
Changes in Physical Activity among United Kingdom University Students Following the Implementation of Coronavirus Lockdown Measures

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Permission
2.2. Design and Sample
2.3. Measures
2.4. Statistical Analyses
2.5. Missing Data
3. Results
3.1. Descriptive Statistics
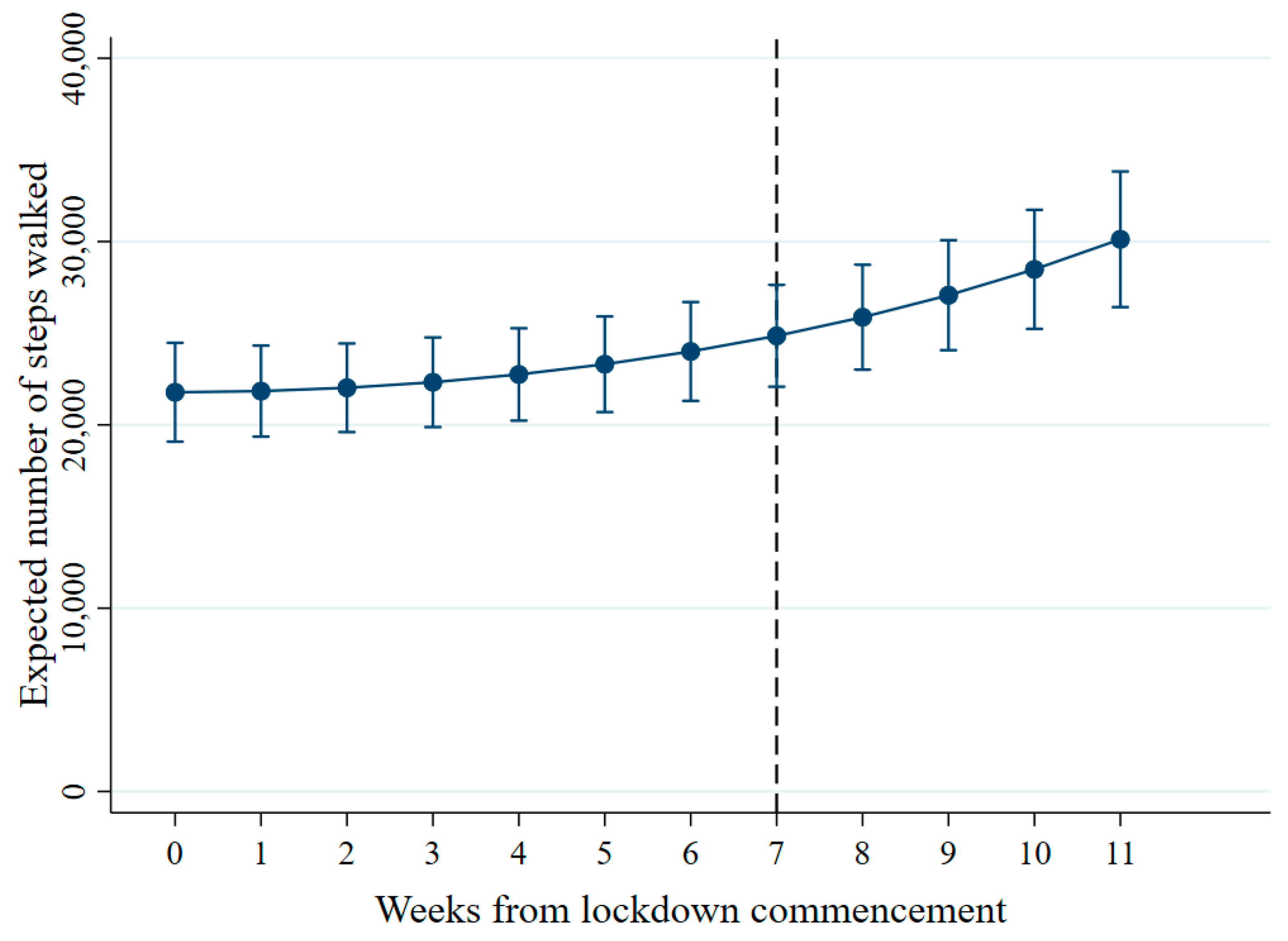
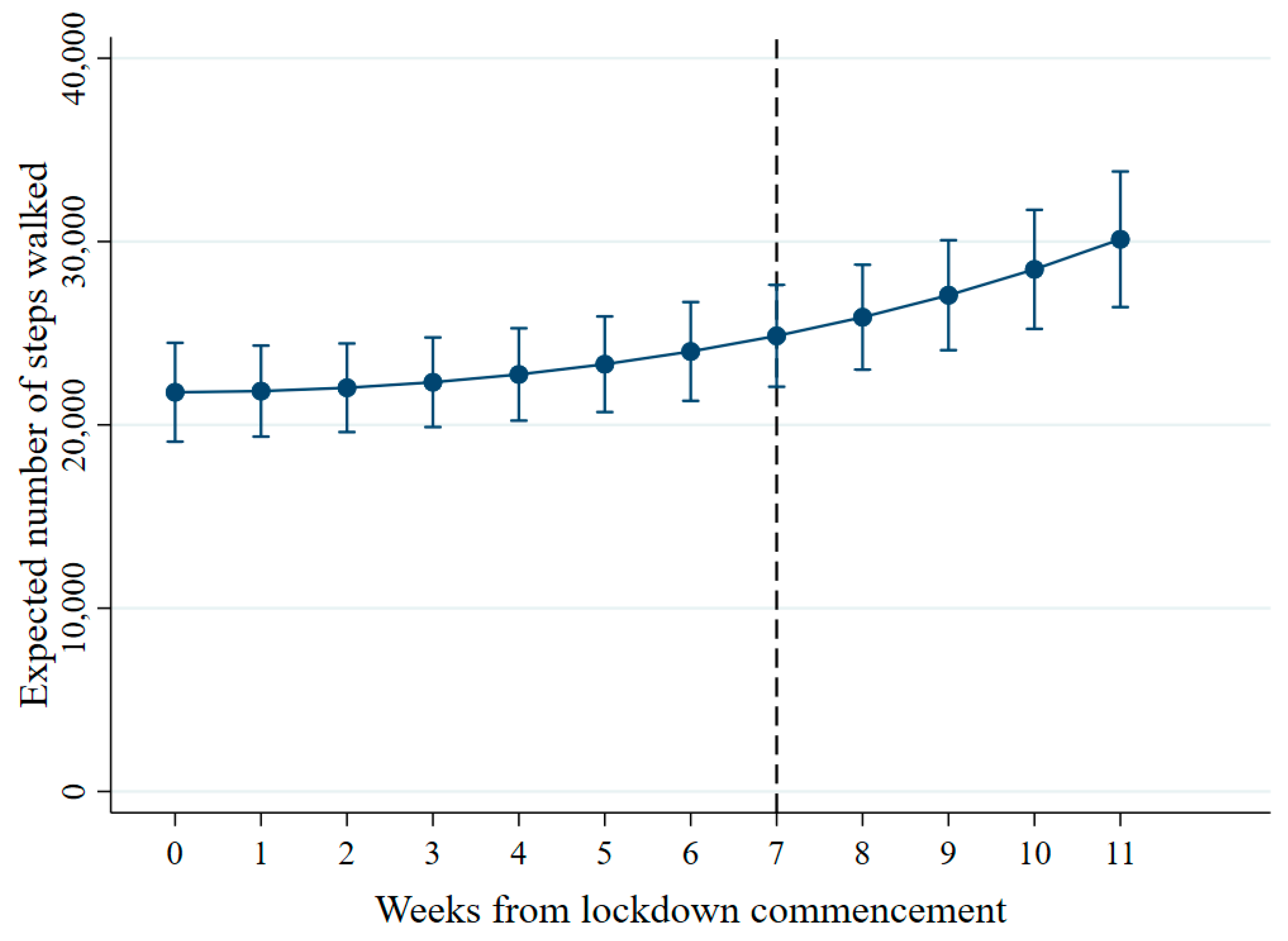
3.2. Trajectories of Steps Walked per Week
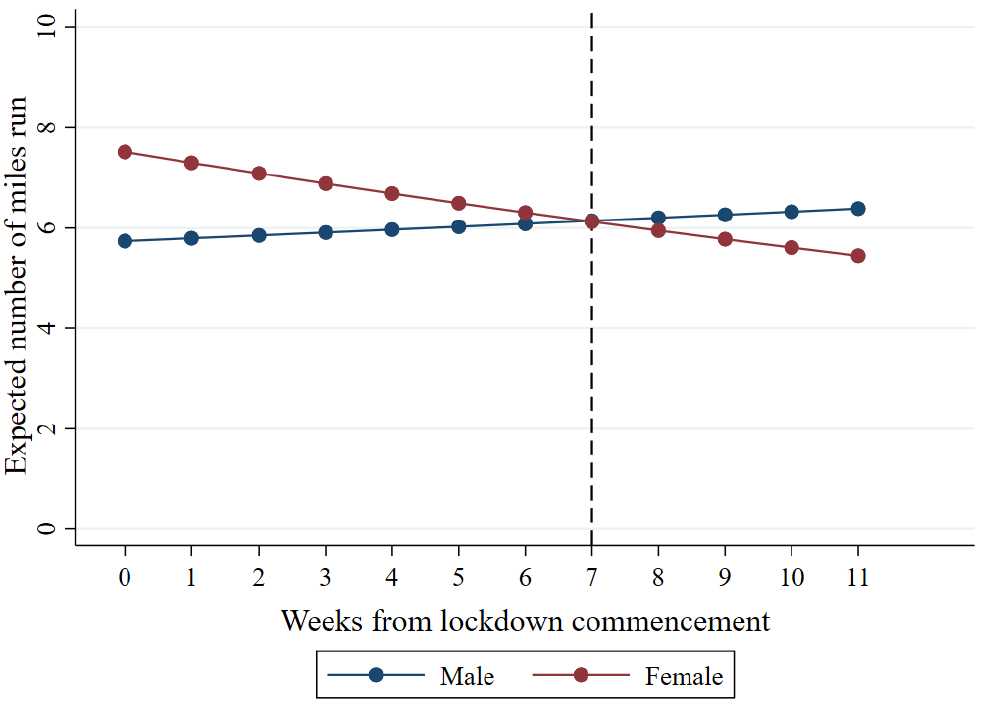
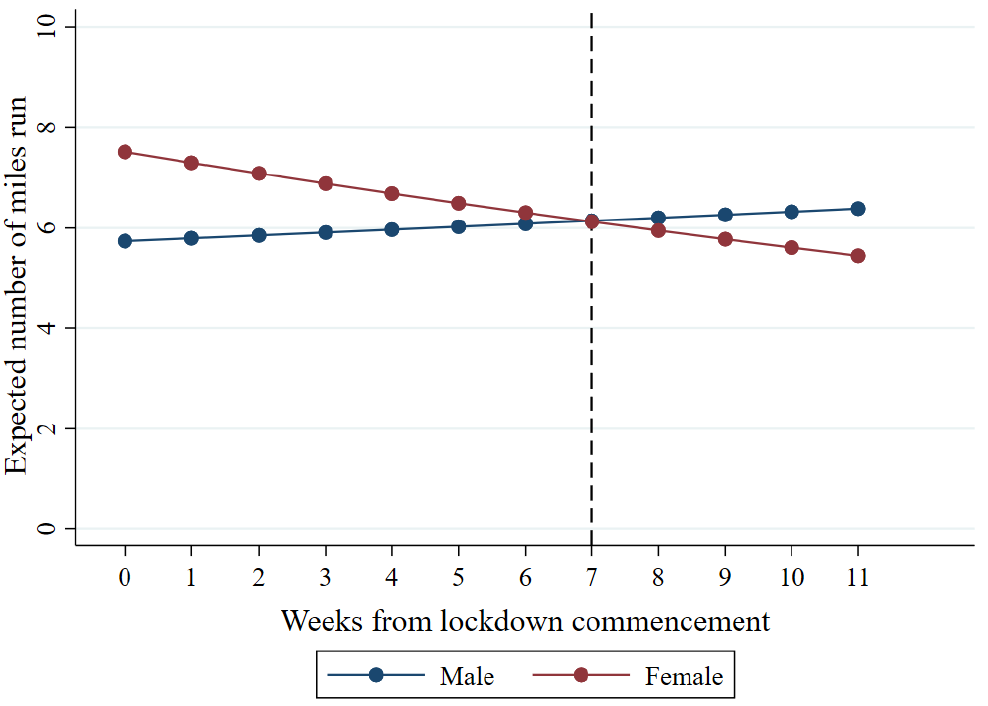
3.3. Trajectories of Miles Run per Week
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Steps Walked Per Week (n = 730) | Miles Run Per Week (n = 264) | |||||||
|---|---|---|---|---|---|---|---|---|
| Timepoint | Missing | Observed | Missing | Observed | ||||
| n | % | n | % | n | % | n | % | |
| Week 0 | 427 | 58.5 | 303 | 41.5 | 194 | 73.5 | 70 | 26.5 |
| Week 1 | 377 | 51.6 | 353 | 48.4 | 185 | 70.1 | 79 | 29.9 |
| Week 2 | 418 | 57.3 | 312 | 42.7 | 168 | 63.6 | 96 | 36.4 |
| Week 3 | 422 | 57.8 | 308 | 42.2 | 152 | 57.6 | 112 | 42.4 |
| Week 4 | 434 | 59.5 | 296 | 40.5 | 160 | 60.6 | 104 | 39.4 |
| Week 5 | 435 | 59.6 | 295 | 40.4 | 157 | 59.5 | 107 | 40.5 |
| Week 6 | 449 | 61.5 | 281 | 38.5 | 172 | 65.2 | 92 | 34.8 |
| Week 7 | 459 | 62.9 | 271 | 37.1 | 194 | 73.5 | 70 | 26.5 |
| Week 8 | 456 | 62.5 | 274 | 37.5 | 177 | 67.0 | 87 | 33.0 |
| Week 9 | 458 | 62.7 | 272 | 37.3 | 186 | 70.5 | 78 | 29.5 |
| Week 10 | 448 | 61.4 | 282 | 38.6 | 194 | 73.5 | 70 | 26.5 |
| Week 11 | 342 | 46.8 | 388 | 53.2 | 155 | 58.7 | 109 | 41.3 |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727. [Google Scholar] [CrossRef] [PubMed]
- Higher Education in Numbers. Available online: https://www.universitiesuk.ac.uk/facts-and-stats/Pages/higher-education-data.aspx (accessed on 3 March 2021).
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. Lancet 2012, 380, 219. [Google Scholar] [CrossRef] [Green Version]
- Herring, M.P. The Effect of Exercise Training on Anxiety Symptoms Among Patients. Arch. Intern. Med. 2010, 170, 321. [Google Scholar] [CrossRef] [PubMed]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for Depression. Cochrane Database Syst. Rev. 2013, 9, CD004366. [Google Scholar]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A.M. Association between Physical Exercise and Mental Health in 1·2 Million Individuals in the USA between 2011 and 2015: A Cross-Sectional Study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Robinson, E.; Boyland, E.; Chisholm, A.; Harrold, J.; Maloney, N.G.; Marty, L.; Mead, B.R.; Noonan, R.; Hardman, C.A. Obesity, eating behavior and physical activity during COVID-19 lockdown: A study of UK adults. Appetite 2021, 156, 104853. [Google Scholar] [CrossRef]
- Savage, M.J.; James, R.; Magistro, D.; Donaldson, J.; Healy, L.C.; Nevill, M.; Hennis, P.J. Mental Health and Movement Be-haviour during the COVID-19 Pandemic in UK University Students: Prospective Cohort Study. Ment. Health Phys. Act. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Luciano, F.; Cenacchi, V.; Vegro, V.; Pavei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2020, 1–10. [Google Scholar] [CrossRef]
- Rodríguez-Larrad, A.; Mañas, I.; Labayen, M.; González-Gross, A.; Espin, S.; Aznar, J.A.; Serrano-Sánchez, F.J.; Vera-Garcia, D.; González-Lamuño, I.; Ara, L.; et al. Impact of COVID-19 Confinement on Physical Activity and Sedentary Behaviour in Spanish University Students: Role of Gender. Int. J. Environ. Res. Public Health 2021, 18, 369. [Google Scholar] [CrossRef]
- Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients 2020, 12, 1865. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.d.C.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Roberts, S.; Reeves, M.; Ryrie, A. The influence of physical activity, sport and exercise motives among UK-based university students. J. Furth. High. Educ. 2014, 39, 598–607. [Google Scholar] [CrossRef]
- Leightley, D.; Puddephatt, J.-A.; Jones, N.; Mahmoodi, T.; Chui, Z.; Field, M.; Drummond, C.; Rona, R.J.; Fear, N.T.; Goodwin, L. A Smartphone App and Personalized Text Messaging Framework (InDEx) to Monitor and Reduce Alcohol Use in Ex-Serving Personnel: Development and Feasibility Study. JMIR mHealth uHealth 2018, 6, e10074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puddephatt, J.-A.; Leightley, D.; Palmer, L.; Jones, N.; Mahmoodi, T.; Drummond, C.; Rona, R.J.; Fear, N.T.; Field, M.; Goodwin, L.; et al. A Qualitative Evaluation of the Acceptability of a Tailored Smartphone Alcohol Intervention for a Military Population: Information About Drinking for Ex-Serving Personnel (InDEx) App. JMIR mHealth uHealth 2019, 7, e12267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight-Agarwal, C.; Davis, D.L.; Williams, L.; Davey, R.; Cox, R.; Clarke, A. Development and Pilot Testing of the Eating4two Mobile Phone App to Monitor Gestational Weight Gain. JMIR mHealth uHealth 2015, 3, e44. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Paras, C.; Tippey, K.; Brown, E.; Sasangohar, F.; Creech, S.; Kum, H.-C.; Lawley, M.; Benzer, J.K. Post-traumatic Stress Disorder and Mobile Health: App Investigation and Scoping Literature Review. JMIR mHealth uHealth 2017, 5, e156. [Google Scholar] [CrossRef]
- Sun, S.; Folarin, A.A.; Ranjan, Y.; Rashid, Z.; Conde, P.; Stewart, C.; Cummins, N.; Matcham, F.; Dalla Costa, G.; Simblett, S.; et al. Using Smartphones and Wearable Devices to Monitor Behavioral Changes During COVID-19. J. Med. Internet Res. 2020, 22, e19992. [Google Scholar] [CrossRef]
- Angosto, S.; Berengüí, R.; Vegara-Ferri, J.M.; López-Gullón, J.M. Motives and Commitment to Sport in Amateurs during Confinement: A Segmentation Study. Int. J. Environ. Res. Public Health 2020, 17, 7398. [Google Scholar] [CrossRef] [PubMed]
- Wickersham, A.; Dickson, H.; Jones, R.; Pritchard, M.; Stewart, R.; Ford, T.; Downs, J. Educational Attainment Trajectories among Children and Adolescents with Depression, and the Role of Sociodemographic Characteristics: Longitudinal Data-Linkage Study. Br. J. Psychiatry 2021, 218, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Detry, M.A.; Ma, Y. Analyzing Repeated Measurements Using Mixed Models. JAMA 2016, 315, 407–408. [Google Scholar] [CrossRef]
- La Gatta, V.; Moscato, V.; Postiglione, M.; Sperli, G. An Epidemiological Neural network exploiting Dynamic Graph Structured Data applied to the COVID-19 outbreak. IEEE Trans. Big Data 2020, 7, 45–55. [Google Scholar] [CrossRef]
- Jalal, A.; Quaid, M.A.K.; Tahir, S.B.U.D.; Kim, K. A Study of Accelerometer and Gyroscope Measurements in Physical Life-Log Activities Detection Systems. Sensors 2020, 20, 6670. [Google Scholar] [CrossRef]
- King’s Move. Available online: https://www.kcl.ac.uk/sport/physical-activity/kings-move (accessed on 3 March 2021).
- Johnson, B. Prime Minister’s Statement on Coronavirus (COVID-19): 11 May 2020. Available online: https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-11-may-2020 (accessed on 3 March 2021).
- Koshoedo, S.; Simkhada, P.; Teijlingen, E.V. Review of Barriers to Engaging Black and Minority Ethnic Groups in Physical Activity in the United Kingdom. Glob. J. Healh Sci. 2009, 1, 85. [Google Scholar] [CrossRef] [Green Version]
- Ige-Elegbede, J.; Pilkington, P.; Gray, S.; Powell, J. Barriers and facilitators of physical activity among adults and older adults from Black and Minority Ethnic groups in the UK: A systematic review of qualitative studies. Prev. Med. Rep. 2019, 15, 100952. [Google Scholar] [CrossRef]
- James, P.; Weissman, J.; Wolf, J.; Mumford, K.G.; Contant, C.K.; Hwang, W.-T.; Taylor, L.; Glanz, K. Comparing GPS, Log, Survey, and Accelerometry to Measure Physical Activity. Am. J. Health Behav. 2016, 40, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Excluded | Analytical Sample | ||
|---|---|---|---|
| Student Users Excluded Due to Ineligibility or Missing Exposure Data (n = 265) | Sample for Steps Trajectory Modelling (n = 730) | Sample for Running Trajectory Modelling (n = 264) | |
| Sociodemographic Characteristics | n (%) | n (%) | n (%) |
| Gender | |||
| Male | 71 (26.8%) | 200 (27.4%) | 95 (36.0%) |
| Female | 174 (65.7%) | 530 (72.6%) | 169 (64.0%) |
| Other | 20 (7.6%) | - | - |
| Ethnicity | |||
| White | 129 (48.7%) | 388 (53.2%) | 162 (61.4%) |
| Black | 7 (2.6%) | 24 (3.3%) | 3 (1.1%) |
| Asian | 77 (29.1%) | 240 (32.9%) | 77 (29.2%) |
| Mixed | 21 (7.9%) | 39 (5.3%) | 11 (4.2%) |
| Other | 15 (5.7%) | 39 (5.3%) | 11 (4.2%) |
| Prefer not to say | 16 (6.0%) | - | - |
| Age in years as of 20 August 2020 | |||
| Median (IQR *) | 22.0 (20.0 to 25.0) | 22.0 (20.0 to 25.0) | 22.5 (20.0 to 25.0) |
| Fixed-Effects Parameter Estimates | IRR (95% CI) | p |
|---|---|---|
| Estimated group differences in week 0 | ||
| Gender | ||
| Male | Reference | - |
| Female | 0.79 (0.65 to 0.94) | 0.010 |
| Ethnicity | ||
| White | Reference | - |
| All other ethnic groups combined | 0.53 (0.45 to 0.62) | <0.001 |
| Age | 1.01 (1.00 to 1.03) | 0.160 |
| Slope of outcome on week in the reference group | ||
| Linear effect | 1.00 (0.97 to 1.03) | 0.984 |
| Quadratic effect | 1.00 (1.00 to 1.01) | 0.047 |
| Fixed-Effects Parameter Estimates | IRR (95% CI) | p |
|---|---|---|
| Estimated group differences in week 0 | ||
| Gender | ||
| Male | Reference | - |
| Female | 1.31 (0.97 to 1.77) | 0.082 |
| Ethnicity | ||
| White | Reference | - |
| All other ethnic groups combined | 0.57 (0.44 to 0.75) | <0.001 |
| Age | 1.02 (1.00 to 1.05) | 0.094 |
| Slope of outcome on week in the reference group | ||
| Linear effect | 1.01 (0.99 to 1.03) | 0.394 |
| Gender x week interaction | ||
| Female | 0.96 (0.94 to 0.99) | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wickersham, A.; Carr, E.; Hunt, R.; Davis, J.P.; Hotopf, M.; Fear, N.T.; Downs, J.; Leightley, D. Changes in Physical Activity among United Kingdom University Students Following the Implementation of Coronavirus Lockdown Measures. Int. J. Environ. Res. Public Health 2021, 18, 2792. https://doi.org/10.3390/ijerph18062792
Wickersham A, Carr E, Hunt R, Davis JP, Hotopf M, Fear NT, Downs J, Leightley D. Changes in Physical Activity among United Kingdom University Students Following the Implementation of Coronavirus Lockdown Measures. International Journal of Environmental Research and Public Health. 2021; 18(6):2792. https://doi.org/10.3390/ijerph18062792
Chicago/Turabian StyleWickersham, Alice, Ewan Carr, Ryan Hunt, Jordan P. Davis, Matthew Hotopf, Nicola T. Fear, Johnny Downs, and Daniel Leightley. 2021. "Changes in Physical Activity among United Kingdom University Students Following the Implementation of Coronavirus Lockdown Measures" International Journal of Environmental Research and Public Health 18, no. 6: 2792. https://doi.org/10.3390/ijerph18062792