
Statistical Estimation of Effects of Implemented Government Policies on COVID-19 Situation in South Korea

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. COVID-19 Confirmed Cases Data
2.2. Oxford COVID-19 Government Response Tracker (OxCGRT) Data
2.3. Segmented Poisson Model
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, J.Y.; Yun, J.G.; Noh, J.Y.; Cheong, H.J.; Kim, W.J. Covid-19 in South Korea—Challenges of Subclinical Manifestations. N. Engl. J. Med. 2020, 382, 1858–1859. [Google Scholar] [CrossRef] [PubMed]
- Eunha, S.; Amna, T.; Wongyeong, C.; Yiseul, L.; Gerardo, C. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. 2020, 93, 339–344. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. Available online: http://www.kdca.go.kr/cdc_eng/ (accessed on 3 January 2021).
- Agoda. Seoul Travel: Top Attractions and Things to Do in Itaewon. Available online: https://www.agoda.com/travel-guides/south-korea/seoul/seoul-travel-top-attractions-things-itaewon?cid=1844104 (accessed on 5 December 2020).
- Kang, C.R.; Lee, J.Y.; Park, Y.; Huh, I.S.; Ham, H.J.; Han, J.K.; Kim, J.I.; Na, B.J.; SCoRR Team. Coronavirus disease exposure and spread from nightclubs, South Korea. Emerg. Infect. Dis. 2020, 26, 2499–2501. [Google Scholar] [CrossRef] [PubMed]
- Gerardo, C. Fitting dynamic models to epidemic outbreaks with quantified uncertainty: A primer for parameter uncertainty, identifiability, and forecasts. Infect. Dis. Modell. 2017, 2, 379–398. [Google Scholar] [CrossRef]
- Gerardo, C.; Viboud, C.; Simonsen, L.; Merler, S.; Vespignani, A. Perspectives on model forecasts of the 2014–2015 ebola epidemic in West Africa: Lessons and the way forward. BMC Med. 2017, 15, 42. [Google Scholar]
- Ferguson, N.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba, Z.; Cuomo-Dannenburg, G.; et al. Impact of Non-Pharmaceutical Interventions (Npis) to Reduce Covid-19 Mortality and Healthcare Demand; Imperial College: London, UK, 2020. [Google Scholar] [CrossRef]
- Brzezinski, A.; Guido, D.; Valentin, K.; Van Dijcke, D. The Covid-19 Pandemic: Government vs. Community Action across the United States; Discussion Paper; CEPR: London, UK, 2020. [Google Scholar]
- Hsiang, S.; Allen, D.; Annan-Phan, S.; Bell, K.; Bolliger, I.; Chong, T.; Druckenmiller, H.; Huang, L.Y.; Hultgren, A.; Krasovich, E.; et al. The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature 2020, 584, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Kawaguchi, K.; Kodama, N.; Tanaka, M. Small Business under the COVID-19 Crisis: Expected Short- and Medium-Run Effects of Anti-Contagion and Economic Policies. 2020. Available online: https://ssrn.com/abstract=3634544 (accessed on 5 December 2020). [CrossRef]
- Lee, D.; Heo, K.; Seo, Y. COVID-19 in South Korea: Lessons for developing countries. World Dev. 2020, 135, 105057. [Google Scholar] [CrossRef] [PubMed]
- Majeed, A.; Seo, Y.; Lee, D. Can the UK emulate the South Korean approach to covid-19? BMJ 2020. Available online: https://www.bmj.com/content/369/bmj.m2084 (accessed on 5 December 2020).
- Kim, A. Second, Worse Wave Underway in Korea: KCDC. The Korea Herald, 18 August 2020. Available online: www.koreaherald.com/view.php?ud=20200818000204 (accessed on 3 January 2021).
- Ock, H.-J. Korea’s COVID-19 Situation More Worrying Than in May: KCDC. The Korea Herald 13 August 2020. Available online: www.koreaherald.com/view.php?ud=20200813000713 (accessed on 3 January 2021).
- Riyaz Ul, K.S. Korea: COVID-19 Forces Ban on Gatherings in Seoul. Available online: https://www.aa.com.tr/en/asia-pacific/skorea-covid-19-forces-ban-on-gatherings-in-seoul/1947798 (accessed on 3 January 2021).
- Blavatnik School of Government, University of Oxford. Coronavirus Government Response Tracker. Available online: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (accessed on 5 December 2020).
- NeurIPS 2020 Data Science for COVID-19 (DS4C). DS4C: Data Science for COVID-19 in South Korea. Available online: https://www.kaggle.com/kimjihoo/coronavirusdataset (accessed on 20 November 2020).
- Korea Information Society Agency Korea Information Society Agency. Available online: https://data.go.kr/data/15043378/openapi.do (accessed on 3 January 2021).
- Codebook for the Oxford Covid-19 Government Response Tracker. Available online: https://github.com/OxCGRT/covid-policytracker/blob/master/documentation/codebook.md (accessed on 20 November 2020).
- Mitacchione, G.; Schiavone, M.; Curnis, A.; Arca, M.; Antinori, S.; Gasparetti, A.; Mascioli, G.; Severino, P.; Sabato, F.; Mancone, M.; et al. Impact of prior statin use on clinical outcomes in COVID-19 patients: Data from tertiary referral hospitals during COVID-19 pandemic in Italy. J. Clin. Lipidol. 2020. [Google Scholar] [CrossRef]
- Mueller, A.L.; McNamara, M.S.; Sinclair, D.A. Why does COVID-19 disproportionately affect older people? Aging 2020, 12, 9959–9981. [Google Scholar] [CrossRef]
- Older Adults, at Greater Risk of Requiring Hospitalization or Dying If Diagnosed with COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html (accessed on 3 January 2021).
- Ho, F.K.; Petermann-Rocha, F.; Gray, S.R.; Bhautesh, D.J.; Katikireddi, S.V.; Niedzwiedz, C.N.; Foster, H.; Hastie, C.E.; Mackay, D.F.; Gill, J.M.R.; et al. Is older age associated with COVID-19 mortality in the absence of other risk factors? General population cohort study of 470,034 participants. PLoS ONE 2020, 15, e0241824. [Google Scholar] [CrossRef] [PubMed]
- Apio, C.; Kamruzzaman, M.; Park, T. Confidence intervals for the COVID-19 neutralizing antibody retention rate in the Korean population. Genomics Inform. 2020, 18, e31. [Google Scholar] [CrossRef] [PubMed]
- Kamruzzaman, M.; Apio, C.; Park, T. Updated confidence intervals for the COVID-19 antibody retention rate in the Korean population. Genomics Inform. 2020, e45. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
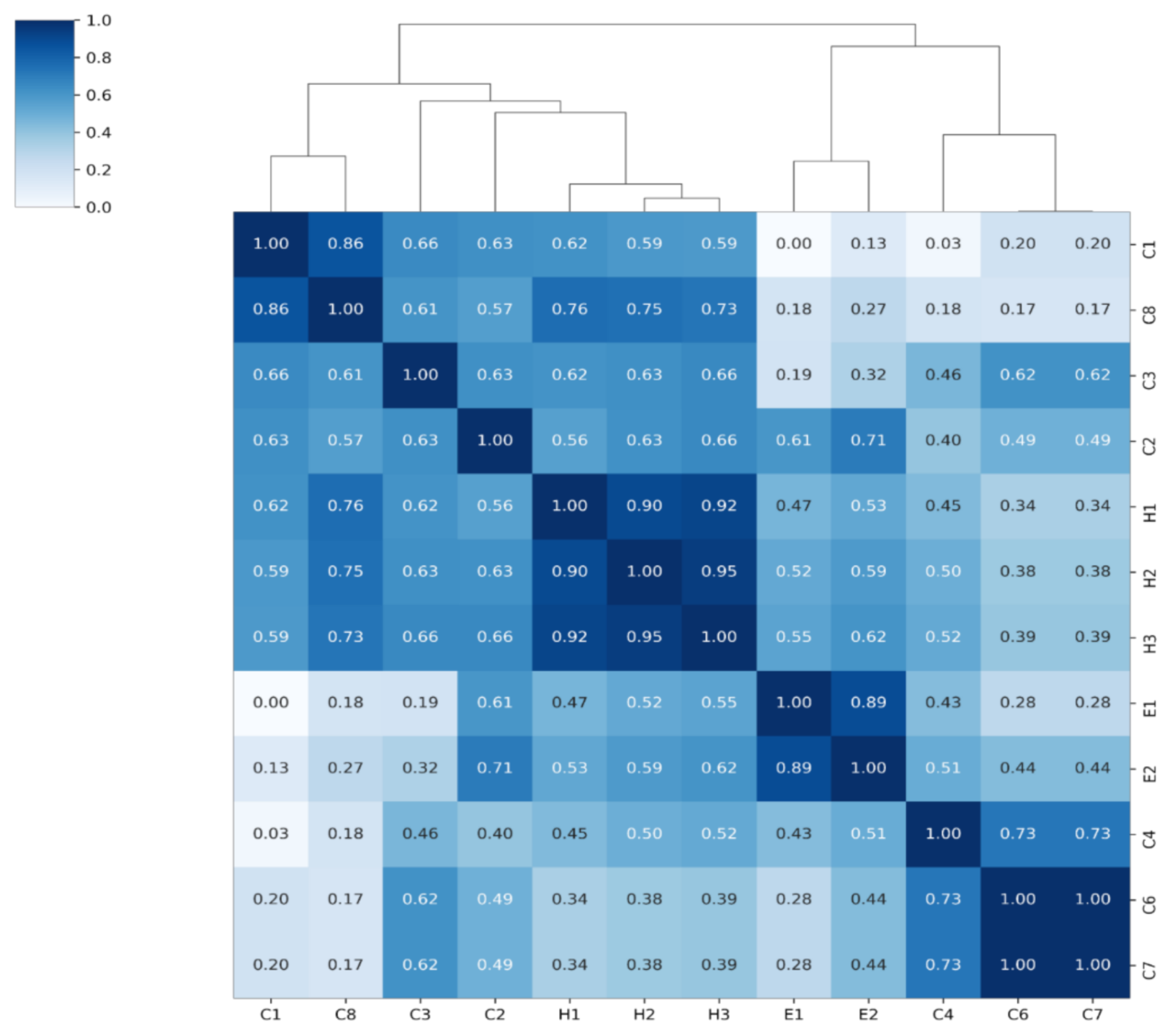
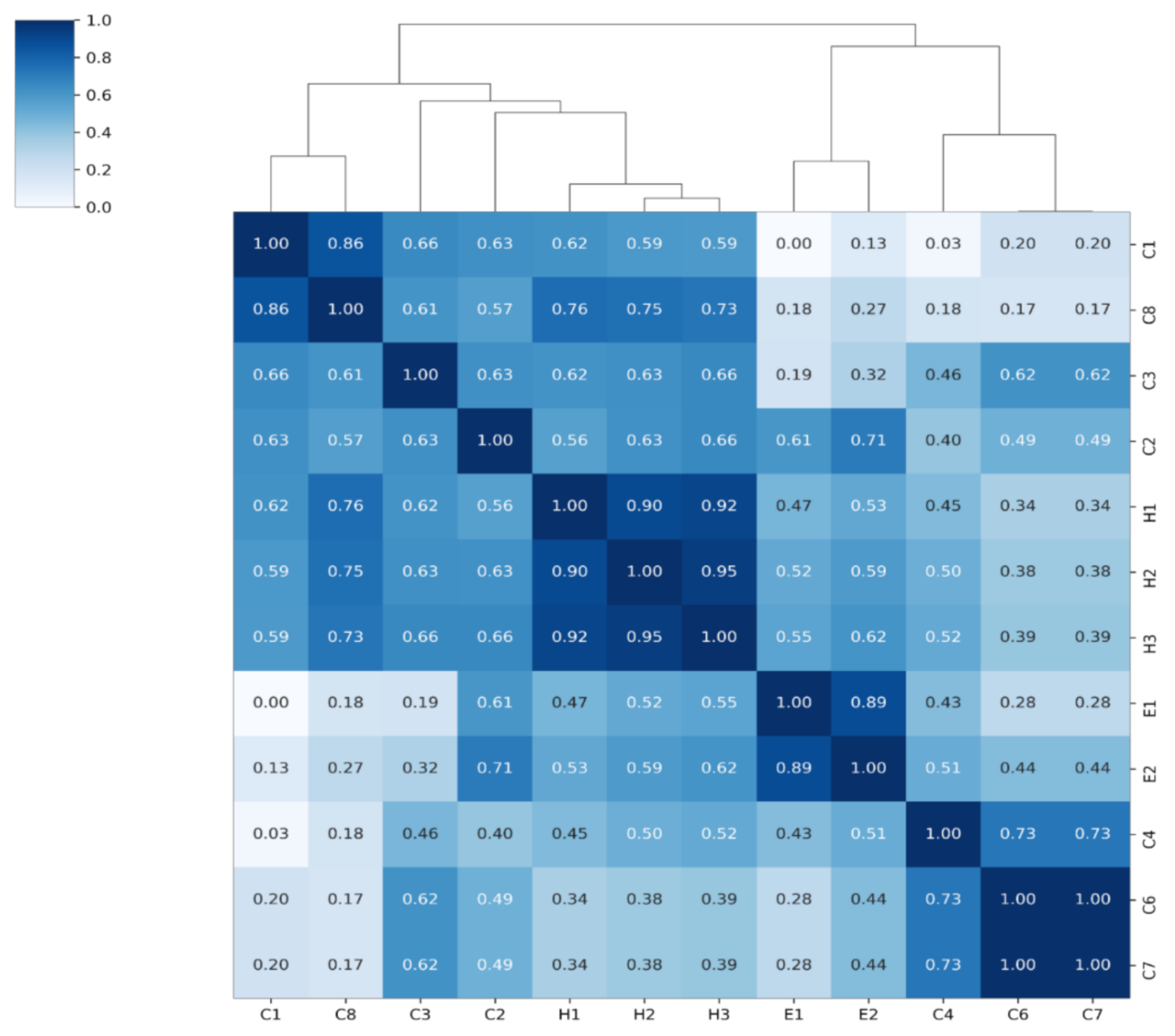
| Index Name | Policies Used in Index from OxCGRT Dataset | Simple Explanation |
|---|---|---|
| Restriction Index (RI) | C4: Restriction on gatherings C6: Stay at home requirements C7: Domestic travel restrictions | Consists of restrictions on meeting, restrictions on going out and domestic travel. The average value of policies related to the movement and contact of people. |
| Closing Index (CI) | C1: School closing C2: Workplace closing C3: Cancel public events C8: International travel controls | Consists of suspension of school, telecommuting, cancellation of public events and travel regulations abroad. The average value of a variable that regulates the gathering of many public events, companies, etc. |
| Economic Index (EI) | E1: Income support E2: Debt/contract relief | The average value of the government’s financial support policy indices. |
| Health Index (HI) | H1: Public information campaign H2: Testing policy H3: Contact tracing | The average value of the government’s health care policy indices. |
| Levels | Idea | Level Description |
|---|---|---|
| 1.0 | Distancing in life | Mandatory quarantine rules for high-risk activities and facilities |
| 1.5 | Workplace closing | Epidemic region: Strengthen quarantine measures, such as limiting the number of multi-use facilities, in order to block the trend through dangerous facilities and activities Other region: Maintain the first stage, but take self-governing measures according to the quarantine situation, such as the possibility of radio waves. |
| 2.0 | Cancel public events | Epidemic region: Prohibit gatherings and events of more than 100 people, bans gatherings of entertainment facilities, allows only packaging and delivery of restaurants after 21:00, expands restrictions on the use of facilities, and mandates the wearing of indoor masks. Other region: The principle of implementing the key measures in step 1.5, and autonomous measures by local governments according to the quarantine situation. |
| 2.5 | Restriction on gathering | Ban gatherings and events of more than 50 people nationwide, banning gatherings such as singing practice sites, suspending major multi-use facilities after 21:00. |
| 3.0 | Closing public transport | Banning gatherings and events of more than 10 people nationwide, and discontinuing the operation of all multi-use facilities other than essential facilities; |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Stringency Index | Korean Government Index |
|---|---|---|---|---|---|---|
| No lagging | 0.0688 | 0.0118 | 0.0354 | −0.0247 | 0.0623 | 0.0137 |
| 1 | 0.0609 | 0.0115 | 0.0356 | 0.0294 | 0.0558 | 0.0100 |
| 2 | 0.0605 | 0.0124 | 0.0368 | 0.0284 | 0.0579 | 0.0084 |
| 3 | 0.0501 | 0.0152 | 0.0332 | 0.0524 | 0.0587 | 0.0058 |
| 4 | 0.0393 | 0.0174 | 0.0327 | 0.1177 | 0.0583 | 0.0033 |
| 5 | 0.0328 | 0.0156 | 0.0303 | −0.0550 | 0.0542 | −0.0016 |
| 6 | 0.0197 | 0.0145 | 0.0262 | −0.1056 | 0.0457 | −0.0055 |
| 7 | 0.0098 | 0.0148 | 0.0265 | −0.0825 | 0.0414 | −0.0090 |
| 8 | −0.0025 | 0.0133 | 0.0317 | −0.0631 | 0.0317 | −0.0147 |
| 9 | −0.0046 | 0.0122 | 0.0344 | −0.0771 | 0.0266 | −0.0179 |
| 10 | −0.0090 | 0.0100 | 0.0357 | −0.0652 | 0.0192 | −0.0197 |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Korean Government Index |
|---|---|---|---|---|---|
| No lagging | 0.0625 | 0.0086 | 0.0286 | −0.0745 | 0.0159 |
| 1 | 0.0541 | 0.0080 | 0.0292 | −0.0286 | 0.0113 |
| 2 | 0.0532 | 0.0089 | 0.0306 | −0.0620 | 0.0096 |
| 3 | 0.0411 | 0.0131 | 0.0247 | −0.0902 | 0.0080 |
| 4 | 0.0301 | 0.0155 | 0.0225 | −0.0416 | 0.0058 |
| 5 | 0.0268 | 0.0124 | 0.0246 | −0.1015 | −0.0001 |
| 6 | 0.0166 | 0.0110 | 0.0231 | −0.1193 | −0.0043 |
| 7 | 0.0090 | 0.0112 | 0.0237 | −0.0959 | −0.0077 |
| 8 | 0.0022 | 0.0089 | 0.0306 | −0.0818 | −0.0137 |
| 9 | 0.0040 | 0.0075 | 0.0355 | −0.0963 | −0.0175 |
| 10 | 0.0022 | 0.0061 | 0.0367 | −0.0854 | −0.0194 |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Stringency Index | Korean Government Index |
|---|---|---|---|---|---|---|
| No lagging | 0.0576 | 0.0167 | 0.0408 | −0.6493 | 0.0546 | 0.0263 |
| 1 | 0.0552 | 0.0177 | 0.0533 | −0.4707 | 0.0558 | 0.0249 |
| 2 | 0.0573 | 0.0181 | 0.0557 | −0.3280 | 0.0573 | 0.0239 |
| 3 | 0.0573 | 0.0246 | 0.0534 | −0.2244 | 0.0680 | 0.0217 |
| 4 | 0.0462 | 0.0288 | 0.0598 | −0.1469 | 0.0706 | 0.0213 |
| 5 | 0.0408 | 0.0311 | 0.0578 | −0.0641 | 0.0738 | 0.0116 |
| 6 | 0.0243 | 0.0296 | 0.0597 | 0.0072 | 0.0637 | 0.0112 |
| 7 | 0.0136 | 0.0197 | 0.0683 | 0.0629 | 0.0453 | 0.0110 |
| 8 | 0.0063 | 0.0127 | 0.0751 | 0.1137 | 0.0303 | 0.0160 |
| 9 | −0.0109 | 0.0054 | 0.0820 | 0.1091 | 0.0093 | 0.0166 |
| 10 | −0.0188 | −0.0001 | 0.0841 | 0.0844 | −0.0023 | 0.0115 |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Korean Government Index |
|---|---|---|---|---|---|
| No lagging | 0.0297 | 0.0121 | 0.0276 | −0.7129 | 0.0349 |
| 1 | 0.0357 | 0.0072 | 0.0384 | −0.3738 | 0.0299 |
| 2 | 0.0518 | 0.0015 | 0.0381 | −0.0785 | 0.0281 |
| 3 | 0.0483 | 0.0095 | 0.0286 | 0.0481 | 0.0304 |
| 4 | 0.0308 | 0.0183 | 0.0303 | 0.0756 | 0.0307 |
| 5 | 0.0211 | 0.0222 | 0.0288 | 0.1042 | 0.0190 |
| 6 | −0.0007 | 0.0287 | 0.0302 | 0.1185 | 0.0160 |
| 7 | −0.0025 | 0.0186 | 0.0491 | 0.1338 | 0.0130 |
| 8 | −0.0015 | 0.0132 | 0.0572 | 0.1895 | 0.0192 |
| 9 | −0.0194 | 0.0155 | 0.0610 | 0.1610 | 0.0189 |
| 10 | −0.0257 | 0.0132 | 0.0649 | 0.1116 | 0.0133 |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Stringency Index | Korean Government Index |
|---|---|---|---|---|---|---|
| No lagging | 0.0770 | 0.0178 | 0.0404 | −0.1727 | 0.0651 | 0.0188 |
| 1 | 0.0707 | 0.0196 | 0.0510 | −0.1170 | 0.0664 | 0.0174 |
| 2 | 0.0688 | 0.0210 | 0.0561 | −0.0765 | 0.0695 | 0.0179 |
| 3 | 0.0634 | 0.0257 | 0.0568 | −0.0397 | 0.0758 | 0.0174 |
| 4 | 0.0502 | 0.0288 | 0.0630 | −0.0014 | 0.0767 | 0.0170 |
| 5 | 0.0410 | 0.0290 | 0.0637 | 0.0277 | 0.0757 | 0.0114 |
| 6 | 0.0219 | 0.0270 | 0.0657 | 0.0546 | 0.0642 | 0.0092 |
| 7 | 0.0073 | 0.0205 | 0.0722 | 0.0865 | 0.0476 | 0.0069 |
| 8 | −0.0046 | 0.0144 | 0.0793 | 0.1179 | 0.0304 | 0.0062 |
| 9 | −0.0216 | 0.0079 | 0.0851 | 0.1236 | 0.0101 | 0.0044 |
| 10 | −0.0304 | 0.0020 | 0.0878 | 0.1211 | −0.0040 | −0.0001 |
| Lag | Closing Index | Restriction Index | Economic Index | Health Index | Korean Government Index |
|---|---|---|---|---|---|
| No lagging | 0.0654 | 0.0071 | 0.0256 | −0.1015 | 0.0215 |
| 1 | 0.0582 | 0.0069 | 0.0355 | −0.0367 | 0.0183 |
| 2 | 0.0572 | 0.0069 | 0.0390 | 0.0149 | 0.0179 |
| 3 | 0.0483 | 0.0137 | 0.0337 | 0.0521 | 0.0184 |
| 4 | 0.0327 | 0.0194 | 0.0362 | 0.0716 | 0.0186 |
| 5 | 0.0253 | 0.0201 | 0.0392 | 0.0828 | 0.0123 |
| 6 | 0.0058 | 0.0226 | 0.0418 | 0.0774 | 0.0102 |
| 7 | −0.0030 | 0.0182 | 0.0526 | 0.0859 | 0.0073 |
| 8 | −0.0092 | 0.0149 | 0.0601 | 0.1057 | 0.0069 |
| 9 | −0.0239 | 0.0142 | 0.0637 | 0.0891 | 0.0056 |
| 10 | −0.0287 | 0.0115 | 0.0655 | 0.0749 | 0.0020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, G.; Apio, C.; Han, K.; Goo, T.; Chung, H.W.; Kim, T.; Kim, H.; Ko, Y.; Lee, D.; Lim, J.; et al. Statistical Estimation of Effects of Implemented Government Policies on COVID-19 Situation in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 2144. https://doi.org/10.3390/ijerph18042144
Heo G, Apio C, Han K, Goo T, Chung HW, Kim T, Kim H, Ko Y, Lee D, Lim J, et al. Statistical Estimation of Effects of Implemented Government Policies on COVID-19 Situation in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(4):2144. https://doi.org/10.3390/ijerph18042144
Chicago/Turabian StyleHeo, Gyujin, Catherine Apio, Kyulhee Han, Taewan Goo, Hye Won Chung, Taehyun Kim, Hakyong Kim, Yeonghyeon Ko, Doeun Lee, Jisun Lim, and et al. 2021. "Statistical Estimation of Effects of Implemented Government Policies on COVID-19 Situation in South Korea" International Journal of Environmental Research and Public Health 18, no. 4: 2144. https://doi.org/10.3390/ijerph18042144
APA StyleHeo, G., Apio, C., Han, K., Goo, T., Chung, H. W., Kim, T., Kim, H., Ko, Y., Lee, D., Lim, J., & Park, T. (2021). Statistical Estimation of Effects of Implemented Government Policies on COVID-19 Situation in South Korea. International Journal of Environmental Research and Public Health, 18(4), 2144. https://doi.org/10.3390/ijerph18042144