
The Moderating Role of Pro-Innovative Leadership and Gender as an Enabler for Future Drone Transports in Healthcare Systems


Abstract
1. Introduction
2. Approach and Research Questions
3. Methods
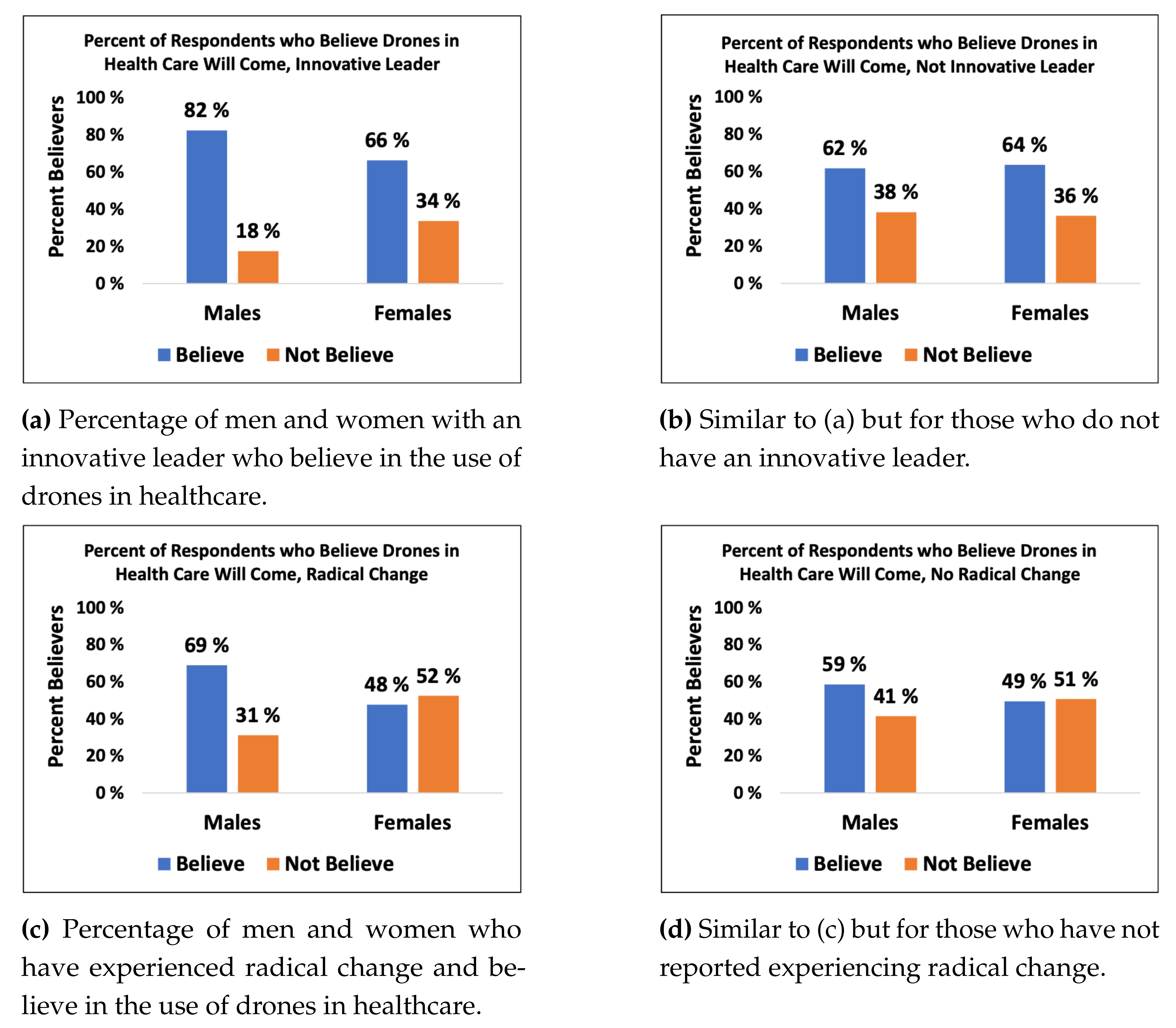
4. Results
5. Discussion
6. Strengths and Limitations
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
Questionnaire
- Your profession? Physician, Nurse, Bioengineer/laboratory employee, Other patient-related work, Administration, Other
- How do you rate your digital competence? Manage—Superuser
- Do you think digital solutions contribute to more efficient health services? Yes/No
- Do you think a new hospital will be beneficial for employees? Yes/No
- Do you think a new hospital will be beneficial for patients? Yes/No
- What do you know about drones in general? Very little—Very much
- Have you heard about drones in healthcare? Yes/No
- Do you think a future drone-based transportation of biological material (blood samples, biopsies, other material) is realistic? Yes/No/Don’t know
- In which area do you think a drone-based transportation can have a positive effect? Time, Quality, Digital, Collaboration and Communication, Don’t know
- In which situations do you think a drone-based transportation can be an advantage over current transportation methods? Long distances, Predictability, Possibility for immediate transport, Consolidations of laboratories, Don’t know
- Do you think your hospital will use drones in the future? Yes/No/Don’t know
- How long do you think it takes to fly a blood sample taken at Rikshospitalet with a drone to Ullevål? 0–15, 15–30, 30–45, 45–60, 60–90 min, Don’t know
- What do you believe are the biggest risks when it comes to drone flights for medical purposes? Flight safety, Data safety, Biological quality, Sample safety
- Does your leader support innovative ideas? Yes/No
- How does your leader react to innovative ideas? With rejecting/With doubt/Open/With interest/With support
- Do you have an arena to discuss and/or test innovative ideas in your unit? Yes/No
- Are you leaders active in planning for future change? Yes/No
- Are you involved in the planning for future change? Yes/No
- Do you think that technological development poses a risk for your hospital? Yes/No/ Don’t know
- From your perspective, does technological development require that the hospital needs to change? Yes/No/Don’t know
- Are you optimistic that technology can improve your work in the future? Pessimistic—Optimistic
- Are you concerned that your work might disappear or that you might lose work as a result of technological development? Yes/No
- Have you experienced significant medical-technical change in your area the last 5–10 years? Yes, radical/Yes, to some degree/Some, but less significant/No
- If you answered yes to the previous question, did technological development lead to logistical/operational change? Not relevant/Yes/No
- How satisfied are you with your work today? Not satisfied—Very satisfied
- What gives you most work satisfaction? Interesting work/Work with patients/Work autonomy/No work-related stress/Nice colleagues/Exciting change projects/Busy and the day goes fast/Good at my work/New challenges
- Do you experience good collaboration and communication with other professions in your work? Disagree—Agree
- Do you have enough time during the day to accomplish your work in a satisfactory way? Yes/No
- Will your work be less or more interesting in the future? Less interesting— More interesting
- How important is it for you to know what you need to do during the day? Not important—Very important
- How often do you have to do unpleasant work? Never/Rarely/Sometimes/Often
- What are the reasons for that feeling? Always behind/Poorly handled organisational change/Delayed work/Too much to do/Poor communication/No support/Inconsistent expectations/Too many patients/Concerned for patients
- Do you think the hospital needs other then medical competence in the future? Yes/No
- What are the biggest challenges for the healthcare system from your perspective? Shortage of resources/Increasing costs/Increasing unnecessary treatments/Competence/Poor communication/Specialisation
- Your age? 0–19/20–29/30–39/40–49/50–59/60 years or older
- Your gender? Female/Male
References
- Bitner, M.J. Service and technology: Opportunities and paradoxes. Manag. Serv. Qual. Int. J. 2001, 11, 375–379. [Google Scholar] [CrossRef]
- Coiera, E.; Hovenga, E.J.S. Building a Sustainable Health System. Yearb. Med. Inf. 2007, 16, 11–18. [Google Scholar]
- Haula, K.; Agbozo, E. A systematic review on unmanned aerial vehicles in Sub-Saharan Africa: A socio-technical perspective. Technol. Soc. 2020, 63, 101357. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; de la Rosa, S.; Sherman, J.; Blauvelt, C.; Matemba, C.; Maxim, L.; Defawe, O.D.; Gueye, A.; Robertson, J.; McKinney, J.; et al. Bi-directional drones to strengthen healthcare provision: Experiences and lessons from Madagascar, Malawi and Senegal. BMJ Glob. Health 2019, 4, e001541. [Google Scholar] [CrossRef]
- Ullah, F.; Sepasgozar, S.; Wang, C. A Systematic Review of Smart Real Estate Technology: Drivers of, and Barriers to, the Use of Digital Disruptive Technologies and Online Platforms. Sustainability 2018, 10, 3142. [Google Scholar] [CrossRef]
- Bai, C.; Dallasega, P.; Orzes, G.; Sarkis, J. Industry 4.0 technologies assessment: A sustainability perspective. Int. J. Prod. Econ. 2020, 229, 107776. [Google Scholar] [CrossRef]
- Amukele, T.K.; Sokoll, L.J.; Pepper, D.; Howard, D.P.; Street, J. Can unmanned aerial systems (drones) be used for the routine transport of chemistry, hematology, and coagulation laboratory specimens? PLoS ONE 2015, 10, e0134020. [Google Scholar] [CrossRef] [PubMed]
- Rosser, J.C., Jr.; Vignesh, V.; Terwilliger, B.A.; Parker, B.C. Surgical and Medical Applications of Drones: A Comprehensive Review. JSLS J. Soc. Laparoendosc. Surg. 2018, 22, e2018.00018. [Google Scholar] [CrossRef] [PubMed]
- Scalea, J.R.; Restaino, S.; Scassero, M.; Blankenship, G.; Bartlett, S.T.; Wereley, N. An Initial Investigation of Unmanned Aircraft Systems (UAS) and Real-Time Organ Status Measurement for Transporting Human Organs. IEEE J. Transl. Eng. Health Med. 2018, 6, 4000107. [Google Scholar] [CrossRef] [PubMed]
- Claesson, A.; Fredman, D.; Svensson, L.; Ringh, M.; Hollenberg, J.; Nordberg, P.; Rosenqvist, M.; Djarv, T.; Osterberg, S.; Lennartsson, J.; et al. Unmanned aerial vehicles (drones) in out-of-hospital-cardiac-arrest. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 124. [Google Scholar] [CrossRef]
- Haidari, L.A.; Brown, S.T.; Ferguson, M.; Bancroft, E.; Spiker, M.; Wilcox, A.; Ambikapathi, R.; Sampath, V.; Connor, D.L.; Lee, B.Y. The economic and operational value of using drones to transport vaccines. Vaccine 2016, 34, 4062–4067. [Google Scholar] [CrossRef] [PubMed]
- Hassanalian, M.; Abdelkefi, A. Classifications, applications, and design challenges of drones: A review. Prog. Aerosp. Sci. 2017, 91, 99–131. [Google Scholar] [CrossRef]
- Amukele, T.K.; Hernandez, J.; Snozek, C.L.H.; Wyatt, R.G.; Douglas, M.; Amini, R.; Street, J. Drone Transport of Chemistry and Hematology Samples Over Long Distances. Am. J. Clin. Pathol. 2017, 148, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lim, G.J.; Cho, J.; Côté, M.J. Drone-Aided Healthcare Services for Patients with Chronic Diseases in Rural Areas. J. Intell. Robot. Syst. 2017, 88, 163–180. [Google Scholar] [CrossRef]
- Otto, A.; Agatz, N.; Campbell, J.; Golden, B.; Pesch, E. Optimization approaches for civil applications of unmanned aerial vehicles (UAVs) or aerial drones: A survey. Networks 2018, 72, 411–458. [Google Scholar] [CrossRef]
- Nentwich, M.; Hórvath, D.M. Delivery Drones from a Technology Assessment Perspective; Overview Report, No.2018-01; ITA: Vienna, Austria, 2018; Available online: http://www.austriaca.at/0xc1aa5576_0x00377231.pdf (accessed on 8 December 2020).
- Khan, R.; Tausif, S.; Javed Malik, A. Consumer acceptance of delivery drones in urban areas. Int. J. Consum. Stud. 2018, 43, 87–101. [Google Scholar] [CrossRef]
- Kellermann, R.; Biehle, T.; Fischer, L. Drones for parcel and passenger transportation: A literature review. Transp. Res. Interdiscip. Perspect. 2020, 4, 100088. [Google Scholar] [CrossRef]
- SESAR Joint Undertaking (EU Body or Agency). European Drones Outlook Study; Publication Office of the EU: Luxembourg, 2017; Available online: https://op.europa.eu/s/oHuM (accessed on 8 December 2020). [CrossRef]
- Müller, S.; Rudolph, C.; Janke, C. Drones for last mile logistics: Baloney or part of the solution? Transp. Res. Procedia 2019, 41, 73–87. [Google Scholar] [CrossRef]
- Wulfovich, S.; Rivas, H.; Matabuena, P. Drones in Healthcare. In Digital Health; Springer International Publishing: Cham, Switzerland, 2018; pp. 159–168. [Google Scholar] [CrossRef]
- Rosamond, W.D.; Johnson, A.M.; Bogle, B.M.; Arnold, E.; Cunningham, C.J.; Picinich, M.; Williams, B.M.; Zègre-Hemsey, J.K. Drone Delivery of an Automated External Defibrillator. N. Engl. J. Med. 2020, 383, 1186–1188. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, K.A.; Wear, N.K.S.; Toska, K.; Hansbo, M.; Berg, J.P.; Fosse, E. Pathologic Blood Samples Tolerate Exposure to Vibration and High Turbulence in Simulated Drone Flights, but Plasma Samples Should be Centrifuged After Flight. IEEE J. Transl. Eng. Health Med. 2021, 9, 4000110. [Google Scholar] [CrossRef]
- Eichleay, M.; Evens, E.; Stankevitz, K.; Parker, C. Using the Unmanned Aerial Vehicle Delivery Decision Tool to Consider Transporting Medical Supplies via Drone. Glob. Health Sci. Pract. 2019, 7, 500. [Google Scholar] [CrossRef] [PubMed]
- Rabta, B.; Wankmüller, C.; Reiner, G. A drone fleet model for last-mile distribution in disaster relief operations. Int. J. Disaster Risk Reduct. 2018, 28, 107–112. [Google Scholar] [CrossRef]
- Carrillo-Larco, R.M.; Moscoso-Porras, M.; Taype-Rondan, A.; Ruiz-Alejos, A.; Bernabe-Ortiz, A. The use of unmanned aerial vehicles for health purposes: A systematic review of experimental studies. Glob. Health Epidemiol. Genom. 2018, 3, e13. [Google Scholar] [CrossRef] [PubMed]
- Kling, R.; Lamb, R. IT and organizational change in digital economies: A socio-technical approach. SIGCAS Comput. Soc. 1999, 29, 17–25. [Google Scholar] [CrossRef]
- Konert, A.; Smereka, J.; Szarpak, L. The Use of Drones in Emergency Medicine: Practical and Legal Aspects. Emerg. Med. Int. 2019, 2019, 3589792. [Google Scholar] [CrossRef]
- Lapointe, L.; Mignerat, M.; Vedel, I. The IT productivity paradox in health: A stakeholder’s perspective. Int. J. Med. Inform. 2011, 80, 102–115. [Google Scholar] [CrossRef]
- Jones, R.W.; Despotou, G. Unmanned Aerial Systems and Healthcare: Possibilities and Challenges. In Proceedings of the 2019 14th IEEE Conference on Industrial Electronics and Applications (ICIEA), Xi’an, China, 19–21 June 2019; pp. 189–194. [Google Scholar] [CrossRef]
- Jones, P.; Kijima, K. Systemic Design: Theory, Methods, and Practice; Springer: Tokyo, Japan, 2019; Volume 8. [Google Scholar]
- Behymer, K.J.; Flach, J.M. From Autonomous Systems to Sociotechnical Systems: Designing Effective Collaborations. She Ji J. Des. Econ. Innov. 2016, 2, 105–114. [Google Scholar] [CrossRef]
- Geels, F.W. System innovations and transitions to sustainability: Challenges for innovation theory. In Proceedings of the SPRU 40th Anniversary Conference, Brighton, UK, 7–9 September 2006; Volume 14. [Google Scholar]
- Krey, M.; Seiler, R. Usage and Acceptance of Drone Technology in Healthcare—Exploring Patients and Physicians Perspective. In Proceedings of the 52nd Hawaii International Conference on System Sciences, Maui, HI, USA, 8–11 January 2019. [Google Scholar]
- Laksham, K. Unmanned aerial vehicle (drones) in public health: A SWOT analysis.(Review Article). J. Fam. Med. Prim. Care 2019, 8, 342. [Google Scholar] [CrossRef] [PubMed]
- Mion, F.U. Flying Drones to Exchange Lab Samples: Service Innovation by the Swiss Multisite Hospital EOC. In Service Design and Service Thinking in Healthcare and Hospital Management: Theory, Concepts, Practice; Pfannstiel, M.A., Rasche, C., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 463–479. [Google Scholar] [CrossRef]
- Hiebert, B.; Nouvet, E.; Jeyabalan, V.; Donelle, L. The Application of Drones in Healthcare and Health-Related Services in North America: A Scoping Review. Drones (Basel) 2020, 4, 30. [Google Scholar] [CrossRef]
- Seyfang, G.; Smith, A. Grassroots innovations for sustainable development: Towards a new research and policy agenda. Environ. Politics 2007, 16, 584–603. [Google Scholar] [CrossRef]
- Smith, A. Translating Sustainabilities between Green Niches and Socio-Technical Regimes. Technol. Anal. Strateg. Manag. 2007, 19, 427–450. [Google Scholar] [CrossRef]
- Boons, F.; McMeekin, A.; Edward Elgar, P. Handbook of Sustainable Innovation; Edward Elgar Publishing: Cheltenham, UK, 2019. [Google Scholar]
- Geels, F.W. Technological transitions as evolutionary reconfiguration processes: A multi-level perspective and a case-study. Res. Policy 2002, 31, 1257–1274. [Google Scholar] [CrossRef]
- Geels, F.W. From sectoral systems of innovation to socio-technical systems: Insights about dynamics and change from sociology and institutional theory. Res. Policy 2004, 33, 897–920. [Google Scholar] [CrossRef]
- van der Geest, S.; Speckmann, J.D.; Streefland, P.H. Primary health care in a multi-level perspective: Towards a research agenda. Soc. Sci. Med. 1990, 30, 1025–1034. [Google Scholar] [CrossRef]
- Geels, F. Socio-technical transitions to sustainability: A review of criticisms and elaborations of the Multi-Level Perspective. Curr. Opin. Environ. Sustain. 2019, 39, 187–201. [Google Scholar] [CrossRef]
- Geels, F.W. Technological Transitions and System Innovations: A Co-Evolutionary and Socio-Technical Analysis; Edward Elgar Publishing: Cheltenham, UK, 2005. [Google Scholar]
- Rotmans, J.; Kemp, R.P.M.; van Asselt, M. More Evolution than Revolution: Transition Management in Public Policy. Foresight J. Insur. Risk Manag. 2001, 3, 15–31. [Google Scholar] [CrossRef]
- Geels, F.; Raven, R. Non-linearity and Expectations in Niche-Development Trajectories: Ups and Downs in Dutch Biogas Development (1973–2003). Technol. Anal. Strateg. Manag. 2006, 18, 375–392. [Google Scholar] [CrossRef]
- Schield, M. Random Sampling versus Representative Samples. In ASA 1994 Proceedings of the Section on Statistical Education; American Statistical Association: Boston, MA, USA, 1994; pp. 107–110. [Google Scholar]
- Salkind, N. Encyclopedia of Research Design; SAGE: Los Angeles, CA, USA, 2010. [Google Scholar]
- Berridge, C.; Furseth, P.I.; Cuthbertson, R.; Demello, S. Technology-Based Innovation for Independent Living: Policy and Innovation in the United Kingdom, Scandinavia, and the United States. J. Aging Soc. Policy 2014, 26, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Alba, J.W.; Hutchinson, J.W. Dimensions of Consumer Expertise. J. Consum. Res. 1987, 13, 411–454. [Google Scholar] [CrossRef]
- Rosenbloom, D.; Berton, H.; Meadowcroft, J. Framing the sun: A discursive approach to understanding multi-dimensional interactions within socio-technical transitions through the case of solar electricity in Ontario, Canada. Res. Policy 2016, 45, 1275–1290. [Google Scholar] [CrossRef]
- Hwang, J.; Lee, J.S.; Kim, H. Perceived innovativeness of drone food delivery services and its impacts on attitude and behavioral intentions: The moderating role of gender and age. Int. J. Hosp. Manag. 2019, 81, 94–103. [Google Scholar] [CrossRef]
- Druckman, J.N.; Bolsen, T. Framing, Motivated Reasoning, and Opinions About Emergent Technologies. J. Commun. 2011, 61, 659–688. [Google Scholar] [CrossRef]
- Cohen, T.; Jones, P. Technological advances relevant to transport—Understanding what drives them. Transp. Res. Part A Policy Pract. 2020, 135, 80–95. [Google Scholar] [CrossRef]
- Roberts, C.; Geels, F. Public Storylines in the British Transition from Rail to Road Transport (1896–2000): Discursive Struggles in the Multi-Level Perspective. Sci. Cult. 2018, 27, 513–542. [Google Scholar] [CrossRef]
- Truog, S.; Maxim, L.; Matemba, C.; Blauvelt, C.; Ngwira, H.; Makaya, A.; Moreira, S.; Lawrence, E.; Ailstock, G.; Weitz, A.; et al. Insights Before Flights: How Community Perceptions Can Make or Break Medical Drone Deliveries. Drones (Basel) 2020, 4, 51. [Google Scholar] [CrossRef]
- Clothier, R.A.; Greer, D.A.; Greer, D.G.; Mehta, A.M. Risk Perception and the Public Acceptance of Drones. Risk Anal 2015, 35, 1167–1183. [Google Scholar] [CrossRef] [PubMed]
- Berg, M. Patient care information systems and health care work: A sociotechnical approach. Int. J. Med. Inform. 1999, 55, 87–101. [Google Scholar] [CrossRef]
- Burns, L.R.; Bradley, E.H.; Weiner, B.J. Shortell and Kaluzny’s Health Care Management: Organization, Design, and Behavior, 7th ed.; Cengage: Boston, MA, USA, 2020. [Google Scholar]
- OECD. Health Expenditure-OECD. Available online: https://www.oecd.org/els/health-systems/health-expenditure.htm#:~:text=LatestOECDfiguresonhealth,2020%2CupdatedinNovember2020 (accessed on 8 February 2021).
- Wallis, W.A. The Statistical Research Group, 1942–1945. J. Am. Stat. Assoc. 1980, 75, 334–335. [Google Scholar] [CrossRef]
- Lazar, J. Research Methods in Human-Computer Interaction; John Wiley: Chichester, UK, 2010. [Google Scholar]
- Amabile, T.M.; Conti, R.; Coon, H.; Lazenby, J.; Herron, M. Assessing the Work Environment for Creativity. Acad. Manag. J. 1996, 39, 1154–1184. [Google Scholar] [CrossRef]


{kind=link}
| Profession | Administration (n = 59) | Bioengineer (n = 54) | Nurse (n = 110) | Other (n = 47) | Other Patient Related (n = 55) | Physician (n = 75) | Total Population | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Category/Variable | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Background | ||||||||||||||
| Mean Age (years) | 41.2 | 11.5 | 39.8 | 12.4 | 32.9 | 12.1 | 39.1 | 13.1 | 39.0 | 11.4 | 35.2 | 12.9 | 37.30 | 14.3 |
| Years Worked in Hospital (years) | 13.5 | 9.5 | 14.8 | 12.4 | 9.3 | 10.2 | 10.1 | 10.7 | 9.3 | 9.9 | 7.2 | 8.3 | 10.6 | 9.6 |
| Self Assessed Digital Competence (score 1–5) | 3.8 | 0.7 | 3.9 | 0.8 | 3.7 | 0.7 | 3.8 | 0.9 | 3.8 | 0.9 | 3.6 | 0.9 | 3.8 | 0.64 |
| Positive Culture for Change (% yes) | 88% | 33% | 74% | 44% | 90% | 30% | 78% | 42% | 73% | 45% | 83% | 38% | 82% | 38% |
| Innovative Leadership (% yes) | 83% | 38% | 74% | 44% | 84% | 37% | 70% | 47% | 71% | 46% | 69% | 46% | 76% | 43% |
| Arena for Innovation (yes) | 59% | 50% | 59% | 50% | 62% | 49% | 65% | 48% | 49% | 50% | 55% | 50% | 57% | 50% |
| Knowledge of Drones | ||||||||||||||
| Knowledge of Drones in Health Care (% yes) | 73% | 45% | 76% | 43% | 56% | 70% | 72% | 62% | 55% | 63% | 49% | 62% | 62% | 63% |
| General Knowledge of Drones (score 1–5) | 2.93 | 0.92 | 2.75 | 0.97 | 2.32 | 0.82 | 3.0 | 1.20 | 2.55 | 1.12 | 2.64 | 1.13 | 2.7 | 1.0 |
| Believe Drones in Future Health Care (% yes) | 81% | 39% | 67% | 48% | 73% | 45% | 54% | 50% | 60% | 49% | 77% | 42% | 70% | 45% |
| Believe Drones in Own Hospital in Future (% yes) | 66% | 48% | 63% | 49% | 67% | 47% | 74% | 44% | 53% | 50% | 64% | 48% | 65% | 48% |
| Technological Experience and Expectations | ||||||||||||||
| Experienced Radical Technological Changes (% yes) | 32% | 47% | 59% | 50% | 39% | 49% | 33% | 47% | 47% | 50% | 49% | 50% | 43% | 49% |
| Believe New Hospital Positive for Employees (% yes) | 68% | 47% | 65% | 48% | 66% | 55% | 70% | 47% | 64% | 73% | 53% | 55% | 57% | 49% |
| Believe New Hospital Positive for Patients (% yes) | 75% | 44% | 69% | 47% | 69% | 52% | 76% | 48% | 58% | 66% | 56% | 55% | 61% | 48% |
| Believe Digitalization may improve Health Care (% yes) | 97% | 18% | 98% | 14% | 98% | 19% | 98% | 15% | 98% | 13% | 99% | 12% | 98% | 15% |
| Hospital need Change to adapt to Technol. Development (% yes) | 92% | 28% | 87% | 34% | 83% | 38% | 65% | 48% | 80% | 40% | 75% | 44% | 82% | 38% |
| Worried Own Work May be removed by Future Technology (%) | 16% | 39% | 9% | 32% | 29% | 39% | 19% | 46% | 12% | 37% | 16% | 36% | 17% | 37% |
| Positive Expectations Technology Improve Own Work (scale 1–5) | 3.90 | 0.90 | 3.87 | 0.99 | 3.93 | 0.82 | 3.87 | 1.26 | 3.62 | 1.03 | 3.67 | 0.93 | 3.83 | 0.81 |
| Males (n = 138) | Females (n = 262) | |||||||
|---|---|---|---|---|---|---|---|---|
| Category/Variable | Mean | SD | Mean | SD | Mean Male/Female | Sig. (2-Tailed) | Mean Difference | Std. Error Difference |
| Background | ||||||||
| Mean Age | 40.07 | 11.68 | 35.46 | 12.70 | 13% | 0.01 | 3.25 | 1.87 |
| Years Worked in Hospital | 10.06 | 9.72 | 10.54 | 10.73 | −5% | ns | −0.99 | ns |
| Self Assessed Digital Competence | 3.92 | 0.84 | 3.67 | 0.78 | 7% | 0.01 | 0.25 | ns |
| Positive Culture for Change | 82% | 39% | 83% | 38% | −1% | 0.05 | 0.06 | <0.05 |
| Innovative Leadership | 75% | 44% | 77% | 42% | −3% | ns | −0.02 | <0.05 |
| Arena for Innovation | 56% | 50% | 60% | 49% | −7% | ns | −0.03 | <0.05 |
| Knowledge of Drones | ||||||||
| General Knowledge of Drone | 3.08 | 0.97 | 2.40 | 0.99 | 28% | 0.001 | 0.69 | <0.01 |
| Knowledge of Drones in Health Care | 67% | 51% | 59% | 65% | 15% | 0.00 | 0.20 | <0.05 |
| Believe Drones in Future Health Care | 78% | 42% | 66% | 47% | 17% | 0.01 | 0.02 | <0.05 |
| Technological Experience and Expectations | ||||||||
| Experienced Radical Technological Changes | 43% | 50% | 43% | 50% | 1% | ns | −0.00 | ns |
| Believe New Hospital Positive for Employees | 64% | 55% | 64% | 55% | 1% | ns | 0.04 | ns |
| Believe New Hospital Positive for Patients | 67% | 52% | 67% | 54% | −1% | ns | 0.03 | ns |
| Believe Digitalization may improve Healthcare | 95% | 22% | 99% | 9% | −4% | ns | −0.04 | 0.02 |
| Hospital need to Change to adapt to Technological Change | 1.28 | 0.36 | 1.41 | 0.41 | −9% | 0.04 | −0.18 | ns |
| Worried Own Work May be removed by Future Technology | 14% | 34% | 19% | 39% | −26% | 0.01 | 0.01 | <0.05 |
| Positive Expectations for own Work | 3.80 | 0.87 | 3.82 | 1.02 | −1% | ns | −0.08 | ns |
| Variable | B | S.E. | Wald | Sig. | Exp(B) |
|---|---|---|---|---|---|
| General Knowledge of Drones | 0.36 | 0.14 | 6.46 | 0.001 | 1.44 |
| Knowledge of Drones in Healthcare | 0.57 | 0.22 | 7.08 | 0.008 | 1.773 |
| Experienced Radical Technological Changes | 0.66 | 0.26 | 6.61 | 0.010 | 1.929 |
| Innovative Leadership | 0.63 | 0.31 | 4.18 | 0.041 | 1.872 |
| Believe Digitalization may improve Healthcare | 0.60 | 0.14 | 18.32 | 0.000 | 1.825 |
| Nurse | 0.67 | 0.31 | 4.69 | 0.030 | 1.95 |
| Physician | 0.89 | 0.36 | 5.97 | 0.015 | 2.43 |
| Administration | 1.00 | 0.40 | 6.32 | 0.012 | 2.73 |
| Age | −0.02 | 0.01 | 4.27 | 0.039 | 0.98 |
| Constant | −1.10 | 0.98 | 1.27 | 0.260 | 0.33 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comtet, H.E.; Johannessen, K.-A. The Moderating Role of Pro-Innovative Leadership and Gender as an Enabler for Future Drone Transports in Healthcare Systems. Int. J. Environ. Res. Public Health 2021, 18, 2637. https://doi.org/10.3390/ijerph18052637
Comtet HE, Johannessen K-A. The Moderating Role of Pro-Innovative Leadership and Gender as an Enabler for Future Drone Transports in Healthcare Systems. International Journal of Environmental Research and Public Health. 2021; 18(5):2637. https://doi.org/10.3390/ijerph18052637
Chicago/Turabian StyleComtet, Hans E., and Karl-Arne Johannessen. 2021. "The Moderating Role of Pro-Innovative Leadership and Gender as an Enabler for Future Drone Transports in Healthcare Systems" International Journal of Environmental Research and Public Health 18, no. 5: 2637. https://doi.org/10.3390/ijerph18052637
APA StyleComtet, H. E., & Johannessen, K.-A. (2021). The Moderating Role of Pro-Innovative Leadership and Gender as an Enabler for Future Drone Transports in Healthcare Systems. International Journal of Environmental Research and Public Health, 18(5), 2637. https://doi.org/10.3390/ijerph18052637