkologe 2016, 22, 121–126. [Google Scholar] [CrossRef]
- Hahn, S.R.; Thompson, K.S.; Wills, T.A.; Stern, V.; Budner, N.S. The difficult doctor-patient relationship: Somatization, personality and psychopathology. J. Clin. Epidemiol. 1994, 47, 647–657. [Google Scholar] [CrossRef]
- Gulbrandsen, P.; Hjortdahl, P.; Fugelli, P. General practitioners’ knowledge of their patients’ psychosocial problems: Multipractice questionnaire survey. BMJ 1997, 314, 1014–1018. [Google Scholar] [CrossRef]
- Wu, W.; Xu, J.; Wang, Y.; Ni, J.; Liu, D.; Zhou, B. Analyzing the influence of medical expenditure on doctor-patient relationship. Chin. Health Serv. Manag. 2013, 5, 332–333, 355. [Google Scholar]
- Skirbekk, H.; Middelthon, A.; Hjortdahl, P.; Finset, A. Mandates of Trust in the Doctor–Patient Relationship. Qual. Health Res. 2011, 21, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Dang, B.N.; Westbrook, R.A.; Njue, S.M.; Giordano, T.P. Building trust and rapport early in the new doctor-patient relationship: A longitudinal qualitative study. BMC Med. Educ. 2017, 17, 32. [Google Scholar] [CrossRef]
- Weber, A.S.; Verjee, M.A.; Musson, D.; Iqbal, N.A.; Mosleh, T.M.; Zainel, A.A.; Al-Salamy, Y. Patient opinion of the doctor-patient relationship in a public hospital in Qatar. Saudi Med. J. 2011, 32, 293. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thiels, C.A.; Bergquist, J.R.; Pandian, T.K.; Heller, S.F. Improving Communication Skills and Professionalism Among General Surgery Residents, One Page at a Time. Mayo Clin. Proc. 2016, 91, 539–541. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Group GW. Grading of Recommendations Assessment, Development and Evaluation. 2011. Available online: https://www.gradeworkinggroup.org/ (accessed on 25 March 2021).
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, D.; Zhou, C.; Yang, L.; Sun, T.; Hao, T.; Peng, X.; Gao, L.; Liu, W.; Mu, Y.; et al. A cross-sectional study on the prevalence and associated risk factors for workplace violence against Chinese nurses. BMJ Open 2017, 7, e013105. [Google Scholar] [CrossRef]
- Yuan, T.; Su, T.; Wang, R.; Li, M. Status quo of hospital violence suffered by medical personnel and study on influencing factors. Chin. J. Med. Manag. Sci. 2017, 7, 66–70. [Google Scholar]
- Liu, Q.; Wang, Z.; Wu, S.; Sun, J.; Liu, Y. Analysis of influencing factors of medical staffs’ perceptions on doctor-patient relationship. Chin. J. Hosp. Adm. 2018, 34, 319–325. [Google Scholar]
- Gao, X.; Wang, S.; Jiang, L.; Lu, Y.; Li, P.; Pu, C. Analysis on the Influances of Sanitary Resource Allocation the Doctor-Patient Relationship from the Perspective of Doctors—A Case Study of Chongqing. Chin. Prim. Health Care 2015, 29, 1–4. [Google Scholar]
- Zhao, P.; Wang, Z.; Huang, Z.; Liu, S.; Geng, S.; Sun, J.; Liu, Y. Status and Influencing Factor Analysis of the Perception of Outpatients Pertaining to Doctor-patient Relationship. Chin. J. Hosp. Adm. 2018, 34, 123–127. [Google Scholar]
- Liu, Y.; Bai, J. The research or current status and causes of medical disputes in part of hospitals in Urumqi. J. Xinjiang Med. Univ. 2010, 33, 554–557. [Google Scholar]
- Zhao, W.; Yang, L. Analysis on the Influencing Factors of Doctor-patient Relationship from the Perspective of Medical Staff. Shenzhen J. Integr. Tradit. Chin. West. Med. Jan. 2017, 27, 182–184. [Google Scholar]
- Zhang, J.; Teng, W.; Tang, M.; Zhu, J.; Cai, W. Influencial Factors Analysis and Policy Discussion of Physician-Patient Relationship in View of Patients’ Side. Chin. Med. Ethics 2011, 24, 199–200. [Google Scholar]
- Yang, J.; Zhang, X.; Chen, J. Basic Cognition on Doctor-patient Relationship Influencing Factors in Patients of Pilot Reform Hospital at Country Level. Chin. Med. Ethics 2014, 27, 92–95. [Google Scholar]
- Deng, F. The current situation and influencing factors of doctor-patient relationship in a hospital in Changsha. Pract. Prev. Med. 2010, 17, 182–183. [Google Scholar]
- Wang, Z.; Meng, X. A Study on the Influencing Factors of Medical Disputes in a City’s 3A Grade Hospitals. J. Math. Med. 2015, 28, 515–517. [Google Scholar]
- Yin, X.Y. Two Misunderstandings in Cognition of Doctor-Patient Relationship and Ethical Analysis. Hosp. Manag. Forum 2005, 2, 37–39. [Google Scholar]
- Zhou, L.; Xu, Z.Q. A comparative study on the cognition of doctors and patients on doctor-patient relationship based on investigation in Jinhua area. Chin. Nurs. Res. 2017, 31, 1013–1016. [Google Scholar]
- Lei, Y.; Wu, M. Survey on Medical Staffs’ Perception of Doctor-Patient Relationship: A Case Study of A Public Hospital in Beijing. Pract. J. Card. Cereb. Pneumal Vasc. Dis. 2010, 18, 1055–1057. [Google Scholar]
- Zhu, L.; Liu, K.; Bai, G.; Yuan, M.; Yi, D. Cognitive Differences of Doctor-patient Relationship between Doctors and Patients in Xilinhot Lnner Mongolia. Mil. Med. J. South China 2012, 26, 258–261. [Google Scholar]
- Yu, C.L.; Chen, Y.X.; Li, J.; Fan, X.W. Evaluation and Investigation on Job Satisfaction of Medical Staff in Public Hospital of Jiangsu Province. Med. Philos. 2020, 41, 40–43. [Google Scholar]
- Sun, L.R.; Yang, Z.L. The Effect of Social Prejudice and Group Threat on the Intergroup Conflict. J. Psychol. Sci. 2013, 36, 949–955. [Google Scholar]
- HE, J.A. Why Do Chinese Physicians Over-Prescribe?: Evidence from a Survey in Shenzhen, China The Doctor-Patient Relationship, Defensive Medicine and Overprescription in Chinese Public Hospitals: Evidence from a Cross-Sectional Survey in Shenzhen City. 2014. Available online: https://repository.eduhk.hk/en/publications/why-do-chinese-physicians-overprescribe-evidence-from-a-survey-in-3 (accessed on 23 March 2021).
- Baker, H. Doctor-Patient Relationship or Doctor-Public Relationship. Can. Med. Assoc. J. 1958, 78, 128–131. [Google Scholar]
- Wang, H.X. To Change the Current Situation of the Expansion of Large Hospitals Should Not Be Blocked. Chin. Health Insur. 2015, 5, 26–27. [Google Scholar]
- Zhang, W. Set up “People-Oriented” thought to Respect the Medical Service Needs of Patients. Jiangsu Health Syst. Manag. 2005, 1, 27. [Google Scholar]
- Lv, G.; Ji, Y.; Yuan, K.H.; Liu, T.F. Analysis on the status quo, dilemma and countermeasures of tiered medical system. Chin. Hosp. 2020, 24, 4–7. [Google Scholar]
- Shen, S.L.; Yu, X.S. Enlightenment of the UK Essential Healthcare System and Its Reform to General Practice Development in China. Chin. Gen. Pract. 2019, 22, 2286–2292. [Google Scholar]
- James, W.C. The patient/physician relationship: One doctor’s view. Health Aff. 1995, 14, 209. [Google Scholar]
- Robinson, G. Effective doctor patient communication: Building bridges and bridging barriers. Can. J. Neurol. Sci. 2002, 29 (Suppl. 2), S30. [Google Scholar] [CrossRef][Green Version]
- Cartwright, L.K. Personality differences in male and female medical students. Psychiatry Med. 1972, 3, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Li, J. Current Situation of Humanistic Care Ability of Medical Staff under the Background of Medical Education Cooperation. Guide Sci. Educ. 2020, 10, 184–185. [Google Scholar]
- Xu, H.; Zhang, Q.J. Investigation on Medical Humanistic Literacy of the Eight-Year Program Cadets in Military Medical Hospital. Med. Philos. 2020, 41, 66–69. [Google Scholar]
- Ying, M.Z.; Wang, Y.J. Medical Humanity and Doctor-Patient Relationship. Med. Educ. Res. Pract. 2014, 22, 1086–1088. [Google Scholar]
- He, X.S. The influence of humanistic care education of medical students on future doctor-patient relationship. China Extracurric. Educ. 2015, z1, 697. [Google Scholar]
- Loh, K.Y.; Sivalingam, N. Enhancing doctor-patient relationship: The humanistic approach. Med. J. Malays. 2008, 63, 85–87. [Google Scholar]
- Alcorta-Garza, A.; González-Guerrero, J.F.; Tavitas-Herrera, S.E.; Rodríguez-Lara, F.J.; Hojat, M. Validity and reliability of the Jefferson Scale of Physician Empathy in Mexican medial students. Salud Ment. 2005, 28, 57–63. [Google Scholar]
- Yang, Y.; Liu, Y.; Zhang, H.; Liu, J.; Liu, H.; Liu, H. Prevalence and influence factors of workplace violence among nurses in 3A grade hospitals. Chin. J. Public Health 2015, 31, 1155–1159. [Google Scholar]
- Loffler, C.; Hock, J.; Hornung, A.; Kundt, G.; Drewelow, E.; Volker, S.; Kreiser, B.; Riedel, J.; Altiner, A. What Makes Happy Doctors? Job Satisfaction of General Practitioners in Mecklenburg-Western Pomerania—A Representative Cross-sectional Study. Gesundheitswesen 2015, 77, 927–931. [Google Scholar]
- Daghio, M.M.; Ciardullo, A.V.; Cadioli, T.; Delvecchio, C.; Menna, A.; Voci, C.; Guidetti, P.; Magrini, N.; Liberati, A. GPs’ satisfaction with the doctor-patient encounter: Findings from a community-based survey. Fam. Pract. 2003, 20, 283–288. [Google Scholar] [CrossRef]
- Archibald, C. Job satisfaction among neonatal nurses. Pediatric Nurs. 2006, 32, 176–179, 162. [Google Scholar]
- Wu, D.; Wang, Y.; Lam, K.F.; Hesketh, T. Health system reforms, violence against doctors and job satisfaction in the medical profession: A cross-sectional survey in Zhejiang Province, Eastern China. BMJ Open 2014, 4, e6431. [Google Scholar] [CrossRef]
- Lu, Y.; Hu, X.; Huang, X.; Zhuang, X.; Guo, P.; Feng, L.; Hu, W.; Chen, L.; Hao, Y. Job satisfaction and associated factors among healthcare staff: A cross-sectional study in Guangdong Province, China. BMJ Open 2016, 6, e11388. [Google Scholar] [CrossRef]
- Zhang, X.; Sleeboom-Faulkner, M. Tensions between medical professionals and patients in mainland China. Camb. Q. Healthc. Ethics 2011, 20, 458–465. [Google Scholar] [CrossRef]
- Han, R.; Wei, L.; Li, J.; Zhang, D.; Li, H. The Mediating Effects of Job Satisfaction on the Association between Doctor-patient Relationship and OCB among Physicians in China. Iran. J. Public Health 2018, 47, 698–705. [Google Scholar] [PubMed]
- Zhang, Y.; Feng, X. Empirical study on determinants of physicians’ job satisfaction in urban public medical institutions. Chin. Health Resour. 2011, 14, 77–79. [Google Scholar]
- Liebman, B.L. Malpractice mobs: Medical dispute resolution in China. Columbia Law Rev. 2013, 113, 181–264. [Google Scholar]
- Wang, L.; Wu, Q.; Shan, L.; Parasor, A.; Li, Y.; Kang, Z.; Hao, J.; Pan, Q.; Liang, Z. Key Dimension Analysis of the Impact of Health Insurance on Doctor-patient Relationship: A Comparative Study Between China and Canada. Chin. Hosp. Manag. 2017, 37, 40–43. [Google Scholar]
- Chin, J.J. Doctor-patient relationship: A covenant of trust. Singap. Med. J. 2001, 42, 579. [Google Scholar]
- Eveleigh, R.M.; Muskens, E.; van Ravesteijn, H.; van Dijk, I.; van Rijswijk, E.; Lucassen, P. An overview of 19 instruments assessing the doctor-patient relationship: Different models or concepts are used. J. Clin. Epidemiol. 2012, 65, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Bending, Z.J. Reconceptualising the Doctor–Patient Relationship: Recognising the Role of Trust in Contemporary Health Care. J. Bioethical Inq. 2015, 12, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Wang, M.; Zuo, Y.; Li, M.; Lin, X.; Zhu, S.; Zheng, Y.; Yu, M.; Lamoureux, E.L. Health literacy, computer skills and quality of patient-physician communication in Chinese patients with cataract. PLoS ONE 2014, 9, e107615. [Google Scholar] [CrossRef]
- Wallis, W. Communication as fundamental to the Doctor-Patient relationship. Acta Biomed. Ateneo Parm. 2008, 79, 52. [Google Scholar]
- Singh, M. Communication as a Bridge to Build a Sound Doctor-Patient/Parent Relationship. Indian J. Pediatrics 2016, 83, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.R. Trusting in the New NHS: Instrumental versus communicative action. Soc. Health Illn. 2008, 30, 349–363. [Google Scholar] [CrossRef]
- Truog, R.D. Patients and doctors--evolution of a relationship. N. Engl. J. Med. 2012, 366, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Kharde, A.P.R.P.J. Dynamics of Doctor-Patient Relationship: A Cross-Sectional Study on Communication and Patient Satisfaction. Int. J. Health Sci. Res. 2016, 2, 65–68. [Google Scholar]
- Zolnierek, K.B.; Dimatteo, M.R. Physician communication and patient adherence to treatment: A meta-analysis. Med. Care 2009, 47, 826–834. [Google Scholar] [CrossRef]
- Duan, G.; Qiu, L.; Yu, W.; Hu, H. Outpatient service quality and doctor-patient relationship: A study in Chinese public hospital. Int. J. Serv. Econ. Manag. 2014, 6, 97. [Google Scholar] [CrossRef]
- Guimin, D.; Weiping, Y.; Jiawei, L.; Hongmei, Y. The research of factors influence doctor-patient relationship quality: Investigation of public hospitals in Sichuan province. In Proceedings of the 2016 13th International Conference on Service Systems and Service Management (ICSSSM), Kunming, China, 24–26 June 2016; pp. 1–6. [Google Scholar]
- Pan, Q.; Liang, L.; Wu, Q.; Hao, J.; Tao, S.; Huang, Z.; Shi, W.; Sun, H.; Jiao, M.; Yu, Y.; et al. Analysis of Factors Influencing the Doctor-patient Relationship: A Perspective Based on the Doctors and Patients in Public Hospitals. Chin. Hosp. Manag. 2016, 36, 68–70. [Google Scholar]
- Chen, Q.; Zheng, H. Review of Research on Doctor-patient Relationship at Home and Abroad. Med. Philos. 2014, 35, 44–48. [Google Scholar]
- Zhu, L.; Yuan, Y. The types, characteristics and countermeasures of doctor-patient contradictions in China at present. Soc. Sci. Res. 2014, 6, 104–111. [Google Scholar]
- Sun, H.; Liu, Y. To solve the dilemma of “difficult to see a doctor and expensive to see a doctor” by tiered diagnosis and treatment: From the perspective of supply and demand. Theor. Explor. 2017, 4, 93–98. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Criteria |
|---|---|
| Study type | Empirical studies published in a peer-reviewed journal |
| Study design | Cross-sectional studies |
| P (Population) | Doctors/Nurses and Patients |
| I (Intervention) | Population with positive attitudes towards the TR |
| C (Comparator) | Population with pessimistic attitudes towards the TR |
| O (Outcomes) | Studies that analysed the current situation and the related determinants, factors or influences of TR |
| Language | None language restrictions |
| Publication period | After 1 January 2000 and before 1 January 2020 |
| Authors | Location | Participants | Sample Size (Effective Response Rate %) | Analytical Perspective | Determinants | Negative Cases Rate *, N (%) |
|---|---|---|---|---|---|---|
| Shi, 2017 [67] | 16 provinces * (municipalities or autonomous regions) | Nurses | 15,970 (74.77) | HWP | Gender, Age, Education level, Marital status, Professional title, Employment form, Income, Department, Years of experience, Working time per day, Time spent in direct contact with patients. | 10,502 (65.76) |
| Zhao, 2017 [73] | Chongqing | Medical personnel | 520 (not stated) | HWP & TIP | HWP: Education level, Professional title, Income satisfaction, Medical ethics, Workload, Whether disputed with patient, Whether medical disputes interfere with work. TIP: Healthcare worker-patient trust. | 421 (80.96) |
| Yuan, 2017 [68] | Shanxi | Medical personnel | 3663 (81.40) | HWP | Gender, Age, Years of experience, Education level, Professional title, Marital status, Employment form, Department, Income. | 2334 (63.72) |
| Liu, 2018 [69] | Nationwide | Medical personnel | 44,086 (not stated) | HWP | Gender, Age, Hospital type, Region, Professional title, Administrative position, Department, Income, Medical liability insurance. | 24,540 (55.66) |
| Gao, 2015 [70] | Chongqing | Doctors | 160 (100) | HWP | Education level, Professional title, Workload, Daily average rate of outpatient visits, Working time per day, Whether disputed with patient, Whether worry about encountering dispute. | 132 (82.50) |
| Zhao, 2018 [71] | Nationwide | Outpatients | 29,105 (99.82) | PP | Hospital type, Region, Age, Gender, Department, Whether first visit, Education level, Medical insurance, Household income, Registration, Registered residence, Sources of patients, Whether have a familiar doctor, Whether have family doctors, Referral. | 8752 (30.07) |
| Zhang, 2011 [74] | Weifang | Patients | 498 (not stated) | PP & TIP | PP: Medical expenses, Whether have family doctors. TIP: Service attitude, Service quality and level, Treatment effect, Whether healthcare worker receives kickbacks on medications or medical devices, Doctor-patient trust, Whether adequate medical information is shared, Whether patient bribes or entertains doctors *. | 234 (46.99) |
| Wang, 2015 [77] | Wuhan | Patients & Medical personnel | Medical personnel: 618 (not stated) Patients: 618 (not stated) | HWP & PP & TIP | HWP: Gender, Age, Years of experience, Education level, Professional title, Career satisfaction, ability to handle dispute. PP: Gender, Registered residence, Age, Education level, Occupation, Medical insurance, operation, Medical expenses. TIP: Service attitude. | Medical personnel: 206 (33.33) Patients: 206 (33.33) |
| Yang, 2014 [75] | Hubei | Patients | 1539 (95.60) | PP & TIP | PP: Age, Education level, Medical insurance. TIP: Healthcare worker-patient communication, Healthcare worker-patient trust. | 203 (13.19) |
| Deng, 2010 [76] | Changsha | Patients & Medical personnel | Medical personnel: 49 Patients: 140 (Total qualified rate: 99.47) | HWP & PP | HWP: Age, Gender, Professional title, Department, Education level. PP: Age, Gender, Education level, Registered residence, Medical insurance, Household income. | Medical personnel: 4 (8.16) Patients: 80 (57.10) |
| Liu, 2010 [72] | Urumqi | Patients | 1514 (not stated) | PP | Medical insurance, Education level | 303 (20.01) |
| Authors | Sample Representativeness | Sample Size | Respondent Rate | Ascertainment of the Exposure | Comparability of Subjects in Different Outcome Groups | Outcome Assessment | Appropriate Statistical Test | Total Score |
|---|---|---|---|---|---|---|---|---|
| Shi, 2017 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Zhao, 2017 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| Yuan, 2017 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Liu, 2018 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| Gao, 2015 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| Zhao, 2018 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Zhang, 2011 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| Wang, 2015 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| Yang, 2014 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Deng, 2010 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 6 |
| Liu, 2010 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mao, Y.; Ning, W.; Zhang, N.; Xie, T.; Liu, J.; Lu, Y.; Zhu, B. The Therapeutic Relationship in China: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3460. https://doi.org/10.3390/ijerph18073460
Mao Y, Ning W, Zhang N, Xie T, Liu J, Lu Y, Zhu B. The Therapeutic Relationship in China: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(7):3460. https://doi.org/10.3390/ijerph18073460
Chicago/Turabian StyleMao, Ying, Wei Ning, Ning Zhang, Tao Xie, Jinnan Liu, Yongbo Lu, and Bin Zhu. 2021. "The Therapeutic Relationship in China: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 7: 3460. https://doi.org/10.3390/ijerph18073460
APA StyleMao, Y., Ning, W., Zhang, N., Xie, T., Liu, J., Lu, Y., & Zhu, B. (2021). The Therapeutic Relationship in China: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(7), 3460. https://doi.org/10.3390/ijerph18073460