
The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer

 , ,
, ,  and
and
Abstract
1. Introduction
2. Methods
2.1. Ethical Considerations
2.2. Study Design and Population
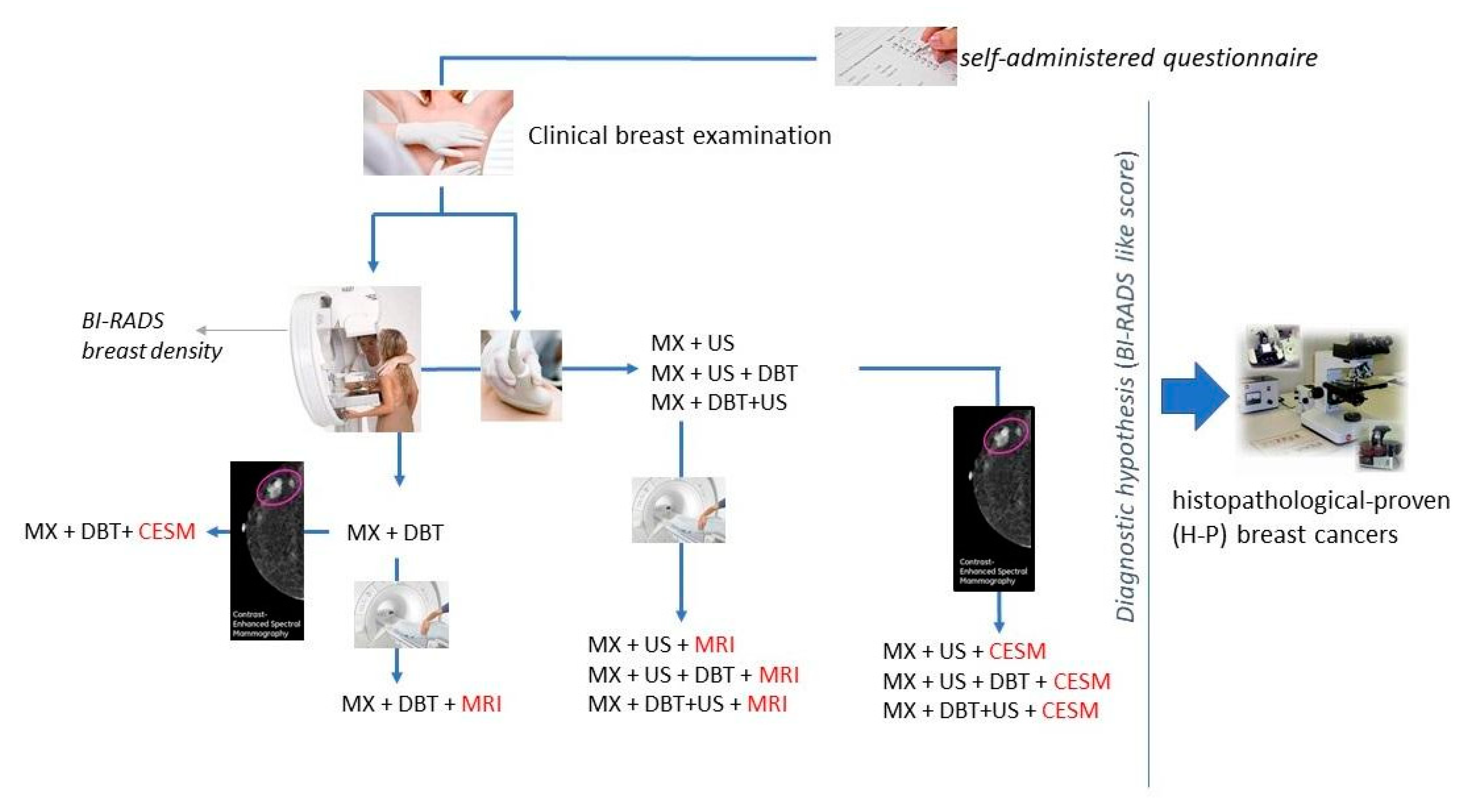
2.3. Diagnostic Protocol
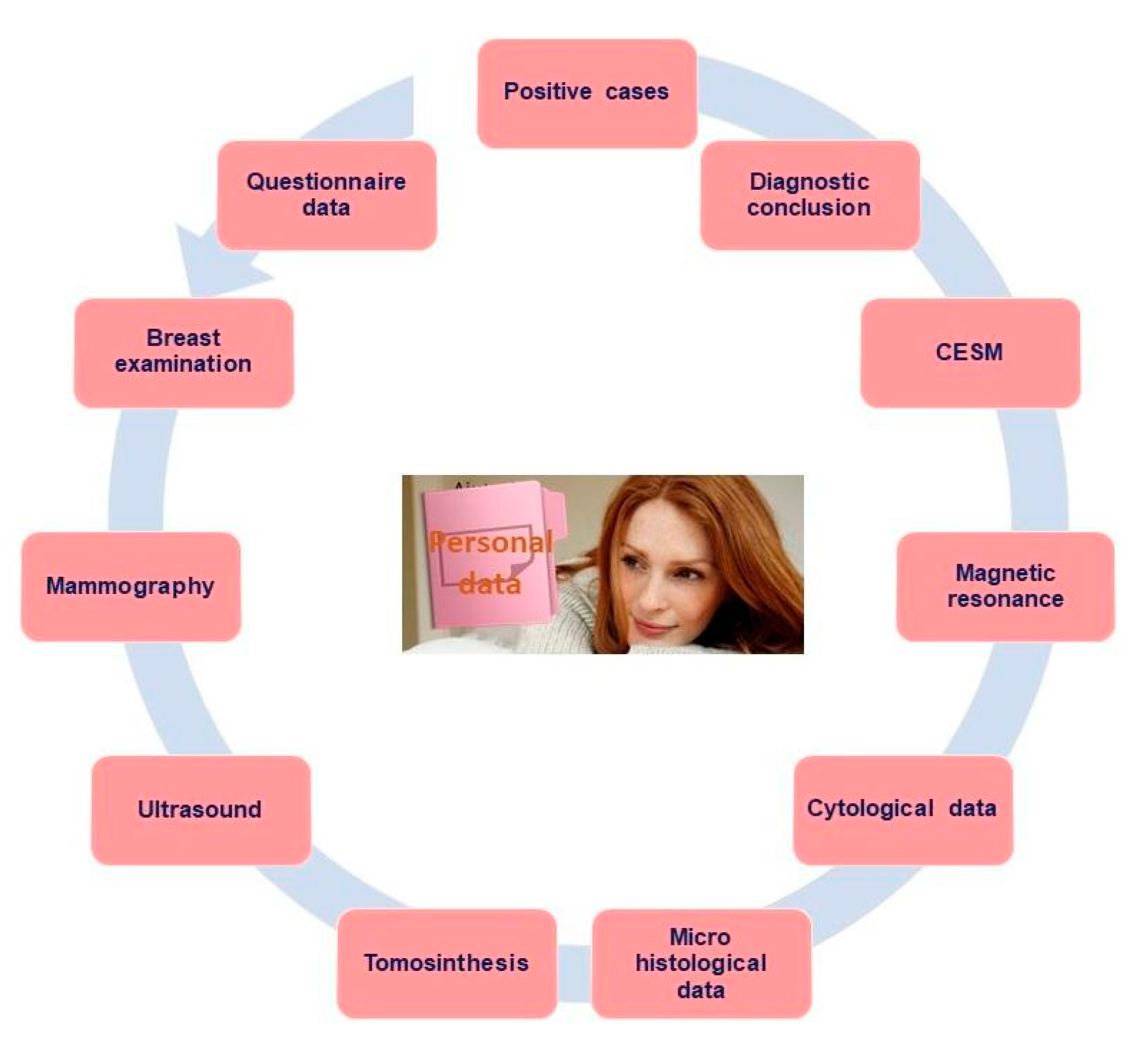
2.4. Data Collection, Measurements and Definitions
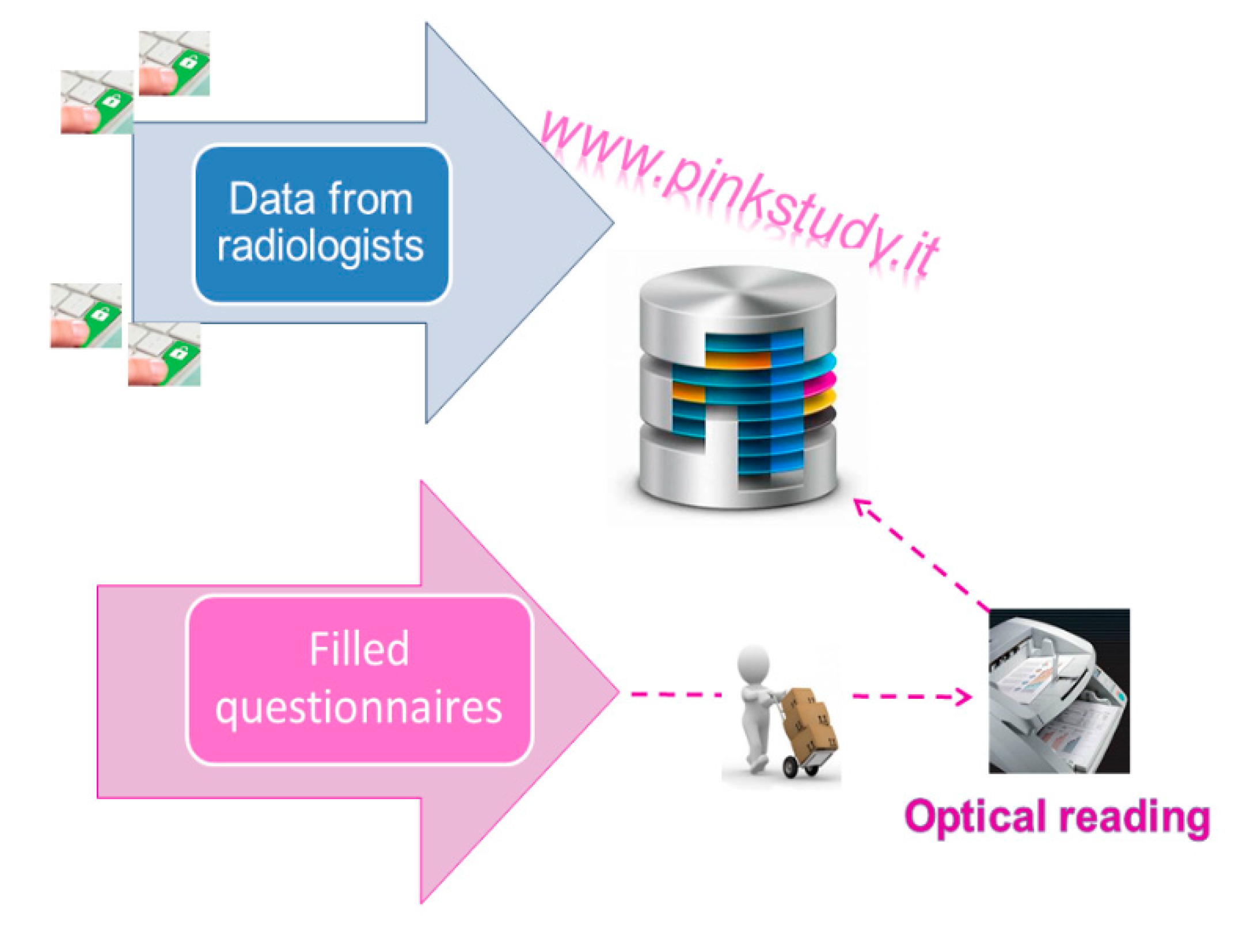
2.4.1. Structuring of the Centralised Database Containing Clinical Standardised Data
2.4.2. Self-Administered Questionnaire
2.4.3. Integration of Clinical Data with the Questionnaire Information
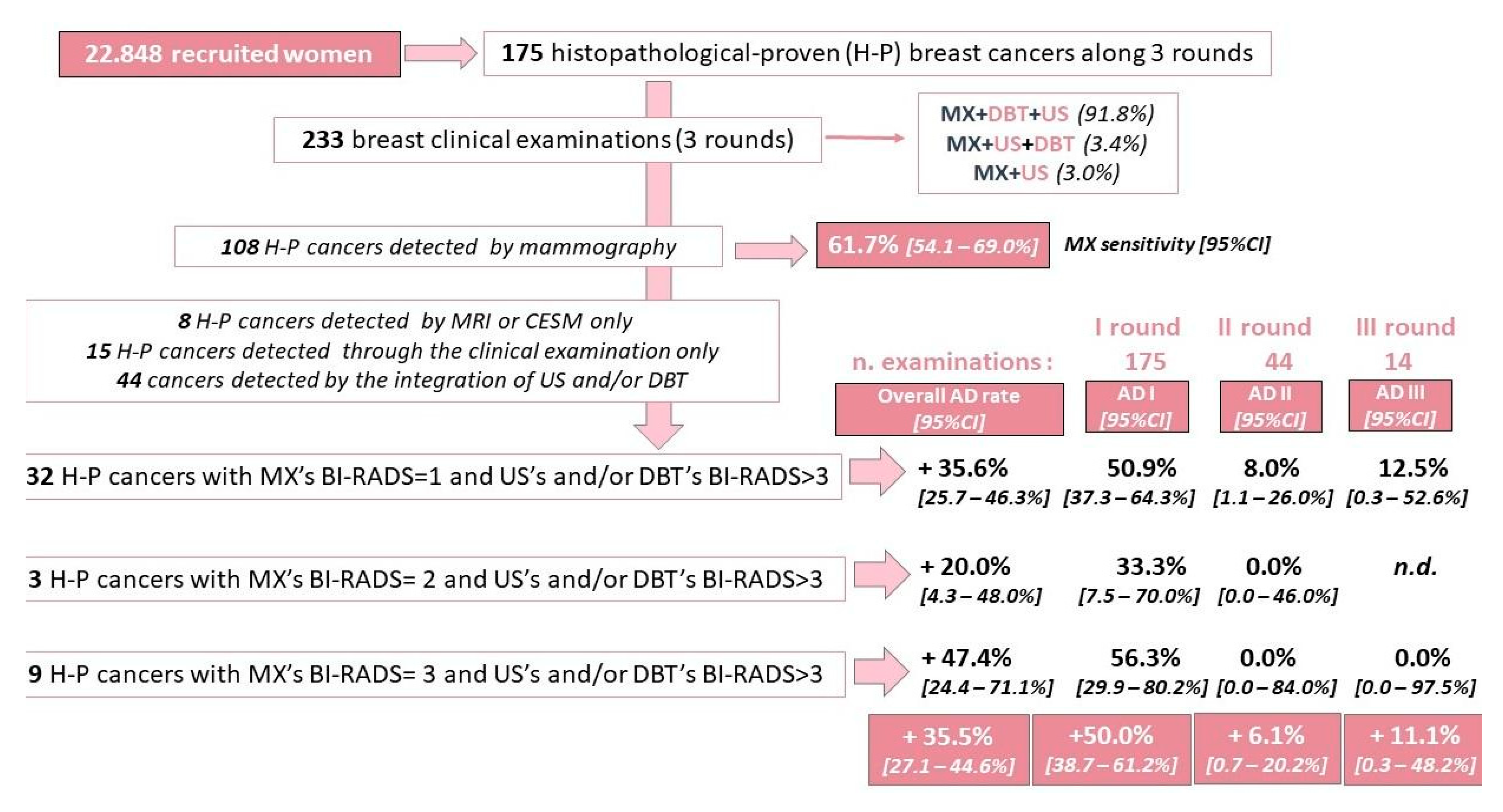
2.4.4. Assessment of Added Diagnostic Accuracy Yielded by Integrated Imaging Tests Compared to Mammographic Assessment Alone
2.5. Verification of Diagnostic Concordance among the Different Imaging Methods
3. Results
3.1. Population Characteristics
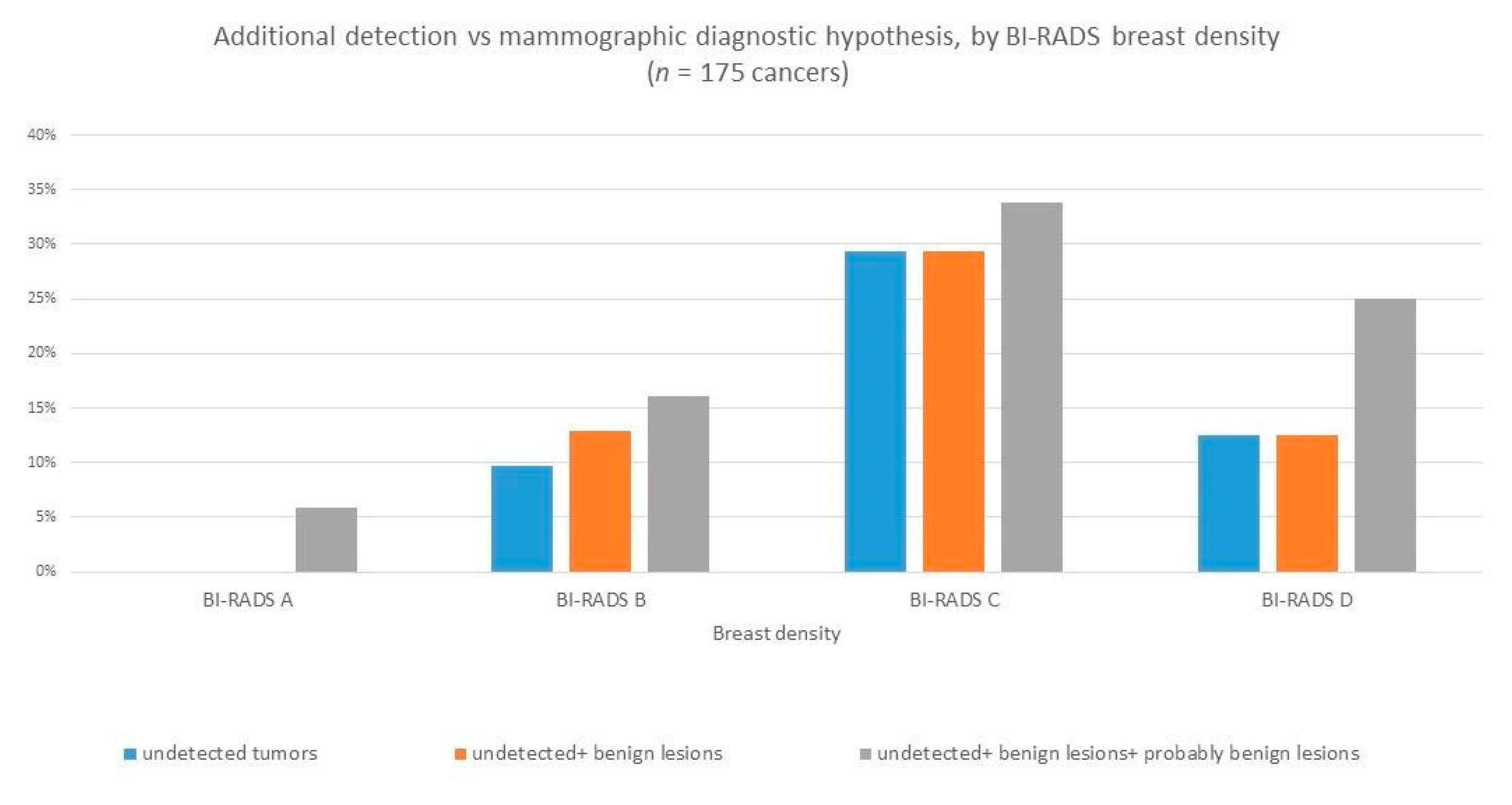
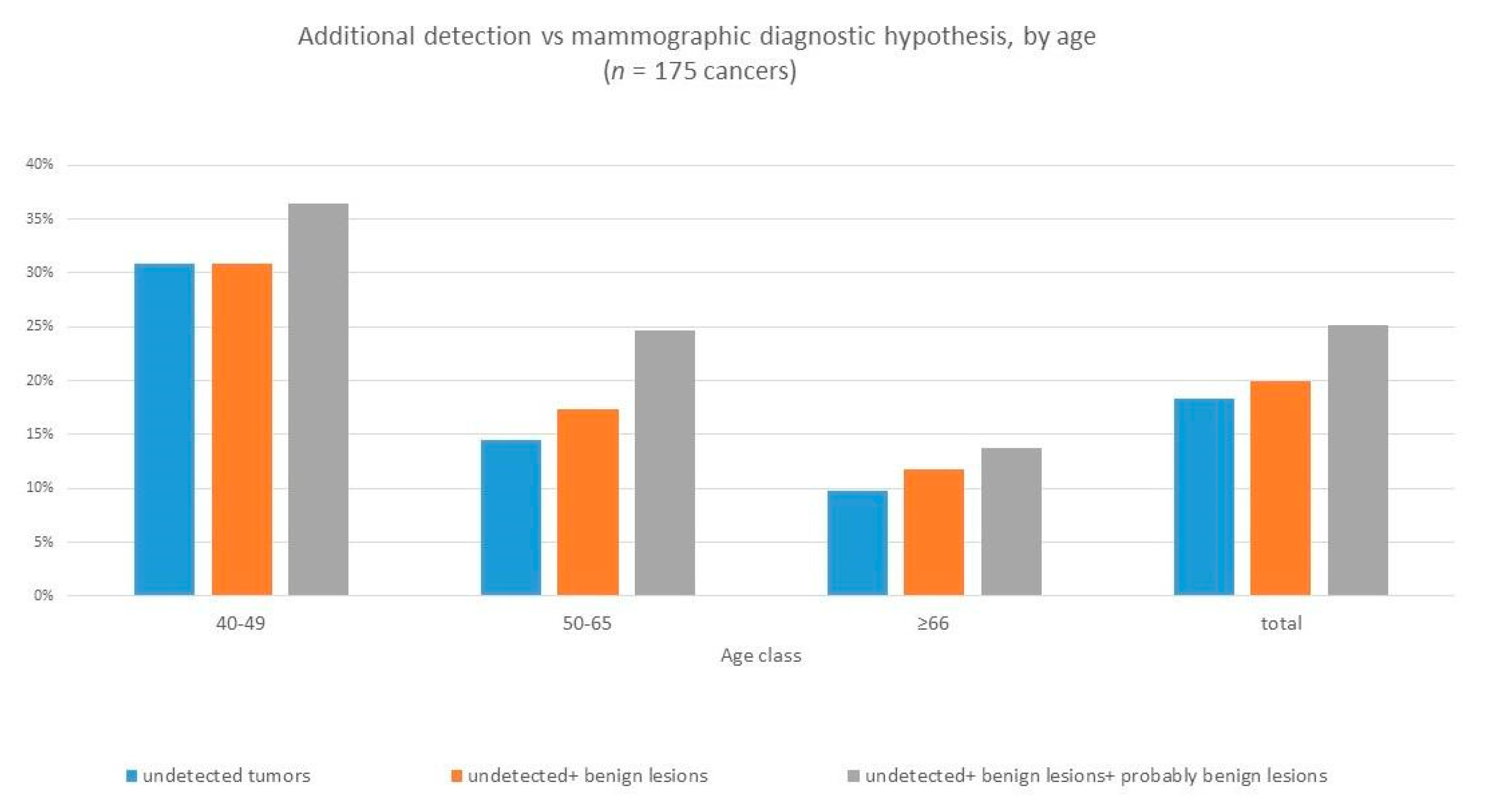
3.2. Gained Detection Rate
4. Discussion
4.1. Study Outcomes and Next Developments
4.2. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Onega, T.; Beaber, E.F.; Sprague, B.L.; Barlow, W.E.; Haas, J.S.; Tosteson, A.N.; DSchnall, M.; Armstrong, K.; Schapira, M.M.; Geller, B.; et al. Breast cancer screening in an era of personalized regimens: A conceptual model and National Cancer Institute initiative for risk-based and preference-based approaches at a population level. Cancer 2014, 120, 2955–2964. [Google Scholar] [CrossRef]
- Veronesi, U.; Luini, A.; Botteri, E.; Zurrida, S.; Monti, S.; Galimberti, V.; Cassano, E.; Latronico, A.; Pizzamiglio, M.; Viale, G.; et al. Nonpalpable breast carcinomas: Long-term evaluation of 1258 cases. Oncologist 2010, 15, 1248–1252. [Google Scholar] [CrossRef][Green Version]
- Berg, W.A.; Blume, J.D.; Cormack, J.B.; Mendelson, E.B.; Lehrer, D.; Böhm-Vélez, M.; Pisano, E.D.; Jong, R.A.; Evans, W.P.; Morton, M.J.; et al. Combined Screening With Ultrasound and Mammography vs Mammography Alone in Women at Elevated Risk of Breast Cancer. JAMA 2008, 299, 2151–2163. [Google Scholar] [CrossRef]
- Tabár, L.; Vitak, B.; Chen, T.H.; Yen, A.M.; Cohen, A.; Tot, T.; Chiu, S.Y.; Chen, S.L.; Fann, J.C.; Rosell, J.; et al. Swedish two-county trial: Impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 2011, 260, 658–663. [Google Scholar] [CrossRef]
- Duffy, S.W.; Tabar, L.; Olsen, A.H.; Vitak, B.; Allgood, P.C.; Chen, T.H.; Yen, A.M.; Smith, R.A. Cancer mortality in the 50–69 year age group before and after screening. J. Med. Screen. 2010, 17, 159–160. [Google Scholar] [CrossRef]
- Skaane, P.; Bandos, A.I.; Gullien, R.; Eben, E.B.; Ekseth, U.; Haakenaasen, U.; Izadi, M.; Jebsen, I.N.; Jahr, G.; Krager, M.; et al. Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology 2013, 267, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.L.; Tidwell, A.L.; Bujnoch, L.J.; Kushwaha, A.C.; Nordmann, A.S.; Sexton, R., Jr. Implementation of breast tomosynthesis in a routine screening practice: An observational study. AJR Am. J. Roentgenol. 2013, 200, 1401–1408. [Google Scholar] [CrossRef]
- Friedewald, S.M.; Rafferty, E.A.; Rose, S.L.; Durand, M.A.; Plecha, D.M.; Greenberg, J.S.; Hayes, M.K.; Copit, D.S.; Carlson, K.L.; Cink, T.M.; et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2014, 311, 2499–2507. [Google Scholar] [CrossRef] [PubMed]
- Tagliafico, A.S.; Mariscotti, G.; Valdora, F.; Durando, M.; Nori, J.; La Forgia, D.; Rosenberg, I.; Caumo, F.; Gandolfo, N.; Sormani, M.P.; et al. A prospective comparative trial of adjunct screening with tomosynthesis or ultrasound in women with mammography-negative dense breasts (ASTOUND-2). Eur. J. Cancer 2018, 104, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA A Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef]
- Ibrahim, M.A.; Hazhirkarzar, B.; Dublin, A.B. Gadolinium Magnetic Resonance Imaging; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482487/ (accessed on 20 December 2020).
- Kuhl, C.K.; Schrading, S.; Leutner, C.C.; Morakkabati-Spitz, N.; Wardelmann, E.; Fimmers, R.; Kuhn, W.; Schild, H.H. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J. Clin. Oncol. 2005, 23, 8469–8476. [Google Scholar] [CrossRef] [PubMed]
- Kriege, M.; Brekelmans, C.T.; Boetes, C.; Besnard, P.E.; Zonderland, H.M.; Obdeijn, I.M.; Manoliu, R.A.; Kok, T.; Peterse, H.; Tilanus-Linthorst, M.M.; et al. Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N. Engl. J. Med. 2004, 351, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Leach, M.O.; Boggis, C.R.; Dixon, A.K.; Easton, D.F.; Eeles, R.A.; Evans, D.G.; Gilbert, F.J.; Griebsch, I.; Hoff, R.J.; Kessar, P.; et al. Screening with magnetic resonance imaging and mammography of a UK population at high familial risk of breast cancer: A prospective multicentre cohort study (MARIBS). Lancet 2005, 365, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Podo, F. Breast MR imaging in women at high-risk of breast cancer. Is something changing in early breast cancer detection? Eur. Radiol. 2007, 17, 873–887. [Google Scholar] [CrossRef]
- Warner, E.; Plewes, D.B.; Hill, K.A.; Causer, P.A.; Zubovits, J.T.; Jong, R.A.; Cutrara, M.R.; DeBoer, G.; Yaffe, M.J.; Messner, S.J.; et al. Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004, 292, 1317–1325. [Google Scholar] [CrossRef]
- Chetlen, A.; Mack, J.; Chan, T. Breast cancer screening controversies: Who, when, why, and how? Clin. Imaging 2016, 40, 279–282. [Google Scholar] [CrossRef]
- Duffy, S.W.; Tabár, L.; Yen, A.M.; Dean, P.B.; Smith, R.A.; Jonsson, H.; Törnberg, S.; Chen, S.L.; Chiu, S.Y.; Fann, J.C.; et al. Mammography screening reduces rates of advanced and fatal breast cancers: Results in 549,091 women. Cancer 2020, 126, 2971–2979. [Google Scholar] [CrossRef]
- Copenhagen: WHO Regional Office for Europe. Screening Programmes: A Short Guide. Increase Effectiveness, Maximize Benefits and Minimize Harm. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/330829/9789289054782-eng.pdf (accessed on 20 December 2020).
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Benbrahim-Tallaa, L.; Bouvard, V.; Bianchini, F.; Straif, K. Breast-Cancer Screening--Viewpoint of the IARC Working Group. N. Engl. J. Med. 2015, 373, 1478–1479. [Google Scholar] [CrossRef]
- Morrell, S.; Barratt, A.; Irwig, L.; Howard, K.; Biesheuvel, C.; Armstrong, B. Estimates of overdiagnosis of invasive breast cancer associated with screening mammography. Cancer Causes Control 2010, 21, 275–282. [Google Scholar] [CrossRef]
- Mannu, G.S.; Wang, Z.; Broggio, J.; Charman, J.; Cheung, S.; Kearins, O.; Dodwell, D.; Darby, S.C. Invasive breast cancer and breast cancer mortality after ductal carcinoma in situ in women attending for breast screening in England, 1988–2014: Population based observational cohort study. BMJ 2020, 369, m1570. [Google Scholar] [CrossRef]
- European Commission Initiative on Breast Cancer. European Guidelines on Breast Cancer Screening and Diagnosis. 2020. Available online: https://healthcare-quality.jrc.ec.europa.eu/european-breast-cancer-guidelines/screening-ages-and-frequencies (accessed on 2 December 2020).
- Miglioretti, D.L.; Zhu, W.; Kerlikowske, K.; Sprague, B.L.; Onega, T.; Buist, D.S.; Henderson, L.M.; Smith, R.A.; Breast Cancer Surveillance Consortium. Breast Tumor Prognostic Characteristics and Biennial vs Annual Mammography, Age, and Menopausal Status. JAMA Oncol. 2015, 1, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.L.; Li, S.; Dite, G.S.; Aung, Y.K.; Evans, C.F.; Trinh, H.N.; Baglietto, L.; Stone, J.; Song, Y.M.; Sung, J.; et al. Interval breast cancer risk associations with breast density, family history and breast tissue aging. Int. J. Cancer 2020, 147, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Niraula, S.; Biswanger, N.; Hu, P.; Lambert, P.; Decker, K. Incidence, Characteristics, and Outcomes of Interval Breast Cancers Compared With Screening-Detected Breast Cancers. JAMA Netw. Open 2020, 3, e2018179. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer 2019, 11, 151–164. [Google Scholar] [CrossRef]
- Di Maggio, C.; Del Favero, C.; Frigerio, A.; Giuseppetti, G.M.; Gozzi, G.; Lattanzio, E.; Pesce, B.; Rosselli Del Turco, M.; Simonetti, G.; Nosenzo, M.A. Charta senologica 2004 (approccio diagnostico alla patologia mammaria). La Radiologia Medica 2004, 108, 569–587. Available online: http://hdl.handle.net/10068/308992 (accessed on 18 December 2020).
- Fass, L. Imaging and cancer: A review. Mol. Oncol. 2008, 2, 115–152. [Google Scholar] [CrossRef]
- Lima, Z.S.; Ebadi, M.R.; Amjad, G.; Younesi, L. Application of Imaging Technologies in Breast Cancer Detection: A Review Article. Open Access Maced. J. Med. Sci. 2019, 7, 838–848. [Google Scholar] [CrossRef]
- Wang, L. Early Diagnosis of Breast Cancer. Sensors 2017, 17, 1572. [Google Scholar] [CrossRef]
- American Cancer Society. American Cancer Society Recommendations for the Early Detection of Breast Cancer. In ACS Breast Cancer Early Detection Recommendations; American Cancer Society: Atlanta, GA, USA, 2020. [Google Scholar]
- American Cancer Society. Breast Cancer Facts & Figures 2019–2020; American Cancer Society, Inc.: Atlanta, GA, USA, 2019. [Google Scholar]
- Tabár, L.; Dean, P.B.; Chen, T.H.-H.; Yen, A.M.-F.; Chen, S.L.-S.; Fann, J.C.-Y.; Chiu, S.Y.-H.; Ku, M.M.-S.; Wu, W.Y.-Y.; Hsu, C.-Y.; et al. The incidence of fatal breast cancer measures the increased effectiveness of therapy in women participating in mammography screening. Cancer 2018, 125, 515–523. [Google Scholar] [CrossRef]
- Bomb, M.; Hiom, S.; Kumar, H.; Moffat, J.; Ormiston-Smith, N.; Woolf, L. Saving Lives, Averting Costs: An Analysis of the Financial Implications of Achieving Earlier Diagnosis of Colorectal, Lung and Ovarian Cancer; Cancer Research: London, UK, 2014; Available online: https://www.cancerresearchuk.org/sites/default/files/saving_lives_averting_costs.pdf (accessed on 2 December 2020).
- Lo-Fo-Wong, D.N.N.; Sitnikova, K.; Sprangers, M.A.G.; De Haes, H.C.J.M. Predictors of health care use of women with breast cancer: A systematic review. Breast J. 2015, 21, 508–513. [Google Scholar] [CrossRef]
- Sun, L.; Legood, R.; Dos-Santos-Silva, I.; Gaiha, S.M.; Sadique, Z. Global treatment costs of breast cancer by stage: A systematic review. PLoS ONE 2018, 13, e0207993. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Geographic Area | Centre Typology | Recruited Women |
|---|---|---|
| NORTH | Public medical centre/hospital | 4593 |
| Private medical centre/hospital | 6738 | |
| IRCCS | 2607 | |
| Subtotal for North Italy | 13,938 | |
| CENTRUM | Public medical centre/hospital | 2387 |
| Private medical centre/hospital | 6305 | |
| Subtotal for Centrum Italy | 8692 | |
| SOUTH | Private medical centre/hospital | 218 |
| Subtotal for South Italy | 218 | |
| Total | 22,848 | |
| Age Class | Density | Women | Percentages by Age Class | Age Class | Density | Women | Percentages by Age Class |
|---|---|---|---|---|---|---|---|
| 40–44 | A | 192 | 6.6% | 65–69 | A | 498 | 25.0% |
| B | 678 | 23.3% | B | 862 | 43.3% | ||
| C | 1248 | 42.9% | C | 536 | 26.9% | ||
| D | 793 | 27.2% | D | 94 | 4.7% | ||
| 45–49 | A | 296 | 6.4% | 70–74 | A | 416 | 28.4% |
| B | 1179 | 25.6% | B | 641 | 43.7% | ||
| C | 2040 | 44.2% | C | 356 | 24.3% | ||
| D | 1096 | 23.8% | D | 54 | 3.7% | ||
| 50–54 | A | 440 | 9.6% | 75–79 | A | 230 | 29.9% |
| B | 1572 | 34.2% | B | 320 | 41.6% | ||
| C | 1841 | 40.0% | C | 189 | 24.6% | ||
| D | 749 | 16.3% | D | 30 | 3.9% | ||
| 55–59 | A | 529 | 14.7% | 80–84 | A | 67 | 27.9% |
| B | 1396 | 38.7% | B | 120 | 50.0% | ||
| C | 1357 | 37.6% | C | 48 | 20.0% | ||
| D | 325 | 9.0% | D | 5 | 2.1% | ||
| 60–64 | A | 485 | 18.5% | >85 | A | 11 | 33.3% |
| B | 1133 | 43.3% | B | 10 | 30.3% | ||
| C | 836 | 31.9% | C | 12 | 36.4% | ||
| D | 164 | 6.3% | D | 0 | 0.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchini, M.; Pieroni, S.; Montrucchio, E.; Nori Cucchiari, J.; Di Maggio, C.; Cassano, E.; Di Nubila, B.; Giuseppetti, G.M.; Nicolucci, A.; Scaperrotta, G.; et al. The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 2456. https://doi.org/10.3390/ijerph18052456
Franchini M, Pieroni S, Montrucchio E, Nori Cucchiari J, Di Maggio C, Cassano E, Di Nubila B, Giuseppetti GM, Nicolucci A, Scaperrotta G, et al. The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer. International Journal of Environmental Research and Public Health. 2021; 18(5):2456. https://doi.org/10.3390/ijerph18052456
Chicago/Turabian StyleFranchini, Michela, Stefania Pieroni, Edgardo Montrucchio, Jacopo Nori Cucchiari, Cosimo Di Maggio, Enrico Cassano, Brunella Di Nubila, Gian Marco Giuseppetti, Alberto Nicolucci, Gianfranco Scaperrotta, and et al. 2021. "The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer" International Journal of Environmental Research and Public Health 18, no. 5: 2456. https://doi.org/10.3390/ijerph18052456
APA StyleFranchini, M., Pieroni, S., Montrucchio, E., Nori Cucchiari, J., Di Maggio, C., Cassano, E., Di Nubila, B., Giuseppetti, G. M., Nicolucci, A., Scaperrotta, G., Belli, P., Santicchia, S., Molinaro, S., & on behalf of the PINK Consortium. (2021). The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer. International Journal of Environmental Research and Public Health, 18(5), 2456. https://doi.org/10.3390/ijerph18052456