
International Total Worker Health: Applicability to Agribusiness in Latin America

 , , ,
, , , 
 , and
, and 
Abstract
1. Introduction
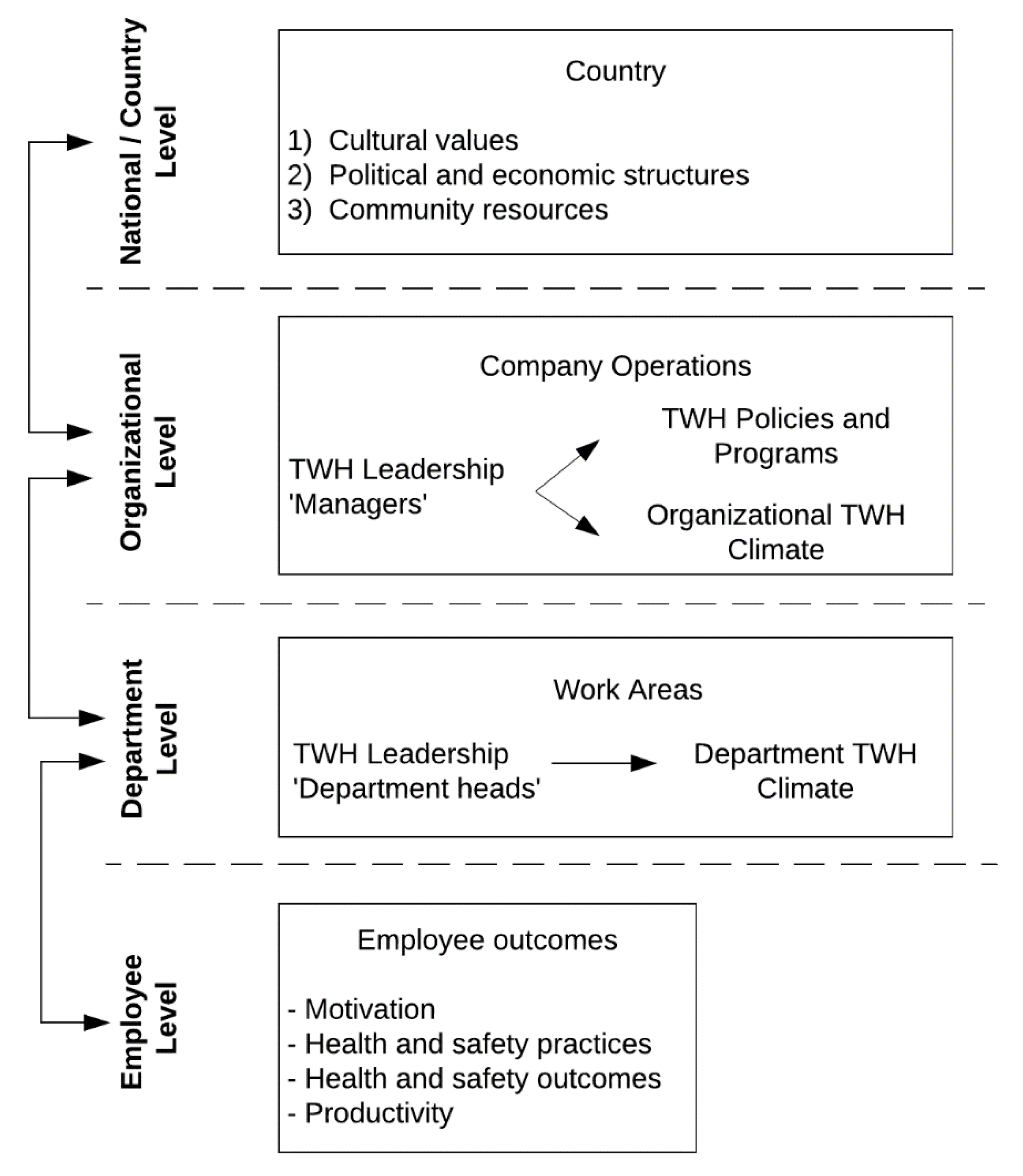
Conceptual Model
2. Case Study: A Model to Apply the TWH Approach to Latin America
2.1. Collaboration Background
2.2. Assessment of Total Worker Health
2.2.1. Key Informant Interviews and Focus Groups
2.2.2. Organizational Assessment
2.2.3. Leadership Self-Assessment
2.2.4. Employee Health and Safety Culture Assessment
2.2.5. Employee Health Risk Assessment and Evaluation of Clinical Consult Data
2.3. Total Worker Health Leadership Training
2.3.1. Total Worker Health Leadership Training Components
2.3.2. Corporate Recommendations
3. Discussion (Lessons Learned)
4. Limitations (Challenges)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- NIOSH Total Worker Health; NIOSH; CDC. Available online: https://www.cdc.gov/NIOSH/twh/ (accessed on 11 November 2020).
- Feltner, C.; Peterson, K.; Weber, R.P.; Cluff, L.; Coker-Schwimmer, E.; Viswanathan, M.; Lohr, K.N. The Effectiveness of Total Worker Health Interventions: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2016, 165, 262–269. [Google Scholar] [CrossRef]
- Anger, K.W.; Elliot, D.L.; Bodner, T.; Olson, R.; Rohlman, D.S.; Truxillo, D.M.; Kuehl, K.S.; Hammer, L.B.; Montgomery, D. Effectiveness of Total Worker Health Interventions. J. Occup. Health Psychol. 2015, 20, 226–247. [Google Scholar] [CrossRef]
- Pronk, N.P. Integrated Worker Health Protection and Promotion Programs: Overview and Perspectives on Health and Economic Outcomes. J. Occup. Environ. Med. Coll. Occup. Environ. Med. 2013, 55, S30–S37. [Google Scholar] [CrossRef] [PubMed]
- Gastañaga, M.d.C. Salud Ocupacional: Historia y Retos Del Futuro. Rev. Peru. Med. Exp. Salud Publica 2012, 29, 177–178. [Google Scholar] [CrossRef] [PubMed]
- Velandia, M.; Hernando, J.; Pinilla, A. From Occupational Health to Safety and Health Management in the Workplace: More than Just Semantic, the Transformation of the General Occupational Hazards System. Innovar 2013, 23, 21–32. [Google Scholar]
- Hernández Palma, H.; Monterrosa Assia, F.; Muñoz Rojas, D. Cultura De Prevencion Para La Seguridad Y Salud En El Trabajo En El Ambito Colombiano. Advocatus 2017, 28, 35–45. [Google Scholar] [CrossRef][Green Version]
- Martinez Barranco, M.P.; Yandun Burbano, E.D. Seguridad y Salud Ocupacional En Ecuador: Contribución Normativa a La Responsabilidad Social Organizacional. INNOVA Res. J. 2017, 2, 58–68. [Google Scholar] [CrossRef]
- García, G.; Calderón, E.; Palacios, B.; Serpa, V.; Peñaherrera, S.; Bermúdez, S. Revisión Documental de Las Encuestas Sobre Condiciones de Seguridad y Salud Ocupacional Realizadas En Países de Centro y Latinoamérica. Hig. Sanid. Ambient. 2016, 16, 1451–1456. [Google Scholar]
- Sorensen, G.; Nagler, E.M.; Pawar, P.; Gupta, P.C.; Pednekar, M.S.; Wagner, G.R. Lost in Translation: The Challenge of Adapting Integrated Approaches for Worker Health and Safety for Low-and Middle-Income Countries. PLoS ONE 2017, 12, e0182607. [Google Scholar] [CrossRef]
- Sorensen, G.; Barbeau, E.; Stoddard, A.M.; Hunt, M.K.; Kaphingst, K.; Wallace, L. Promoting Behavior Change among Working-Class, Multiethnic Workers: Results of the Healthy Directions—Small Business Study. Am. J. Public Health 2005, 95, 1389–1395. [Google Scholar] [CrossRef]
- Hunt, M.K.; Barbeau, E.M.; Lederman, R.; Stoddard, A.M.; Chetkovich, C.; Goldman, R.; Wallace, L.; Sorensen, G. Process Evaluation Results from the Healthy Directions-Small Business Study. Health Educ. Behav. 2007, 34, 90–107. [Google Scholar] [CrossRef]
- Barbeau, E.; Roelofs, C.; Youngstrom, R.; Sorensen, G.; Stoddard, A.; LaMontagne, A.D. Assessment of Occupational Safety and Health Programs in Small Businesses. Am. J. Ind. Med. 2004, 45, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Hammer, L.B.; Truxillo, D.M.; Bodner, T.; Rineer, J.; Pytlovany, A.C.; Richman, A. Effects of a Workplace Intervention Targeting Psychosocial Risk Factors on Safety and Health Outcomes. Biomed. Res. Int. 2015, 2015, 836967. [Google Scholar] [CrossRef]
- Sorensen, G.; Barbeau, E.M.; Stoddard, A.M.; Hunt, M.K.; Goldman, R.; Smith, A.; Brennan, A.A.; Wallace, L. Tools for Health: The Efficacy of a Tailored Intervention Targeted for Construction Laborers. Cancer Causes Control 2007, 18, 51–59. [Google Scholar] [CrossRef]
- Caspi, C.E.; Dennerlein, J.T.; Kenwood, C.; Stoddard, A.M.; Hopcia, K.; Hashimoto, D.; Sorensen, G. Results of a Pilot Intervention to Improve Health and Safety for Health Care Workers. J. Occup. Environ. Med. 2013, 55, 1449–1455. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.; Wright, R.R.; Elliot, D.L.; Hess, J.A.; Thompson, S.; Buckmaster, A.; Luther, K.; Wipfli, B. The COMPASS Pilot Study: A Total Worker HealthTM Intervention for Home Care Workers. J. Occup. Environ. Med. 2015, 57, 406–416. [Google Scholar] [CrossRef]
- Von Thiele Schwarz, U.; Augustsson, H.; Hasson, H.; Stenfors-Hayes, T. Promoting Employee Health by Integrating Health Protection, Health Promotion, and Continuous Improvement: A Longitudinal Quasi-Experimental Intervention Study. J. Occup. Environ. Med. 2015, 57, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Olson, R.; Anger, W.K.; Elliot, D.L.; Wipfli, B.; Gray, M. A New Health Promotion Model for Lone Workers: Results of the Safety & Health Involvement for Truckers (SHIFT) Pilot Study. J. Occup. Environ. Med. 2009, 51, 1233–1246. [Google Scholar] [CrossRef]
- Wipfli, B.; Olson, R.; Koren, M. Weight-Loss Maintenance among SHIFT Pilot Study Participants 30-Months after Intervention. J. Occup. Environ. Med. 2013, 55, 1–3. [Google Scholar] [CrossRef]
- Schenker, M.B. Preventive Medicine and Health Promotion Are Overdue in the Agricultural Workplace. J. Public Health Policy 1996, 17, 275–305. [Google Scholar] [CrossRef] [PubMed]
- Donham, K.J.; Meppelink, S.M.; Kelly, K.M.; Rohlman, D.S. Health Indicators of a Cohort of Midwest Farmers: Health Outcomes of Participants in the Certified Safe Farm Program. J. Agromedicine 2019, 24, 228–238. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Labor Force, Total|Data. Available online: https://data.worldbank.org/indicator/SL.TLF.TOTL.IN?end=2020&name_desc=false&start=2020&type=shaded&view=map (accessed on 11 November 2020).
- Wadsworth, E.; Walters, D. Safety and Health at the Heart of the Future of Work: Building on 100 Years of Experience; International Labour Office: Geneva, Switzerland, 2019; ISBN 978-92-2-133152-0. [Google Scholar]
- Veiga de Cabo, J.; Maqueda Blasco, J.; Andrus, J.; Gross, S.; Cassanha Galvao, L.A.; Florencio Corvalan, C.; Fortune, A.-K.; Pages, A.; Marti, M.C.; Escoto, L.R.; et al. Cooperation Framework between the Pan American Health Organization (PAHO), Regional Office for the Americas of the Word Health Organization (WHO) and the National School of Occupational Medicine of the Carlos III Institute on Health and Work Safety. Med. Segur. Trab. (Madr.) 2010, 56, 266–270. [Google Scholar]
- Sorensen, G.; McLellan, D.L.; Sabbath, E.L.; Dennerlein, J.T.; Nagler, E.M.; Hurtado, D.A.; Pronk, N.P.; Wagner, G.R. Integrating Worksite Health Protection and Health Promotion: A Conceptual Model for Intervention and Research. Prev. Med. (Baltim.) 2016, 91, 188–196. [Google Scholar] [CrossRef]
- Schwatka, N.V.; Tenney, L.; Dally, M.J.; Scott, J.; Brown, C.E.; Weitzenkamp, D.; Shore, E.; Newman, L.S. Small Business Total Worker Health: A Conceptual and Methodological Approach to Facilitating Organizational Change. Occup. Health Sci. 2018, 2, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Burke, M.J.; Signal, S.M. Workplace Safety: A Multilevel, Interdisciplinary Perspective. Res. Pers. Hum. Resour. Manag. 2010, 29, 1–47. [Google Scholar] [CrossRef]
- Thibault, T.; Gulseren, D.B.; Kelloway, E.K. The benefits of transformational leadership and transformational leadership training on health and safety outcomes. In Increasing Occupational Health and Safety in Workplaces; Edward Elgar Publishing: Cheltenham, UK, 2019; ISBN 9781788118088. [Google Scholar]
- Burke, W.W.; Litwin, G.H. A Causal Model of Organizational Performance and Change. J. Manag. 1992, 18. [Google Scholar] [CrossRef]
- Pantaleon. Reporte Desarrollo Responsable 2019. 2019. Available online: https://www.pantaleon.com/reportes-desarrollo-responsable/ (accessed on 11 November 2020).
- Dally, M.; Butler-Dawson, J.; Sorensen, C.J.; Van Dyke, M.; James, K.A.; Krisher, L.; Jaramillo, D.; Newman, L.S. Wet Bulb Globe Temperature and Recorded Occupational Injury Rates among Sugarcane Harvesters in Southwest Guatemala. Int. J. Environ. Res. Public Health 2020, 17, 8195. [Google Scholar] [CrossRef] [PubMed]
- Butler-Dawson, J.; Krisher, L.; Asensio, C.; Cruz, A.; Tenney, L.; Weitzenkamp, D.; Dally, M.; Asturias, E.J.; Newman, L.S. Risk Factors for Declines in Kidney Function in Sugarcane Workers in Guatemala. J. Occup. Environ. Med. 2018, 60, 548–558. [Google Scholar] [CrossRef] [PubMed]
- Krisher, L.; Butler-Dawson, J.; Yoder, H.; Pilloni, D.; Dally, M.; Johnson, E.C.; Jaramillo, D.; Cruz, A.; Asensio, C.; Newman, L.S. Electrolyte Beverage Intake to Promote Hydration and Maintain Kidney Function in Guatemalan Sugarcane Workers Laboring in Hot Conditions. J. Occup. Environ. Med. 2020, 62, e696–e703. [Google Scholar] [CrossRef]
- Butler-Dawson, J.; Krisher, L.; Yoder, H.; Dally, M.; Sorensen, C.; Johnson, R.J.; Asensio, C.; Cruz, A.; Johnson, E.C.; Carlton, E.J.; et al. Evaluation of Heat Stress and Cumulative Incidence of Acute Kidney Injury in Sugarcane Workers in Guatemala. Int. Arch. Occup. Environ. Health 2019, 92, 977–990. [Google Scholar] [CrossRef]
- Sorensen, C.J.; Butler-Dawson, J.; Dally, M.; Krisher, L.; Griffin, B.R.; Johnson, R.J.; Lemery, J.; Asensio, C.; Tenney, L.; Newman, L.S. Risk Factors and Mechanisms Underlying Cross-Shift Decline in Kidney Function in Guatemalan Sugarcane Workers. J. Occup. Environ. Med. 2019, 61, 239–250. [Google Scholar] [CrossRef]
- Stumpf, A.M.; Erlandson, G.; Ruths, J.; Meinke, D.K.; Newman, L.S.; Krisher, L.; Pilloni, D.; Cruz, A.; Asensio, C. Noise Exposures of Sugar Cane Mill Workers in Guatemala. Int. J. Audiol. 2020, 59, S48–S53. [Google Scholar] [CrossRef]
- Tenney, L.; Fan, W.; Dally, M.; Scott, J.; Haan, M.; Rivera, K.; Newman, M.; Newman, L.S. Health LinksTM Assessment of Total Worker Health® Practices as Indicators of Organizational Behavior in Small Business. J. Occup. Environ. Med. 2019, 61, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention Worksite Health ScoreCard; Workplace Health Promotion; CDC. Available online: https://www.cdc.gov/workplacehealthpromotion/initiatives/healthscorecard/index.html (accessed on 8 December 2020).
- Neira, M. Healthy Workplaces: A Model for Action; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Denison, D.R. What Is the Difference between Organizational Culture and Organizational Climate? A Native’s Point of View on a Decade of Paradigm Wars. Acad. Manag. Rev. 1996, 21, 619–654. [Google Scholar] [CrossRef]
- Yanar, B.; Amick, B.C.; Lambraki, I.; D’Elia, T.; Severin, C.; Van Eerd, D. How Are Leaders Using Benchmarking Information in Occupational Health and Safety Decision-Making? Saf. Sci. 2019, 116, 245–253. [Google Scholar] [CrossRef]
- Flynn, M.A.; Castellanos, E.; Flores-Andrade, A. Safety Across Cultures: Understanding the Challenges. Prof. Saf. 2018, 63, 28–32. [Google Scholar]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Assessment Components | ||||
|---|---|---|---|---|
| Assessment Constructs | Organizational Assessment | TWH Leadership Self-Assessment | Employee Health and Safety Culture | Employee Health Risk Assessment |
| Organizational Supports | Leadership Supports | Leadership Supports | Employee well-being | |
| Health Policies and Programs | Employee Workplace Assessment | Organizational supports | Overall health | |
| Safety Policies and Programs | Support for Health Programs and Policies | Health and Safety motivations | Work stress | |
| Engagement | Support for Safety Programs and Policies | Organizational commitment to health and safety | Tobacco use | |
| Evaluation | Leadership Engagement | Health and safety climate | Physical activity | |
| Health and Safety Program Evaluation | Health and safety behaviors | Absenteeism | ||
| Leadership Practices | Psychological safety | Presenteeism | ||
| Department Demographics | Leadership commitment to health and safety | Fatigue | ||
| Access to benefits | ||||
| Perceived work hazards | ||||
| Total Worker Health Leadership in-Person Training Objectives and Description—4-h One-Day Training |
|---|
|
|
|
|
| Outline of TWH Recommendations |
|---|
| (1) Maintain established workplace safety programs and policies |
| (2) Integrate health and safety programs through the inclusion of wellness and wellbeing programs |
(3) Address the prevention of chronic diseases
|
(4) Address stress and mental health
|
(5) Address sleep deprivation and fatigue
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaramillo, D.; Krisher, L.; Schwatka, N.V.; Tenney, L.; Fisher, G.G.; Clancy, R.L.; Shore, E.; Asensio, C.; Tetreau, S.; Castrillo, M.E.; et al. International Total Worker Health: Applicability to Agribusiness in Latin America. Int. J. Environ. Res. Public Health 2021, 18, 2252. https://doi.org/10.3390/ijerph18052252
Jaramillo D, Krisher L, Schwatka NV, Tenney L, Fisher GG, Clancy RL, Shore E, Asensio C, Tetreau S, Castrillo ME, et al. International Total Worker Health: Applicability to Agribusiness in Latin America. International Journal of Environmental Research and Public Health. 2021; 18(5):2252. https://doi.org/10.3390/ijerph18052252
Chicago/Turabian StyleJaramillo, Diana, Lyndsay Krisher, Natalie V. Schwatka, Liliana Tenney, Gwenith G. Fisher, Rebecca L. Clancy, Erin Shore, Claudia Asensio, Stephane Tetreau, Magda E. Castrillo, and et al. 2021. "International Total Worker Health: Applicability to Agribusiness in Latin America" International Journal of Environmental Research and Public Health 18, no. 5: 2252. https://doi.org/10.3390/ijerph18052252
APA StyleJaramillo, D., Krisher, L., Schwatka, N. V., Tenney, L., Fisher, G. G., Clancy, R. L., Shore, E., Asensio, C., Tetreau, S., Castrillo, M. E., Amenabar, I., Cruz, A., Pilloni, D., Zamora, M. E., Butler-Dawson, J., Dally, M., & Newman, L. S. (2021). International Total Worker Health: Applicability to Agribusiness in Latin America. International Journal of Environmental Research and Public Health, 18(5), 2252. https://doi.org/10.3390/ijerph18052252