
Indoor Model Simulation for COVID-19 Transport and Exposure

 , , , and
, , , and
Abstract
1. Introduction
- Contact spread either by the direct pathway or indirect (i.e., contaminated surface) pathway;
- Transmission by the inhalation of aerosols and droplets either at short range (commonly known as droplet transmission) or long range (commonly known as airborne transmission).
2. Materials and Methods
2.1. Model Overview
- During respiratory activities, such as talking, singing, coughing, or sneezing, aerosols and droplets of virus-laden respiratory tract fluid are emitted into the surrounding air;
- These droplets are subject to evaporation and thus shrink in size and become dry particles (hereafter, the infectious particles). Some will become small enough to remain airborne for minutes to hours. SARS-CoV-2 may remain infectious in such particles over these time scales;
- A susceptible person inhales the infectious particles.
2.2. Formation and Emission of SARS-CoV-2 Aerosols: Physical Characterisitics
- Open-close cycling of airway structures in the distal lung;
- Open-close cycling of glottic structures, primarily during talking and singing;
- Shear forces due to high-velocity gas flow, primarily in the upper respiratory tract;
- Articulation of consonants, generating saliva particles from the oral cavity.
- Tidal volume breathing generates airflow velocities around 1 m/s in the trachea and bronchi;
- Talking generates airflow velocities up to 5 m/s at the initial or starting phase of the motion;
- Coughing generates airflow velocities between 2–50 m/s;
- Sneezing generates airflow velocities more than 100 m/s.
2.3. Exposure to Airborne Particles Containing SARS-CoV-2
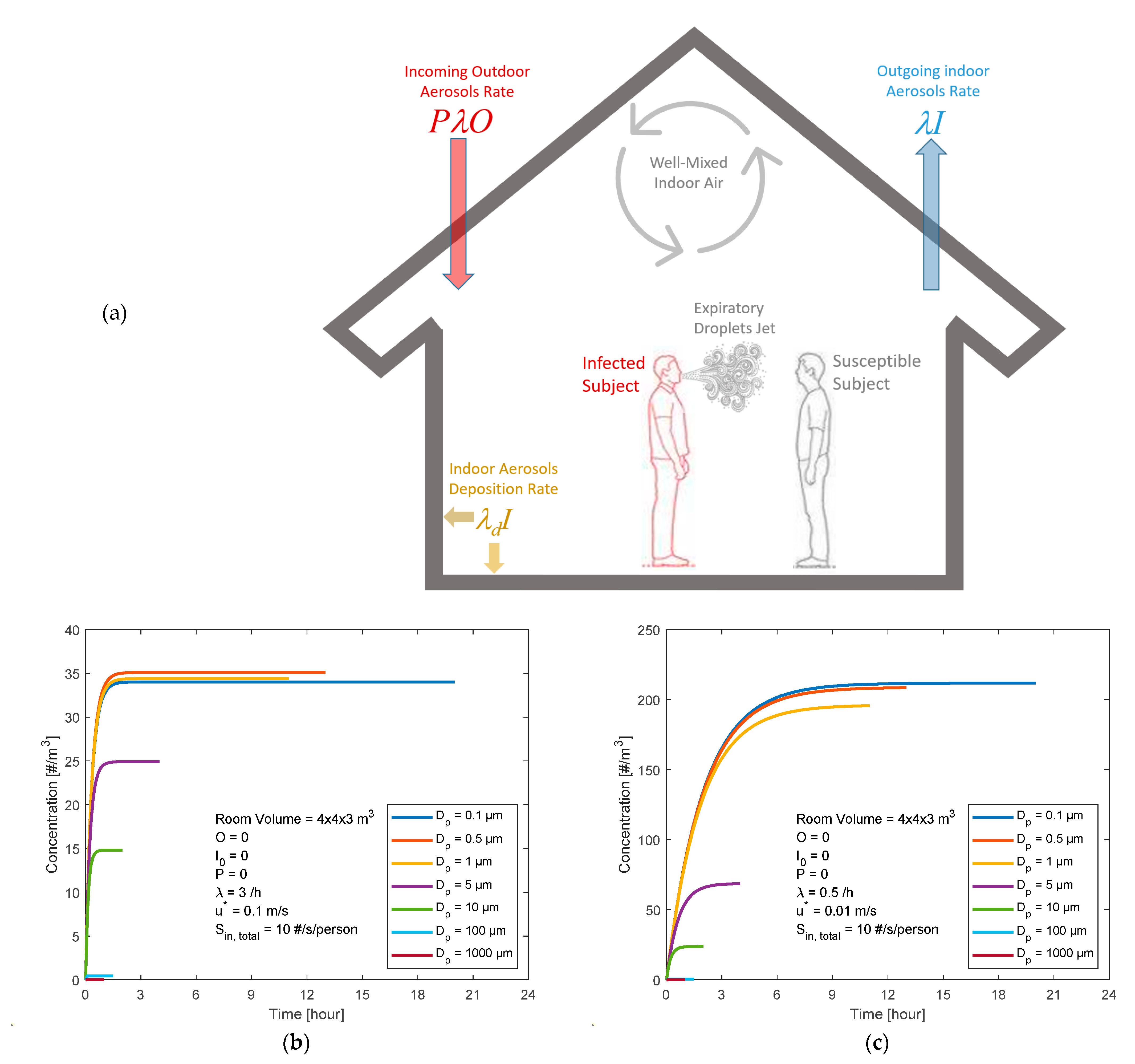
2.3.1. Indoor Aerosol Model
2.3.2. Inhaled Deposited Dose Model
3. Results
3.1. Scenarios of Expiratory Airborne Particles Indoors: Exposure Levels
- ▪
- A room (4 × 4 × 3 m3) with well-mixed indoor air;
- ▪
- A clean (not contaminated) room at t = 0 (i.e., airborne particles containing SARS-CoV-2 concentrations indoors I0 = 0 m−3);
- ▪
- Clean outdoor air (i.e., airborne particles containing SARS-CoV-2 concentrations outdoors O = 0 m−3);
- ▪
- The penetration factor (P) was set to zero;
- ▪
- Ventilation rate (λ) varying within the range of 0.5–3 h−1;
- -
- Well-ventilated indoor air (i.e., high ventilation rate λ = 3 h−1 and low friction velocity u* = 0.1 m/s);
- -
- Poorly ventilated indoor air (i.e., low ventilation rate λ = 0.5 h−1 and low friction velocity u* = 0.01 m/s);
- ▪
- The deposition rate (λd) depends on the particle diameter (Dp) and the turbulent mixing conditions (i.e., friction velocity u* in the range 0.01–0.1 m/s);
- ▪
- Occupancy by a person with the virus who emits expiratory airborne particles carrying SARS-CoV-2 virions;
- ▪
- The expiratory airborne particles of relevance for transmission of COVID-19 through inhalation have particle diameters (Dp) within the range of 0.1–1000 µm;
- ▪
- Emission rates may vary by many orders of magnitude, depending on the characteristics of the source. Here, as an example, we use a rate of 10 viruses/second;
- -
- The viruses are assumed to be uniformly distributed on the particles, with an equal number for all particle sizes and with 7 size bins in the range of 0.1–1000 µm (i.e., ~1.4 viruses/second in each particle size bin);
- -
- The true size distribution is not known, but large particles will contain more viruses while, on the other hand, there are many small particles by number;
- -
3.2. Scenarios of COVID-19 Exposure: Inhaled Deposited Dose Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Sensitivity Analysis for the Simple Indoor Aerosol Model (IAM)
- Empty room;
- Unoccupied;
- Well-mixed indoor air;
- Constant model parameters (O, P, λ, λd, and Sin).




References
- Chen, L.; Liu, W.; Zhang, Q.; Xu, K.; Ye, G.; Wu, W.; Sun, Z.; Liu, F.; Wu, K.; Zhong, B.; et al. RNA based mNGS approach identifies a novel human coronavirus from two individual pneumonia cases in 2019 Wuhan outbreak. Emerg. Microbes Infect. 2020, 9, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef]
- World Health Organization. Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Infections in Health Care; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- How COVID-19 Spreads. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/about/transmission.html (accessed on 15 January 2021).
- Asadi, S.; Bouvier, C.; Wexler, A.S.; Ristenpart, W.D. The coronavirus pandemic and aerosols: Does COVID-19 transmit via expiratory particles? Aerosol Sci. Technol. 2020, 6, 635–638. [Google Scholar] [CrossRef]
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic characteristics and RNA concentration of SARS-CoV-2 aerosol in Wuhan hospitals during COVID-19 Outbreak. bioRxiv 2020. [Google Scholar] [CrossRef]
- Tellier, R.; Li, Y.; Cowling, B.J.; Tang, J.W. Recognition of aerosol transmission of infectious agents: A commentary. BMC Infect. Dis. 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Jones, R.M.; Brosseau, L.M. Aerosol transmission of infectious disease. J. Occup. Environ. Med. 2015, 57, 501–508. [Google Scholar] [CrossRef]
- Xie, X.; Li, Y.; Sun, H.; Liu, L. Exhaled droplets due to talking and coughing. J. R. Soc. Interface 2009, 6, S703–S714. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Li, Y. Airborne spread of infectious agents in the indoor environment. Am. J. Infect. Control. 2016, 44, S102–S108. [Google Scholar] [CrossRef]
- Xie, X.; Li, Y.; Chwang, A.T.Y.; Ho, P.L.; Seto, W.H. How far droplets can move in indoor environments? revisiting the Wells evaporation-falling curve. Indoor Air 2007, 17, 211–225. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Bushmaker, T.; Morris, D.; Holbrook, M.; Gamble, A.; Williamson, B.; Tamin, A.; Harcourt, J.; Thornburg, N.; Gerber, S.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 1–3. [Google Scholar] [CrossRef]
- Casanova, L.M.; Jeon, S.; Rutala, W.A.; Weber, D.J.; Sobsey, M.D. Effects of air temperature and relative humidity on coronavirus survival on surfaces. Appl. Environ. Microbiol. 2010, 76, 2712–2717. [Google Scholar] [CrossRef]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect. 2020, 104, 246–251. [Google Scholar] [CrossRef]
- Kampf, G. Potential role of inanimate surfaces for the spread of coronaviruses and their inactivation with disinfectant agents. Infect. Prev. Pr. 2020, 2, 100044. [Google Scholar] [CrossRef]
- Chin, A.W.H.; Chu, J.T.S.; Perera, M.R.A.; Hui, K.P.Y.; Yen, H.-L.; Chan, M.C.W.; Peiris, M.; Poon, L.L.M. Stability of SARS-CoV-2 in different environmental conditions. Lancet 2020, 1, e10. [Google Scholar]
- Popa, A.; Genger, J.-W.; Nicholson, M.D.; Penz, T.; Schmid, D.; Aberle, S.W.; Agerer, B.; Lercher, A.; Endler, L.; Colaço, H.; et al. Genomic epidemiology of superspreading events in Austria reveals mutational dynamics and transmission properties of SARS-CoV-2. Sci. Trans. Med. 2020, eabe2555. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.C.; Ricks, K.M.; Jay, A.; Raymond, J.L.; Rossi, F.; Zeng, X.; Scruggs, J.; Dyer, D.; Frick, O.; Koehler, J.W.; et al. Development of a coronavirus disease 2019 nonhuman primate model using airborne exposure. PLoS ONE 2021, 16, e0246366. [Google Scholar] [CrossRef]
- Buonanno, G.; Stabile, L.; Morawska, L. Estimation of airborne viral emission: Quanta emission rate of SARS-CoV-2 for infection risk assessment. Environ. Intern. 2020, 141, 105794. [Google Scholar] [CrossRef]
- Prentiss, M.G.; Chu, A.; Berggren, K.K. Superspreading events without superspreaders: Using high attack rate events to estimate No for airborne transmission of COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Karimzadeh, S.; Bhopal, R.; Tien, H.N. Review of Infective Dose, Routes of Transmission, and Outcome of COVID-19 Caused by the SARS-CoV-2 Virus: Comparison with Other Respiratory Viruses. 2020. Available online: https://www.preprints.org (accessed on 26 February 2021).
- Lelieveld, J.; Helleis, F.; Borrmann, S.; Cheng, Y.; Drewnick, F.; Haug, G.; Klimach, T.; Sciare, J.; Su, H.; Pöschl, U. Model calculations of aerosol transmission and infection risk of COVID-19 in indoor environments. Int. J. Environ. Res. Public Health 2020, 17, 8114. [Google Scholar] [CrossRef] [PubMed]
- Bredberg, A.; Gobom, J.; Almstrand, A.-C.; Larsson, P.; Blennow, K.; Olin, A.-C.; Mirgorodskaya, E. Exhaled endogenous particles contain lung proteins. Clin. Chem. 2012, 58, 431–440. [Google Scholar] [CrossRef]
- Alsved, M.; Matamis, A.; Bohlin, R.; Richter, M.; Bengtsson, P.E.; Fraenkel, C.J.; Medstrand, P.; Löndahl, J. Exhaled respiratory particles during singing and talking. Aerosol Sci. Technol. 2020, 54, 1245–1248. [Google Scholar] [CrossRef]
- Wilson, N.M.; Norton, A.; Young, F.P.; Collins, D.W. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: A narrative review. Anaesthesia 2020, 75, 1086–1095. [Google Scholar] [CrossRef] [PubMed]
- Almstrand, A.-C.; Bake, B.; Ljungström, E.; Larsson, P.; Bredberg, A.; Mirgorodskaya, E.; Olin, A.-C. Effect of airway opening on production of exhaled particles. J. Appl. Physiol. 2010, 108, 584–588. [Google Scholar] [CrossRef]
- Wells, F.W. Airborne Contagion and Air Hygiene. An Ecological Study of Droplet Infections; Harvard University Press: Cambridge, UK, 1955; p. 423. [Google Scholar]
- Walker, J.S.; Archer, J.; Gregson, F.K.; Michel, S.E.; Bzdek, B.R.; Reid, J.P. Accurate representations of the microphysical processes occurring during the transport of exhaled aerosols and droplets. ACS Cent. Sci. 2021, 7, 200–209. [Google Scholar] [CrossRef]
- Hussein, T.; Löndahl, J.; Paasonen, P.; Koivisto, A.J.; Petäjä, T.; Hämeri, K.; Kulmala, M. Modeling regional deposited dose of submicron aerosol particles. Sci. Total. Environ. 2013, 458–460, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Hussein, T.; Kulmala, M. Indoor aerosol modeling: Basic principles and practical applications. Water Air Soil Pollut. Focus 2007, 8, 23–34. [Google Scholar] [CrossRef]
- Nazaroff, W.W. Indoor Particle Dynamics. Indoor Air 2004, 14, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.R. How Much Air do We Breath? California Environmental Protection Agency: Sacramento, CA, USA, 1994. [Google Scholar]
- ICRP. Annals of the International Commission on Radiological Protection ICRP Publication 66: Human Respiratory Tract Model. for Radiological Protection; International Commission on Radiological Protection: Ottawa, ON, Canada, 1994. [Google Scholar]
- Anjilvel, S.; Asgharian, B. A multiple-path model of particle deposition in the rat lung. Toxicol. Sci. 1995, 28, 41–50. [Google Scholar] [CrossRef]
- Löndahl, J.; Massling, A.; Pagels, J.; Swietlicki, E.; Vaclavik, E.; Loft, S. Size-resolved respiratory-tract deposition of fine and ultrafine hydrophobic and hygroscopic aerosol particles during rest and exercise. Inhal. Toxicol. 2007, 19, 109–116. [Google Scholar] [CrossRef]
- Xu, Q.; Fan, Q.Y.; Duan, N.; Wang, W.; Chen, J.H. Air-borne spread pathway in intensive care unit (ICU) of specialized SARS hospital. Chin. J. Nosoconmiol. 2005, 15, 1380–1382. [Google Scholar]
- Alsved, M.; Fraenkel, C.-J.; Bohgard, M.; Widell, A.; Söderlund-Strand, A.; Lanbeck, P.; Holmdahl, T.; Isaxon, C.; Gudmundsson, A.; Medstrand, P.; et al. Sources of airborne norovirus in hospital outbreaks. Clin. Infect. Dis. 2020, 70, 2023–2028. [Google Scholar] [CrossRef]
- Wells, W.F. On air-borne infection—Study II droplets and droplet nuclei. Am. J. Epidemiol. 1934, 20, 611–618. [Google Scholar] [CrossRef]
- LeClair, J.M.; Zaia, J.A.; Levin, M.J.; Congdon, R.G.; Goldmann, D.A. Airborne transmission of chickenpox in a hospital. N. Engl. J. Med. 1980, 302, 450–453. [Google Scholar] [CrossRef]
- Garner, J.S. Hospital infection control practices advisory committee guideline for isolation precautions in hospitals. Infect. Control. Hosp. Epidemiol. 1996, 17, 53–80. [Google Scholar] [CrossRef]
- Escombe, A.R.; Oeser, C.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Martínez, C.; Caviedes, L.; Sheen, P.; Gonzalez, A.; Noakes, C.; et al. The detection of airborne transmission of tuberculosis from HIV-infected patients, using an in vivo air sampling model. Clin. Infect. Dis. 2007, 44, 1349–1357. [Google Scholar] [CrossRef]
- Wan, M.P.; Chao, C.Y.H.; Chao, Y.H.C. Transport characteristics of expiratory droplets and droplet nuclei in indoor environments with different ventilation airflow patterns. J. Biomech. Eng. 2006, 129, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Huang, X.; Yu, I.T.S.; Wong, T.W.; Qian, H. Role of air distribution in SARS transmission during the largest nosocomial outbreak in Hong Kong. Indoor Air 2005, 15, 83–95. [Google Scholar] [CrossRef]
- Xiao, S.; Li, Y.; Wong, T.-W.; Hui, D.S.C. Role of fomites in SARS transmission during the largest hospital outbreak in Hong Kong. PLoS ONE 2017, 12, e0181558. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Guo, Y.; Xia, L.; Zhou, Q. Structural basis for the recognition of the 2019-nCoV by human ACE2. bioRxiv 2020. [Google Scholar] [CrossRef]
- Booth, T.F.; Kournikakis, B.; Bastien, N.; Ho, J.; Kobasa, D.; Stadnyk, L.; Li, Y.; Spence, M.; Paton, S.; Henry, B.; et al. Detection of airborne severe acute respiratory syndrome (SARS) coronavirus and environmental contamination in SARS outbreak units. J. Infect. Dis. 2005, 191, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.J.; Chang, H.-L.; Cheung, T.Y.-Y.; Tang, A.F.-Y.; Fisk, T.L.; Ooi, S.P.-L.; Kuo, H.-W.; Jiang, D.D.-S.; Chen, K.-T.; Lando, J.; et al. Transmission of the severe acute respiratory syndrome on aircraft. N. Engl. J. Med. 2003, 349, 2416–2422. [Google Scholar] [CrossRef]
- Fineberg, H.V. Rapid Expert Consultation on the Possibility of Bioaerosol Spread of SARS-CoV-2 for the COVID-19 Pandemic; The National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Is the Coronavirus Airborne? Experts Can’t Agree. Nature News. 2020. Available online: https://www.nature.com/articles/d41586-020-00974-w (accessed on 3 January 2021).
- Qian, H.; Zheng, X. Ventilation control for airborne transmission of human exhaled bio-aerosols in buildings. J. Thorac. Dis. 2018, 10, S2295–S2304. [Google Scholar] [CrossRef]
- Kleiboeker, S.; Cowden, S.; Grantham, J.; Nutt, J.; Tyler, A.; Berg, A.; Altrich, M. SARS-CoV-2 viral load assessment in respiratory samples. J. Clinical Virol. 2020, 129, 104439. [Google Scholar] [CrossRef]
- van Kampen, J.J.; van de Vijver, D.A.; Fraaij, P.L.; Haagmans, B.L.; Lamers, M.M.; Okba, N.; van den Akker, J.P.; Endeman, H.; Gommers, D.A.; Cornelissen, J.J.; et al. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nat. Commun. 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Gregson, F.K.A.; Watson, N.A.; Orton, C.M.; Haddrell, A.E.; McCarthy, L.P.; Finnie, T.J.R.; Gent, N.; Donaldson, G.C.; Shah, P.L.; Calder, J.D.; et al. Comparing aerosol concentrations and particle size distributions generated by singing, speaking and breathing. Aerosol Sci. Technol. 2021, 1–15. [Google Scholar] [CrossRef]
- Lindsley, W.G.; Blachere, F.M.; Beezhold, D.H.; Thewlis, R.E.; Noorbakhsh, B.; Othumpangat, S.; Goldsmith, W.T.; McMillen, C.M.; Andrew, M.E.; Burrell, C.N.; et al. Viable influenza A virus in airborne particles expelled during coughs versus exhalations. Influ. Other Respir. Viruses 2016, 10, 404–413. [Google Scholar] [CrossRef]
- Asadi, S.; Wexler, A.S.; Cappa, C.D.; Barreda, S.; Bouvier, N.M.; Ristenpart, W.D. Aerosol emission and superemission during human speech increase with voice loudness. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.A.; Ausiello, D.; Salzman, J.; Devlin, T.; Langer, R.; Beddingfield, B.J.; Fears, A.C.; Doyle-Meyers, L.A.; Redmann, R.K.; Killeen, S.Z.; et al. Exhaled aerosol increases with COVID-19 infection, age, and obesity. Proc. Natl. Acad. Sci. USA 2021, 118, 2021830118. [Google Scholar] [CrossRef] [PubMed]
- Heyder, J.; Gebhart, J.; Rudolf, G.; Schiller, C.F.; Stahlhofen, W. Deposition of particles in the human respiratory-tract in the size range 0.005–15 µm. J. Aerosol Sci. 1986, 17, 811–825. [Google Scholar] [CrossRef]
- Duguid, J.P. The size and the duration of air-carriage of respiratory droplets and droplet-nuclei. Epidemiol. Infect. 1946, 44, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Loudon, R.G.; Roberts, R.M. Droplet expulsion from the respiratory tract. Am. Rev. Respir. Dis. 1967, 95, 435–442. [Google Scholar] [PubMed]
- Papineni, R.S.; Rosenthal, F.S. The Size distribution of droplets in the exhaled breath of healthy human subjects. J. Aerosol Med. 1997, 10, 105–116. [Google Scholar] [CrossRef]
- Yan, J.; Grantham, M.; Pantelic, J.; de Mesquita, P.J.B.; Albert, B.; Liu, F.J.; Ehrman, S.; Milton, D.K. Infectious virus in exhaled breath of symptomatic seasonal influenza cases from a college community. Proc. Natl. Acad. Sci. USA 2018, 115, 1081–1086. [Google Scholar] [CrossRef]
- Morawska, L.; Johnson, G.; Ristovski, Z.; Hargreaves, M.; Mengersen, K.; Corbett, S.; Chao, C.; Li, Y.; Katoshevski, D. Size distribution and sites of origin of droplets expelled from the human respiratory tract during expiratory activities. J. Aerosol Sci. 2009, 40, 256–269. [Google Scholar] [CrossRef]
- Jiang, J.; Fu, Y.V.; Liu, L.; Kulmala, M. Transmission via aerosols: Plausible differences among emerging coronaviruses. Aerosol Sci. Technol. 2020, 54, 865–868. [Google Scholar] [CrossRef]
- Spena, A.; Palombi, L.; Corcione, M.; Carestia, M.; Spena, V.A. On the Optimal Indoor Air Conditions for SARS-CoV-2 Inactivation. An Enthalpy-Based Approach. Int. J. Environ. Res. Public Health 2020, 17, 6083. [Google Scholar] [CrossRef]
- Spena, A.; Palombi, L.; Corcione, M.; Quintino, A.; Carestia, M.; Spena, V.A. Predicting SARS-CoV-2 weather-induced seasonal virulence from atmospheric air enthalpy. Int. J. Environ. Res. Public Health 2020, 17, 9059. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Activity | Female | Male | DF Curve Type |
|---|---|---|---|
| Yard work | 1.08 | 1.74 | Exercise |
| Walking (4.0 km/h) | 1.20 | 1.38 | Exercise |
| Standing | 0.48 | 0.66 | At rest |
| Sitting | 0.42 | 0.54 | At rest |
| Room Conditions | VE | 0.1 µm | 0.5 µm | 1 µm | 5 µm | 10 µm | Total | ||
|---|---|---|---|---|---|---|---|---|---|
| DF | 0.34 | 0.12 | 0.24 | 0.89 | 0.83 | ||||
| Tightly Closed (ventilation = 0.5 h−1) | Male | Rest | 0.63 | 46 | 16 | 30 | 39 | 13 | 143 |
| Exercise | 1.56 | 114 | 40 | 74 | 94 | 31 | 354 | ||
| Female | Rest | 0.45 | 33 | 11 | 21 | 27 | 9 | 101 | |
| Exercise | 1.15 | 84 | 29 | 54 | 70 | 23 | 260 | ||
| Well-Ventilated (ventilation = 3 h−1) | Male | Rest | 0.63 | 7 | 3 | 6 | 14 | 9 | 39 |
| Exercise | 1.56 | 19 | 7 | 13 | 36 | 20 | 94 | ||
| Female | Rest | 0.45 | 6 | 1 | 4 | 10 | 6 | 27 | |
| Exercise | 1.15 | 14 | 4 | 10 | 26 | 14 | 69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussein, T.; Löndahl, J.; Thuresson, S.; Alsved, M.; Al-Hunaiti, A.; Saksela, K.; Aqel, H.; Junninen, H.; Mahura, A.; Kulmala, M. Indoor Model Simulation for COVID-19 Transport and Exposure. Int. J. Environ. Res. Public Health 2021, 18, 2927. https://doi.org/10.3390/ijerph18062927
Hussein T, Löndahl J, Thuresson S, Alsved M, Al-Hunaiti A, Saksela K, Aqel H, Junninen H, Mahura A, Kulmala M. Indoor Model Simulation for COVID-19 Transport and Exposure. International Journal of Environmental Research and Public Health. 2021; 18(6):2927. https://doi.org/10.3390/ijerph18062927
Chicago/Turabian StyleHussein, Tareq, Jakob Löndahl, Sara Thuresson, Malin Alsved, Afnan Al-Hunaiti, Kalle Saksela, Hazem Aqel, Heikki Junninen, Alexander Mahura, and Markku Kulmala. 2021. "Indoor Model Simulation for COVID-19 Transport and Exposure" International Journal of Environmental Research and Public Health 18, no. 6: 2927. https://doi.org/10.3390/ijerph18062927
APA StyleHussein, T., Löndahl, J., Thuresson, S., Alsved, M., Al-Hunaiti, A., Saksela, K., Aqel, H., Junninen, H., Mahura, A., & Kulmala, M. (2021). Indoor Model Simulation for COVID-19 Transport and Exposure. International Journal of Environmental Research and Public Health, 18(6), 2927. https://doi.org/10.3390/ijerph18062927