
Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Questionnaires
2.3. Ethical Consideration
2.4. Statistical Methods
3. Results
3.1. Socio-Demographic and Clinical Characteristics of the Study Group
3.2. Level of Non-Adherence (INAS Scores) and Beliefs about Medication (BMQ Scores)
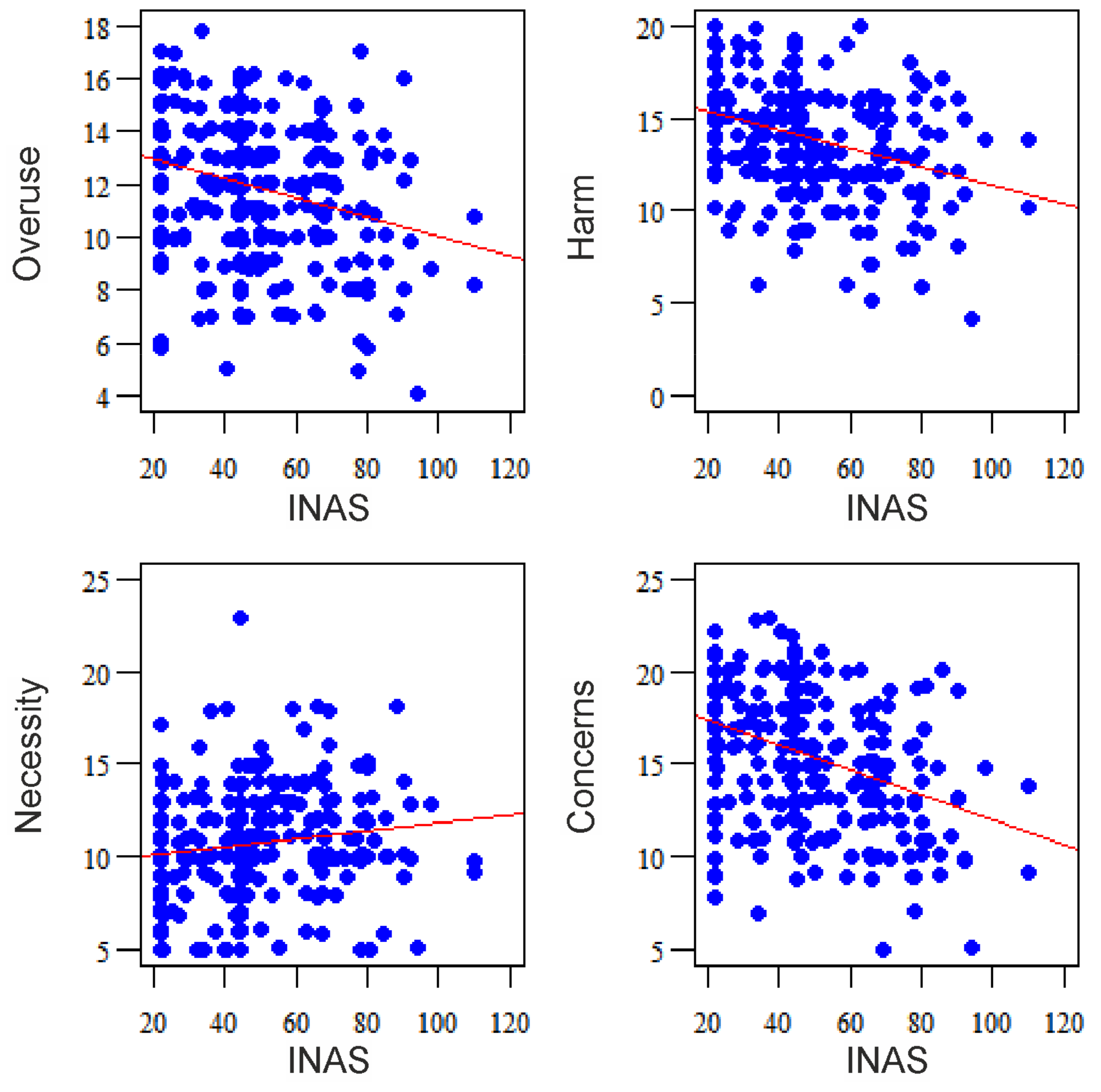
3.3. Correlation Analysis for Non-Adherence and Beliefs about Medication
3.4. Predictors of Intentional Non-Adherence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adherence to Long-Term Therapies—Evidence for Action. Available online: https://apps.who.int/medicinedocs/en/d/Js4883e/8.5.4.html (accessed on 10 January 2021).
- Bosworth, H.B.; Zullig, L.L.; Mendys, P.; Ho, M.; Trygstad, T.; Granger, C.; Oakes, M.M.; Granger, B.B. Health Information Technology: Meaningful Use and Next Steps to Improving Electronic Facilitation of Medication Adherence. JMIR Med. Inform. 2016, 4, e9. [Google Scholar] [CrossRef]
- Vrijens, B.; Antoniou, S.; Burnier, M.; de la Sierra, A.; Volpe, M. Current situation ofmedication adherence in hypertension. Front. Pharmacol. 2017, 8, 100. [Google Scholar] [CrossRef] [PubMed]
- Rosen, O.Z.; Fridman, R.; Rosen, B.T.; Shane, R.; Pevnick, J.M. Medication adherence as a predictor of 30-day hospital readmissions. Patient Prefer Adherence. 2017, 11, 801–810. [Google Scholar] [CrossRef]
- Gaciong, Z. Nieprzestrzeganie zaleceń terapeutycznych w leczeniu chorób przewlekłych. In Nieprzestrzeganie Zaleceń Terapeutycznych: Od Przyczyn do Praktycznych Rozwiązań: Podręcznik dla Lekarzy i Studentów Kierunków Medycznych; Diabetologia, W., Gaciong, Z., Kardas, P., Eds.; NaukowaFundacjaPolpharmy: Warszawa, Poland, 2015; pp. 113–122. [Google Scholar]
- Jankowska-Polańska, B.; Chudiak, A.; Uchmanowicz, I.; Dudek, K.; Mazur, G. Selected factors affecting adherence in the pharmacological treatment of arterial hypertension. Patient Prefer Adherence 2017, 11, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Karbownik, M.S.; Jankowska-Polańska, B.; Horne, R.; Górski, K.M.; Kowalczyk, E.; Szemraj, J. Adaptation and validation of the Polish version of the Beliefs about Medicines Questionnaire among cardiovascular patients and medical students. PLoS ONE 2020, 15, e0230131. [Google Scholar] [CrossRef]
- Glombiewski, J.A.; Nestoriuc, Y.; Rief, W.; Glaesmer, H.; Braehler, E. Medication adherence in the general population. PLoS ONE 2012, 7, e50537. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, J.; Buxton, M.; McGarry, T.; Sheldon, R.; Chancellor, J. Patients’ preferences for characteristics associated with treatments for osteoarthritis. Rheumatology 2004, 43, 337–345. [Google Scholar] [CrossRef]
- Ashoorkhani, M.; Majdzadeh, R.; Gholami, J.; Eftekhar, H.; Bozorgi, A. Understanding Non-Adherence to Treatment in Hypertension: A Qualitative Study. Int. J. Community Based Nurs. Midwifery 2018, 6, 314–323. [Google Scholar]
- Foot, H.; La Caze, A.; Gujral, G.; Cottrell, N. The necessity-concerns framework predicts adherence to medication in multiple illness conditions: A meta-analysis. Patient Educ. Couns. 2016, 99, 706–717. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Chapman, S.C.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: A meta-analytic review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef]
- Wei, L.; Champman, S.; Li, X.; Li, X.; Li, S.; Chen, R.; Bo, N.; Chater, A.; Horne, R. Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: A cross-sectional study in China. BMJ Open 2017, 7, e017293. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J.; Hankins, M. The Beliefs about Medicines Questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Weinman, J.; Graham, S.; Canfield, M.; Kleinstäuber, M.; Perera, A.I.; Dalbeth, N.; Petrie, K.J. The Intentional Non-Adherence Scale (INAS): Initial development and validation. J. Psychosom. Res. 2018, 115, 110–116. [Google Scholar] [CrossRef]
- Najjuma, J.N.; Brennaman, L.; Nabirye, R.C.; Ssedyabane, F.; Maling, S.; Bajunirwe, F.; Muhindo, R. Adherence to Antihypertensive Medication: An Interview Analysis of Southwest Ugandan Patients’ Perspectives. Ann. Glob. Health 2020, 86, 58. [Google Scholar] [CrossRef]
- Wells, R.E.; Kaptchuk, T.J. To tell the truth, the whole truth, may do patients harm: The problem of the nocebo effect for informed consent. Am. J. Bioeth. 2012, 12, 22–29. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatry Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 6 April 2020).
- Bae, S.G.; Kam, S.; Park, K.S.; Kim, K.Y.; Hong, N.S.; Kim, K.S.; Lee, Y.M.; Lee, W.K.; Choe, M.S. Factors related to intentional and unintentional medication nonadherence in elderly patients with hypertension in rural community. Patient Prefer Adherence 2016, 10, 1979–1989. [Google Scholar] [CrossRef]
- Lowry, K.P.; Dudley, T.K.; Oddone, E.Z.; Bosworth, H.B. Intentional and unintentional nonadherence to antihypertensive medication. Ann. Pharmacother. 2005, 39, 1198–1203. [Google Scholar] [CrossRef]
- Gadkari, A.S.; McHorney, C.A. Unintentional non-adherence to chronic prescription medications: How unintentional is it really? BMC Health Serv. Res. 2012, 12, 98. [Google Scholar] [CrossRef]
- Eliasson, L.; Clifford, S.; Barber, N.; Marin, D. Exploring chronic myeloid leukemia patients’ reasons for not adhering to the oral anticancer drug imatinib as prescribed. Leuk. Res. 2011, 35, 626–630. [Google Scholar] [CrossRef]
- Raynor, D.K.; Savage, I.; Knapp, P.; Henley, J. We are the experts: People with asthma talk about their medicine information needs. Patient Educ. Couns. 2004, 53, 167–174. [Google Scholar] [CrossRef]
- Atkins, L.; Fallowfield, L. Intentional and non-intentional non-adherence to medication amongst breast cancer patients. Eur. J. Cancer 2006, 42, 2271–2276. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 1999, 47, 555–567. [Google Scholar] [CrossRef]
- Unni, E.J.; Farris, K.B. Unintentional non-adherence and belief in medicines in older adults. Patient Educ. Couns. 2011, 83, 265–268. [Google Scholar] [CrossRef] [PubMed]
- LeporiniCDeSarroGRusso, E. Adherence to therapy and adverse drug reactions: Is there a link? Expert Opin. Drug Saf. 2014, 13, 41–55. [Google Scholar]
- Clyne, B.; Cooper, J.A.; Boland, F.; Hughes, C.M.; Fahey, T.; Smith, S.M.; OPTI-SCRIPT Study Team. Beliefs about prescribed medication among older patients with polypharmacy: A mixed methods study in primary care. Br. J. Gen. Pract. 2017, 67, e507–e518. [Google Scholar] [CrossRef]
- Modig, S.; Kristensson, J.; Troein, M.; Brorsson, A.; Midlöv, P. Frail elderly patients experiences of information on medication. A qualitative study. BMC Geriatr. 2012, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Modig, S.; Kristensson, J.; Ekwall, A.; Hallberg, I.R.; Midlöv, P. Frail elderly patients in primary care—Their medication knowledge and beliefs about prescribed medicines. Eur. J. Clin. Pharmacol. 2009, 65, 151–155. [Google Scholar] [CrossRef]
- Náfrádi, L.; Galimberti, E.; Nakamoto, K.; Schulz, P.J. Intentional and Unintentional Medication Non-Adherence in Hypertension: The Role of Health Literacy, Empowerment and Medication Beliefs. J. Public Health Res. 2016, 5, 762. [Google Scholar] [CrossRef]
- Schüz, B.; Marx, C.; Wurm, S.; Warner, L.M.; Ziegelmann, J.P.; Schwarzer, R.; Tesch-Römer, C. Medication beliefs predict medication adherence in older adults with multiple illnesses. J. Psychosom. Res. 2011, 70, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Cramer, J.A. Enhancing patient compliance in the elderly. Drugs Aging 1998, 12, 7–15. [Google Scholar] [CrossRef]
- Cea-Calvo, L.; Marín-Jiménez, I.; de Toro, J.; Fuster-RuizdeApodaca, M.J.; Fernández, G.; Sánchez-Vega, N.; Orozco-Beltrán, D. Different Associations of Intentional and Non-Intentional Non-Adherence Behaviors with Patient Experience with Healthcare and Patient Beliefs in Medications: A Survey of Patients with Chronic Conditions. Patient Prefer Adherence 2020, 14, 2439–2450. [Google Scholar] [CrossRef] [PubMed]
- Świątoniowska-Lonc, N.; Polański, J.; Tański, W.; Jankowska-Polańska, B. Impact of Cognitive Impairment on Adherence to Treatment and Self-Care in Patients with Type 2 Diabetes Mellitus. Diabetes Metab. Syndr. Obes. 2021, 14, 193–203. [Google Scholar] [CrossRef]
- Jankowska-Polańska, B.; Katarzyna, L.; Lidia, A.; Joanna, J.; Dudek, K.; Izabella, U. Cognitive function and adherence to anticoagulation treatment in patients with atrial fibrillation. J. Geriatr. Cardiol. 2016, 13, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Jankowska-Polańska, B.; Świątoniowska-Lonc, N.; Sławuta, A.; Krówczyńska, D.; Dudek, K.; Mazur, G. Patient-Reported Compliance in older age patients with chronic heart failure. PLoS ONE 2020, 15, e0231076. [Google Scholar] [CrossRef] [PubMed]
- Grant, R.W.; Devita, N.G.; Singer, D.E.; Meigs, J.B. Polypharmacy and medication adherence in patients with type 2 diabetes. Diabetes Care 2003, 26, 1408–1412. [Google Scholar] [CrossRef]
- Labrie, N.H.M.; Schulz, P.J. The effects of general practitioners’ use of argumentation to support their treatment advice: Results of an experimental study using video-vignettes. Health Commun. 2014, 30, 951–961. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total (N = 300) | |
|---|---|---|
| Age [years] | Mean (SD) | 71.71 (8.12) |
| Gender | Male | 106 (35.33%) |
| Female | 194 (64.67%) | |
| Education | None or primary school | 130 (43.33%) |
| Secondary school | 137 (45.67%) | |
| University | 33 (11.00%) | |
| Marital status | Married or living with partner | 188 (62.67%) |
| Single or divorced | 112 (37.33%) | |
| BMI | Normal | 40 (13.33%) |
| Overweight | 125 (41.67%) | |
| Obesity | 95 (31.67%) | |
| Obesity class II | 25 (8.33%) | |
| Obesity class III | 15 (5.00%) | |
| SBP [mmHg] | Mean (SD) | 141.11(40.15) |
| DBP [mmHg] | Mean (SD) | 81.38 (7.4) |
| Number of chronic diseases | Mean (SD) | 1.88 (0.94) |
| Total number of medications taken | Mean (SD) | 1.97 (1.96) |
| Number of hypertensive drugs | Mean (SD) | 2.12 (1.03) |
| Questionnaire | N | Range | Mean | SD | Mean per Question | |
|---|---|---|---|---|---|---|
| INAS | 300 | 22–110 | 47.28 | 19.12 | - | |
| BMQ | Overuse | 300 | 4–20 | 11.92 | 2.67 | 2.98 |
| Harm | 300 | 4–20 | 13.96 | 2.84 | 3.49 | |
| Necessity | 300 | 5–25 | 10.68 | 2.88 | 2.14 | |
| Concerns | 300 | 5–25 | 15.50 | 3.54 | 3.10 | |
| Variable | Parameter | 95% CI | p | ||
|---|---|---|---|---|---|
| Gender | Male | ref. | |||
| Female | −1.134 | −5.396 | 3.129 | 0.603 | |
| Age | [years] | −0.352 | −0.614 | −0.09 | 0.009 * |
| Education | None or primary school | ref. | |||
| Secondary school | 2.194 | −2.291 | 6.679 | 0.339 | |
| University | −1.419 | −8.594 | 5.755 | 0.699 | |
| Marital status | Married or living with partner | ref. | |||
| Single or divorced | 5.646 | 1.201 | 10.092 | 0.013 * | |
| SBP | [mmHg] | 0.038 | −0.013 | 0.089 | 0.145 |
| DBP | [mmHg] | −0.154 | −0.436 | 0.128 | 0.287 |
| Number of chronic diseases | −2.374 | −4.565 | −0.183 | 0.035 * | |
| Number of hypertensive drugs | 0.413 | −1.581 | 2.408 | 0.685 | |
| MMSE | −0.36 | −0.932 | 0.212 | 0.218 | |
| BMI | Normal | ref. | |||
| Overweight | 3.116 | −3.295 | 9.528 | 0.342 | |
| Obesity | 1.567 | −5.005 | 8.14 | 0.641 | |
| BMQ | Overuse | −0.091 | −1.114 | 0.932 | 0.862 |
| Harm | −0.88 | −1.957 | 0.197 | 0.111 | |
| Necessity | 0.472 | −0.294 | 1.238 | 0.228 | |
| Concerns | −1.376 | −2.097 | −0.655 | <0.001* | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Świątoniowska-Lonc, N.; Polański, J.; Mazur, G.; Jankowska-Polańska, B. Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2825. https://doi.org/10.3390/ijerph18062825
Świątoniowska-Lonc N, Polański J, Mazur G, Jankowska-Polańska B. Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension. International Journal of Environmental Research and Public Health. 2021; 18(6):2825. https://doi.org/10.3390/ijerph18062825
Chicago/Turabian StyleŚwiątoniowska-Lonc, Natalia, Jacek Polański, Grzegorz Mazur, and Beata Jankowska-Polańska. 2021. "Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension" International Journal of Environmental Research and Public Health 18, no. 6: 2825. https://doi.org/10.3390/ijerph18062825
APA StyleŚwiątoniowska-Lonc, N., Polański, J., Mazur, G., & Jankowska-Polańska, B. (2021). Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension. International Journal of Environmental Research and Public Health, 18(6), 2825. https://doi.org/10.3390/ijerph18062825