
Community Living, Intellectual Disability and Extensive Support Needs: A Rights-Based Approach to Assessment and Intervention


Abstract
1. Introduction
- (a)
- Analysis of the extent to which a set of indicators contributes to measure the latent variables under study (i.e., professional practices aimed at promoting the right to living independently, alongside those of habilitation and rehabilitation and privacy of people with ID).
- (b)
- Analysis of the differences in these latent variables between people with ID and extensive support needs and people with ID and less intense support needs.
- (c)
- Analysis of the interaction effect between the home environment where people with ID live and the differences among the latent variables under study. (i.e., professional practices aimed at promoting the right to living independently, habilitation and rehabilitation and privacy).
2. Materials and Methods
2.1. Participants
2.2. Instrument
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Analysis Using ESEM Models of the Extent to Which the Set of Indicators Developed Allows the Study, Minimizing Measurement Error, of the Latent Variables That Are the Object of Research: Right to Living Independently and Being Included in the Community, Right to Privacy and Right to Habilitation and Rehabilitation
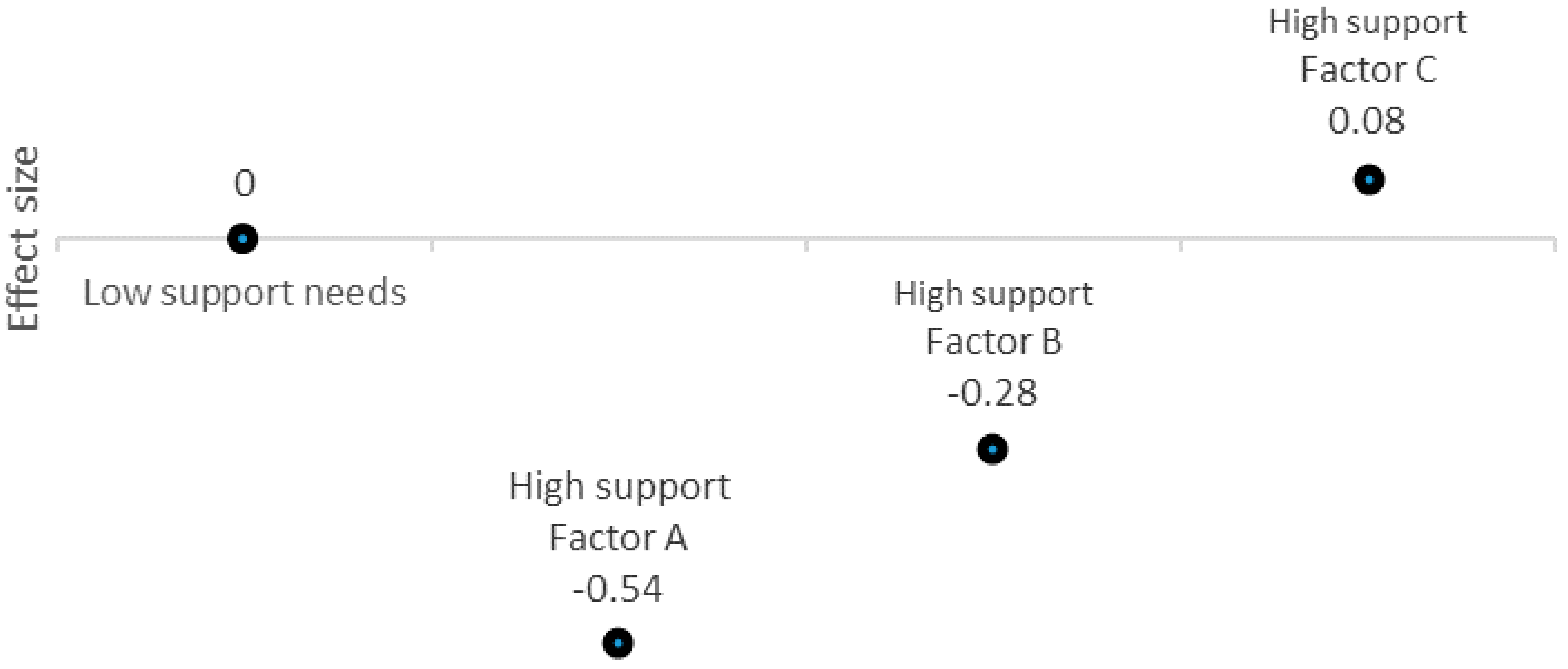
3.2. Analysis of Differences in the Latent Variables under Study between People with Intellectual Disability and Extensive Support Needs and People with Low Support Needs
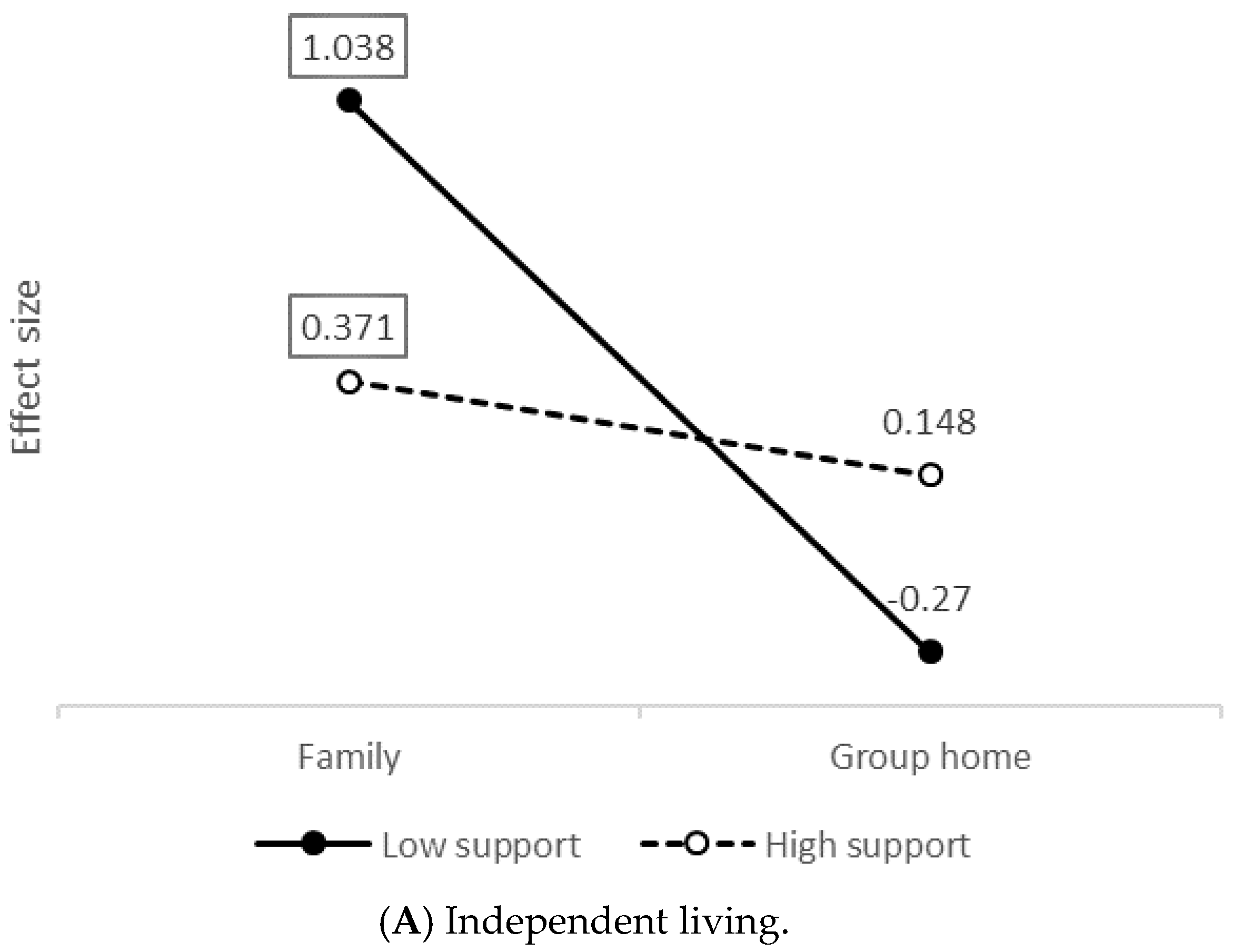
3.3. Analysis of the Interaction Effect between Living Environment and Differences in the Latent Variables under Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Convention on the Rights of Persons with Disabilities. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html#Fulltext (accessed on 21 December 2020).
- Verdugo, M.A.; Gómez, L.E.; Arias, B.; Navas, P.; Schalock, R.L. Measuring quality of life in people with intellectual and multiple disabilities: Validation of the San Martín scale. Res. Dev. Disabil. 2014, 35, 75–86. [Google Scholar] [CrossRef]
- Kozma, A.; Mansell, J.; Beadle-Brown, J. Outcomes in different residential settings for people with intellectual disability: A systematic review. Am. J. Intellect. Dev. Disabil. 2009, 114, 193–222. [Google Scholar] [CrossRef] [PubMed]
- Beadle-Brown, J.; Leigh, J.; Whelton, B.; Richardson, L.; Beecham, J.; Baumker, T.; Bradshaw, J. Quality of life and quality of support for people with severe intellectual disability and complex needs. J. Appl. Res. Intellect. Disabil. 2016, 29, 409–421. [Google Scholar] [CrossRef]
- Netten, A.; Beadle-Brown, J.; Trukeschitz, B.; Towers, A.; Welch, E.; Forder, J.; Smith, J.; Alden, E. Measuring the Outcomes of Care Homes: Final Report. Available online: www.pssru.ac.uk/pdf/dp2696_2.pdf (accessed on 21 December 2020).
- Baker, P.A. Individual and service factors affecting deinstitutionalization and community use of people with intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2007, 20, 105–109. [Google Scholar] [CrossRef]
- Nakken, H.; Vlaskamp, C. A need for a taxonomy for profound intellectual and multiple disabilities. J. Policy Pract. Intellect. Disabil. 2007, 4, 83–87. [Google Scholar] [CrossRef]
- Navas, P.; Verdugo, M.A. Todos Somos Todos: Análisis de los Apoyos Recibidos por Personas con Discapacidad Intelectual y Mayores Necesidades de Apoyo; Real Patronato sobre Discapacidad: Madrid, Spain, 2018; Available online: https://sid-inico.usal.es/documentacion/todos-somos-todos-analisis-de-los-apoyos-recibidos-por-personas-con-discapacidad-intelectual-y-mayores-necesidades-de-apoyo/ (accessed on 3 January 2021).
- Bigby, C.; Fyffe, C. Position statement on housing and support for people with severe or profound intellectual disability. J. Intellect. Dev. Disabil. 2009, 34, 96–100. [Google Scholar] [CrossRef]
- Doukas, T.; Fergusson, A.; Fullerton, M.; Grace, J. Supporting People with Profound and Multiple Learning Disabilities; PMLD Link: Cambridgeshire, UK, 2017; Available online: http://www.pmldlink.org.uk/wp-content/uploads/2017/11/Standards-PMLD-h-web.pdf (accessed on 3 January 2021).
- Mansell, J. Raising our sights: Services for adults with profound intellectual and multiple disabilities. Tizard Learn. Disabil. Rev. 2010, 15, 5–12. [Google Scholar] [CrossRef]
- Samuel, J.; Pritchard, M. The ignored minority: Meeting the needs of people with profound learning disability. Tizard Learn. Disabil. Rev. 2001, 6, 34–44. [Google Scholar] [CrossRef]
- Verdugo, M.A.; Navas, P. Todos Somos Todos: Derechos y Calidad de Vida de las Personas con Discapacidad Intelectual y Mayores Necesidades de Apoyo; Real Patronato sobre Discapacidad: Madrid, Spain, 2017. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Schalock, R.L.; Borthwick-Duffy, S.A.; Bradley, V.J.; Buntinx, W.H.E.; Coulter, D.L.; Craig, E.M.; Gomez, S.C.; Lachapelle, Y.; Luckasson, R.; Reeve, A.; et al. Intellectual Disability: Definition, Classification, and Systems of Supports, 11th ed.; American Association on Intellectual and Developmental Disabilities: Washington, DC, USA, 2010. [Google Scholar]
- Shogren, K.A.; Luckasson, R.; Schalock, R.L. The definition of “context” and its application in the field of intellectual disability. J. Policy Pract. Intellect. Disabil. 2014, 11, 109–116. [Google Scholar] [CrossRef]
- Björnsdóttir, K.; Stefánsdóttir, G.V.; Stefánsdóttir, Á. ‘It’s my life’ Autonomy and people with intellectual disabilities. J. Intellect. Disabil. 2015, 19, 5–21. [Google Scholar] [CrossRef]
- Dew, A.; Collings, S.; Dillon Savage, I.; Gentle, E.; Dowse, L. “Living the life I want”: A framework for planning engagement with people with intellectual disability and complex support needs. J. Appl. Res. Intellect. Disabil. 2019, 32, 401–412. [Google Scholar] [CrossRef]
- Vega, V.; Álvarez, I.; Jenaro, C. Autodeterminación: Explorando las autopercepciones de adultos con síndrome de Down chilenos. Siglo Cero 2018, 49, 89–104. [Google Scholar] [CrossRef]
- van Bakel, M.; Einarsson, I.; Arnaud, C.; Craig, S.; Michelsen, S.I.; Pildava, S.; Uldall, P.; Cans, C. Monitoring the prevalence of severe intellectual disability in children across Europe: Feasibility of a common database. Dev. Med. Child Neurol. 2014, 56, 361–369. [Google Scholar] [CrossRef]
- Arvio, M.; Sillanpää, M. Prevalence, etiology and comorbidity of severe and profound intellectual disability in Finland. J. Intellect. Disabil. Res. 2003, 47, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Emerson, E. Estimating Future Numbers of Adults with Profound Multiple Learning Disabilities in England. Tizard Learn. Disabil. Rev. 2009, 14, 49–55. [Google Scholar] [CrossRef]
- Kreuger, L.; Van Exel, J.; Nieboer, A. Needs of persons with severe intellectual disabilities: A Q-methodological study of clients with severe behavioural disorders and severe intellectual disabilities. J. Appl. Res. Intellect. Disabil. 2008, 21, 466–476. [Google Scholar] [CrossRef]
- Petry, K.; Maes, B.; Vlaskamp, C. Measuring the quality of life of people with profound multiple disabilities using the QOL-PMD: First results. Res. Dev. Disabil. 2009, 30, 1394–1405. [Google Scholar] [CrossRef]
- Beadle-Brown, J.; Murphy, G.; DiTerlizzi, M. Quality of life for the Camberwell cohort. J. Appl. Res. Intellect. Disabil. 2009, 22, 380–390. [Google Scholar] [CrossRef]
- Vos, P.; De Cock, P.; Petry, K.; Van Den Noortgate, W.; Maes, B. What makes them feel like they do? Investigating the subjective well-being in people with severe and profound disabilities. Res. Dev. Disabil. 2010, 31, 1623–1632. [Google Scholar] [CrossRef] [PubMed]
- Córdoba-Andrade, L.; Salamanca-Duque, L.M.; Mora-Anto, A. Calidad de vida en personas con discapacidad intelectual y múltiple de 4 a 21 años de edad. Psychologia 2019, 13, 79–94. [Google Scholar] [CrossRef]
- Lombardi, M.; Croce, L.; Claes, C.; Vandevelde, S.; Schalock, R.L. Factors predicting quality of life for people with intellectual disability: Results from the ANFFAS study in Italy. J. Intellect. Dev. Disabil. 2016, 41, 338–347. [Google Scholar] [CrossRef]
- Balboni, G.; Mumbardó-Adam, C.; Coscarelli, A. Influence of adaptive behaviour on the quality of life of adults with intellectual and developmental disabilities. J. Appl. Res. Intellect. Disabil. 2020, 33, 584–594. [Google Scholar] [CrossRef]
- Gur, A. Challenging behavior, functioning difficulties, and quality of life of adults with intellectual disabilities. Int. J. Dev. Disabil. 2018, 64, 45–52. [Google Scholar] [CrossRef]
- Memisevic, H.; Hadzic, S.; Zecic, S.; Mujkanovic, E. Predictors of quality of life in people with intellectual disability in Bosnia and Herzegovina. Int. J. Disabil. Hum. Dev. 2016, 15, 299–304. [Google Scholar] [CrossRef]
- Peña-Salazar, C.; Arrufat, F.; Fontanet, A.; Font, J.; Mas, S.; Roura-Poch, P.; Santos, J.M. The role of mental health and challenging behaviour in the quality of life in people with intellectual disabilities in Spain. Adv. Ment. Health Intellect. Disabil. 2018, 12, 34–43. [Google Scholar] [CrossRef]
- Beadle-Brown, J.; Mansell, J.; Kozma, A. Deinstitutionalization in intellectual disabilities. Curr. Opin. Psychiatr. 2007, 20, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Sáenz, I. Influencia del tipo de vivienda en la calidad de vida de las personas mayores con discapacidad intelectual o del desarrollo. Siglo Cero 2018, 49, 89–106. [Google Scholar] [CrossRef]
- Bigby, C.; Clement, T.; Mansell, J.; Beadle-Brown, J. ‘It’s pretty hard with our ones, they can’t talk, the more able bodied can participate’: Staff attitudes about the applicability of disability policies to people with severe and profound intellectual disabilities. J. Intellect. Disabil. Res. 2009, 53, 363–376. [Google Scholar] [CrossRef]
- Korinko, K.J. Quality of Life of People with Profound Developmental Disabilities Based upon Residential Settings. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2016. [Google Scholar]
- Bigby, C.; Cooper, B.; Reid, K. Making Life Good in the Community: Measures of Resident Outcomes and Staff Perceptions of the Move from an Institution; Department of Human Services: Melbourne, VIC, Australia, 2012. [Google Scholar]
- Young, L.; Ashman, A.F. Deinstitutionalisation in Australia Part II: Results from a long-term study. Br. J. Dev. Disabil. 2004, 50, 29–45. [Google Scholar] [CrossRef]
- Bigby, C.; Bould, E.; Beadle-Brown, J. Comparing costs and outcomes of supported living with group homes in Australia. J. Intellect. Dev. Disabil. 2018, 43, 295–307. [Google Scholar] [CrossRef]
- Young, L.; Ashman, A.F. Deinstitutionalization for older adults with severe mental retardation: Results from Australia. Am. J. Ment. Retard. 2004, 109, 397–412. [Google Scholar] [CrossRef]
- McCarron, M.; Lombard-Vance, R.; Murphy, E.; May, P.; Webb, N.; Sheaf, G.; McCallion, M.C.; Stancliffe, R.; Norman, C.; Smith, V.; et al. Effect of deinstitutionalisation on quality of life for adults with intellectual disabilities: A systematic review. BMJ Open 2019, 9, e025735. [Google Scholar] [CrossRef]
- McConkey, R.; Keogh, F.; Bunting, B.; García-Iriarte, E. Changes in the self-rated well-being of people who move from congregated settings to personalized arrangements and group home placements. J. Intellect. Disabil. 2018, 22, 49–60. [Google Scholar] [CrossRef] [PubMed]
- White, G.W.; Lloyd Simpson, J.; Gonda, C.; Ravesloot, C.; Coble, Z. Moving from independence to interdependence: A conceptual model for better understanding community participation of centers for independent living consumers. J. Disabil. Policy Stud. 2010, 20, 233–240. [Google Scholar] [CrossRef]
- Bellamy, G.; Croot, L.; Bush, A.; Berry, H.; Smith, A. A study to define: Profound and multiple learning disabilities (PMLD). J. Intellect. Disabil. 2010, 14, 221–235. [Google Scholar] [CrossRef]
- Šiška, J.; Beadle-Brown, J. Transition from Institutional Care to Community-Based Services in 27 EU Member States: Final Report; Research Report for the European Expert Group on Transition from Institutional to Community-Based Care; European Commission: Brussels, Belgium, 2020; Available online: https://www.mhe-sme.org/wp-content/uploads/2020/06/EEG-DI-REPORT-2020_with-foreword.pdf (accessed on 21 December 2020).
- Díaz, E. Evolución histórica de los servicios de atención a las personas en situación de dependencia: Del modelo de internamiento al enfoque comunitario. Intersticios. Rev. Sociol. Pensam. Crit. 2014, 8, 87–101. [Google Scholar]
- Ruíz, S.; Rodríguez, P.; Izuzquiza, D. Personal Assistants in the Promotion of Independent Living for Persons with Intellectual Disability: A Basic Applied Investigation. Siglo Cero 2019, 50, 19–38. [Google Scholar] [CrossRef]
- Concluding Observations on the Combined Second and Third Periodic Reports of Spain; United Nations: New York, NY, USA, 2019; Available online: https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CRPD%2fC%2fESP%2fCO%2f2-3&Lang=es (accessed on 21 December 2020).
- Parker, C. An Overview of Article 19 of the UN Convention on the Rights of Persons with Disabilities. In Focus on Article 19 of the UN Convention on the Rights of Persons with Disabilities; European Coalition for Community Living: Brussels, Belgium, 2009. [Google Scholar]
- Gómez, L.E.; Monsalve, A.; Morán, M.; Alcedo, M.; Lombardi, M.; Schalock, R.L. Measurable Indicators of CRPD for People with Intellectual and Developmental Disabilities within the Quality of Life Framework. Int. J. Environ. Res. Public Health 2020, 17, 5123. [Google Scholar] [CrossRef] [PubMed]
- Bigby, C.; Knox, M.; Beadle-Brown, J.; Bould, E. Identifying good group homes: Qualitative indicators using a quality of life framework. Intellect. Dev. Disabil. 2014, 52, 348–366. [Google Scholar] [CrossRef]
- Bigby, C.; Beadle-Brown, J. Improving quality of life outcomes in supported accommodation for people with intellectual disability: What makes a difference? J. Appl. Res. Intellect. Disabil. 2016, 31, e182–e200. [Google Scholar] [CrossRef]
- Felce, D.; Emerson, E. Living with support in a home in the community: Predictors of behavioral development and household and community activity. Ment. Retard. Dev. Disabil. Res. Rev. 2001, 7, 75–83. [Google Scholar] [CrossRef] [PubMed]
- García Iriarte, E.; Stockdale, J.; McConkey, R.; Keogh, F. The role of support staff as people move from congregated settings to group homes and personalized arrangements in Ireland. J. Intellect. Disabil. 2016, 20, 152–164. [Google Scholar] [CrossRef]
- King, E.; Okodogbe, T.; Burke, E.; McCarron, M.; McCallion, P.; O’Donovan, M.A. Activities of daily living and transition to community living for adults with intellectual disabilities. Scand. J. Occup. Ther. 2017, 24, 357–365. [Google Scholar] [CrossRef]
- Mansell, J.; Beadle-Brown, J. Active Support: Enabling and Empowering People with Intellectual Disabilities; Jessica Kingsley Publishers: Philadelphia, PA, USA, 2012. [Google Scholar]
- Thompson, J.R.; Bryant, B.; Campbell, E.M.; Craig, E.M.; Hughes, C.; Rotholtz, D.A. Support Intensity Scale; American Association on Mental Retardation: Washington, DC, USA, 2004. [Google Scholar]
- Asparouhov, T.; Muthén, B. Exploratory structural equation modeling. Struct. Equ. Model. 2009, 16, 397–438. [Google Scholar] [CrossRef]
- Marsh, H.W.; Muthén, B.; Asparouhov, T.; Lüdtke, O.; Robitzsch, A.; Morin, A.J.S.; Trautwein, U. Exploratory structural equation modeling, integrating CFA and EFA: Application to students’ evaluations of university teaching. Struct. Equ. Model. 2009, 16, 439–476. [Google Scholar] [CrossRef]
- Marsh, H.W.; Lüdtke, O.; Muthén, B.; Asparouhov, T.; Morin, A.J.; Trautwein, U.; Nagengast, B. A new look at the big five factor structure through exploratory structural equation modeling. Psychol. Assess. 2010, 22, 471–491. [Google Scholar] [CrossRef] [PubMed]
- Morin, A.J.; Arens, A.K.; Marsh, H.W. A bifactor exploratory structural equation modeling framework for the identification of distinct sources of construct-relevant psychometric multidimensionality. Struct. Equ. Model. Multidiscip. J. 2016, 23, 116–139. [Google Scholar] [CrossRef]
- Beauducel, A.; Herzberg, P.Y. On the performance of maximum likelihood versus means and variance adjusted weighted least squares estimation in CFA. Struct. Equ. Model. 2006, 13, 186–203. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Garrido, L.E.; Barrada, J.R.; Aguasvivas, J.A.; Martínez-Molina, A.; Arias, V.B.; Golino, H.F.; Legaz, E.; Ferrís, G.; Rojo-Moreno, L. Is small still beautiful for the Strengths and Difficulties Questionnaire? Novel findings using exploratory structural equation modeling. Assessment 2020, 27, 1349–1367. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, T.A. Using the modification index and standardized expected parameter change for model modification. J. Exp. Educ. 2012, 80, 26–44. [Google Scholar] [CrossRef]
- Saris, W.E.; Satorra, A.; van der Veld, W.M. Testing structural equation models or detection of misspecifications? Struct. Equ. Model. 2009, 16, 561–582. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2014. [Google Scholar]
- Pallisera, M.; Fullana, J.; Vilà, M.; Castro, M.; Diaz-Garolera, G.; Valls, M.J.; Mejía, P. Diseño de la guía GAS-VI para la evaluación del apoyo a la vida independiente de personas con discapacidad intelectual. Rev. Esp. Discapac. 2020, 8, 79–102. [Google Scholar] [CrossRef]
- Fisher, K.R.; Purcal, C.; Jones, A.; Lutz, D.; Robinson, S.; Kayess, R. What place is there for shared housing with individualized disability support? Disabil. Rehabil. 2019, 43, 1–9. [Google Scholar] [CrossRef]
- Björnsdóttir, K.; Stefánsdóttir, G.V. Double Sexual Standards: Sexuality and People with Intellectual Disabilities Who Require Intensive Support. Sex. Disabil. 2020, 38, 421–438. [Google Scholar] [CrossRef]
- Cuervo, T.; Iglesias, M.T.; Fernández, S. Efectos y beneficios de la Planificación Centrada en la Persona (PCP) en las personas adultas con discapacidad intelectual, en las organizaciones y en la comunidad. Estado de la cuestión. Siglo Cero 2017, 48, 25–40. [Google Scholar] [CrossRef]
- Mata, G.; Carratalá, A. Planificación Centrada en la Persona. Experiencia de la Fundación San Francisco de Borja para Personas con Discapacidad Intelectual; FEAPS: Madrid, Spain, 2007. [Google Scholar]
- Duggan, C.; Linehan, C. The role of ‘natural supports’ in promoting independent living for people with disabilities; A review of existing literature. Br. J. Learn. Disabil. 2013, 41, 199–207. [Google Scholar] [CrossRef]
- Puyaltó, C.; Pallisera, M. Living Independently in Spain: Barriers and Supports from the Views of People with Intellectual Disabilities. Int. J. Disabil. Dev. Educ. 2018, 67, 306–319. [Google Scholar] [CrossRef]
- Deguara, M.; Jelassi, O.; Micallef, B.; Callus, A.M. How we like to live when we have the chance. Br. J. Learn. Disabil. 2012, 40, 123–127. [Google Scholar] [CrossRef]
- Jones, J.L.; Gallus, K.L. Understanding deinstitutionalization: What families value and desire in the transition to community living. Res. Pract. Pers. Sev. Disabil. 2016, 41, 116–131. [Google Scholar] [CrossRef]
- Tabatabaina, M. Listening to families’ views regarding institutionalization & deinstitutionalization. J. Intellect. Dev. Disabil. 2003, 28, 241–259. [Google Scholar]
- Owen, F.; Griffiths, D.M.; Condillac, R. The Ontario Facilities Initiative: Perceptions of the deinstitutionalization process. J. Intellect. Dev. Disabil. 2015, 21, 50–59. [Google Scholar]
- Bigby, C.; Knox, M.; Beadle-Brown, J.; Clement, T.; Mansell, J. Uncovering dimensions of culture in underperforming group homes for people with severe intellectual disability. Intellect. Dev. Disabil. 2012, 50, 452–467. [Google Scholar] [CrossRef]
- Bigby, C.; Fyffe, C. Tensions between institutional closure and deinstitutionalization: What can be learned from Victoria’s institutional redevelopment? Disabil. Soc. 2006, 21, 567–581. [Google Scholar] [CrossRef]
- Otamendi, N.; Navas, P. Calidad de vida de personas con discapacidad intelectual en proceso de envejecimiento en entornos de vivienda. Rev. Esp. Discapac. 2018, 6, 27–47. [Google Scholar] [CrossRef]
- Gómez, L.E.; Schalock, R.L.; Verdugo, M.A. A new paradigm in the field of intellectual and developmental disabilities: Characteristics and evaluation. Psicothema 2021, 33, 28–35. [Google Scholar]
- Schalock, R.L.; Verdugo, M.A.; Gómez, L.E. The Quality of Life Supports Paradigm: Its Description and Application in the Field of Intellectual and Developmental Disabilities. J. Policy. Pract. Intellect. Disabil. 2020, (in press).
- Verdugo, M.A.; Schalock, R.L.; Gómez, L.E. The Quality of Life Supports Model: Twenty-Five Years of Parallel Paths Have Come Together. Siglo Cero. (in press).
- Coll, T.; Comas, J.; Cornellà, A.; Diaz, G.; Fontané, À.; Fullana, J.; González, C.; Martí, P.; Pallisera, M.; Puyalto, C.; et al. “Where to Live and with Whom”. Barriers to and Supports for Independent Living from the Viewpoint of Advisors with Disabilities; Institute of Educational Research, University of Girona: Girona, Spain, 2016. [Google Scholar]
- Bould, E.; Bigby, C.; Iacono, T.; Beadle-Brown, J. Factors associated with increases over time in the quality of Active Support in supported accommodation services for people with intellectual disabilities: A multi-level model. Res. Dev. Disab. 2019, 94, 103477. [Google Scholar] [CrossRef]
- United Nations. General Comment No. 5 (2017) on Living Independently and being Included in the Community. Available online: https://tbinternet.ohchr.org/_layouts/15/treatybodyexternal/Download.aspx?symbolno=CRPD/C/GC/5&Lang=en (accessed on 21 December 2020).
- Verdugo, M.A.; Jenaro, C. Living Independently and Being Included in the Community. 2019. Available online: https://sid.usal.es/idocs/F8/FDO27487/ES_ANED%202018_19.pdf (accessed on 2 March 2021).
- Simmons, B. The phenomenology of intersubjectivity and research with profoundly disabled children: Developing an experiential framework for analysing lived social experiences. In Seen and Heard: Exploring Participation, Engagement and Voice for Children with Disabilities; Twomey, M., Carroll, C., Eds.; Peter Lang: Oxford, UK, 2018. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Variables | ESN * (n = 470) | LSN * (n = 259) | Total (N = 729) |
|---|---|---|---|
| Age | |||
| Range | 18–76 | 20–78 | 18–78 |
| M (SD) | 37.05 (12.79) | 39.06 (12.57) | 37.76 (12.74) |
| Sex | |||
| Male %(n) | 57.4 (270) | 54.8 (142) | 56.5 (412) |
| Female %(n) | 42.6 (200) | 45.2 (117) | 43.5 (317) |
| Diagnosis | |||
| ID %(n) | 51.3 (241) | 76.1 (197) | 60.1 (438) |
| Down Syndrome %(n) | 14.7 (69) | 11.2 (29) | 13.4 (98) |
| Cerebral Palsy %(n) | 16.4 (77) | 4.2 (11) | 12.1 (88) |
| ASD %(n) | 11.1 (52) | 6.9 (18) | 9.6 (70) |
| Other %(n) | 6.6 (31) | 1.5 (4) | 4.8 (35) |
| Severity of ID | |||
| Mild %(n) | 6.8 (32) | 37.5 (97) | 17.7(129) |
| Moderate %(n) | 23.0 (108) | 51.4 (133) | 33.1 (241) |
| Severe %(n) | 50.0 (235) | 9.3 (24) | 35.5 (259) |
| Profound %(n) | 18.9 (89) | 0.4 (1) | 12.3 (90) |
| Unknown %(n) | 1.3 (6) | 1.6. (4) | 1.9 (10) |
| Other disabilities %(n) | 63.0 (296) | 41.7 (108) | 55.4 (404) |
| Residential Setting | |||
| Family (receiving professional support in family home) %(n) | 66.1 (310) | 70.3 (182) | 67.5 (492) |
| Residential facility or nursing home %(n) | 31.5 (148) | 20.8 (54) | 27.7 (202) |
| Group Home %(n) | 2.3 (11) | 8.9(23) | 4.7 (34) |
| Convention Article | Items |
|---|---|
| Article 19. Right to Living Independently and Being Included in the Community | Regularly participates in community activities The person with disability is who ultimately and with the relevant support makes choices and decisions related to aspects of daily living (what clothes to wear, who they interact with, the activities they perform…) The person with disability has chosen the people who are part of his/her personal support circle The organization provides the necessary support so that, if desired, the person may live in his/her home, regardless of age or disability |
| Article 22. Respect for Privacy | The person has decided who may access his/her personal information The person has a private and intimate space inside the place where he/she lives The person’s privacy and intimacy are respected in the services provided by the organization (e.g., knocking before entering, closing the door when showering the person, when the person is using the toilet, etc.) |
| Article 26. Habilitation and Rehabilitation | The person’s interests are closely observed to provide activities that may respond to the person’s preferences The aim of the support provided by the organization’s professionals is that the person may achieve growing levels of participation in daily activities The approach of the individual support plan is multidimensional and holistic to improve the person’s quality of life The individual support plan includes clear strategies and enough supports to enable the person’s inclusion in ordinary settings |
| Item/Factor | F1 | F2 | F3 | iECV |
|---|---|---|---|---|
| A1 | 0.47 | −0.04 | 0.28 | 0.73 |
| A2 | 0.60 | 0.15 | 0.07 | 0.93 |
| A3 | 0.94 | −0.01 | −0.04 | 0.99 |
| A4 | 0.48 | 0.28 | 0.00 | 0.75 |
| B1 | 0.26 | 0.44 | −0.02 | 0.74 |
| B2 | 0.01 | 0.74 | 0.05 | 0.99 |
| B3 | 0.02 | 0.68 | 0.10 | 0.98 |
| C1 | −0.08 | 0.06 | 0.89 | 0.99 |
| C2 | 0.11 | −0.02 | 0.85 | 0.98 |
| C3 | −0.11 | 0.05 | 0.84 | 0.98 |
| C4 | 0.14 | −0.06 | 0.75 | 0.96 |
| ω | 0.70 | 0.66 | 0.90 |
| Covariable | Model | df | CS | RMSEA | CFI | TLI |
|---|---|---|---|---|---|---|
| Sex | Saturated | 24 | 70 | 0.055 | 0.992 | 0.979 |
| Invariant | 32 | 71 | 0.044 | 0.994 | 0.987 | |
| Null | 35 | 53 | 0.029 | 0.997 | 0.994 | |
| Age | Saturated | 24 | 67 | 0.056 | 0.993 | 0.980 |
| Invariant | 32 | 65 | 0.042 | 0.994 | 0.988 | |
| Null | 35 | 54 | 0.031 | 0.997 | 0.994 | |
| Support needs | Saturated | 24 | 71 | 0.055 | 0.993 | 0.979 |
| Invariant | 32 | 84 | 0.051 | 0.992 | 0.983 | |
| Partial invariant | 31 | 72 | 0.046 | 0.993 | 0.986 | |
| Null | 35 | 126 | 0.064 | 0.986 | 0.973 | |
| Disability | Saturated | 24 | 65 | 0.053 | 0.993 | 0.981 |
| Invariant | 32 | 75 | 0.047 | 0.993 | 0.985 | |
| Null | 35 | 66 | 0.038 | 0.995 | 0.990 | |
| Comorbidity | Saturated | 24 | 72 | 0.056 | 0.992 | 0.979 |
| Invariant | 32 | 77 | 0.047 | 0.993 | 0.985 | |
| Null | 35 | 59 | 0.033 | 0.996 | 0.993 | |
| Home | Saturated | 24 | 72 | 0.056 | 0.992 | 0.975 |
| Invariant | 40 | 81 | 0.040 | 0.993 | 0.987 | |
| Null | 46 | 139 | 0.056 | 0.985 | 0.975 |
| Model | df | CS | RMSEA | CFI | TLI |
|---|---|---|---|---|---|
| Exhaustive | 79 | 108 | 0.026 | 0.994 | 0.991 |
| Parsimonious | 74 | 128 | 0.027 | 0.995 | 0.992 |
| Interaction | 107 | 131 | 0.020 | 0.996 | 0.994 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Esteban, L.; Navas, P.; Verdugo, M.Á.; Arias, V.B. Community Living, Intellectual Disability and Extensive Support Needs: A Rights-Based Approach to Assessment and Intervention. Int. J. Environ. Res. Public Health 2021, 18, 3175. https://doi.org/10.3390/ijerph18063175
Esteban L, Navas P, Verdugo MÁ, Arias VB. Community Living, Intellectual Disability and Extensive Support Needs: A Rights-Based Approach to Assessment and Intervention. International Journal of Environmental Research and Public Health. 2021; 18(6):3175. https://doi.org/10.3390/ijerph18063175
Chicago/Turabian StyleEsteban, Laura, Patricia Navas, Miguel Ángel Verdugo, and Víctor B. Arias. 2021. "Community Living, Intellectual Disability and Extensive Support Needs: A Rights-Based Approach to Assessment and Intervention" International Journal of Environmental Research and Public Health 18, no. 6: 3175. https://doi.org/10.3390/ijerph18063175
APA StyleEsteban, L., Navas, P., Verdugo, M. Á., & Arias, V. B. (2021). Community Living, Intellectual Disability and Extensive Support Needs: A Rights-Based Approach to Assessment and Intervention. International Journal of Environmental Research and Public Health, 18(6), 3175. https://doi.org/10.3390/ijerph18063175