
A New Perspective for Improving the Human Resource Development of Primary Medical and Health Care Institutions: A Structural Equation Model Study

Abstract
1. Introduction
2. Pre-Investigation
2.1. Participants and Procedures
2.2. Measures
2.3. Data Analysis
3. Investigation
3.1. Participants and Procedures
3.2. Measures
3.3. Data Analysis
3.4. Exploratory Factor Analysis and Research Hypotheses
3.4.1. Sense of Gain (SG)
3.4.2. Remuneration and Development (RD)
3.4.3. Internal Organization Development (IOD)
3.4.4. Condition of the City Where the PMHCI Is Located (CCPL)
3.4.5. Job Responsibilities (JR)
3.4.6. Family Support (FS)
3.4.7. Patient Factor (PF)
3.5. Confirmatory Factor Analysis
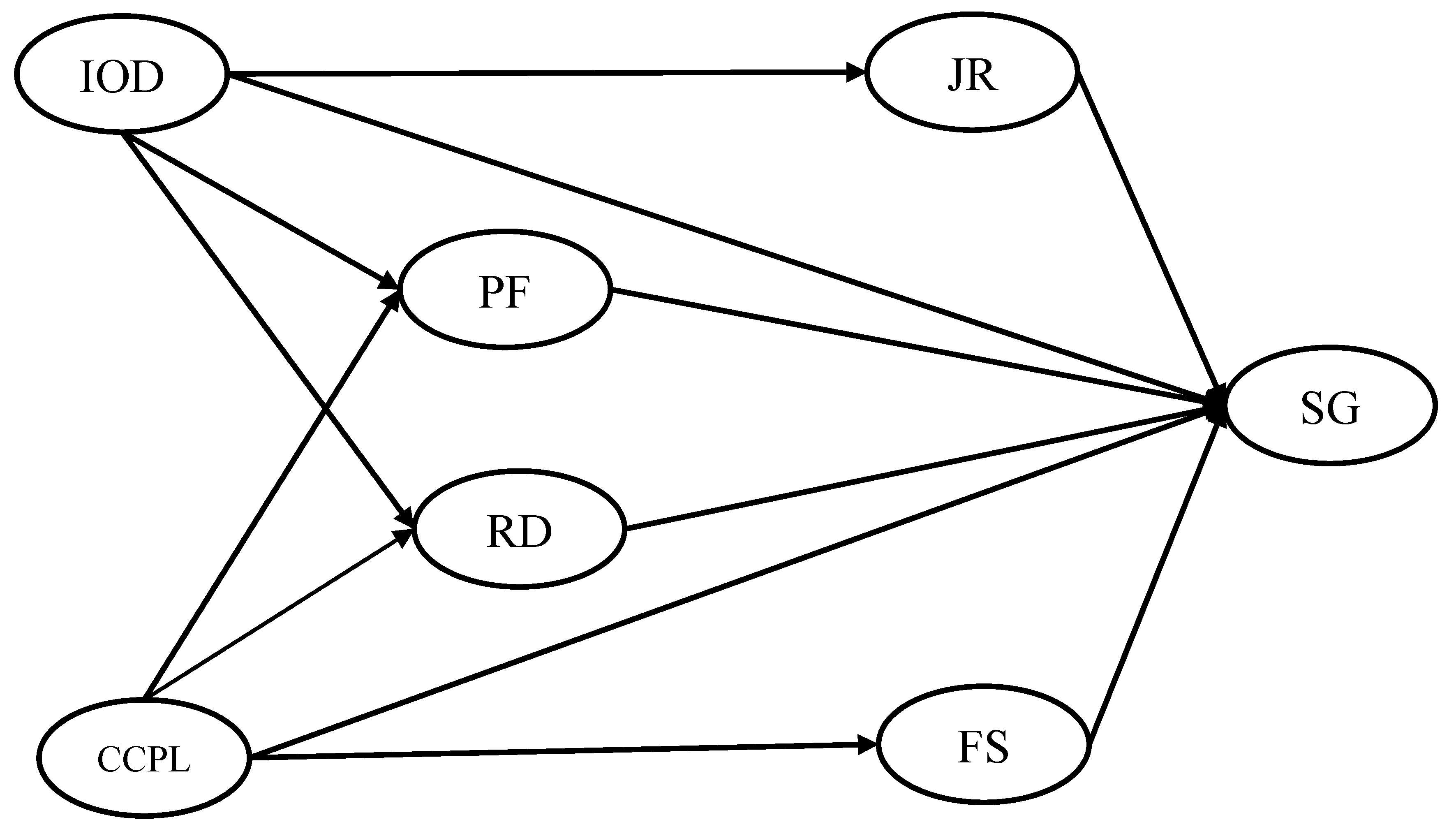
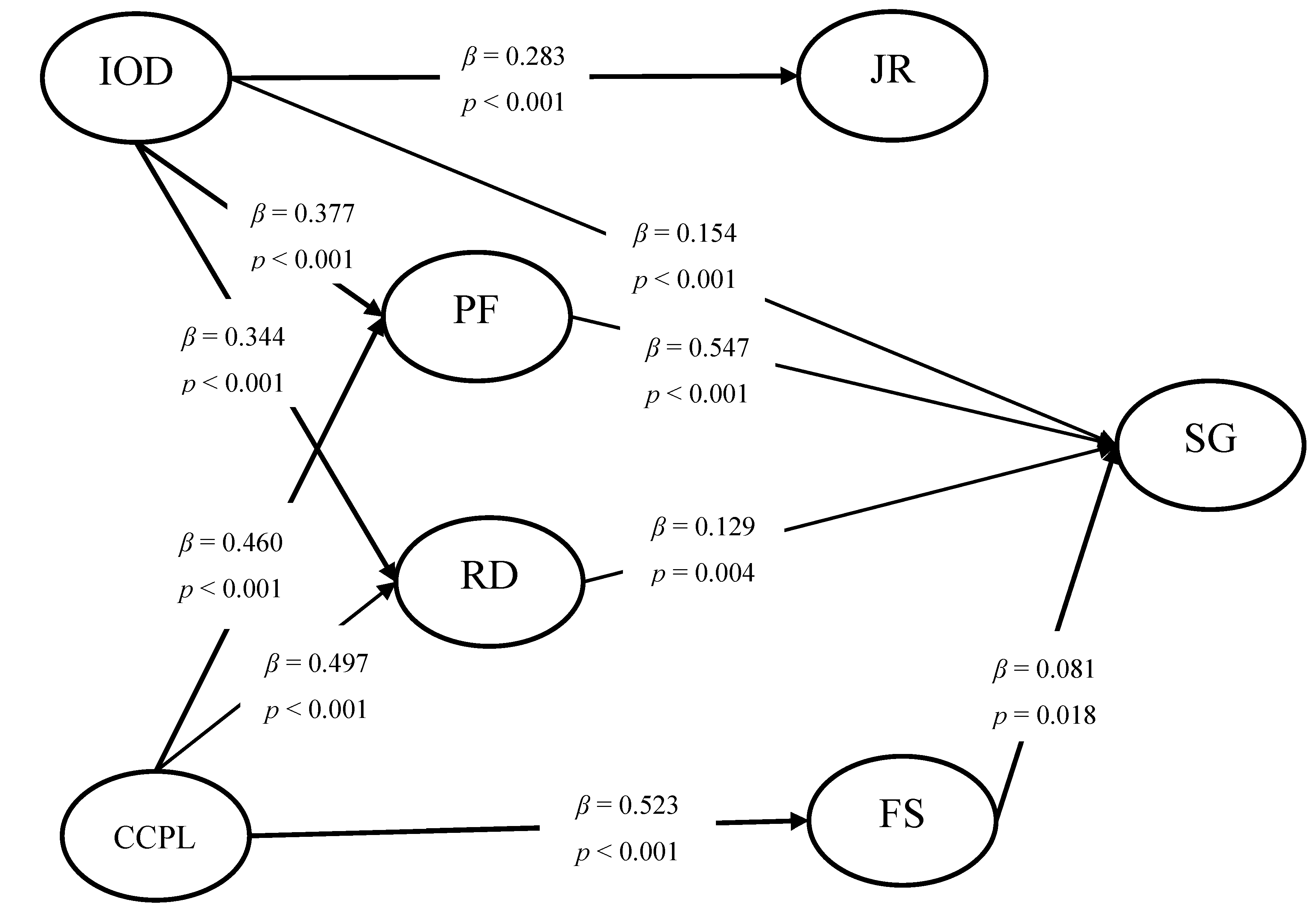
3.6. Structural Model Analysis
4. Discussion
Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Magnussen, L.; Ehiri, J.; Jolly, P. Comprehensive versus selective primary health care: Lessons for global health policy. Health Aff. 2004, 23, 167–176. [Google Scholar] [CrossRef]
- Gyawali, B.; Khanal, P.; Mishra, S.R.; van Teijlingen, E.; Meyrowitsch, D.W. Building Strong Primary Health Care to Tackle the Growing Burden of Non-Communicable Diseases in Nepal. Glob. Health Action 2020, 13. [Google Scholar] [CrossRef]
- Gemelas, J.C. Post-ACA Trends in the US Primary Care Physician Shortage with Index of Relative Rurality. J. Rural Health 2020. [Google Scholar] [CrossRef]
- Yip, W.; Hsiao, W. China’s health care reform: A tentative assessment. China Econ. Rev. 2009, 20, 613–619. [Google Scholar] [CrossRef]
- Lu, C.; Zhang, Z.X.; Lan, X.T. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.H.; Wang, Y.; Zeng, Y.X.; Gao, G.F.; Liang, X.F.; Zhou, M.G.; Wan, X.; Yu, S.C.; Jiang, Y.H.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Zheng, A.; Fang, Q.; Zhu, Y.; Jiang, C.; Jin, F.; Wang, X. An application of ARIMA model for predicting total health expenditure in China from 1978–2022. J. Glob. Health 2020, 10. [Google Scholar] [CrossRef]
- Li, J.M.; Chen, X.L.; Han, X.L.; Zhang, G.H. Spatiotemporal matching between medical resources and population ageing in China from 2008 to 2017. BMC Public Health 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Huang, X.; Zhang, X.; Chen, L. Family Economic Burden of Elderly Chronic Diseases: Evidence from China. Healthcare 2019, 7, 99. [Google Scholar] [CrossRef]
- Yang, G.H.; Kong, L.Z.; Zhao, W.H.; Wan, X.; Zhai, Y.; Chen, L.C.; Koplan, J.P. Health System Reform in China 3 Emergence of chronic non-communicable diseases in China. Lancet 2008, 372, 1697–1705. [Google Scholar] [CrossRef]
- Gong, P.; Liang, S.; Carlton, E.J.; Jiang, Q.W.; Wu, J.Y.; Wang, L.; Remais, J.V. Urbanisation and health in China. Lancet 2012, 379, 843–852. [Google Scholar] [CrossRef]
- CPC Central Committee; The State Council. Opinions on Deepening the Reform of the Medical and Health Care System. Available online: http://www.gov.cn/test/2009-04/08/content_1280069.htm (accessed on 26 December 2020).
- Shen, X.; Yang, W.; Sun, S. Analysis of the Impact of China’s Hierarchical Medical System and Online Appointment Diagnosis System on the Sustainable Development of Public Health: A Case Study of Shanghai. Sustainability 2019, 11, 6564. [Google Scholar] [CrossRef]
- The State Council of the People’s Republic of China. Guidance on Promoting the Construction of Hierarchical Medical System. Available online: http://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm (accessed on 27 December 2020).
- Li, M.N.; Zhang, Y.; Lu, Y.; Yu, W.Y.; Nong, X.; Zhang, L.L. Factors influencing two-way referral between hospitals and the community in China: A system dynamics simulation model. Simul-T Soc. Mod. Sim. 2018, 94, 765–782. [Google Scholar] [CrossRef]
- The Center of Statistical Information National Health Commission of the Republic of Health. China Health Statistics Yearbook 2020; Peking Union Medical College Press: Beijing, China, 2020.
- Wang, H.H.X.; Wang, J.J.; Wong, S.Y.S.; Wong, M.C.S.; Li, F.J.; Wang, P.X.; Zhou, Z.H.; Zhu, C.Y.; Griffiths, S.M.; Mercer, S.W. Epidemiology of multimorbidity in China and implications for the healthcare system: Cross-sectional survey among 162,464 community household residents in southern China. BMC Med. 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Parry, J. GP based primary care is only just starting to emerge in China. Br. Med. J. 2010, 341. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Sun, T.; Jin, Y.S.; Wang, Y.P. Spatial Organization of Hierarchical Medical Services within the City Proper of Tianjin, China: Towards Efficient Medical Alliances. Sustainability 2019, 11, 229. [Google Scholar] [CrossRef]
- Yip, W.C.-M.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Li, J.; Wang, P.; Kong, X.; Liang, H.; Zhang, X.; Shi, L. Patient satisfaction between primary care providers and hospitals: A cross-sectional survey in Jilin province, China. Int. J. Qual. Health C 2016, 28, 346–354. [Google Scholar] [CrossRef]
- Xu, X.L.; Zhou, L.L.; Antwi, H.A.; Chen, X. Evaluation of health resource utilization efficiency in community health centers of Jiangsu Province, China. Hum. Resour. Health 2018, 16. [Google Scholar] [CrossRef]
- Huang, M.F.; Wei, D.H.; Rubino, L.; Wang, L.S.; Li, D.Z.; Ding, B.F.; Li, G. “Three essential elements” of the primary health care system: A comparison between California in the US and Guangdong in China. Fam. Med. Community Health 2015, 3, 23–29. [Google Scholar] [CrossRef]
- Luo, Z.N.; Bai, X.; Min, R.; Tang, C.M.; Fang, P.Q. Factors influencing the work passion of Chinese community health service workers: An investigation in five provinces. BMC Fam. Pract. 2014, 15. [Google Scholar] [CrossRef]
- Ge, C.X.; Fu, J.L.; Chang, Y.; Wang, L. Factors associated with job satisfaction among Chinese community health workers: A cross-sectional study. BMC Public Health 2011, 11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.J.; Yang, R.R.; Wang, W.; Gillespie, J.; Clarke, S.; Yan, F. Job satisfaction of urban community health workers after the 2009 healthcare reform in China: A systematic review. Int. J. Qual. Health C 2016, 28, 14–21. [Google Scholar] [CrossRef]
- Chin-Quee, D.; Mugeni, C.; Nkunda, D.; Uwizeye, M.R.; Stockton, L.L.; Wesson, J. Balancing workload, motivation and job satisfaction in Rwanda: Assessing the effect of adding family planning service provision to community health worker duties. Reprod. Health 2016, 13. [Google Scholar] [CrossRef]
- Liu, G.G.; Vortherms, S.A.; Hong, X. China’s Health Reform Update. Annu. Rev. Public Health 2017, 38, 431–448. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, R.J. Implicit Theories of Intelligence, Creativity, and Wisdom. J. Pers. Soc. Psychol. 1985, 49, 607–627. [Google Scholar] [CrossRef]
- Dweck, C.S.; Chiu, C.Y.; Hong, Y.Y. Implicit Theories and Their Role in Judgments and Reactions—A World from 2 Perspectives. Psychol. Inq. 1995, 6, 267–285. [Google Scholar] [CrossRef]
- Burnette, J.L.; O’Boyle, E.H.; VanEpps, E.M.; Pollack, J.M.; Finkel, E.J. Mind-Sets Matter: A Meta-Analytic Review of Implicit Theories and Self-Regulation. Psychol. Bull. 2013, 139, 655–701. [Google Scholar] [CrossRef]
- Lord, R.G.; Epitropaki, O.; Foti, R.J.; Hansbrough, T.K. Implicit leadership theories, implicit followership theories, and dynamic processing of leadership information. Annu. Rev. Organ. Psychol. Organ. Behav. 2020, 7, 49–74. [Google Scholar] [CrossRef]
- De France, K.; Hollenstein, T. Implicit theories of emotion and mental health during adolescence: The mediating role of emotion regulation. Cogn. Emot. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.; O’Connor, A.; Seery, N.; Hyland, T.; Canty, D. Implicit theories of intelligence in STEM education: Perspectives through the lens of technology education students. Int. J. Technol. Des. Educ. 2019, 29, 75–106. [Google Scholar] [CrossRef]
- Ashton, M.C.; Lee, K. A defence of the lexical approach to the study of personality structure. Eur. J. Personal. 2005, 19, 5–24. [Google Scholar] [CrossRef]
- Saucier, G.; Goldberg, L.R. Lexical studies of indigenous personality factors: Premises, products, and prospects. J. Pers. 2001, 69, 847–879. [Google Scholar] [CrossRef] [PubMed]
- Chapman, D.S.; Reeves, P.; Chapin, M. A Lexical Approach to Identifying Dimensions of Organizational Culture. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Thalmayer, A.G.; Saucier, G.; Ole-Kotikash, L.; Payne, D. Personality Structure in East and West Africa: Lexical Studies of Personality in Maa and Supyire-Senufo. J. Pers. Soc. Psychol. 2020, 119, 1132–1152. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.E. The Main Dimensions of Sport Personality Traits: A Lexical Approach. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice—A review and recommended 2-step approach. Psychol. Bull. 1988, 103, 411–423. [Google Scholar] [CrossRef]
- Golini, N.; Egidi, V. The Latent Dimensions of Poor Self-Rated Health: How Chronic Diseases, Functional and Emotional Dimensions Interact Influencing Self-Rated Health in Italian Elderly. Soc. Indic. Res. 2016, 128, 321–339. [Google Scholar] [CrossRef]
- Fan, N. Strategy Use in Second Language Vocabulary Learning and Its Relationships with the Breadth and Depth of Vocabulary Knowledge: A Structural Equation Modeling Study. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Harerimana, A.; Mtshali, N.G. Using Exploratory and Confirmatory Factor Analysis to understand the role of technology in nursing education. Nurse Educ. Today 2020, 92. [Google Scholar] [CrossRef]
- Nikolaou, P.; Basbas, S.; Politis, I.; Borg, G. Trip and Personal Characteristics towards the Intention to Cycle in Larnaca, Cyprus: An EFA-SEM Approach. Sustainability 2020, 12, 4250. [Google Scholar] [CrossRef]
- Joseph, F.; Hair, J.; William, C.B.; Barry, J.B.; Rolph, E.A. Multivariate Data Analysis; Pearson Education Limited: Edinburgh, UK, 2014. [Google Scholar]
- Anand, S.; Barnighausen, T. Health workers at the core of the health system: Framework and research issues. Health Policy 2012, 105, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Head, B.; Middleton, A.; Zeigler, C. Work Satisfaction among Hospice and Palliative Nurses. J. Hosp. Palliat. Nurses 2019, 21, E1–E11. [Google Scholar] [CrossRef]
- Vikstrom, S.; Johansson, K. Professional pride: A qualitative descriptive study of nursing home staff’s experiences of how a quality development project influenced their work. J. Clin. Nurs. 2019, 28, 2760–2768. [Google Scholar] [CrossRef] [PubMed]
- Valizadeh, L.; Zamanzadeh, V.; Habibzadeh, H.; Alilu, L.; Gillespie, M.; Shakibi, A. Threats to nurses’ dignity and intent to leave the profession. Nurs. Ethics 2018, 25, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Guo, A.; Wang, Y.; Zhao, Y.; Yang, X.; Li, H.; Duckitt, R.; Liang, W. Human Resource Staffing and Service Functions of Community Health Services Organizations in China. Ann. Fam. Med. 2008, 6, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Morrissy, L.; Boman, P.; Mergler, A. Nursing a Case of the Blues: An Examination of the Role of Depression in Predicting Job-Related Affective Well-Being in Nurses. Issues Ment. Health Nurs. 2013, 34, 158–168. [Google Scholar] [CrossRef]
- Willemse, B.M.; De Jonge, J.; Smit, D.; Visser, Q.; Depla, M.F.I.A.; Pot, A.M. Staff’s person-centredness in dementia care in relation to job characteristics and job-related well-being: A cross-sectional survey in nursing homes. J. Adv. Nurs. 2015, 71, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Pizarro, J.P.; Martin, M.E.; Di Giusto, C. Adolescents Work Values. Rev. Psicodidact. 2011, 16, 381–399. [Google Scholar]
- He, R.; Liu, J.; Zhang, W.-H.; Zhu, B.; Zhang, N.; Mao, Y. Turnover intention among primary health workers in China: A systematic review and meta-analysis. BMJ Open 2020, 10. [Google Scholar] [CrossRef]
- Liu, J.A.; Wang, Q.; Lu, Z.X. Job satisfaction and its modeling among township health center employees: A quantitative study in poor rural China. BMC Health Serv. Res. 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Jin, Y.; Wang, D.; Zhao, S.; Sang, X.; Yuan, B. Job satisfaction, burnout, and turnover intention among primary care providers in rural China: Results from structural equation modeling. BMC Fam. Pract. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Hu, X.-M.; Huang, X.-L.; Zhuang, X.-D.; Guo, P.; Feng, L.-F.; Hu, W.; Chen, L.; Zou, H.; Hao, Y.-T. The relationship between job satisfaction, work stress, work-family conflict, and turnover intention among physicians in Guangdong, China: A cross-sectional study. BMJ Open 2017, 7. [Google Scholar] [CrossRef]
- Espasandín-Bustelo, F.; Ganaza-Vargas, J.; Diaz-Carrion, R. Employee happiness and corporate social responsibility: The role of organizational culture. Empl. Relat. Int. J. 2020. [Google Scholar] [CrossRef]
- Zhang, W.W.; Ung, C.O.L.; Lin, G.H.; Liu, J.; Li, W.J.; Hu, H.; Xi, X.Y. Factors Contributing to Patients’ Preferences for Primary Health Care Institutions in China: A Qualitative Study. Front. Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Van der Doef, M.; Maes, S. The Job Demand-Control(-Support) model and psychological well-being: A review of 20 years of empirical research. Work Stress 1999, 13, 87–114. [Google Scholar] [CrossRef]
- Haeusser, J.A.; Mojzisch, A.; Niesel, M.; Schulz-Hardt, S. Ten years on: A review of recent research on the Job Demand-Control (-Support) model and psychological well-being. Work Stress 2010, 24, 1–35. [Google Scholar] [CrossRef]
- Kwok, S.Y.C.L.; Cheng, L.; Wong, D.F.K. Family Emotional Support, Positive Psychological Capital and Job Satisfaction among Chinese White-Collar Workers. J. Happiness Stud. 2015, 16, 561–582. [Google Scholar] [CrossRef]
- Chan, X.W.; Kalliath, P.; Chan, C.; Kalliath, T. How does family support facilitate job satisfaction? Investigating the chain mediating effects of work-family enrichment and job-related well-being. Stress Health 2020, 36, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Nei, D.; Snyder, L.A.; Litwiller, B.J. Promoting retention of nurses A meta-analytic examination of causes of nurse turnover. Health Care Manag. Rev. 2015, 40, 237–253. [Google Scholar] [CrossRef]
- Hoffner, C.A.; Levine, K.J.; Toohey, R.A. Socialization to work in late adolescence: The role of television and family. J. Broadcast Electron. 2008, 52, 282–302. [Google Scholar] [CrossRef]
- Sang, T.Q.; Zhou, H.L.; Li, M.H.; Li, W.T.; Shi, H.B.; Chen, H.B.; Zhou, H.G. Investigation of the differences between the medical personnel’s and general population’s view on the doctor-patient relationship in China by a cross-sectional survey. Glob. Health 2020, 16. [Google Scholar] [CrossRef]
- Cai, R.; Tang, J.; Deng, C.; Lv, G.; Xu, X.; Sylvia, S.; Pan, J. Violence against health care workers in China, 2013–2016: Evidence from the national judgment documents. Hum. Resour. Health 2019, 17. [Google Scholar] [CrossRef]
- Shi, Y.; Xue, H.; Ma, Y.; Wang, L.; Gao, T.; Shi, L.; Wang, Y.; Cui, M.; Wang, C.; Yang, X.; et al. Prevalence of occupational exposure and its influence on job satisfaction among Chinese healthcare workers: A large-sample, cross-sectional study. BMJ Open 2020, 10. [Google Scholar] [CrossRef]
- Du, Y.; Wang, W.; Washburn, D.J.; Lee, S.; Towne, S.D., Jr.; Zhang, H.; Maddock, J.E. Violence against healthcare workers and other serious responses to medical disputes in China: Surveys of patients at 12 public hospitals. BMC Health Serv. Res. 2020, 20. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.-P.; Li, C.-Y.; Hu, S.C. Job stress and burnout in hospital employees: Comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Jimenez, B.; Galvez-Herrer, M.; Rodriguez-Carvajal, R.; Vergel, A.I.S. A study of physicians’ intention to quit: The role of burnout, commitment and difficult doctor-patient interactions. Psicothema 2012, 24, 263–270. [Google Scholar]
- Gan, Y.; Gong, Y.H.; Chen, Y.W.; Cao, S.Y.; Li, L.Q.; Zhou, Y.F.; Herath, C.; Li, W.Z.; Song, X.Y.; Li, J.; et al. Turnover intention and related factors among general practitioners in Hubei, China: A cross-sectional study. BMC Fam. Pract. 2018, 19. [Google Scholar] [CrossRef]
- Choi, S.L.; Goh, C.F.; Adam, M.B.H.; Tan, O.K. Transformational leadership, empowerment, and job satisfaction: The mediating role of employee empowerment. Hum. Resour. Health 2016, 14. [Google Scholar] [CrossRef]
- Chen, Y.; Zahedi, F.M. Individuals’ internet security perceptions and behaviors: Polycontextual contrasts between the United States and China. Mis. Q. 2016, 40, 205–222. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; Organ, D.W. Self-reports in organizational research—Problems and prospects. J. Manag. 1986, 12, 531–544. [Google Scholar] [CrossRef]
- Zhang, M.; Yan, F.; Wang, W.; Li, G. Is the effect of person-organisation fit on turnover intention mediated by job satisfaction? A survey of community health workers in China. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.Z.; Wang, H.P.; Wang, D.; Yuan, B.B. Job satisfaction of the primary healthcare providers with expanded roles in the context of health service integration in rural China: A cross-sectional mixed methods study. Hum. Resour. Health 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhu, B.; Wu, J.; Mao, Y. Job satisfaction, work stress, and turnover intentions among rural health workers: A cross-sectional study in 11 western provinces of China. BMC Fam. Pract. 2019, 20. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | Items | Standardized Factor Loading | CR a | AVE b | Cronbach’s Alpha |
|---|---|---|---|---|---|
| Condition of the City Where the PMHCI Is Located CCPL | Development | 0.866 | 0.897 | 0.637 | 0.861 |
| Environment | 0.848 | ||||
| Culture and Customs | 0.762 | ||||
| Transportation | 0.758 | ||||
| Location | 0.748 | ||||
| Remuneration and Development RD | Working Bonus | 0.867 | 0.951 | 0.638 | 0.951 |
| Medical Insurance | 0.853 | ||||
| Working Subsidy | 0.846 | ||||
| Performance Assessment | 0.807 | ||||
| Professional Title Promotion | 0.803 | ||||
| Social Insurance and Accumulation | 0.792 | ||||
| Wage | 0.787 | ||||
| Holidays Arrangements | 0.779 | ||||
| Authorized Strength | 0.754 | ||||
| Position Promotion | 0.749 | ||||
| Individual Development | 0.737 | ||||
| Internal Organization Development IOD | Software and Hardware Facilities | 0.835 | 0.897 | 0.592 | 0.895 |
| Specialist Construction | 0.801 | ||||
| Learning Atmosphere | 0.788 | ||||
| Human resource allocation | 0.752 | ||||
| Teaching and scientific research | 0.727 | ||||
| Department Setting | 0.706 | ||||
| Job Responsibilities JR | Working Intensity | 0.921 | 0.909 | 0.715 | 0.907 |
| Working Stress | 0.889 | ||||
| Working Hours | 0.782 | ||||
| Workload | 0.780 | ||||
| Family Support FS | House | 0.858 | 0.883 | 0.654 | 0.882 |
| Parents | 0.814 | ||||
| Children | 0.784 | ||||
| Spouse | 0.775 | ||||
| Patient Factor PF | Respect in Physician | 0.832 | 0.866 | 0.617 | 0.862 |
| Patient–Doctor Relationship | 0.806 | ||||
| Trust in Physician | 0.760 | ||||
| Moral Character of Patients | 0.741 | ||||
| Sense of Gain SG | Fulfilling Personal Value | 0.849 | 0.859 | 0.670 | 0.858 |
| Professional Pride | 0.833 | ||||
| Job-Related Well-being | 0.772 |
| CCPL a | RD b | IOD c | JR d | FS e | SG f | PF g | |
|---|---|---|---|---|---|---|---|
| CCPL | 0.798 | ||||||
| RD | 0.689 | 0.799 | |||||
| IOD | 0.610 | 0.637 | 0.769 | ||||
| JR | 0.305 | 0.232 | 0.262 | 0.845 | |||
| FS | 0.498 | 0.459 | 0.329 | 0.275 | 0.808 | ||
| SG | 0.597 | 0.625 | 0.611 | 0.209 | 0.448 | 0.819 | |
| PF | 0.669 | 0.694 | 0.645 | 0.319 | 0.512 | 0.770 | 0.786 |
| df | /df | RMSEA a | CFI b | TLI c | IFI d | ||
|---|---|---|---|---|---|---|---|
| Without common method factor | 2535.443 | 608 | 4.170 | 0.060 | 0.921 | 0.913 | 0.921 |
| With common method factor | 2507.799 | 661 | 4.100 | 0.059 | 0.922 | 0.915 | 0.922 |
| Fit Indices | df | RMSEA a | CFI b | TLI c | IFI d | ||
|---|---|---|---|---|---|---|---|
| Value in the models | 1988.127 | 611 | 3.254 | 0.050 | 0.943 | 0.938 | 0.943 |
| Path | Effect Sizes | Boot SE | Z | p | Bias-Corrected 95%CI | Percentile 95%CI | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||||
| Int1 a | 0.252 | 0.046 | 5.478 | <0.001 | 0.169 | 0.351 | 0.167 | 0.347 |
| Int2 b | 0.042 | 0.021 | 2.000 | 0.046 | 0.004 | 0.087 | 0.001 | 0.084 |
| Int3 c | 0.064 | 0.028 | 2.286 | 0.011 | 0.011 | 0.123 | 0.009 | 0.120 |
| Int4 d | 0.206 | 0.037 | 5.568 | <0.001 | 0.142 | 0.289 | 0.140 | 0.286 |
| Int5 e | −0.016 | 0.011 | −1.455 | 0.147 | −0.038 | 0.004 | −0.038 | 0.004 |
| Int6 f | 0.044 | 0.020 | 2.200 | 0.028 | 0.008 | 0.089 | 0.006 | 0.086 |
| Total Indirect Effect | 0.593 | 0.069 | 8.594 | <0.001 | 0.462 | 0.732 | 0.457 | 0.730 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, H.; Cao, P.; Yu, J.; Zhang, J.; Jiang, H.; Zhao, Q.; Yu, X. A New Perspective for Improving the Human Resource Development of Primary Medical and Health Care Institutions: A Structural Equation Model Study. Int. J. Environ. Res. Public Health 2021, 18, 2560. https://doi.org/10.3390/ijerph18052560
Jia H, Cao P, Yu J, Zhang J, Jiang H, Zhao Q, Yu X. A New Perspective for Improving the Human Resource Development of Primary Medical and Health Care Institutions: A Structural Equation Model Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2560. https://doi.org/10.3390/ijerph18052560
Chicago/Turabian StyleJia, Huanhuan, Peng Cao, Jianxing Yu, Jingru Zhang, Hairui Jiang, Qize Zhao, and Xihe Yu. 2021. "A New Perspective for Improving the Human Resource Development of Primary Medical and Health Care Institutions: A Structural Equation Model Study" International Journal of Environmental Research and Public Health 18, no. 5: 2560. https://doi.org/10.3390/ijerph18052560
APA StyleJia, H., Cao, P., Yu, J., Zhang, J., Jiang, H., Zhao, Q., & Yu, X. (2021). A New Perspective for Improving the Human Resource Development of Primary Medical and Health Care Institutions: A Structural Equation Model Study. International Journal of Environmental Research and Public Health, 18(5), 2560. https://doi.org/10.3390/ijerph18052560