
Examining the Associations between Indigenous Rangers, Culture and Wellbeing in Australia, 2018–2020

 ,
,  , ,
, ,
Abstract
1. Introduction
The Mayi Kuwayu Study and Proof-of-Concept Study
- examine if associations between Ranger status and health and wellbeing continue to be observed in Central Australia;
- examine if the associations between Ranger status and health and wellbeing are observed among non-Central Australian Rangers; and,
- determine the mediating effect of Indigenous cultural factors and Ranger status on wellbeing outcomes.
2. Methods
2.1. Mayi Kuwayu Study
2.2. Participant Eligibility
2.3. Variables
2.3.1. Wellbeing Outcome Measures
2.3.2. Covariates
2.3.3. Cultural Factors
2.4. Statistical Analysis
Mediation Analysis
- ≥a little bit included the groupings “a little bit, a fair bit, a lot” (1) and “want to but can’t, not at all” (0);
- ≥a fair bit included the groupings “a fair bit, a lot” (1) and “want to but can’t, not at all, a little bit” (0); and,
- a lot included the groupings “a lot” (1) and “want to but can’t, not at all, a little bit, a fair bit” (0).
2.5. Ethics and Data Use Approval
3. Results
3.1. Participant Characteristics
Socioeconomic
3.2. Cultural Factors
3.3. Wellbeing Outcomes of Rangers Compared to Non-Rangers, by Location
3.3.1. Central Australia
3.3.2. Non-Central Australia
3.4. Mediation between Ranger, Culture and Wellbeing Outcomes
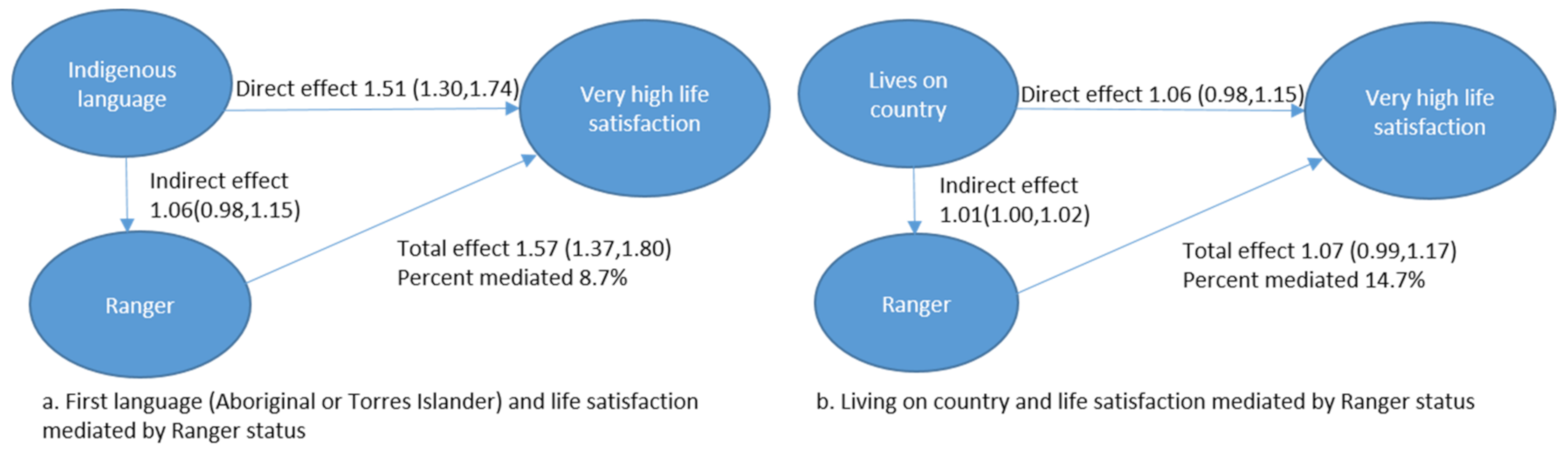
3.4.1. Cultural Factors Mediating the Association between Ranger Status and Very High Life Satisfaction
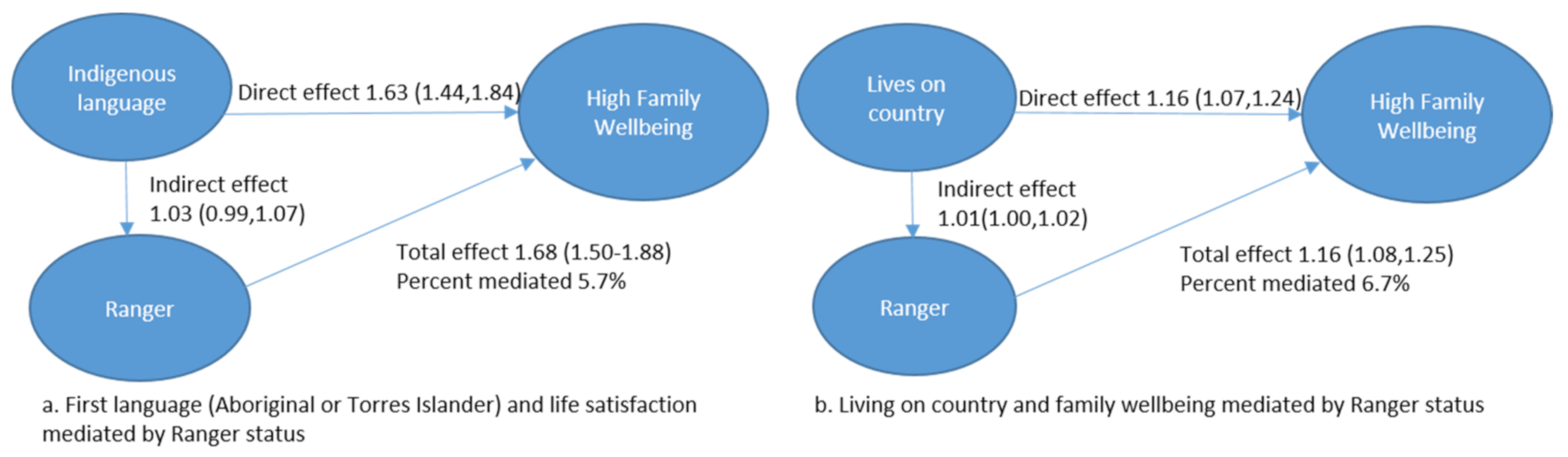
3.4.2. Cultural Factors Mediating the Association between Ranger Status and High Family Wellbeing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourke, S.; Wright, A.; Guthrie, J.; Russell, L.; Dunbar, T.; Lovett, R. Evidence Review of Indigenous Culture for Health and Wellbeing. Int. J. Health Wellness Soc. 2018, 8, 11–27. [Google Scholar] [CrossRef]
- Burgess, C.P.; Johnston, F.H.; Berry, H.L.; McDonnell, J.; Yibarbuk, D.; Gunabarra, C.; Mileran, A.; Bailie, R.S. Healthy country, healthy people: The relationship between Indigenous health status and “caring for country”. Med. J. Aust. 2009, 190, 567–572. [Google Scholar] [CrossRef] [PubMed]
- McDermott, R.; O’Dea, K.; Rowley, K.; Knight, S.; Burgess, P. Beneficial impact of the homelands movement on health outcomes in central Australian Aborigines. Aust. N. Z. J. Public Health 1998, 22, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Rowley, K.G.; O’Dea, K.; Anderson, I.; McDermott, R.; Saraswati, K.; Tilmouth, R.; Roberts, I.; Fitz, J.; Wang, Z.; Jenkins, A.; et al. Lower than expected morbidity and mortality for an Australian Aboriginal population: 10-year follow-up in a decentralised community. Med. J. Aust. 2008, 188, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Biddle, N.; Swee, H. The relationship between wellbeing and Indigenous land, language and culture in Australia. Aust. Geogr. 2012, 43, 215–232. [Google Scholar] [CrossRef]
- Dorais, L.-J. Language, Culture and Identity: Some Inuit Examples. Can. J. Nativ. Stud. 1995, 15, 293–308. [Google Scholar]
- Oster, R.T.; Grier, A.; Lightning, R.; Mayan, M.J.; Toth, E.L. Cultural continuity, traditional Indigenous language, and diabetes in Alberta First Nations: A mixed methods study. Int. J. Equity Health 2014, 13, 92. [Google Scholar] [CrossRef]
- Hallett, D.; Chandler, M.J.; Lalonde, C.E. Aboriginal language knowledge and youth suicide. Cogn. Dev. 2007, 22, 392–399. [Google Scholar] [CrossRef]
- Chandler, M.J.; Lalonde, C.E. Transferring whose Knowledge? Exchanging Whose Best Practices? On Knowing about Indigenous Knowledge and Aboriginal Suicide. In Aboriginal Policy Research; Beavan, D., White, J., Eds.; Althouse Press: London, ON, Canada, 2006. [Google Scholar]
- Durie, M. Understanding health and illness: Research at the interface between science and indigenous knowledge. Int. J. Epidemiol. 2004, 33, 1138–1143. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.A.; Dewar, J. Traditional Indigenous Approaches to Healing and the modern welfare of Traditional Knowledge, Spirituality and Lands: A critical reflection on practices and policies taken from the Canadian Indigenous Example. Int. Indig. Policy J. 2011, 2. [Google Scholar] [CrossRef]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, P.R.; Bang, A.; Coimbra, P.C.E.A., Jr.; et al. Indigenous and tribal peoples’ health: A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Kingsley, J.; Townsend, M.; Henderson-Wilson, C.; Bolam, B. Developing an Exploratory Framework Linking Australian Aboriginal Peoples’ Connection to Country and Concepts of Wellbeing. Int. J. Environ. Res. Public Health 2013, 10, 678–698. [Google Scholar] [CrossRef] [PubMed]
- Parter, C.; Wilson, S.; Hartz, D.L. The Closing the Gap (CTG) Refresh: Should Aboriginal and Torres Strait Islander culture be incorporated in the CTG framework? How? Aust. N. Z. J. Public Health 2019, 43, 5–7. [Google Scholar] [CrossRef]
- Matsumoto, D. Culture and Modern Life; Thomson Brooks, Cole Publishing Co.: Belmont, CA, USA, 1997. [Google Scholar]
- Green, J.W. Cultural Awareness in the Human Services: A Multi-Ethnic Approach, 3rd ed.; Allyn and Bacon: Toronto, ON, Canada, 1999. [Google Scholar]
- United Nations. United Nations Declaration of the Rights of the Indigenous Peoples; United Nations: New York, NY, USA, 2007. [Google Scholar]
- Salmon, M.; Doery, K.; Dance, P.; Chapman, J.; Gilbert, R.; Williams, R.; Raymond, L. Defining the Indefinable: Descriptors of Aboriginal and Torres Strait Islander Peoples’ Cultures and Their Links to Health and Wellbeing; Australian National University: Canberra, Australia, 2018. [Google Scholar]
- Australian Government. Coalition of Aboriginal Peak Organisations. National Partnership Agreeement on Closing the Gap; ACT, Australian Government: Canberra, Australia, 2020.
- Australian Government. National Aboriignal and Torres Strait Islander Health Plan 2013–2023. In Department of Health; ACT: Canberra, Australia, 2013. [Google Scholar]
- Department of Social Services. Closing the Gap of Inidgenous Australians: Working on Country Indigenous Rangers; Department of Social Services Budget, Australian Government: Canberra, Australia, 2020.
- Garnett, S.T.; Burgess, C.P.; Johnston, F.H.; Lea, T. Healthy Country, Healthy People: Policy Implications of Links between Indigenous Human Health and Environmental Condition in Tropical Australia. Aust. J. Public Adm. 2009, 68, 53–66. [Google Scholar] [CrossRef]
- Larson, S.; Stoeckl, N.; Jarvis, D.; Addison, J.; Grainger, D.; Watkin Lui, F. Indigenous land and sea management programs (ILSMPs) enhance the wellbeing of Indigenous Australians. Int. J. Environ. Res. Public Health 2020, 17, 125. [Google Scholar] [CrossRef]
- Jones, R.; Thurber, K.A.; Chapman, J.; D’Este, C.; Dunbar, T.; Wenitong, M.; Eades, S.J.; Strelein, L.; Davey, M.; Du, W.; et al. Study protocol: Our Cultures Count, the Mayi Kuwayu Study, a national longitudinal study of Aboriginal and Torres Strait Islander wellbeing. BMJ Open 2018, 8, e023861. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Thurber, K.; Wright, A.; Chapman, J.; Donohoe, P.; Davis, V.; Lovett, R. Associations between Participation in a Ranger Program and Health and Wellbeing Outcomes among Aboriginal and Torres Strait Islander People in Central Australia: A Proof of Concept Study. Int. J. Environ. Res. Public Health 2018, 15, 1478. [Google Scholar] [CrossRef]
- Wright, A.; Thurber, K.A.; Yap, M.; Du, W.; Banks, E.; Walker, J.; Irwin, F.; Sanders, W.; Lovett, R. Who responds? An examination of response rates to a national postal survey of Aboriginal and Torres Strait Islander adults, 2018–2019. BMC Med. Res. Methodol. 2020, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Bombak, A.E. Self-rated health and public health: A critical perspective. Front. Public Health 2013, 1, 15. [Google Scholar] [CrossRef]
- McNamara, B.J.; Banks, E.; Gubhaju, L.; Williamson, A.; Joshy, G.; Raphael, B.; Eades, S.J. Measuring psychological distress in older Aboriginal and Torres Strait Islanders Australians: A comparison of the K-10 and K-5. Aust. N. Z. J. Public Health 2014, 38, 567–573. [Google Scholar] [CrossRef]
- Silburn, S. Strengthening the Capacity of Aboriginal Children, Families and Communities; Curtin University of Technology & Telethon Institute for Child Health Research Perth: Nedlands, Australia, 2006. [Google Scholar]
- Australian Bureau of Statistics. 1270.0.55.005—Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, July 2016 Canberra, ACT, Australia: ABS. 2018. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Latestproducts/1270.0.55.005Main%20Features1July%202016?opendocument&tabname=Summary&prodno=1270.0.55.005&issue=July%202016&num=&view= (accessed on 21 November 2020).
- Jones, R.; Chapman, J.; Lovett, R. Mayi Kuwayu Development: Summary Report; Aboriginal and Torres Strait Islander Health Team, Research School of Population Health, Australian National University: Canberra, Australia, 2019. [Google Scholar]
- Richardson, D.B.; Kinlaw, A.C.; MacLehose, R.F.; Cole, S.R. Standardized binomial models for risk or prevalence ratios and differences. Int. J. Epidemiol. 2015, 44, 1660–1672. [Google Scholar] [CrossRef] [PubMed]
- Walsh, F.; Holmes, M. ‘Good Things that Come to Us’: Benefits and Challenges of the CLC Ranger Program from the View of Aboriginal Rangers; Evaluation report for the Central Land Council; Central Land Council: Alice Springs, Australia, 2017. [Google Scholar]
- Kingsley, J.Y.; Townsend, M.; Phillips, R.; Aldous, D. “If the land is healthy… it makes the people healthy”: The relationship between caring for Country and health for the Yorta Yorta Nation, Boonwurrung and Bangerang Tribes. Health Place 2009, 15, 291–299. [Google Scholar] [CrossRef]
- Schultz, R.; Abbott, T.; Yamaguchi, J.; Cairney, S. Australian Indigenous Land Management, Ecological Knowledge and Languages for Conservation. EcoHealth 2019, 16, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Cartographer Indigenous Protected Areas and Commonwealth Funded Indigenous Ranger Groups-February 2020; National Indigenous Australians Agency: Canberra, Australia, 2020.
- Markham, F.; Biddle, N. Income, Poverty and Inequality; ACT, Centre for Aboriginal Economic Policy Research (CAEPR): Canberra, Australia, 2018. [Google Scholar]
- Australian Institue of Health and Welfare. Measuring the Social and Emotional Wellbeing of Aboriginal and Torres Striat Islander Peoples; AIHW: Canberra, Australia, 2009. [Google Scholar]
- Brinckley, M.-M.; Calabria, B.; Walker, J.; Thurber, K.A.; Lovett, R. Reliability, validity, clinical utility of a culturally modified Kessler Scale (MK-K5) in the Aboriginal and Torres Strait Islander Population (under review).
- Le Grande, M.; Ski, C.F.; Thompson, D.R.; Scuffham, P.; Kularatna, S.; Jackson, A.C.; Brown, A. Social and emotional wellbeing assessment instruments for use with Indigenous Australians: A critical review. Soc. Sci. Med. 2017, 187, 164–173. [Google Scholar] [CrossRef]
- Kowal, E. Is culture the problem or the solution? Outstation health and the politics of remoteness. In Culture Crisis; Altman, J., Hinkson, M., Eds.; Anthropology and Politics in Aboriginal Australia, University of New South Wales: Sydney, Australia, 2010; pp. 179–194. [Google Scholar]
- Schultz, R.; Cairney, S. Caring for country and the health of Aboriginal and Torres Strait Islander Australians. Med. J. Aust. 2017, 207, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.; Campbell, D. Translating Aboriginal Land Rights into Development Outcomes: Factors Contributing to a Successful Program in Central Australia; Cenre for Aboriginal Economic Policy Research: Canberra, Australia, 2016. [Google Scholar]
- National Native Title Tribunal. Indigenous Estates: Land Granted under Specified Indigenous Land Granted Instruments Canberra: Geospatial Services, National Native Title Tribunal. 2020. Available online: http://www.nntt.gov.au/Maps/Indigenous_Estates_and_Determinations_A1L.pdf (accessed on 12 October 2020).
- Hunt, J. ‘Caring for country’: A review of Aboriginal engagement in environmental management in New South Wales. Australas. J. Environ. Manag. 2012, 19, 213–226. [Google Scholar] [CrossRef]
- Hudson, S. Charlatan Training: How Aboriginal Health Workers Are Being Short-Changed; Centre for Independent Studies: Sydney, Australia, 2012. [Google Scholar]
- Hughes, H. Lands of Shame: Aboriginal and Torres Strait Islander “Homelands” in Transition; Centre for Independent Studies: Sydney, Australia, 2007. [Google Scholar]
- Austin-Broos, D. A Different Inequality: The Politics of Debate about Remote Aboriginal Australia; Allen & Unwin: Crows Nest, Australia, 2011. [Google Scholar]
- Dockery, A.M. Inter-generational transmission of Indigenous culture and children’s wellbeing: Evidence from Australia. Int. J. Intercult. Relat. 2020, 74, 80–93. [Google Scholar] [CrossRef]
- Colquhoun, S.; Dockery, A.M. The Link between Indigenous Culture and Wellbeing: Qualitative Evidence for Australian Aboriginal Peoples; The Centre for Labour Market Research, Curtin Business School, Curtin University; Curtin Business School; Curtin University: Perth, Australia, 2012. [Google Scholar]
- Central Land Council. CLC Rangers: The Benefits of Ranger Work; Central Land Council: Alice Springs, Australia, 2018. [Google Scholar]



{kind=link}
{kind=link}
| Study Elements | 2017 Proof of Concept Study [25] | Current Study—Using Mayi Kuwayu Data |
|---|---|---|
| Sample size | Total sample: 203 43 Rangers: 160 non-Rangers | Central Australia participants: 102 Rangers, 494 non-Rangers, total 596.non-Central Australia participants: 164 Rangers, 8931 non-Rangers, total 9095 Total participants: 266 rangers: 9425 non-Rangers, total 9691 |
| Geographical coverage | Central Australia | National, includes participants in all states and remoteness areas. The analysis focuses on Central Australia compared to non-Central Australia. |
| Recruitment process | Field-based recruitment | Postal Field-based recruitment |
| Outcome variables | Psychological Wellbeing (K5) Life satisfaction General Health Family wellbeing | Psychological wellbeing (K5) Life satisfaction * General Health Family wellbeing * |
| Adjustment variables | Financial status (income) Employment Education Health risk factor score Health condition score | Family financial status * Employment Education Health risk factor score Health condition score |
| Covariates | Gender | Gender, age Remoteness (non-Central Australia) |
| Mediation analysis | Not included | Language: first language, confidence in speaking language, intensity of speaking language Connection to country: Lives on country, spends time on country, has cultural responsibilities for country. |
| % (n) | Geographic Location | Total | |||||
|---|---|---|---|---|---|---|---|
| Central Australia | Non-Central Australia | ||||||
| Non-Ranger | Ranger * | Non-Ranger | Ranger * | Non-Ranger | Ranger * | Total | |
| n = 494 | n = 102 | n = 8931 | n = 164 | n = 9425 | n = 266 | n = 9691 | |
| Gender | |||||||
| Male | 32.2% (159) | 61.8% (63) | 37.5% (3351) | 63.4% (104) | 37.2% (3510) | 62.8% (167) | 37.9% (3677) |
| Female | 63.0% (311) | 33.3% (34) | 60.1% (5364) | 32.9% (54) | 60.2% (5675) | 33.1% (88) | 59.5% (5763) |
| Missing | 4.9% (24) | 4.9% (5) | 2.4% (216) | 3.7% (6) | 2.5% (240) | 4.1% (11) | 2.6% (251) |
| Age group | |||||||
| 16–34 | 41.3% (204) | 44.1% (45) | 29.4% (2629) | 26.2% (43) | 30.1% (2833) | 33.1% (88) | 30.1% (2921) |
| 35–54 | 39.1% (193) | 39.2% (40) | 30.3% (2707) | 39.0% (64) | 30.8% (2900) | 39.1% (104) | 31.0% (3004) |
| <54 | 19.6% (97) | 16.7% (17) | 40.3% (3595) | 34.8% (57) | 39.2% (3692) | 27.8% (74) | 38.9% (3766) |
| Missing | 5.3% (26) | 7.3% (12) | 8.5% (756) | 7.3% (12) | 8.3% (808) | 7.1% (19) | 8.4% (789) |
| Employment | |||||||
| unemployed | 56.9% (281) | 19.6% (20) | 46.6% (4164) | 46.3% (76) | 47.2% (4445) | 36.1% (96) | 46.9% (4541) |
| employed | 43.1% (213) | 80.4% (82) | 53.4% (4767) | 53.7% (88) | 52.8% (4980) | 63.9% (170) | 53.1% (5150) |
| Financial Status | |||||||
| Low | 20.0% (99) | 18.6% (19) | 15.5% (1380) | 18.3% (30) | 15.7% (1479) | 18.4% (49) | 15.8% (1528) |
| Medium | 54.7% (270) | 57.8% (59) | 68.6% (6131) | 65.9% (108) | 67.9% (6401) | 62.8% (167) | 67.8% (6568) |
| High | 3.0% (15) | ≤19.6% (≤20) | 6.1% (549) | 6.7% (11) | 6.0% (564) | 5.6% (15) | 6.0% (579) |
| Missing or unsure | 22.3% (110) | ≤19.6% (≤20) | 9.8% (871) | 9.1% (15) | 10.4% (981) | 13.2% (35) | 10.5% (1016) |
| Education level | |||||||
| Yr 10 or less | 66.6% (329) | 61.8% (63) | 43.4% (3880) | 43.9% (72) | 44.7% (4209) | 50.8% (135) | 44.8% (4344) |
| Yr 12, Trade or Tertiary | 24.3% (120) | 32.4% (33) | 37.2% (3324) | 33.5% (55) | 36.5% (3444) | 33.1% (88) | 36.4% (3532) |
| University | 3.8% (19) | ≤4.9% (≤5) | 17.5% (1560) | 21.3% (35) | 16.8% (1579) | 14.7% (39) | 16.7% (1618) |
| Missing | 5.3% (26) | ≤4.9% (≤5) | 1.9% (167) | 1.2% (2) | 2.0% (193) | 1.5% (4) | 2.0% (197) |
| Remoteness Area | |||||||
| major cities | 0 | 0 | 44.3% (3958) | 22.0% (36) | 42.0% (3958) | 13.5% (36) | 41.2% (3994) |
| inner regional | 0 | 0 | 30.7% (2741) | 26.8% (44) | 29.1% (2741) | 16.5% (44) | 28.7% (2785) |
| outer regional | 1.8% (9) | ≤4.9% (≤5) | 19.4% (1734) | 31.1% (51) | 18.5% (1743) | 19.5% (52) | 18.5% (1795) |
| remote | 29.8% (147) | 11.8% (12) | 1.6% (140) | 8.5% (14) | 3.0% (287) | 9.8% (26) | 3.2% (313) |
| very remote | 65.4% (323) | 84.3% (86) | 2.5% (224) | 7.9% (13) | 5.8% (547) | 37.2% (99) | 6.7% (646) |
| missing | 3.0% (15) | ≤4.9% (≤5) | 1.5% (134) | 3.7% (6) | 1.6%(149) | 3.4% (9) | 1.6% (158) |
| Geographic Location | Total | ||||||
|---|---|---|---|---|---|---|---|
| Central Australia Ranger Status | Non-Central Australia Ranger Status | ||||||
| Non-Ranger | Ranger * | Non-Ranger | Ranger * | Non-Ranger | Ranger * | Total | |
| n = 494 | n = 102 | n = 8931 | n = 164 | n = 9425 | n = 266 | n = 9691 | |
| What is your first language? | |||||||
| English or other | 36.2% (179) | 23.5% (24) | 93.5% (8353) | 81.1% (133) | 90.5% (8532) | 59.0% (157) | 89.7% (8689) |
| Aboriginal/Torres Strait Islander | 56.1% (277) | 61.8% (63) | 2.8% (251) | 8.5% (14) | 5.6% (528) | 28.9% (77) | 6.2% (605) |
| Missing | 7.7% (38) | 14.7% (15) | 3.7% (327) | 10.4% (17) | 3.9% (365) | 12.0% (32) | 4.1% (397) |
| Do you speak any Aboriginal/Torres Strait Islander language? | |||||||
| No | 17.6% (87) | 6.9% (7) | 64.0% (5713) | 25.6% (42) | 61.5% (5800) | 18.4% (49) | 60.4% (5849) |
| Yes, a little bit | 24.3% (120) | 22.5% (23) | 27.8% (2487) | 50.6% (83) | 27.7% (2607) | 39.8% (106) | 28.0% (2713) |
| Yes, a fair bit | 9.1% (45) | 6.9% (7) | 2.8% (253) | 14.6% (24) | 3.2% (298) | 11.7% (31) | 3.4% (329) |
| Yes, a lot | 41.9% (207) | 55.9% (57) | 1.4% (123) | 5.5% (9) | 3.5% (330) | 24.8% (66) | 4.1% (396) |
| Missing | 7.1% (35) | 7.8% (8) | 4.0% (355) | 3.7% (6) | 4.1% (390) | 5.3% (14) | 4.2% (404) |
| I am confident in speaking language. | |||||||
| Want to but can’t | 6.9% (34) | 2.0% (2) | 26.6% (2377) | 16.5% (27) | 25.6% (2411) | 10.9% (29) | 25.2% (2440) |
| Not at all | 7.3% (36) | 4.9% (5) | 27.7% (2478) | 9.8% (16) | 26.7% (2514) | 7.9% (21) | 26.2% (2535) |
| A little bit | 16.8% (83) | 17.6% (18) | 15.4% (1377) | 34.1% (56) | 15.5% (1460) | 27.8% (74) | 15.8% (1534) |
| A fair bit | 7.3% (36) | 6.9% (7) | 4.8% (429) | 13.4% (22) | 4.9% (465) | 10.9% (29) | 5.1% (494) |
| A lot | 53.2% (263) | 63.7% (65) | 3.9% (350) | 13.4% (22) | 6.5% (613) | 32.7% (87) | 7.2% (700) |
| Unsure | 3.0% (15) | 1.0% (1) | 8.2% (730) | 3.0% (5) | 7.9% (745) | 2.3% (6) | 7.7% (751) |
| Missing | 5.5% (27) | 3.9% (4) | 13.3% (1190) | 9.8% (16) | 12.9% (1217) | 7.5% (20) | 12.8% (1237) |
| Do you currently live on your country/Island? | |||||||
| no/unsure | 51.6% (255) | 41.2% (42) | 68.2% (6094) | 51.2% (84) | 67.4% (6349) | 47.4% (126) | 66.8% (6475) |
| yes | 43.9% (217) | 52.9% (54) | 28.2% (2521) | 43.9% (72) | 29.1% (2738) | 47.4% (126) | 29.6% (2864) |
| Missing | 4.5% (22) | 5.9% (6) | 3.5% (316) | 4.9% (8) | 3.6% (338) | 5.3% (14) | 3.6% (352) |
| How much time do you spend on country? | |||||||
| Want to but can’t | 4.0% (20) | 0.0% (0) | 16.2% (1450) | 11.0% (18) | 15.6% (1470) | 6.8% (18) | 15.4% (1488) |
| Not at all | 9.3% (46) | 0.0% (0) | 27.5% (2454) | 6.1% (10) | 26.5% (2500) | 3.8% (10) | 25.9% (2510) |
| A little bit | 19.6% (97) | 5.9% (6) | 28.1% (2510) | 25.6% (42) | 27.7% (2607) | 18.0% (48) | 27.4% (2655) |
| A fair bit | 16.6% (82) | 22.5% (23) | 11.1% (989) | 22.6% (37) | 11.4% (1071) | 22.6% (60) | 11.7% (1131) |
| A lot | 42.5% (210) | 65.7% (67) | 8.3% (743) | 29.3% (48) | 10.1% (953) | 43.2% (115) | 11.0% (1068) |
| Missing | 7.9% (39) | 5.9% (6) | 8.8% (785) | 5.5% (9) | 8.7% (824) | 5.6% (15) | 8.7% (839) |
| Do you have cultural responsibility for country? | |||||||
| no cultural responsibilities for country | 31.8% (157) | 17.6% (18) | 75.8% (6767) | 42.1% (69) | 73.5% (6924) | 32.7% (87) | 72.3% (7011) |
| cultural responsibilities for country | 68.2% (337) | 82.4% (84) | 24.2% (2164) | 57.9% (95) | 26.5% (2501) | 67.3% (179) | 27.7% (2680) |
| Non-Ranger (Reference Group) 1.0 | Central Australia | Non-Central Australia | ||||
|---|---|---|---|---|---|---|
| n | PR | 95% CI | n | PR | 95% CI | |
| Very high life satisfaction | 556 | 1.31 | 1.09,1.57 | 8811 | 1.29 | 1.06,1.57 |
| adjusted for education | 556 | 1.32 | 1.09,1.58 | 8811 | 1.28 | 1.05,1.56 |
| adjusted for financial status | 556 | 1.28 | 1.07,1.55 | 8811 | 1.26 | 1.05,1.50 |
| adjusted for employment | 556 | 1.35 | 1.13,1.62 | 8811 | 1.32 | 1.08,1.60 |
| adjusted for health condition score | 556 | 1.29 | 1.07,1.55 | 8811 | 1.34 | 1.10,1.63 |
| adjusted for risk factor score | 556 | 1.29 | 1.07,1.55 | 8811 | 1.33 | 1.10,1.61 |
| adjusted for remoteness | 8811 | 1.31 | 1.08,1.60 | |||
| Very good general health | 572 | 1.06 | 0.98,1.15 | 8868 | 1.02 | 0.91,1.13 |
| adjusted for education | 554 * | 1.07 | 0.98,1.16 | 8868 | 0.99 | 0.89,1.09 |
| adjusted for financial status | 553 * | 1.05 | 0.97,1.15 | 8868 | 0.98 | 0.89,1.07 |
| adjusted for employment | 572 | 1.06 | 0.97,1.16 | 8868 | 1.01 | 0.92,1.11 |
| adjusted for health condition score | 572 | 1.06 | 0.98,1.15 | 8868 | 1.04 | 0.94,1.14 |
| adjusted for risk factor score | 528 * | 1.07 | 0.98,1.17 | 8868 | 1.04 | 0.95,1.15 |
| adjusted for remoteness | 8868 | 1.02 | 0.92,1.13 | |||
| High psychological wellbeing | 510 | 0.87 | 0.66,1.15 | 8240 | 1.05 | 0.92,1.21 |
| adjusted for education | 510 | 0.95 | 0.71,1.27 | 8240 | 1.08 | 0.94,1.23 |
| adjusted for financial status | 510 | 0.96 | 0.72,1.28 | 8240 | 1.02 | 0.90,1.16 |
| adjusted for employment | 510 | 0.91 | 0.68,1.22 | 8240 | 1.07 | 0.94,1.22 |
| adjusted for health condition score | 510 | 0.95 | 0.72,1.26 | 8240 | 1.05 | 0.89,1.24 |
| adjusted for risk factor score | 510 | 0.96 | 0.72,1.27 | 8240 | 1.05 | 0.92,1.20 |
| adjusted for remoteness | 8240 | 1.09 | 0.95,1.25 | |||
| High family wellbeing | 538 | 1.17 | 1.01,1.36 | 8465 | 1.37 | 1.14,1.65 |
| adjusted for education | 538 | 1.35 | 1.15,1.58 | 8465 | 1.36 | 1.17,1.59 |
| adjusted for financial status | 538 | 1.18 | 1.01,1.38 | 8465 | 1.37 | 1.18,1.58 |
| adjusted for employment | 538 | 1.23 | 1.05,1.43 | 8465 | 1.38 | 1.18,1.61 |
| adjusted for health condition score | 538 | 1.20 | 1.03,1.39 | 8465 | 1.38 | 1.18,1.62 |
| adjusted for risk factor score | 538 | 1.21 | 1.04,1.41 | 8465 | 1.39 | 1.19,1.63 |
| adjusted for remoteness | 8465 | 1.33 | 1.14,1.56 | |||
| Mediator | Natural Direct Effect * | Natural Indirect Effect * | Total Effect * | % Mediated |
|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | ||
| Do you speak any Aboriginal/Torres Strait Islander words/language? | ||||
| ≥A little bit | 1.39 (1.06,1.85) | 1.06 (0.89,1.36) | 1.54 (1.27,1.85) | 13.5% |
| ≥A fair bit | 1.35 (0.99,1.83) | 1.13 (0.98,1.30) | 1.54 (1.27,1.88) | 28.3% |
| A lot | 1.32 (1.04,1.66) | 1.17 (1.02,1.33) | 1.54 (1.27,1.88) | 36.4% |
| Are you confident in speaking your Aboriginal language? | ||||
| ≥A little bit | 1.22 (0.92,1.62) | 1.32 (1.04,1.66) | 1.61 (1.32,1.96) | 58.3% |
| ≥A fair bit | 1.26 (0.97,1.62) | 1.29 (1.07,1.46) | 1.62 (1.32,1.97) | 47.9% |
| A lot | 1.32(1.04,1.68) | 1.22 (1.04,1.67) | 1.61 (1.32,1.96) | 41.8% |
| Has cultural responsibilities for country? | ||||
| Yes | 1.48 (1.14,1.90) | 1.05 (0.89,1.25) | 1.56 (1.29,1.88) | 11.0% |
| How much time do you spend on country? | ||||
| ≥A little bit | 1.24 (0.94,1.95) | 1.25 (1.02,1.51) | 1.55 (1.27,1.88) | 50.9% |
| ≥A fair bit | 1.11 (0.88,1.50) | 1.38 (1.11,1.72) | 1.54(1.27,1.88) | 74.6% |
| A lot | 1.12 (0.87,1.46) | 1.37 (1.14,2.12) | 1.55(1.28,1.88) | 71.8% |
| Mediator | Natural Direct Effect * | Natural Indirect Effect * | Total Effect * | % Mediated |
|---|---|---|---|---|
| PR (95% CI) | PR (95% CI) | PR (95% CI) | ||
| Do you speak any Aboriginal/Torres Strait Islander words/language? | ||||
| ≥A little bit | 1.39 (1.01,1.59) | 1.11 (0.91,1.37) | 1.54 (1.29,1.84) | 24.2% |
| ≥A fair bit | 1.37 (1.11,1.69) | 1.07 (0.96,1.23) | 1.54(1.29,1.84) | 15.7% |
| A lot | 1.40 (1.16,1.71) | 1.06 (0.96,1.17) | 1.54 (1.29,1.84) | 13.5% |
| Are you confident in speaking your Aboriginal language? | ||||
| ≥A little bit | 1.39 (1.06,1.81) | 1.14 (0.93,1.40) | 1.58 (1.32,1.88) | 28.6% |
| ≥A fair bit | 1.46 (1.17,1.82) | 1.08 (0.94,1.23) | 1.58 (1.32,1.88) | 16.8% |
| A lot | 1.49 (1.21,1.83) | 1.06 (0.95,1.18) | 1.58 (1.32,1.88) | 12.7% |
| Has cultural responsibilities for country? | ||||
| Yes | 1.35 (1.06,1.71) | 1.14 (0.98,1.35) | 1.55 (1.30,1.84) | 29.9% |
| How much time do you spend on country? | ||||
| ≥A little bit | 1.40 (1.15,1.67) | 1.10 (0.92,1.33) | 1.56 (1.30,1.86) | 21.4% |
| ≥A fair bit | 1.24 (0.95,1.60) | 1.26 (1.04,1.52) | 1.56 (1.30,1.86) | 52.0% |
| A lot | 1.38 (1.10,1.71) | 1.13 (0.99,1.29) | 1.56 (1.30,1.87) | 27.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wright, A.; Yap, M.; Jones, R.; Richardson, A.; Davis, V.; Lovett, R. Examining the Associations between Indigenous Rangers, Culture and Wellbeing in Australia, 2018–2020. Int. J. Environ. Res. Public Health 2021, 18, 3053. https://doi.org/10.3390/ijerph18063053
Wright A, Yap M, Jones R, Richardson A, Davis V, Lovett R. Examining the Associations between Indigenous Rangers, Culture and Wellbeing in Australia, 2018–2020. International Journal of Environmental Research and Public Health. 2021; 18(6):3053. https://doi.org/10.3390/ijerph18063053
Chicago/Turabian StyleWright, Alyson, Mandy Yap, Roxanne Jones, Alice Richardson, Vanessa Davis, and Raymond Lovett. 2021. "Examining the Associations between Indigenous Rangers, Culture and Wellbeing in Australia, 2018–2020" International Journal of Environmental Research and Public Health 18, no. 6: 3053. https://doi.org/10.3390/ijerph18063053
APA StyleWright, A., Yap, M., Jones, R., Richardson, A., Davis, V., & Lovett, R. (2021). Examining the Associations between Indigenous Rangers, Culture and Wellbeing in Australia, 2018–2020. International Journal of Environmental Research and Public Health, 18(6), 3053. https://doi.org/10.3390/ijerph18063053