
A Family-Based Lifestyle Intervention Focusing on Fathers and Their Children Using Co-Creation: Study Protocol of the Run Daddy Run Intervention

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Development of the Run Daddy Run Intervention
2.2. The Run Daddy Run Intervention
2.2.1. Content of the Run Daddy Run Intervention
2.2.2. Participants
2.2.3. Sample Size
2.2.4. Recruitment
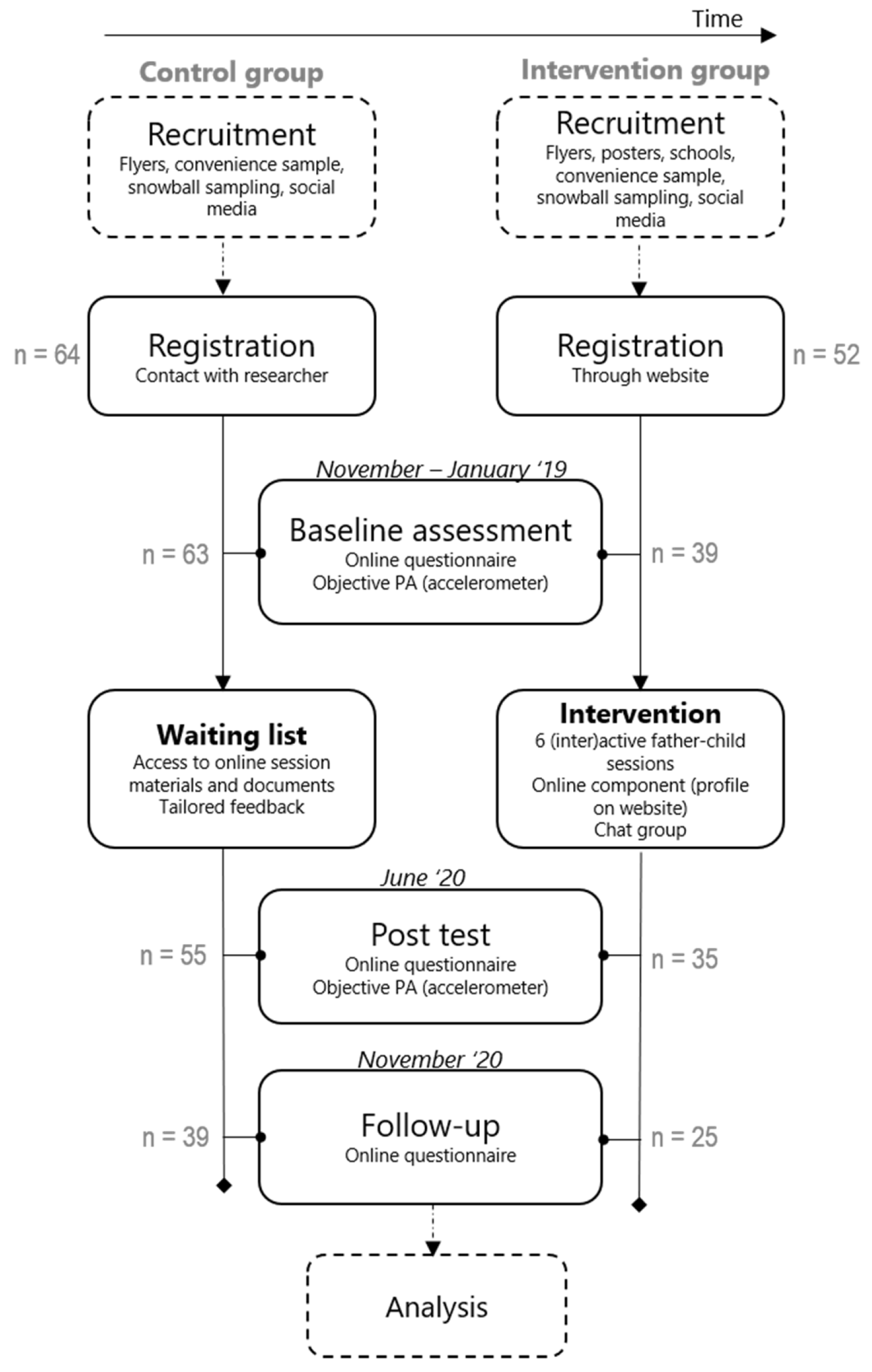
2.2.5. Study Design and Randomization
2.2.6. Procedure
2.2.7. Measurements (Effect Evaluation)
Co-Physical Activity and Co-Screen Time
Physical Activity
Sedentary Behavior
Body Mass Index
Determinants of (co-)PA and (co-)ST
PA Family Context, Quality of the Father-Child Relationship and Parental Practices towards PA
2.2.8. Data Analysis
2.2.9. Data Management
2.2.10. Process Evaluation
2.3. Ethics Approval and Consent to Participate
3. Results: Developed Intervention and Prospected Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Trial Governance
Trial Registration Number
Abbreviations
| PA | Physical activity |
| SB | Sedentary behavior |
| BMI | Body mass index |
| Co-PA | Co-physical activity |
| IG | Intervention group |
| CG | Control group |
References
- Verloigne, M.; Van Lippevelde, W.; Maes, L.; Yildirim, M.; Chinapaw, M.; Manios, Y.; Androutsos, O.; Kovacs, E.; Bringolf-Isler, B.; Brug, J.; et al. Levels of physical activity and sedentary time among 10-to 12-year-old boys and girls across 5 European countries using accelerometers: An observational study within the ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef]
- Maher, C.; Olds, T.S.; Eisenmann, J.C.; Dollman, J. Screen time is more strongly associated than physical activity with overweight and obesity in 9- to 16-year-old Australians. Acta Paediatr. 2012, 101, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Van Sluijs, E.M.; McMinn, A.M.; Griffin, S.J. Effectiveness of interventions to promote physical activity in children and adolescents: Systematic review of controlled trials. BMJ 2007, 335, 703. [Google Scholar] [CrossRef] [PubMed]
- Golan, M. Parents as agents of change in childhood obesity–from research to practice. Int. J. Pediatric Obes. 2006, 1, 66–76. [Google Scholar] [CrossRef]
- Sterdt, E.; Liersch, S.; Walter, U. Correlates of physical activity of children and adolescents: A systematic review of reviews. Health Educ. J. 2014, 73, 72–89. [Google Scholar] [CrossRef]
- González-García, H.; Pelegrín, A.; Carballo, J. Parental Educational Styles as a Predictor of Sport Success and Sports Competition Level. Rev. Int. Med. Cienc. Act. Física Deporte 2018, 18, 589–604. [Google Scholar]
- Golan, M.; Crow, S. Targeting parents exclusively in the treatment of childhood obesity: Long-term results. Obes. Res. 2004, 12, 357–361. [Google Scholar] [CrossRef]
- Golan, M.; Weizman, A. Familial approach to the treatment of childhood obesity: Conceptual model. J. Nutr. Educ. 2001, 33, 102–107. [Google Scholar] [CrossRef]
- Määttä, S.; Ray, C.; Roos, E. Associations of parental influence and 10–11-year-old children’s physical activity: Are they mediated by children’s perceived competence and attraction to physical activity? Scand. J. Public Health 2014, 42, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Lubans, D.R.; Callister, R.; Okely, A.D.; Burrows, T.L.; Fletcher, R.; Collins, C.E. The ‘Healthy Dads, Healthy Kids’ randomized controlled trial: Efficacy of a healthy lifestyle program for overweight fathers and their children. Int. J. Obes. 2011, 35, 436–447. [Google Scholar] [CrossRef]
- Latomme, J.; Van Stappen, V.; Cardon, G.; Morgan, P.; Lateva, M.; Chakarova, N.; Kivelä, J.; Lindström, J.; Androutsos, O.; González-Gil, E. The Association between Children’s and Parents’ Co-TV Viewing and Their Total Screen Time in Six European Countries: Cross-Sectional Data from the Feel4diabetes-Study. Int. J. Environ. Res. Public Health 2018, 15, 2599. [Google Scholar] [CrossRef]
- Freeman, E.; Fletcher, R.; Collins, C.E.; Morgan, P.J.; Burrows, T.; Callister, R. Preventing and treating childhood obesity: Time to target fathers. Int. J. Obes. 2012, 36, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Sebire, S.J.; Wood, L.; Pool, L.; Zahra, J.; Thompson, J.L.; Lawlor, D.A. Associations between objectively assessed child and parental physical activity: A cross-sectional study of families with 5–6 year old children. BMC Public Health 2014, 14, 655. [Google Scholar] [CrossRef]
- Ferreira, I.; van der Horst, K.; Wendel-Vos, W.; Kremers, S.; van Lenthe, F.J.; Brug, J. Environmental correlates of physical activity in youth—A review and update. Obes Rev 2007, 8, 129–154. [Google Scholar] [CrossRef] [PubMed]
- Fuemmeler, B.F.; Anderson, C.B.; Masse, L.C. Parent-child relationship of directly measured physical activity. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 17. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D. The influence of fathers on children’s physical activity and dietary behaviors: Insights, recommendations and future directions. Curr. Obes. Rep. 2017, 6, 324–333. [Google Scholar] [CrossRef]
- Latomme, J.; Huys, N.; Cardon, G.; Morgan, P.J.; Lateva, M.; Chakarova, N.; Kivelä, J.; Lindström, J.; Androutsos, O.; González-Gil, E.M. Do physical activity and screen time mediate the association between European fathers’ and their children’s weight status? Cross-sectional data from the Feel4Diabetes-study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Craig, L. Do Australians share parenting? Time-diary evidence on fathers’ and mothers’ time with children. In Proceedings of the Australian Institute of Family Studies 8th Annual Conference, Melbourne, Austrilia, 12–14 February 2003. [Google Scholar]
- Laflamme, D.; Pomerleau, A.; Malcuit, G. A comparison of fathers’ and mothers’ involvement in childcare and stimulation behaviors during free-play with their infants at 9 and 15 months. Sex Roles 2002, 47, 507–518. [Google Scholar] [CrossRef]
- Fletcher, R.; May, C.; St George, J.; Morgan, P.J.; Lubans, D.R. Fathers’ perceptions of rough-and-tumble play: Implications for early childhood services. Australas. J. Early Child. 2011, 36, 131. [Google Scholar] [CrossRef]
- Paquette, D. Theorizing the father-child relationship: Mechanisms and developmental outcomes. Hum. Dev. 2004, 47, 193–219. [Google Scholar] [CrossRef]
- Lindsey, E.W.; Cremeens, P.R.; Caldera, Y.M. Mother–child and father–child mutuality in two contexts: Consequences for young children’s peer relationships. Infant Child Dev. Int. J. Res. Pract. 2010, 19, 142–160. [Google Scholar] [CrossRef]
- Morgan, P.J.; Young, M.D.; Lloyd, A.B.; Wang, M.L.; Eather, N.; Miller, A.; Murtagh, E.M.; Barnes, A.T.; Pagoto, S.L. Involvement of Fathers in Pediatric Obesity Treatment and Prevention Trials: A Systematic Review. Pediatrics 2017, 139, e20162635. [Google Scholar] [CrossRef] [PubMed]
- McLean, N.; Griffin, S.; Toney, K.; Hardeman, W. Family involvement in weight control, weight maintenance and weight-loss interventions: A systematic review of randomised trials. Int. J. Obes. 2003, 27, 987–1005. [Google Scholar] [CrossRef]
- Lloyd, A.B.; Lubans, D.R.; Plotnikoff, R.C.; Collins, C.E.; Morgan, P.J. Maternal and paternal parenting practices and their influence on children’s adiposity, screen-time, diet and physical activity. Appetite 2014, 79, 149–157. [Google Scholar] [CrossRef]
- Davison, K.K.; Cutting, T.M.; Birch, L.L. Parents’ activity-related parenting practices predict girls’ physical activity. Med. Sci. Sports Exerc. 2003, 35, 1589. [Google Scholar]
- Edwardson, C.L.; Gorely, T. Activity-related parenting practices and children’s objectively measured physical activity. Pediatr. Exerc. Sci. 2010, 22, 105–113. [Google Scholar] [CrossRef]
- Morgan, P.J.; Collins, C.E.; Plotnikoff, R.C.; Callister, R.; Burrows, T.; Fletcher, R.; Okely, A.D.; Young, M.D.; Miller, A.; Lloyd, A.B. The ‘Healthy Dads, Healthy Kids’ community randomized controlled trial: A community-based healthy lifestyle program for fathers and their children. Prev. Med. 2014, 61, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Young, M.D.; Barnes, A.T.; Eather, N.; Pollock, E.R.; Lubans, D.R. Engaging fathers to increase physical activity in girls: The “dads and daughters exercising and empowered”(DADEE) randomized controlled trial. Ann. Behav. Med. 2019, 53, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Young, M.D.; Lubans, D.R.; Barnes, A.T.; Eather, N.; Pollock, E.R.; Morgan, P.J. Impact of a father–daughter physical activity program on girls’ social–emotional well-being: A randomized controlled trial. J. Consult. Clin. Psychol. 2019, 87, 294. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690. [Google Scholar] [CrossRef]
- Sniehotta, F.F. Towards a theory of intentional behaviour change: Plans, planning, and self-regulation. Br. J. Health Psychol. 2009, 14, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Forsetlund, L.; Bradley, P.; Forsen, L.; Nordheim, L.; Jamtvedt, G.; Bjørndal, A. Randomised controlled trial of a theoretically grounded tailored intervention to diffuse evidence-based public health practice [ISRCTN23257060]. BMC Med Educ. 2003, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Gourlan, M.; Bernard, P.; Bortolon, C.; Romain, A.; Lareyre, O.; Carayol, M.; Ninot, G.; Boiché, J. Efficacy of theory-based interventions to promote physical activity. A meta-analysis of randomised controlled trials. Health Psychol. Rev. 2016, 10, 50–66. [Google Scholar] [CrossRef]
- Tully, L.A.; Piotrowska, P.J.; Collins, D.A.; Mairet, K.S.; Black, N.; Kimonis, E.R.; Hawes, D.J.; Moul, C.; Lenroot, R.K.; Frick, P.J. Optimising child outcomes from parenting interventions: fathers’ experiences, preferences and barriers to participation. BMC Public Health 2017, 17, 550. [Google Scholar] [CrossRef]
- Budd, K.S.; O’Brien, T.P. Father involvement in behavioral parent training: An area in need of research. Behav. Ther. 1982, 5, 85–89. [Google Scholar]
- Strand, S.; Lindsay, G.; Cullen, M.A.; Cullen, S.; Band, S.; Davis, H.; Conlon, G.; Barlow, J.; Evans, R. Parenting Early Intervention Programme evaluation-DFE-RR121A. University of Oxford: Oxford, UK, 2011. [Google Scholar]
- Pollock, E.R.; Young, M.D.; Lubans, D.R.; Barnes, A.T.; Eather, N.; Coffey, J.E.; Hansen, V.; Morgan, P.J. Impact of a Father–Daughter Physical Activity Intervention: An Exploration of Fathers’ Experiences. J. Child Fam. Stud. 2020, 29, 3609–3620. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Jackson, C.; Shaw, S.; Janamian, T. Achieving research impact through co-creation in community-based health services: Literature review and case study. Milbank Q. 2016, 94, 392–429. [Google Scholar] [CrossRef] [PubMed]
- Zwass, V. Co-creation: Toward a taxonomy and an integrated research perspective. Int. J. Electron. Commer. 2010, 15, 11–48. [Google Scholar] [CrossRef]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.; De Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F. Framework, principles and recommendations for utilising participatory methodologies in the co-creation and evaluation of public health interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef]
- Sanders, E.B.-N.; Stappers, P.J. Co-creation and the new landscapes of design. Co-Design 2008, 4, 5–18. [Google Scholar] [CrossRef]
- Verloigne, M.; Altenburg, T.M.; Chinapaw, M.J.M.; Chastin, S.; Cardon, G.; De Bourdeaudhuij, I. Using a co-creational approach to develop, implement and evaluate an intervention to promote physical activity in adolescent girls from vocational and technical schools: A case control study. Int. J. Environ. Res. Public Health 2017, 14, 862. [Google Scholar] [CrossRef]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of community-based research: Assessing partnership approaches to improve public health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Internal Med. 2013, 158, 200–207. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions. 2014; Silverback Publishing: Sutton, UK, 2015. [Google Scholar]
- Les MacLeod EdD, M. Making SMART goals smarter. Phys. Exec. 2012, 38, 68. [Google Scholar]
- Vervloet, M.; Linn, A.J.; van Weert, J.C.; De Bakker, D.H.; Bouvy, M.L.; Van Dijk, L. The effectiveness of interventions using electronic reminders to improve adherence to chronic medication: A systematic review of the literature. J. Am. Med. Inform. Assoc. 2012, 19, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Spittaels, H.; De Bourdeaudhuij, I.; Vandelanotte, C. Evaluation of a website-delivered computer-tailored intervention for increasing physical activity in the general population. Prev. Med. 2007, 44, 209–217. [Google Scholar] [CrossRef]
- Eysenbach, G. The law of attrition. J. Med Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A general power analysis program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Bayley, J.; Wallace, L.M.; Choudhry, K. Fathers and parenting programmes: Barriers and best practice. Community Pract. 2009, 82, 28–31. [Google Scholar]
- Elliott, S.A.; Baxter, K.A.; Davies, P.S.; Truby, H. Accuracy of self-reported physical activity levels in obese adolescents. J. Nutr. Metab. 2014, 2014. [Google Scholar] [CrossRef]
- Matthews, C.; Welk, G. Use of self-report instruments to assess physical activity. Phys. Act. Assess. Health-Relat. Res. 2002, 107, 123. [Google Scholar]
- Feng, Y.; Wong, C.K.; Janeja, V.; Kuber, R.; Mentis, H.M. Comparison of tri-axial accelerometers step-count accuracy in slow walking conditions. Gait Posture 2017, 53, 11–16. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. 2011, 8, 115. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Rahman, M.M.; Liang, C.Y.; Gu, D.; Ding, Y.; Akter, M. Understanding Levels and Motivation of Physical Activity for Health Promotion among Chinese Middle-Aged and Older Adults: A Cross-Sectional Investigation. J. Healthc. Eng. 2019, 2019, 9828241. [Google Scholar] [CrossRef] [PubMed]
- Heesch, K.C.; Hill, R.L.; Aguilar-Farias, N.; Van Uffelen, J.G.; Pavey, T. Validity of objective methods for measuring sedentary behaviour in older adults: A systematic review. Int. J. Behav. Nutr. Phys. 2018, 15, 119. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.I.; Roldán-Jiménez, C.; Martín-Martín, J.; González-Sánchez, M.; Gutiérrez Sánchez, D. Cross-Cultural Adaptation and Psychometric Testing of the International Sedentary Assessment Tool for the Spanish Population. Int. J. Environ. Res. Public Health 2020, 17, 758. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Owen, N.; Bauman, A.E.; Sallis, J.F.; Brown, W. Correlates of adults’ participation in physical activity: Review and update. Med. Sci. Sports Exerc. 2002, 34, 1996–2001. [Google Scholar] [CrossRef]
- Van Der Horst, K.; Paw, M.J.; Twisk, J.W.; Van, W.M. A brief review on correlates of physical activity and sedentariness in youth. Med. Sci. Sports Exerc. 2007, 39, 1241–1250. [Google Scholar] [CrossRef]
- Lloyd, A.B.; Lubans, D.R.; Plotnikoff, R.C.; Morgan, P.J. Paternal Lifestyle-Related Parenting Practices Mediate Changes in Children’s Dietary and Physical Activity Behaviors: Findings From the Healthy Dads, Healthy Kids Community Randomized Controlled Trial. J. Phys. Act. Health 2015, 12, 1327–1335. [Google Scholar] [CrossRef]
- Lee, S.M.; Nihiser, A.; Strouse, D.; Das, B.; Michael, S.; Huhman, M. Correlates of children and parents being physically active together. J. Phys. Act. Health 2010, 7, 776–783. [Google Scholar] [CrossRef][Green Version]
- Lloyd, A.; Lubans, D.; Plotnikoff, R.; Morgan, P. Impact of the ‘Healthy Dads, Healthy Kids’ lifestyle programme on the activity- and diet-related parenting practices of fathers and mothers. Pediatr. Obes. 2014, 9, e149–e155. [Google Scholar] [CrossRef]
- Niermann, C.; Krapf, F.; Renner, B.; Reiner, M.; Woll, A. Family health climate scale (FHC-scale): Development and validation. Int. J. Behav. Nutr. Phys. 2014, 11, 30. [Google Scholar] [CrossRef]
- Doyle, O.; Pecukonis, E.; Harrington, D. The nurturant fathering scale: A confirmatory factor analysis with an African American sample of college students. Res. Soc. Work Pract. 2011, 21, 319–327. [Google Scholar] [CrossRef]
- Finley, G.E.; Schwartz, S.J. The father involvement and nurturant fathering scales: Retrospective measures for adolescent and adult children. Educ. Psychol. Meas. 2004, 64, 143–164. [Google Scholar] [CrossRef]
- Finleyr, G. Father contact and perceived affective quality of fathering 1n trinidad. Rev. Lnternmericana Psicol./Interam. J. Psychol. 1997, 31, 315–319. [Google Scholar]
- Schwartz, S.J.; Finley, G.E. Father involvement, nurturant fathering, and young adult psychosocial functioning: Differences among adoptive, adoptive stepfather, and nonadoptive stepfamilies. J. Fam. Issues 2006, 27, 712–731. [Google Scholar] [CrossRef]
- Sallis, J.F.; Taylor, W.C.; Dowda, M.; Freedson, P.S.; Pate, R.R. Correlates of vigorous physical activity for children in grades 1 through 12: Comparing parent-reported and objectively measured physical activity. Pediatr. Exerc. Sci. 2002, 14, 30–44. [Google Scholar] [CrossRef]
- Taylor, W.C.; Sallis, J.F.; Dowda, M.; Freedson, P.S.; Eason, K.; Pate, R.R. Activity patterns and correlates among youth: Differences by weight status. Pediatr. Exerc. Sci. 2002, 14, 418–431. [Google Scholar] [CrossRef]
- Gattshall, M.L.; Shoup, J.A.; Marshall, J.A.; Crane, L.A.; Estabrooks, P.A. Validation of a survey instrument to assess home environments for physical activity and healthy eating in overweight children. Int. J. Behav. Nutr. Phys. 2008, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; de Vries, S.I.; Goldbohm, R.A.; Dagnelie, P.C.; de Vries, N.K.; van Buuren, S.; Thijs, C. Association between parenting practices and children’s dietary intake, activity behavior and development of body mass index: The KOALA Birth Cohort Study. Int. J. Behav. Nutr. Phys. 2011, 8, 18. [Google Scholar] [CrossRef]
- Timperio, A.; Salmon, J.; Ball, K.; Baur, L.A.; Telford, A.; Jackson, M.; Salmon, L.; Crawford, D. Family physical activity and sedentary environments and weight change in children. Int. J. Pediatr. Obes. 2008, 3, 160–167. [Google Scholar] [CrossRef]
- IBM. IBM SPSS Statistics for Windows (Version 26.0) [Computer Software]; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef]
- Saunders, R.P.; Evans, M.H.; Joshi, P. Developing a process-evaluation plan for assessing health promotion program implementation: A how-to guide. Health Promot. Pract. 2005, 6, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Schuler, D.; Namioka, A. Participatory Design: Principles and Practices; CRC Press: Boca Raton, FL, USA, 1993. [Google Scholar]
- Eng, T.R. The eHealth Landscape: A Terrain Map of Emerging Information and Communication Technologies in Health and Health Care; The Robert Wood Johnson Foundation: Princeton, NJ, USA, 2001. [Google Scholar]
- Free, C.; Phillips, G.; Watson, L.; Galli, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef]
- Wantland, D.J.; Portillo, C.J.; Holzemer, W.L.; Slaughter, R.; McGhee, E.M. The effectiveness of Web-based vs. non-Web-based interventions: A meta-analysis of behavioral change outcomes. J. Med. Internet Res. 2004, 6, e40. [Google Scholar] [CrossRef]
- Pedersen, S.J.; Cooley, P.D.; Mainsbridge, C. An e-health intervention designed to increase workday energy expenditure by reducing prolonged occupational sitting habits. Work 2014, 49, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Webb, T.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010, 12, e4. [Google Scholar] [CrossRef] [PubMed]
- Ritterband, L.M.; Thorndike, F.P.; Cox, D.J.; Kovatchev, B.P.; Gonder-Frederick, L.A. A behavior change model for internet interventions. Ann. Behav. Med. 2009, 38, 18–27. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Müller, A.M.; Short, C.E.; Hingle, M.; Nathan, N.; Williams, S.L.; Lopez, M.L.; Parekh, S.; Maher, C.A. Past, present, and future of eHealth and mHealth research to improve physical activity and dietary behaviors. J. Nutr. Educ. Behav. 2016, 48, 219–228.e211. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Saelens, B.E. Assessment of physical activity by self-report: Status, limitations, and future directions. Res. Q. Exerc. Sport 2000, 71 (Suppl. S2), 1–14. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Behavior Change Wheel | Researcher | Co-Creation Part (Researcher and Fathers) |
|---|---|---|
| Stage 1: understanding the problem describing intervention goals | ||
| Step 1 Identifying the (health) problem, selecting and specifying target behavior |
| / |
| Step 2 Understanding the problem and identifying what needs to change |
| Co-creation session 1 |
| ||
| Step 3 Defining the intervention goals |
| Co-creation session 2 |
| ||
| Step 4 Selecting COM-B and TDF |
| / |
| Stage 2: translate findings into intervention | ||
| Step 5 Selecting intervention functions |
| / |
| Step 6 and 7 Selecting BCTs and practical strategies |
| Co-creation session 3 |
| ||
| Step 8 Integration |
| Co-creation session 4 |
| ||
| Stage 3: refining and pre-testing | ||
| Step 9 Refining |
| Co-creation interviews (Group B) |
| ||
| Step 10 Pre-testing—pilot study | (out of the scope of this article) | |
| Co-Creation Group A | Co-Creation Group B | |
|---|---|---|
| Number of participants (n) | 5 | 5 |
| Region | West-Flanders, Belgium | East-Flanders, Belgium |
| Age, in years (range) | 36–50 | 31–47 |
| BMI, kg/m² (range) | 21.6–24.6 | 22.5–32.15 |
| Education | ||
| 0 | 1 |
| 0 | 1 |
| 2 | 1 |
| 3 | 2 |
| Number of children in the family (range) | 2–3 | 2–3 |
| Age range (yrs.) of all children in the household | 7–12 | 4–14 |
| Intervention Goals |
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Session Number | Theme | |
|---|---|---|
| Informative Part Theme Based on Identified Barriers for Co-PA According to Fathers | Active Part Theme Based on 2 to 4 FMS | |
| 1 | General introduction, importance of (co-)PA and role of the father | Jumping, landing, running and coordination |
| 2 | Motivation for (co-)PA | Throwing, kicking, catching and rolling |
| 3 | Co-PA preferences and common co-PA interests | Rotating, rolling, pulling and pushing |
| 4 | Social support | Dribbling and striking |
| 5 | Screen time | Carrying, wheedling, crawling and lifting |
| 6 | Co-PA as a habit, rehearsal and summary | All FMS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Latomme, J.; Morgan, P.J.; De Craemer, M.; Brondeel, R.; Verloigne, M.; Cardon, G. A Family-Based Lifestyle Intervention Focusing on Fathers and Their Children Using Co-Creation: Study Protocol of the Run Daddy Run Intervention. Int. J. Environ. Res. Public Health 2021, 18, 1830. https://doi.org/10.3390/ijerph18041830
Latomme J, Morgan PJ, De Craemer M, Brondeel R, Verloigne M, Cardon G. A Family-Based Lifestyle Intervention Focusing on Fathers and Their Children Using Co-Creation: Study Protocol of the Run Daddy Run Intervention. International Journal of Environmental Research and Public Health. 2021; 18(4):1830. https://doi.org/10.3390/ijerph18041830
Chicago/Turabian StyleLatomme, Julie, Philip J. Morgan, Marieke De Craemer, Ruben Brondeel, Maïté Verloigne, and Greet Cardon. 2021. "A Family-Based Lifestyle Intervention Focusing on Fathers and Their Children Using Co-Creation: Study Protocol of the Run Daddy Run Intervention" International Journal of Environmental Research and Public Health 18, no. 4: 1830. https://doi.org/10.3390/ijerph18041830
APA StyleLatomme, J., Morgan, P. J., De Craemer, M., Brondeel, R., Verloigne, M., & Cardon, G. (2021). A Family-Based Lifestyle Intervention Focusing on Fathers and Their Children Using Co-Creation: Study Protocol of the Run Daddy Run Intervention. International Journal of Environmental Research and Public Health, 18(4), 1830. https://doi.org/10.3390/ijerph18041830