
Use of mHealth Technology for Patient-Reported Outcomes in Community-Dwelling Adults with Acquired Brain Injuries: A Scoping Review

 , , , , and
, , , , and
Abstract
:1. Introduction
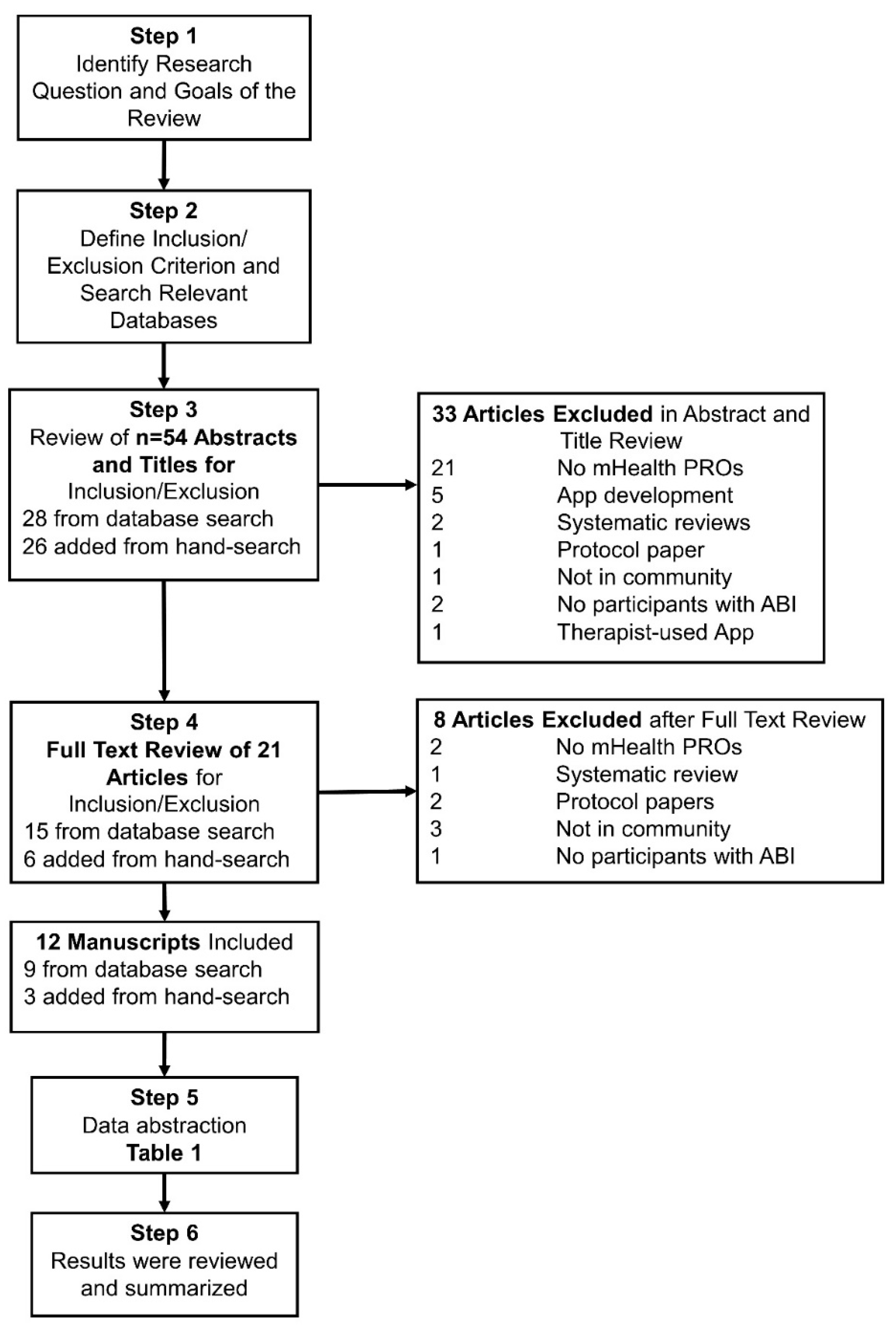
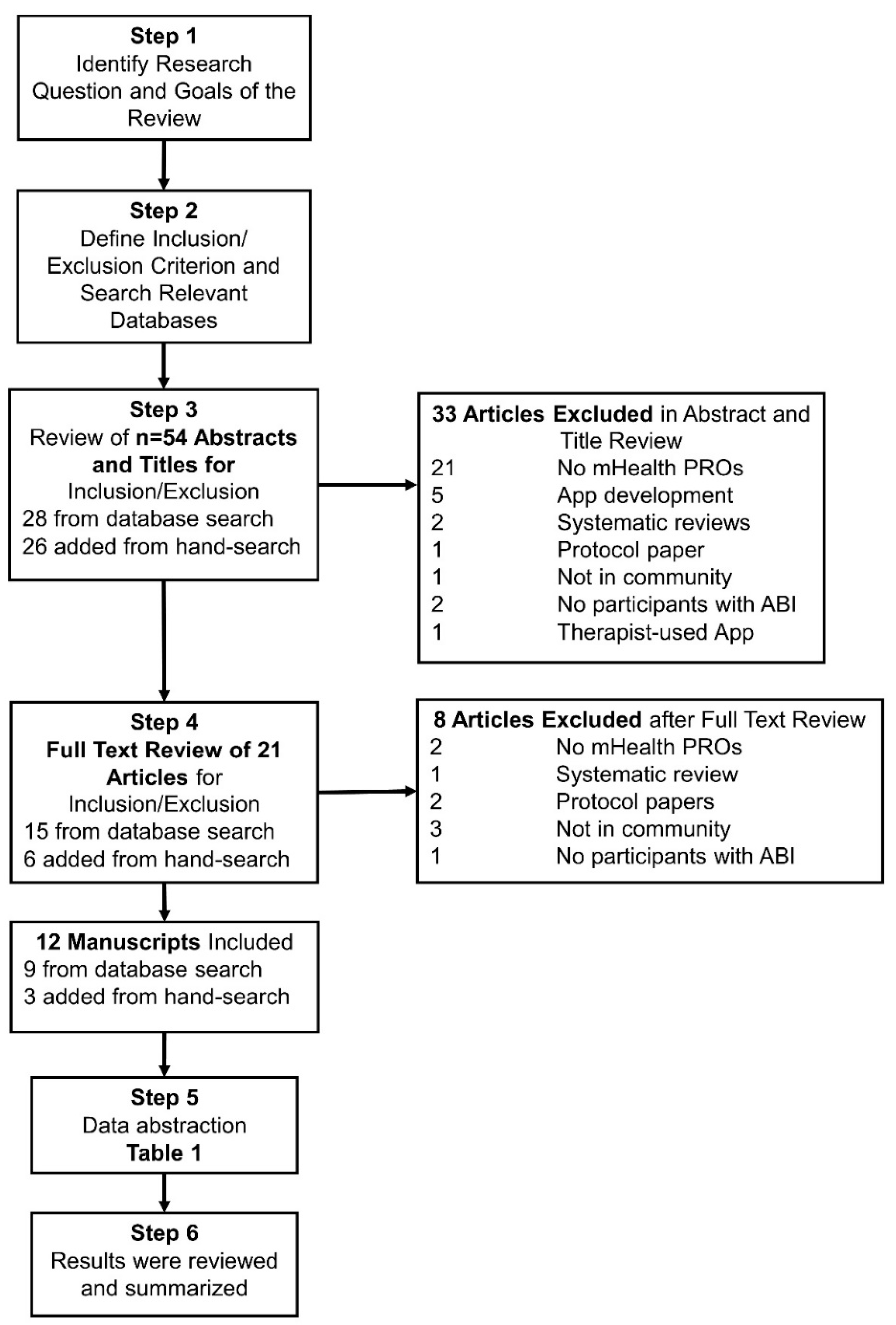
2. Materials and Methods
3. Results
3.1. Characteristics of Included Studies
3.2. Summary of mHealth Technology Used and Constructs Measured
3.3. Inclusion of Ecological Momentary Assessment via mHealth
3.4. Traumatic Brain Injury Studies and Findings
3.5. Stroke Studies and Findings
4. Discussion
Limitations
5. Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Coronado, V.G.; McGuire, L.C.; Sarmiento, K.; Bell, J.; Lionbarger, M.R.; Jones, C.D.; Geller, A.I.; Khoury, N.; Xu, L. Trends in Traumatic Brain Injury in the U.S. and the Public Health Response: 1995–2009. J. Saf. Res. 2012, 43, 299–307. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, 139–596. [Google Scholar] [CrossRef] [PubMed]
- Corrigan, J.D.; Hammond, F.M. Traumatic Brain Injury as a Chronic Health Condition. Arch. Phys. Med. Rehabil. 2013, 94, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.F.; Hahn, M.G.; Baum, C.M.; Perlmutter, M.S.; Sheedy, C.; Dromerick, A.W. Screening Patients with Stroke for Rehabilitation Needs: Validation of the Post-Stroke Rehabilitation Guidelines. Neurorehabilit. Neural Repair 2006, 20, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Masel, B.E.; DeWitt, D.S. Traumatic Brain Injury: A Disease Process, Not an Event. J. Neurotrauma 2010, 27, 1529–1540. [Google Scholar] [CrossRef] [Green Version]
- McMillan, T.M.; Teasdale, G.M.; Stewart, E. Disability in Young People and Adults after Head Injury: 12-14 Year Follow-up of a Prospective Cohort. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1086–1091. [Google Scholar] [CrossRef]
- Andelic, N.; Howe, E.I.; Hellstrøm, T.; Sanchez, M.F.; Lu, J.; Løvstad, M.; Røe, C. Disability and Quality of Life 20 Years after Traumatic Brain Injury. Brain Behav. 2018, 8, e01018. [Google Scholar] [CrossRef] [PubMed]
- Graven, C.; Brock, K.; Hill, K.; Joubert, L. Are Rehabilitation and/or Care Co-Ordination Interventions Delivered in the Community Effective in Reducing Depression, Facilitating Participation and Improving Quality of Life after Stroke? Disabil. Rehabil. 2011, 33, 1501–1520. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. National Center for Injury Prevention and Control; Division of Unintentional Injury Prevention: Atlanta, GA, USA, 2015. [Google Scholar]
- Turner, B.; Fleming, J.; Cornwell, P.; Worrall, L.; Ownsworth, T.; Haines, T.; Kendall, M.; Chenoweth, L. A Qualitative Study of the Transition from Hospital to Home for Individuals with Acquired Brain Injury and Their Family Caregivers. Brain Inj. 2007, 21, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Baker-Sparr, C.; Hart, T.; Bergquist, T.; Bogner, J.; Dreer, L.; Juengst, S.; Mellick, D.; O’Neil-Pirozzi, T.M.; Sander, A.M.; Whiteneck, G.G. Internet and Social Media Use After Traumatic Brain Injury: A Traumatic Brain Injury Model Systems Study. J. Head Trauma Rehabil. 2018, 33, E9–E17. [Google Scholar] [CrossRef]
- Street, L.N.W.; Washington, S.; Inquiries, D. 20036 202 419 4300|M. 202 419 4349|F. 202 419 4372|M. Mobile Fact Sheet. Pew Res. Cent. Internet Sci. Tech. 2017. Available online: http://www.pewinternet.org/fact-sheet/mobile (accessed on 2 February 2017).
- Ernsting, C.; Dombrowski, S.U.; Oedekoven, M.; Sullivan, J.L.O.; Kanzler, M.; Kuhlmey, A.; Gellert, P. Using Smartphones and Health Apps to Change and Manage Health Behaviors: A Population-Based Survey. J. Med. Internet Res. 2017, 19, e101. [Google Scholar] [CrossRef] [PubMed]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [Green Version]
- Osborne, C.L.; Juengst, S.B.; Smith, E.E. Identifying User-Centered Content, Design, and Features for Mobile Health Apps to Support Long-Term Assessment, Behavioral Intervention, and Transitions of Care in Neurological Rehabilitation: An Exploratory Study: Br. J. Occup. Ther. 2020. [Google Scholar] [CrossRef]
- Kwan, V.; Bihelek, N.; Anderson, V.; Yeates, K. A Review of Smartphone Applications for Persons with Traumatic Brain Injury: What Is Available and What Is the Evidence? J. Head Trauma Rehabil. 2019, 34, E45–E51. [Google Scholar] [CrossRef]
- Lynch, E.A.; Jones, T.M.; Simpson, D.B.; Fini, N.A.; Kuys, S.S.; Borschmann, K.; Kramer, S.; Johnson, L.; Callisaya, M.L.; Mahendran, N.; et al. Activity Monitors for Increasing Physical Activity in Adult Stroke Survivors. Cochrane Database Syst. Rev. 2018, 7, CD012543. [Google Scholar] [CrossRef]
- Zhou, X.; Du, M.; Zhou, L. Use of Mobile Applications in Post-Stroke Rehabilitation: A Systematic Review. Top. Stroke Rehabil. 2018, 489–499. [Google Scholar] [CrossRef]
- Juengst, S.B.; Hart, T.; Sander, A.M.; Nalder, E.J.; Pappadis, M.R. Mobile Health Interventions for Traumatic Brain Injuries. Curr. Phys. Med. Rehabil. Rep. 2019, 7, 341–356. [Google Scholar] [CrossRef]
- Anthes, E. Mental Health: There’s an App for That. Nat. News 2016, 532, 20. [Google Scholar] [CrossRef] [PubMed]
- Plackett, R.; Thomas, S.; Thomas, S. Professionals’ Views on the Use of Smartphone Technology to Support Children and Adolescents with Memory Impairment Due to Acquired Brain Injury. Disabil. Rehabil. Assist. Technol. 2017, 12, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.; Sinclair, K.; Seabrook, E.; McKay, A.; Ponsford, J. Smartphones as Assistive Technology Following Traumatic Brain Injury: A Preliminary Study of What Helps and What Hinders. Disabil. Rehabil. 2017, 39, 2387–2394. [Google Scholar] [CrossRef]
- Morris, J.; Jones, M.; Thompson, N.; Wallace, T.; DeRuyter, F. Clinician Perspectives on MRehab Interventions and Technologies for People with Disabilities in the United States: A National Survey. Int. J. Environ. Res. Public. Health 2019, 16, 4220. [Google Scholar] [CrossRef] [Green Version]
- Bradley, S.E.; Haun, J.; Powell-Cope, G.; Haire, S.; Belanger, H.G. Qualitative Assessment of the Use of a Smart Phone Application to Manage Post-Concussion Symptoms in Veterans with Traumatic Brain Injury. Brain Inj. 2020, 34, 1031–1038. [Google Scholar] [CrossRef]
- Jenkins, C.; Burkett, N.-S.; Ovbiagele, B.; Mueller, M.; Patel, S.; Brunner-Jackson, B.; Saulson, R.; Treiber, F. Stroke Patients and Their Attitudes toward MHealth Monitoring to Support Blood Pressure Control and Medication Adherence. mHealth 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.J. Assessing the Benefits of Using Assistive Technologies and Other Supports for Thinking, Remembering and Learning. Disabil. Rehabil. 2005, 27, 731–739. [Google Scholar] [CrossRef]
- Kettlewell, J.; Phillips, J.; Radford, K.; dasNair, R. Informing Evaluation of a Smartphone Application for People with Acquired Brain Injury: A Stakeholder Engagement Study. BMC Med. Inform. Decis. Mak. 2018, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.S.; Ryu, G.W.; Choi, M. Methodological Strategies for Ecological Momentary Assessment to Evaluate Mood and Stress in Adult Patients Using Mobile Phones: Systematic Review. JMIR MHealth UHealth 2019, 7, e11215. [Google Scholar] [CrossRef]
- Heron, K.E.; Smyth, J.M. Ecological Momentary Interventions: Incorporating Mobile Technology into Psychosocial and Health Behaviour Treatments. Br. J. Health Psychol. 2010, 15, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Pavliscsak, H.; Little, J.R.; Poropatich, R.K.; McVeigh, F.L.; Tong, J.; Tillman, J.S.; Smith, C.H.; Fonda, S.J. Assessment of Patient Engagement with a Mobile Application among Service Members in Transition. J. Am. Med. Inform. Assoc. 2016, 23, 110–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juengst, S.B.; Graham, K.M.; Pulantara, I.W.; McCue, M.; Whyte, E.M.; Dicianno, B.E.; Parmanto, B.; Arenth, P.M.; Skidmore, E.R.D.; Wagner, A.K. Pilot Feasibility of an MHealth System for Conducting Ecological Momentary Assessment of Mood-Related Symptoms Following Traumatic Brain Injury. Brain Inj. 2015, 29, 1351–1361. [Google Scholar] [CrossRef] [PubMed]
- Wiebe, D.J.; Nance, M.L.; Houseknecht, E.; Grady, M.F.; Otto, N.; Sandsmark, D.K.; Master, C.L. Ecologic Momentary Assessment to Accomplish Real-Time Capture of Symptom Progression and the Physical and Cognitive Activities of Patients Daily Following Concussion. JAMA Pediatr. 2016, 170, 1108–1110. [Google Scholar] [CrossRef]
- Worthen-Chaudhari, L.; McGonigal, J.; Logan, K.; Bockbrader, M.A.; Yeates, K.O.; Mysiw, W.J. Reducing Concussion Symptoms among Teenage Youth: Evaluation of a Mobile Health App. Brain Inj. 2017, 31, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Sufrinko, A.M.; Howie, E.K.; Charek, D.B.; Elbin, R.J.; Collins, M.W.; Kontos, A.P. Mobile Ecological Momentary Assessment of Postconcussion Symptoms and Recovery Outcomes. J. Head Trauma Rehabil. 2019, 34, E40–E48. [Google Scholar] [CrossRef] [PubMed]
- Juengst, S.B.; Terhorst, L.; Kew, C.L.; Wagner, A.K. Variability in Daily Self-Reported Emotional Symptoms and Fatigue Measured over Eight Weeks in Community Dwelling Individuals with Traumatic Brain Injury. Brain Inj. 2019, 33, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Lenaert, B.; Neijmeijer, M.; van Kampen, N.; van Heugten, C.; Ponds, R. Poststroke Fatigue and Daily Activity Patterns During Outpatient Rehabilitation: An Experience Sampling Method Study. Arch. Phys. Med. Rehabil. 2020, 101, 1001–1008. [Google Scholar] [CrossRef]
- Lenaert, B.; Colombi, M.; van Heugten, C.; Rasquin, S.; Kasanova, Z.; Ponds, R. Exploring the Feasibility and Usability of the Experience Sampling Method to Examine the Daily Lives of Patients with Acquired Brain Injury. Neuropsychol. Rehabil. 2017, 754–766. [Google Scholar] [CrossRef]
- Cooray, C.; Matusevicius, M.; Wahlgren, N.; Ahmed, N. Mobile Phone-Based Questionnaire for Assessing 3 Months Modified Rankin Score After Acute Stroke: A Pilot Study. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Seo, W.K.; Kang, J.; Jeon, M.; Lee, K.; Lee, S.; Kim, J.H.; Oh, K.; Koh, S.B. Feasibility of Using a Mobile Application for the Monitoring and Management of Stroke-Associated Risk Factors. J. Clin. Neurol. Seoul Korea 2015, 11, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Villain, M.; Sibon, I.; Renou, P.; Poli, M.; Swendsen, J. Very Early Social Support Following Mild Stroke Is Associated with Emotional and Behavioral Outcomes Three Months Later. Clin. Rehabil. 2017, 31, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Fors, U.; Kamwesiga, J.T.; Eriksson, G.M.; von Koch, L.; Guidetti, S. User Evaluation of a Novel SMS-Based Reminder System for Supporting Post-Stroke Rehabilitation. BMC Med. Inform. Decis. Mak. 2019, 19, 122. [Google Scholar] [CrossRef] [PubMed]
- Lenaert, B.; Meulders, A.; van Heugten, C.M. Tired of Pain or Painfully Tired? A Reciprocal Relationship between Chronic Pain and Fatigue. Pain 2018, 159, 1178–1179. [Google Scholar] [CrossRef] [PubMed]
- Shiffman, S. Conceptualizing Analyses of Ecological Momentary Assessment Data. Nicotine Tob. Res. Off. J. Soc. Res. Nicotine Tob. 2014, 16 (Suppl. 2), S76–87. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Runyan, J.D.; Steenbergh, T.A.; Bainbridge, C.; Daugherty, D.A.; Oke, L.; Fry, B.N. A Smartphone Ecological Momentary Assessment/Intervention “App” for Collecting Real-Time Data and Promoting Self-Awareness. PLoS ONE 2013, 8, e71325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smyth, J.M.; Stone, A.A. Ecological Momentary Assessment Research in Behavioral Medicine. J. Happiness Stud. 2003, 4, 35–52. [Google Scholar] [CrossRef]
- Burke, L.E.; Shiffman, S.; Music, E.; Styn, M.A.; Kriska, A.; Smailagic, A.; Siewiorek, D.; Ewing, L.J.; Chasens, E.; French, B.; et al. Ecological Momentary Assessment in Behavioral Research: Addressing Technological and Human Participant Challenges. J. Med. Internet Res. 2017, 19, e77. [Google Scholar] [CrossRef]
- Lui, J.H.L.; Marcus, D.K.; Barry, C.T. Evidence-Based Apps? A Review of Mental Health Mobile Applications in a Psychotherapy Context. Prof. Psychol. Res. Pract. 2017, 48, 199–210. [Google Scholar] [CrossRef]
- Edbrooke-Childs, J.; Smith, J.; Rees, J.; Edridge, C.; Calderon, A.; Saunders, F.; Wolpert, M.; Deighton, J. An App to Help Young People Self-Manage When Feeling Overwhelmed (ReZone): Protocol of a Cluster Randomized Controlled Trial. JMIR Res. Protoc. 2017, 6, e213. [Google Scholar] [CrossRef]
- English, L.L.; Dunsmuir, D.; Kumbakumba, E.; Ansermino, J.M.; Larson, C.P.; Lester, R.; Barigye, C.; Ndamira, A.; Kabakyenga, J.; Wiens, M.O. The PAediatric Risk Assessment (PARA) Mobile App to Reduce Postdischarge Child Mortality: Design, Usability, and Feasibility for Health Care Workers in Uganda. JMIR MHealth UHealth 2016, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebden, L.; Cook, A.; van der Ploeg, H.P.; Allman-Farinelli, M. Development of Smartphone Applications for Nutrition and Physical Activity Behavior Change. JMIR Res. Protoc. 2012, 1, e9. [Google Scholar] [CrossRef]
- Mena, L.; Felix, V.; Ostos, R.; Gonzalez, J.; Cervantes, A.; Ochoa, A.; Ruiz, C.; Ramos, R.; Maestre, G. Mobile Personal Health System for Ambulatory Blood Pressure Monitoring. Comput. Math. Methods Med. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, I.; Ahmad, N.S.; Ali, S.; Ali, S.; George, A.; Danish, H.S.; Uppal, E.; Soo, J.; Mobasheri, M.H.; King, D.; et al. Medication Adherence Apps: Review and Content Analysis. JMIR MHealth UHealth 2018, 6, e62. [Google Scholar] [CrossRef] [PubMed]
- Byambasuren, O.; Sanders, S.; Beller, E.; Glasziou, P. Prescribable MHealth Apps Identified from an Overview of Systematic Reviews. NPJ Digit. Med. 2018, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellbeing, Recovery and Mental Health. Available online: https://www.cambridge.org/core/books/wellbeing-recovery-and-mental-health/26DC535A216270DB76A571337DC20F1D (accessed on 16 December 2020).
- Rowland, S.P.; Fitzgerald, J.E.; Holme, T.; Powell, J.; McGregor, A. What Is the Clinical Value of MHealth for Patients? NPJ Digit. Med. 2020, 3, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nouri, R.; Niakan Kalhori, S.R.; Ghazisaeedi, M.; Marchand, G.; Yasini, M. Criteria for Assessing the Quality of MHealth Apps: A Systematic Review. J. Am. Med. Inform. Assoc. 2018, 25, 1089–1098. [Google Scholar] [CrossRef] [Green Version]
- Pham, Q.; Graham, G.; Carrion, C.; Morita, P.P.; Seto, E.; Stinson, J.N.; Cafazzo, J.A. A Library of Analytic Indicators to Evaluate Effective Engagement with Consumer MHealth Apps for Chronic Conditions: Scoping Review. JMIR MHealth UHealth 2019, 7, e11941. [Google Scholar] [CrossRef]
- Jones, M.; Morris, J.; Deruyter, F. Mobile Healthcare and People with Disabilities: Current State and Future Needs. Int. J. Environ. Res. Public. Health 2018, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, C.; Bergin, M.; Wells, J.S. Theoretical Perspectives of Adherence to Web-Based Interventions: A Scoping Review. Int. J. Behav. Med. 2018, 25, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Burkow, T.M.; Vognild, L.K.; Johnsen, E.; Bratvold, A.; Risberg, M.J. Promoting Exercise Training and Physical Activity in Daily Life: A Feasibility Study of a Virtual Group Intervention for Behaviour Change in COPD. BMC Med. Inform. Decis. Mak. 2018, 18, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajani, N.B.; Weth, D.; Mastellos, N.; Filippidis, F.T. Use of Gamification Strategies and Tactics in Mobile Applications for Smoking Cessation: A Review of the UK Mobile App Market. BMJ Open 2019, 9, e027883. [Google Scholar] [CrossRef] [PubMed]
- Timpel, P.; Cesena, F.H.Y.; da Silva Costa, C.; Soldatelli, M.D.; Gois, E.; Castrillon, E.; Díaz, L.J.J.; Repetto, G.M.; Hagos, F.; Castillo Yermenos, R.E.; et al. Efficacy of Gamification-Based Smartphone Application for Weight Loss in Overweight and Obese Adolescents: Study Protocol for a Phase II Randomized Controlled Trial. Ther. Adv. Endocrinol. Metab. 2018, 9, 167–176. [Google Scholar] [CrossRef]
- Moeckli, J.; Cram, P.; Cunningham, C.; Reisinger, H.S. Staff Acceptance of a Telemedicine Intensive Care Unit Program: A Qualitative Study. J. Crit. Care 2013, 28, 890–901. [Google Scholar] [CrossRef] [PubMed]
- Sittig, D.F.; Krall, M.A.; Dykstra, R.H.; Russell, A.; Chin, H.L. A Survey of Factors Affecting Clinician Acceptance of Clinical Decision Support. BMC Med. Inform. Decis. Mak. 2006, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Blumenthal, J.; Wilkinson, A.; Chignell, M. Physiotherapists’ and Physiotherapy Students’ Perspectives on the Use of Mobile or Wearable Technology in Their Practice. Physiother. Can. 2018, 70, 251–261. [Google Scholar] [CrossRef]
- Centers for Medicare & Medicaid Services (CMS), HHS Medicare Program. Revisions to Payment Policies under the Physician Fee Schedule, Clinical Laboratory Fee Schedule, Access to Identifiable Data for the Center for Medicare and Medicaid Innovation Models & Other Revisions to Part B for CY 2015. Final Rule with Comment Period. Fed Regist. 2014, 79, 67547–68010. Available online: https://pubmed.ncbi.nlm.nih.gov/25507411/ (accessed on 25 September 2020).
- 4 Trends in Gartner Hype Cycle for Customer Service and Customer Engagement. Available online: //www.gartner.com/smarterwithgartner/4-trends-gartner-hype-cycle-customer-service-customer-engagement/ (accessed on 5 January 2021).
- Gartner Top Strategic Predictions for 2018 and Beyond. Available online: //www.gartner.com/smarterwithgartner/gartner-top-strategic-predictions-for-2018-and-beyond/ (accessed on 5 January 2021).

{kind=link}
| Authors (Year) [Reference] | Title | Sample | Construct/s & Measures | Design |
|---|---|---|---|---|
| Traumatic Brain Injury | ||||
| Pavliscsk et al. (2016) [33] | Assessment of patient engagement with a mobile application among service members in transition. | n = 95 service members Gender: 80 male; 15 female Average Age: 34.7–39.7 Severity: unknown Chronicity: unknown Other: participants grouped by health status (see below) n = 40 w/o Behavioral Health Problem Gender: 33 male;7 female Average Age: 39.7 (10.4) n = 22 w/ Behavioral Health Problem(s) Only Gender: 16 male; 6 female Average Age: 34.7 (10.3) n = 24 w Behavioral Health Problem(s) Plus PTSD and/or TBI Gender: 22 male;2 female Average Age: 37.7 (10.2) n = 9 w/ PTSD and/or TBI Gender: 9 male; 0 female Average Age: 38.7 (12.3) | Participant engagement
| Secondary data analysis of one arm of a multisite prospective RCT. Frequency of Assessment: Participants received 7 daily questionnaires (each sent once per week) for up to 36 weeks. |
| Juengst et al. (2015) | Pilot feasibility of an mHealth system for conducting ecological momentary assessment of mood-related symptoms following traumatic brain injury. | n = 20 community-dwelling adults with TBI (3 completed baseline assessments only). Gender: 12 male; 8 female Average Age: 36.7 (12.4) Average Time Since Injury: 5.2 (3.6) | Feasibility:
| Prospective, repeated-measures. Mood-related symptoms assessed at Baseline, and over 8 weeks using the iPerform app and biweekly phone interviews. |
| Wiebe et al. (2016) | Ecologic Momentary Assessment to Accomplish Real-Time Capture of Symptom Progression and the Physical and Cognitive Activities of Patients Daily Following Concussion | n = 34 youth with concussion. Gender: 18 male; 16 female Median Age: 15 (IQR 13–16) Median Time Since Injury: 6 days (IQR 3–10) | Concussion Symptoms
| Baseline in person and then two weeks of daily (several times per day) symptom and activity reporting |
| Worthen-Chaudhari et al. (2017) | Reducing concussion symptoms among teenage youth: phase I and II evaluation of a mobile health app | Phase I: n = 20 youth with concussion Average Age: 16.6 +/− 1.6 years Gender: Males 6 (30%) Phase II: n = 22 youth with concussion Average Age: 15.6+/− 1.7 years Gender: Males 5 (22.7%) | Concussion Symptoms
| Phase I and Phase II open-label, non-randomized trial Event-related reporting with a target of 1x daily for 5/7 days per week for 3 weeks. |
| Sufrinko et al. (2019) | Mobile Ecological Momentary Assessment of Post-concussion Symptoms and Recovery Outcomes. | n = 20 athletes with sports-related concussion (SRC) Sex: 12 male; 8 female Age Range: 12–19 | Post-Concussion Symptoms
“mEMA symptom score” (modified PCSS, excluding nighttime sleep symptoms): total symptom score, symptom factor scores (cognitive-migraine-fatigue, somatic, affective). “Patient recovery duration”: days until medical clearance. | Prospective study. Visit 1—<72 h post-injury. Included clinical testing measures. Visit 2—6–18 days post-injury. Included clinical testing measures. mEMA questionnaire—surveys sent at 3 fixed times blocks (morning, afternoon, and evening), every day until medical clearance or second follow-up (whichever came first). Included activity type and mEMA symptom score measures. |
| Juengst et al. (2019) | Variability in daily self-reported emotional symptoms and fatigue measured over eight weeks in community dwelling individuals with traumatic brain injury. | n = 18 people with TBI Average Age =38.3 (22–60), Gender: 10 men; 8 women | EMA of mood:
| Secondary data analysis Participants were in a feasibility study using smartphone to assess daily mood-related symptoms in m-s TBI. Mood related symptoms were collected for 8 weeks daily. |
| TBI and Stroke | ||||
| Lenaert et al. (2018) | Exploring the feasibility and usability of the experience sampling method to examine the daily lives of patients with acquired brain injury | In the Netherlands: n = 17 adults with stroke or traumatic brain injury Stroke: n = 9 TBI: n = 8 Age range: 18–65 Average Age: 44.2 (14.5) Gender: Males 8 (47%) | Mood: Positive & Negative Affect Schedule (PANAS) Location Social Context Activities Physical well-being (including fatigue) | Longitudinal observational study. 10 random moments daily for 6 days to measure mood, location & context, activities, and well-being. |
| Stroke | ||||
| Cooray et al. (2015) | Mobile Phone-Based Questionnaire for Assessing 3 Months Modified Rankin Score After Acute Stroke: A Pilot Study. | n = 48 acute stroke patients and/or their caregivers Responses from:
Average Age: 67 | Modified Rankin Scale (mRS): measure of functional level (degree of disability/dependence) after stroke. Rankin Focused Assessment (RFA): structured form of the mRS (reduces inter-rater variability). Translated to Swedish. | Cohort study Participants were reminded via monthly messages in the app of participation. At 3 months, participants were sent RFA via the app. Within 1 week after RFA, personnel blinded to participants’ scores rated participants using mRS in clinic. |
| Seo et al. (2015) | Feasibility of using a mobile application for the monitoring & management of stroke-associated risk factors. | n = 48 Average Age: 52.65+/− 10.25 years Gender: Males 36 (75%) | Daily reports and measures of risk factors for stroke:
| Prospective, single-center, single-arm, open-label clinical trial |
| Villain et al. (2017) | Very early social support following mild stroke is associated with emotional and behavioral outcomes three months later. | n = 34 patients with mild ischemic stroke Average Age: 57 Gender: 36% female | Depression and anxiety:
Electronic interview | Cohort design (data collected baseline and 3 months post hospital discharge) Used an ordinal scale (EMA) 1 day 5x/day and another for 7 days 5x/day @ 3 months later; mood and depression symptoms: 7-point ordinal scale (EMA) |
| Fors et al. (2019) | User evaluation of a novel SMS-based reminder system for supporting post-stroke rehabilitation. | In Uganda: n = 15 people with stroke participated in SMS study. 2 patients dropped out, 2 did not participate in interviews (interview n = 11). 11 family members and 4 OT also participated in interviews. Age/Gender: No age and gender presented. | Success rate for performing three daily activities: Daily SMS responses Experiences with the SMS tool: Individual semi-structured interviews to learn user opinions. OT Feedback: questionnaire | Mixed Methods Texts to remind participants to complete daily activities for 8 weeks. Participants responded if completed. Semi-structured interviews w/ participants, family, OTs. |
| Lenaert et al. (2020) | Poststroke Fatigue and Daily Activity Patterns During Outpatient Rehabilitation: An Experience Sampling Method Study | In Netherlands: n = 26 adults with stroke Average Age: 55.3 (7.6) Gender: Males 13 (50%) | Fatigue: Fatigue Severity Scale (FSS). Anxiety and depression: Hospital Depression Anxiety Scale (HADS) | Longitudinal observational study. 10 random moments daily for 6 days to measure fatigue and activity |
| Authors [Reference] | Technology Used | EMA | Purpose | Outcome Measures and Results |
|---|---|---|---|---|
| Traumatic Brain Injury | ||||
| Pavliscsk et al. [33] | “mCare” application: bidirectional mobile health system through which participants answered the weekly questionnaires. 2-Way App Participants completed questionnaires, and participants and providers could exchange messages through app. App developed for community use only | Yes | To examine the relationship between health status (behavioral health problems, TBI, and PTSD) and engagement with the mCare mobile app among wounded Service Members rehabilitating in the community. | Participant engagement: encompassed exposure to mCare, percentage of questionnaires responded to, and response time. Acceptable Compliance In general, participants responded to ≥60% of the questionnaires each week, and in ≤10 h. Those with behavioral problems, though, had several weeks with a <50% response rate, and had the longest response times. Exposure to mCare, total questionnaires responded to, and response time did not differ significantly by health status. Older age and higher General Well-Being Schedule scores (self-report questionnaire, measuring an individual’s sense of well-being) were associated with greater and faster responses. Psychometric Properties Reported for EMA: No |
| Juengst et al. | iPerform: a user-centered, cross-platform smartphone app. 2-Way App User interface interacts with participant. Participants sent notifications to complete assessments. Maintains connection with clinician/ researcher portal; could set assessment schedules and sent messages through app. App developed for community use only | Yes | To assess the feasibility and validity of an mHealth system for tracking mood-related symptoms after TBI. | Good compliance: Participants correctly completed 73.4% of all scheduled assessments. On average, daily assessments took <2 min to complete. High satisfaction with smartphone apps: 6.3 of 7. Participants found apps easy to use: 6.2 of 7. Psychometric Properties Reported for EMA: Yes Validity of conducting these assessments via smartphone application in this population: PHQ-9 and GAD-7 scores from phone interview and mobile app were highly correlated—(r = 0.81–0.97) |
| Wiebe et al. | iPod Touch & accelerometer (Custom app loaded on iPod) 1-Way App: Participants answered questions via app. App training during initial clinical visit, all measures collected in the community. | Yes | To determine feasibility of EMA after youth concussion, gather real-time cognitive and physical activity, and compare objective measures with real-time self-reported symptoms. | Good compliance: 82% responded to >80% of prompts. Cognitive exertion and concussion symptoms were positively correlated on the same day and on the following 2 days. Physical activity and concussion symptoms were negatively correlated on the same day and 2 following days. Most participants (68%) were no longer reporting symptoms at the end of the two weeks. Psychometric Properties Reported for EMA: No |
| Worthen-Chaudhari et al. | Mobile device app (Gamified symptom reporting app: Battle Royal Power Pack) 2-Way App: Patient symptom reporting via gamification and logged activity. Research coordinator could be invited as an “ally” to send comments, emails, etc. App developed for community use only. | Yes | To evaluate if reporting symptoms in a social game designed mobile health app complimented medical care for unresolved symptoms of concussion. | Feasibility and satisfaction: Phase I Positive changes in SCAT-3 concussion symptoms, depression, optimism: Phase II No significant correlations between concussion symptom change and optimism change. Phase I Barriers to Compliance: 6 of 14 participants had barriers. Barriers included: Discontinuation of medical care 3 Internet challenges: 1 Extracurriculars: 1 Other illness during study: 1 Phase II Barriers to Compliance: Not reported Mobile apps that integrate social game mechanics with a heroic narrative may support health management in teenagers with unresolved concussion symptoms. Psychometric Properties Reported for EMA: No |
| Sufrinko et al. | Mobile ecological momentary assessment (mEMA) application. 1-Way App: Participants sent notifications to complete assessments. App developed for community use only | Yes | Evaluate mEMA as an approach to measure SRC symptoms, explore the relationships between clinical outcomes and mEMA, and determine whether mEMA was advantageous for predicting recovery outcomes compared to traditional symptom report. | Compliance: 52.4% for prompts and 50.4% per participant. Symptoms were lower in the morning compared with afternoon and evening. Higher mEMA symptoms were reported during vestibular compared with physical and sedentary activities. mEMA symptoms were positively associated with PCSS, VOMS, and recovery time, but not neurocognitive scores. mEMA symptom score was a better predictor of recovery time than PCSS at either clinic visit. Psychometric Properties Reported for EMA: No |
| Juengst et al. | iPerform: a user-centered, cross-platform smartphone app. 2-Way App Participants sent notifications to complete assessments; Clinicians could set custom assessment schedules and sent messages through app. App developed for community use only | Yes | To identify potential characteristics that differed between individuals having high versus low variability in symptom reporting. | Significant within-person variability in reporting across all measures. Women, people with more symptoms, or people with higher cognitive performance report high variability Compliance reported in previous publication (Juengst, et al., 2015) Psychometric Properties Reported for EMA: No (previously reported in Juengst et al., 2015) |
| Lenaert et al. | Smartphone application (PsyMate) 1-Way App: Participants were prompted with beeps to complete surveys. App developed for community use only. | Yes | Investigate the feasibility of using experience sampling in individuals with ABI and explore the usability of experience sampling data | Compliance: 71% response rate High feasibility and no dropouts, with reports of being user-friendly. Participants reported that questions in PsyMate were a good representation of their experiences. Physical activity and fatigue predicted more negative affect on the same day, but not on later days. Provides a good example of instructions and planning Psychometric Properties Reported for EMA: No |
| Cooray et al. | Medipal: smartphone (iPhone and Android) app used to answer questionnaire. 1-Way App: Participants answered questionnaire via app. App training during hospital stay, not used until after discharge to community. | No | To investigate whether automatic assessment of the mRS based on a mobile phone questionnaire may serve an alternative to mRS assessments at clinical visits after stroke. | Compliance: 48/62 (77%) completed the assessment Median 3-month clinical visit mRS: 2. Mean 3-month clinical visit mRS: 2.3. Dichotomized mRS outcome separating functionally independent (mRS score 0–2) from dependent (mRS score 3–5) showed 83% agreement and unweighted kappa of 0.66 (95% confidence interval 0.45–0.87). Psychometric Properties Reported for electronic measure: Yes 62.5% agreement between clinical visit and mobile mRS assessment. Weighted kappa: 0.89 (95% confidence interval 0.82–0.96). Unweighted kappa: 0.53 (95% confidence interval 0.36–0.70). |
| Seo et al. | Smartphone application 2-Way App: Participants answered questionnaire via app. If data out of normal range, they received an automated alarm, as did researcher/clinician. App developed for community use only. | Yes | To assess feasibility of tracking vascular risk factors to improve risk management in persons with stroke | Fair Compliance: 50% labeled as compliant (defined by authors as completing >47 of 180 days) Adherence, blood pressure, HbA1c, waist circumference, smoking status. Averages number of days tracked (out of 180) was 60.42 ± 50.17; median = 47, range:1–180. Target achievement for parameters did not differ based on compliance. A shift in risk profiles in a favorable direction was observed in the entire sample. Psychometric Properties Reported for EMA: No |
| Villain et al. | Personal Digital Assistant (PDA) Palm Tungsten E2. Software and custom-designed measurement tool not described. 1-Way (PDA) Participants responded to a rating of mood App was started in the clinic with follow-up in community | Yes | Determine the association between the intensity of material and social support measured using EMA in the acute post-stroke phase with the occurrence of depressive symptoms and daily life activities 3 months later | Acceptable compliance: 77.3% (33/44) completed 3-month follow-up EMA Patient perceptions of the quality of moral support during hospitalization was associated with later decrease in depressive symptoms (ᵧ = 0.097, t = −2.141, p = 0.041) and with later increase in ADL participation (ᵧ = 0.367, t = 2.783, p = 0.011). Greater perceived material support was associated with later increases in ADLs (ᵧ = 0.333, t = 2.710, p = 0.0112). Psychometric Properties Reported for EMA: No |
| Fors et al. | SMS text message via phone (not smart phone). International commercial SMS API service called Twilio™ (Twilio.com). 2-Way Participants responded to text messages and local OTs could use web-based management system to see responses and respond via text Text messaging occurred only in community | Yes | Test the usability of a SMS based reminder system to remind patients to perform daily rehab activities and to measure rate of performance from users. Preferences of stakeholders also captured from patients, family members, and therapists. | Compliance: not reported Family and patients had positive opinions. Technical issues:
|
| Lenaert et al. | Smartphone application (PsyMate) 1-Way App: Participants were prompted with beeps to complete surveys. App developed for community use only. | Yes | To investigate post-stroke fatigue in relation to daily activity patterns during long-term post-stroke rehabilitation. | Acceptable compliance: 39 out of 60 questionnaires completed per participant (65% completion rate). Participants indicated at least “some fatigue” in 85% of momentary assessments and more severe fatigue in 61% of momentary assessments. Participants were relaxing, nothing, or resting in 48.9% of assessments, were doing household activities, self-care, or transport in 24.7% of assessments, and doing something else in 22.3% of assessments. Fatigue was highest when participants were “doing nothing” or “resting”. Higher effort and lower enjoyment were associated with higher fatigue. More physical activity was associated with more fatigue. Current fatigue was higher when earlier activities required more effort or more physical activity. Psychometric Properties Reported for EMA: No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juengst, S.B.; Terhorst, L.; Nabasny, A.; Wallace, T.; Weaver, J.A.; Osborne, C.L.; Burns, S.P.; Wright, B.; Wen, P.-S.; Kew, C.-L.N.; et al. Use of mHealth Technology for Patient-Reported Outcomes in Community-Dwelling Adults with Acquired Brain Injuries: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2173. https://doi.org/10.3390/ijerph18042173
Juengst SB, Terhorst L, Nabasny A, Wallace T, Weaver JA, Osborne CL, Burns SP, Wright B, Wen P-S, Kew C-LN, et al. Use of mHealth Technology for Patient-Reported Outcomes in Community-Dwelling Adults with Acquired Brain Injuries: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(4):2173. https://doi.org/10.3390/ijerph18042173
Chicago/Turabian StyleJuengst, Shannon B., Lauren Terhorst, Andrew Nabasny, Tracey Wallace, Jennifer A. Weaver, Candice L. Osborne, Suzanne Perea Burns, Brittany Wright, Pey-Shan Wen, Chung-Lin Novelle Kew, and et al. 2021. "Use of mHealth Technology for Patient-Reported Outcomes in Community-Dwelling Adults with Acquired Brain Injuries: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 4: 2173. https://doi.org/10.3390/ijerph18042173
APA StyleJuengst, S. B., Terhorst, L., Nabasny, A., Wallace, T., Weaver, J. A., Osborne, C. L., Burns, S. P., Wright, B., Wen, P.-S., Kew, C.-L. N., & Morris, J. (2021). Use of mHealth Technology for Patient-Reported Outcomes in Community-Dwelling Adults with Acquired Brain Injuries: A Scoping Review. International Journal of Environmental Research and Public Health, 18(4), 2173. https://doi.org/10.3390/ijerph18042173