
Sex Difference in the Association between Electronic Cigarette Use and Subsequent Cigarette Smoking among U.S. Adolescents: Findings from the PATH Study Waves 1–4



Abstract
1. Introduction
2. Materials and Methods
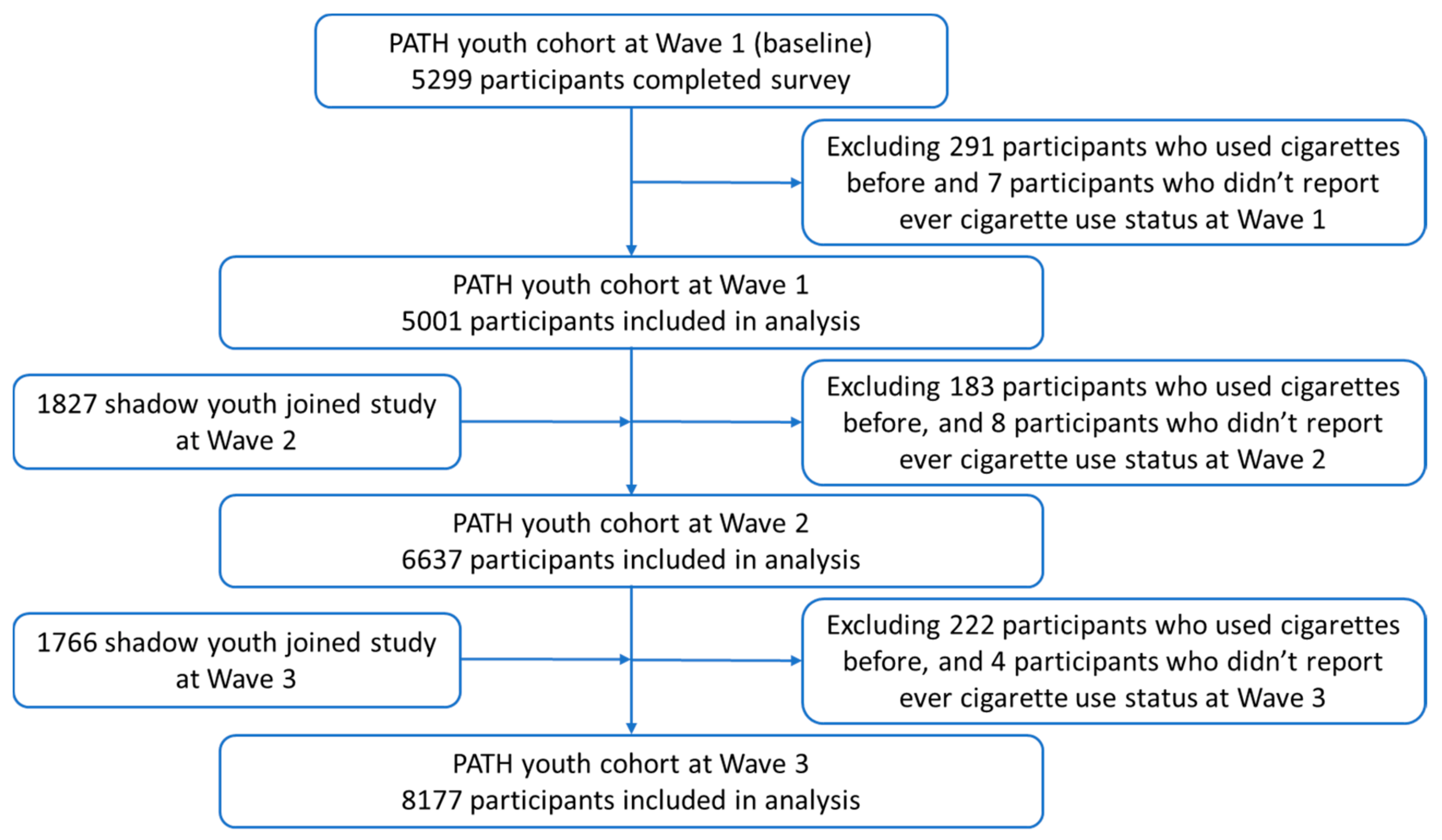
2.1. Study Sample and Design
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sample and Demographic Characteristics
3.2. Past-30-Day Cigarette Smoking at 12-Month Follow-up Waves
3.3. Multivariate Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2014.
- Johnston, L.D.; Miech, R.A.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Patrick, M.E. Monitoring the Future National Survey Results on Drug Use, 1975–2018: Overview, Key Findings on Adolescent Drug Use; University of Michigan, Institute for Social Research (ISR): Ann Arbor, MI, USA, 2019. [Google Scholar]
- National Institute on Drug Abuse. Study: Surge of Teen Vaping Levels off, but Remains High as of Early 2020. Available online: https://www.drugabuse.gov/news-events/news-releases/2020/12/study-surge-of-teen-vaping-levels-off-but-remains-high-as-of-early-2020 (accessed on 27 January 2021).
- U.S. Department of Health and Human Services. E-Cigarette Use among Youth and Young Adults: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2016.
- Khouja, J.N.; Suddell, S.F.; Peters, S.E.; Taylor, A.E.; Munafò, M.R. Is e-cigarette use in non-smoking young adults associated with later smoking? A systematic review and meta-analysis. Tob. Control 2020. [Google Scholar] [CrossRef]
- Huang, J.; Duan, Z.; Kwok, J.; Binns, S.; Vera, L.E.; Kim, Y.; Szczypka, G.; Emery, S.L. Vaping versus JUULing: How the extraordinary growth and marketing of JUUL transformed the US retail e-cigarette market. Tob. Control 2019, 28, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.W.; Neff, L.J.; Park-Lee, E.; Ren, C.; Cullen, K.A.; King, B.A. E-cigarette use among middle and high school students—United States, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1310. [Google Scholar] [CrossRef] [PubMed]
- Soneji, S.; Barrington-Trimis, J.L.; Wills, T.A.; Leventhal, A.M.; Unger, J.B.; Gibson, L.A.; Yang, J.; Primack, B.A.; Andrews, J.A.; Miech, R.A. Association between initial use of e-cigarettes and subsequent cigarette smoking among adolescents and young adults: A systematic review and meta-analysis. JAMA Pediatr. 2017, 171, 788–797. [Google Scholar] [CrossRef]
- Leventhal, A.M.; Strong, D.R.; Kirkpatrick, M.G.; Unger, J.B.; Sussman, S.; Riggs, N.R.; Stone, M.D.; Khoddam, R.; Samet, J.M.; Audrain-McGovern, J. Association of electronic cigarette use with initiation of combustible tobacco product smoking in early adolescence. JAMA 2015, 314, 700–707. [Google Scholar] [CrossRef]
- Primack, B.A.; Soneji, S.; Stoolmiller, M.; Fine, M.J.; Sargent, J.D. Progression to traditional cigarette smoking after electronic cigarette use among US adolescents and young adults. JAMA Pediatr. 2015, 169, 1018–1023. [Google Scholar] [CrossRef]
- Amos, A.; Greaves, L.; Nichter, M.; Bloch, M. Women and tobacco: A call for including gender in tobacco control research, policy and practice. Tob. Control 2012, 21, 236–243. [Google Scholar] [CrossRef]
- Solomon, A. Gender, women, and the future of tobacco control. Drugs Alcohol Today 2020. [Google Scholar] [CrossRef]
- Regitz-Zagrosek, V. Sex and gender differences in health: Science & Society Series on Sex and Science. EMBO Rep. 2012, 13, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Pogun, S.; Yararbas, G. Sex differences in nicotine action. Nicotine Psychopharmacol. 2009, 261–291. [Google Scholar]
- Schmidt, H.D.; Rupprecht, L.E.; Addy, N.A. Neurobiological and neurophysiological mechanisms underlying nicotine seeking and smoking relapse. Mol. Neuropsychiatry 2018, 4, 169–189. [Google Scholar] [CrossRef] [PubMed]
- Benowitz, N.L.; Lessov-Schlaggar, C.N.; Swan, G.E.; Jacob, P., III. Female sex and oral contraceptive use accelerate nicotine metabolism. Clin. Pharmacol. Ther. 2006, 79, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, K.P.; Wang, S.; Kim, S.-J.; McGovern, E.; Nabulsi, N.; Gao, H.; Labaree, D.; Tagare, H.D.; Sullivan, J.M.; Morris, E.D. Sex differences in the brain’s dopamine signature of cigarette smoking. J. Neurosci. 2014, 34, 16851–16855. [Google Scholar] [CrossRef]
- Jacobs, W.; Goodson, P.; Barry, A.E.; McLeroy, K.R. The role of gender in adolescents’ social networks and alcohol, tobacco, and drug use: A systematic review. J. Sch. Health 2016, 86, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Waldron, I. Patterns and causes of gender differences in smoking. Soc. Sci. Med. 1991, 32, 989–1005. [Google Scholar] [CrossRef]
- Piper, M.E.; Cook, J.W.; Schlam, T.R.; Jorenby, D.E.; Smith, S.S.; Bolt, D.M.; Loh, W.-Y. Gender, race, and education differences in abstinence rates among participants in two randomized smoking cessation trials. Nicotine Tob. Res. 2010, 12, 647–657. [Google Scholar] [CrossRef]
- Riehm, K.E.; Young, A.S.; Feder, K.A.; Krawczyk, N.; Tormohlen, K.N.; Pacek, L.R.; Mojtabai, R.; Crum, R.M. Mental health problems and initiation of e-cigarette and combustible cigarette use. Pediatrics 2019, 144. [Google Scholar] [CrossRef]
- Upadhyaya, H.P.; Deas, D.; Brady, K.T.; Kruesi, M. Cigarette smoking and psychiatric comorbidity in children and adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 1294–1305. [Google Scholar] [CrossRef]
- Audrain-McGovern, J.; Rodriguez, D.; Kassel, J.D. Adolescent smoking and depression: Evidence for self-medication and peer smoking mediation. Addiction 2009, 104, 1743–1756. [Google Scholar] [CrossRef]
- National Institute on Drug Abuse; Food and Drug Administration Center for Tobacco Products. Population Assessment of Tobacco and Health (PATH) Study [United States] Public-Use Files. Inter-University Consortium for Political and Social Research [Distributor]; National Institutes of Health National Institute on Drug Abuse: Bethesda, MD, USA, 2020.
- Hyland, A.; Ambrose, B.K.; Conway, K.P.; Borek, N.; Lambert, E.; Carusi, C.; Taylor, K.; Crosse, S.; Fong, G.T.; Cummings, K.M. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob. Control 2017, 26, 371–378. [Google Scholar] [CrossRef]
- Inter-University Consortium for Political and Social Research. Population Assessment of Tobacco and Health (PATH) Study [United States] Public-Use Files ICPSR Public-Use Files User Guide. Available online: https://www.icpsr.umich.edu/files/NAHDAP/documentation/ug36498-all.pdf (accessed on 21 January 2021).
- National Institute on Drug Abuse; Food Drug Administration Center for Tobacco Products. Population Assessment of Tobacco and Health (PATH) Study [United States] Restricted-Use Files. Inter-university Consortium for Political and Social Research [distributor]; National Institutes of Health National Institute on Drug Abuse: Atlanta, GA, USA, 2020.
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Kasza, K.A.; Edwards, K.C.; Tang, Z.; Stanton, C.A.; Sharma, E.; Halenar, M.J.; Taylor, K.A.; Donaldson, E.; Hull, L.C.; Day, H. Correlates of tobacco product initiation among youth and adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob. Control 2020, 29, s191–s202. [Google Scholar] [CrossRef]
- Kasza, K.A.; Edwards, K.C.; Tang, Z.; Stanton, C.A.; Sharma, E.; Halenar, M.J.; Taylor, K.A.; Donaldson, E.A.; Hull, L.C.; Bansal-Travers, M. Correlates of tobacco product cessation among youth and adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob. Control 2020, 29, s203–s215. [Google Scholar] [CrossRef] [PubMed]
- Edwards, K.C.; Kasza, K.A.; Tang, Z.; Stanton, C.A.; Sharma, E.; Halenar, M.J.; Taylor, K.A.; Donaldson, E.A.; Hull, L.C.; Bansal-Travers, M. Correlates of tobacco product reuptake and relapse among youth and adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob. Control 2020, 29, s216–s226. [Google Scholar] [CrossRef]
- Stanton, C.A.; Sharma, E.; Seaman, E.L.; Kasza, K.A.; Edwards, K.C.; Halenar, M.J.; Taylor, K.A.; Day, H.; Anic, G.; Hull, L.C. Initiation of any tobacco and five tobacco products across 3 years among youth, young adults and adults in the USA: Findings from the PATH Study Waves 1–3 (2013–2016). Tob. Control 2020, 29, s178–s190. [Google Scholar] [CrossRef] [PubMed]
- Conway, K.P.; Green, V.R.; Kasza, K.A.; Silveira, M.L.; Borek, N.; Kimmel, H.L.; Sargent, J.D.; Stanton, C.; Lambert, E.; Hilmi, N. Co-occurrence of tobacco product use, substance use, and mental health problems among adults: Findings from Wave 1 (2013–2014) of the Population Assessment of Tobacco and Health (PATH) Study. Drug Alcohol Depend. 2017, 177, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Conway, K.P.; Green, V.R.; Kasza, K.A.; Silveira, M.L.; Borek, N.; Kimmel, H.L.; Sargent, J.D.; Stanton, C.A.; Lambert, E.; Hilmi, N. Co-occurrence of tobacco product use, substance use, and mental health problems among youth: Findings from wave 1 (2013–2014) of the population assessment of tobacco and health (PATH) study. Addict. Behav. 2018, 76, 208–217. [Google Scholar] [CrossRef]
- Kong, G.; Kuguru, K.E.; Krishnan-Sarin, S. Gender differences in US adolescent e-cigarette use. Curr. Addict. Rep. 2017, 4, 422–430. [Google Scholar] [CrossRef]
- Perkins, K.A. Acute responses to nicotine and smoking: Implications for prevention and treatment of smoking in lower SES women. Drug Alcohol Depend. 2009, 104, S79–S86. [Google Scholar] [CrossRef]
- Sofuoglu, M.; Mooney, M. Subjective responses to intravenous nicotine: Greater sensitivity in women than in men. Exp. Clin. Psychopharmacol. 2009, 17, 63. [Google Scholar] [CrossRef]
- Rubinstein, M.L.; Shiffman, S.; Rait, M.A.; Benowitz, N.L. Race, gender, and nicotine metabolism in adolescent smokers. Nicotine Tob. Res. 2013, 15, 1311–1315. [Google Scholar] [CrossRef]
- Kong, G.; Morean, M.E.; Cavallo, D.A.; Camenga, D.R.; Krishnan-Sarin, S. Sources of electronic cigarette acquisition among adolescents in Connecticut. Tob. Regul. Sci. 2017, 3, 10–16. [Google Scholar] [CrossRef]
- Green, V.R.; Conway, K.P.; Silveira, M.L.; Kasza, K.A.; Cohn, A.; Cummings, K.M.; Stanton, C.A.; Callahan-Lyon, P.; Slavit, W.; Sargent, J.D. Mental health problems and onset of tobacco use among 12-to 24-year-olds in the PATH study. J. Am. Acad. Child Adolesc. Psychiatry 2018, 57, 944–954.e944. [Google Scholar] [CrossRef] [PubMed]
- Flay, B.R. School-based smoking prevention programs with the promise of long-term effects. Tob. Induc. Dis. 2009, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Kulig, J.W. Tobacco, alcohol, and other drugs: The role of the pediatrician in prevention, identification, and management of substance abuse. Pediatrics 2005, 115, 816–821. [Google Scholar] [CrossRef]
- Coughlin, S.S. Recall bias in epidemiologic studies. J. Clin. Epidemiol. 1990, 43, 87–91. [Google Scholar] [CrossRef]
- Chapman, S.; Bareham, D.; Maziak, W. The gateway effect of e-cigarettes: Reflections on main criticisms. Nicotine Tob. Res. 2019, 21, 695–698. [Google Scholar] [CrossRef] [PubMed]
- Shahab, L.; Beard, E.; Brown, J. Association of initial e-cigarette and other tobacco product use with subsequent cigarette smoking in adolescents: A cross-sectional, matched control study. Tob. Control 2020. [Google Scholar] [CrossRef]
- Morgenstern, M.; Nies, A.; Goecke, M.; Hanewinkel, R. E-Cigarettes and the Use of Conventional Cigarettes: A cohort study in 10th grade students in Germany. Dtsch. Ärzteblatt Int. 2018, 115, 243. [Google Scholar] [CrossRef]


{kind=link}
| Wave 1 (n = 5001) | Wave 2 (n = 6637) | Wave 3 (n = 8177) | |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Interview status | |||
| Youth (aged 12–17) | 5001 (100) | 4864 (73.3) | 4711 (57.6) |
| Shadow youth (aged 9–11) | 0 (0) | 1773 (26.7) | 3466 (42.4) |
| P30D e-cigarette use | |||
| Yes | 19 (0.4) | 53 (0.9) | 112 (1.5) |
| No | 4949 (99.6) | 6538 (99.1) | 8033 (98.5) |
| Age group | |||
| 12–14 | 4388 (96.7) | 5147 (77.0) | 5175 (63.3) |
| 15–17 | 168 (3.3) | 1490 (23.0) | 3002 (36.7) |
| Sex | |||
| Male | 2551 (50.8) | 3365 (50.8) | 4190 (51.1) |
| Female | 2450 (49.2) | 3253 (49.2) | 3963 (48.9) |
| Race/ethnicity | |||
| Non-Hispanic White | 2334 (53.4) | 2984 (52.5) | 3624 (51.7) |
| Non-Hispanic Black | 722 (14.4) | 899 (13.9) | 1087 (13.6) |
| Non-Hispanic Other | 447 (9.2) | 586 (9.7) | 739 (10.1) |
| Hispanic | 1498 (23.0) | 1946 (23.9) | 2402 (24.6) |
| Sexual orientation (ages 14+) | |||
| Straight/Heterosexual | 1455 (94.9) | 2867 (92.3) | 4145 (90.9) |
| Gay, lesbian, bisexual, or other | 75 (5.1) | 234 (7.7) | 421 (9.1) |
| Parental education | |||
| Less than high school | 1009 (17.4) | 1199 (16.4) | 1511 (15.9) |
| High school graduate | 907 (17.3) | 1105 (17.0) | 1392 (16.4) |
| Some college or associate degree | 1024 (19.9) | 1882 (30.3) | 2519 (31.0) |
| Bachelor’s degree or above | 2032 (45.4) | 1928 (36.6) | 2583 (36.7) |
| P30D use of other tobacco products 1 | |||
| Yes | 19 (0.4) | 32 (0.6) | 56 (0.7) |
| No | 4757 (99.6) | 6461 (99.4) | 8059 (99.3) |
| Past year internalizing problems | |||
| Low | 2558 (52.5) | 3420 (52.6) | 4023 (50.7) |
| Moderate | 1432 (29.4) | 1771 (27.7) | 2205 (28.0) |
| High | 856 (18.1) | 1269 (19.7) | 1704 (21.3) |
| Past year externalizing problems | |||
| Low | 1901 (39.8) | 2776 (43.4) | 3397 (43.2) |
| Moderate | 1446 (30.7) | 1738 (27.8) | 2127 (27.8) |
| High | 1368 (29.5) | 1807 (28.8) | 2249 (29.1) |
| Covariates at Corresponding Baseline Wave | P30D Cigarette Smoking at Follow-up Waves | ||
|---|---|---|---|
| Wave 2 (n = 5001) | Wave 3 (n = 6637) | Wave 4 (n = 8177) | |
| % (95% CI) | % (95% CI) | % (95% CI) | |
| Total | 1.2 (0.9–1.6) | 0.9 (0.7–1.2) | 1.5 (1.2–1.8) |
| P30D e-cigarette use | |||
| Yes | 4.0 (0.5–27.7) | 12.6 (5.1–27.6) | 9.1 (4.9–16.4) |
| No | 1.2 (0.9–1.6) | 0.8 (0.6–1.2) | 1.4 (1.1–1.7) |
| Age group | |||
| 12–14 | 1.1 (0.8–1.6) | 0.7 (0.5–1.1) | 0.9 (0.6–1.2) |
| 15–17 | 1.9 (0.6–5.9) | 1.7 (1.2–2.5) | 2.6 (2.0–3.5) |
| Sex | |||
| Male | 0.8 (0.5–1.3) | 0.6 (0.4–1.0) | 1.7 (1.3–2.1) |
| Female | 1.6 (1.1–2.2) | 1.3 (0.9–1.8) | 1.4 (1.0–1.9) |
| Race/ethnicity | |||
| Non-Hispanic White | 1.3 (0.9–2.0) | 1.3 (0.9–1.8) | 1.9 (1.4–2.5) |
| Non-Hispanic Black | 0.5 (0.2–1.7) | 0.3 (0.1–0.8) | 0.8 (0.4–1.7) |
| Non-Hispanic Other | 1.1 (0.4–3.2) | 1.1 (0.4–2.9) | 1.0 (0.5–1.8) |
| Hispanic | 1.2 (0.7–2.0) | 0.6 (0.3–1.1) | 1.4 (1.0–2.0) |
| Sexual orientation (ages 14+) | |||
| Straight/Heterosexual | 1.7 (1.0–2.7) | 1.0 (0.7–1.6) | 2.0 (1.5–2.5) |
| Gay, lesbian, bisexual, or other | 4.7 (1.6–12.9) | 3.3 (1.5–7.1) | 5.3 (3.4–8.3) |
| Parental education | |||
| Less than high school | 1.5 (0.8–2.8) | 0.6 (0.3–1.5) | 2.1 (1.4–3.0) |
| High school graduate | 1.7 (0.9–3.0) | 1.4 (1.7–2.8) | 1.4 (0.9–2.2) |
| Some college or associate degree | 1.9 (1.1–3.0) | 0.8 (0.5–1.3) | 1.8 (1.3–2.5) |
| Bachelor’s degree or above | 0.6 (0.3–1.0) | 0.8 (0.5–1.4) | 1.1 (0.7–1.7) |
| P30D use of other tobacco products 1 | |||
| Yes | 4.5 (0.5–30.8) | 8.7 (2.2–29.0) | 12.7 (6.1–24.8) |
| No | 1.2 (0.9–1.6) | 0.9 (0.7–1.2) | 1.4 (1.2–1.8) |
| Past year internalizing problems | |||
| Low | 0.7 (0.4–1.2) | 0.6 (0.4–1.0) | 1.3 (0.9–1.8) |
| Moderate | 1.5 (0.9–2.5) | 1.2 (0.7–2.0) | 1.1 (0.7–1.7) |
| High | 1.8 (1.1–3.0) | 1.4 (0.8–2.4) | 2.6 (1.9–3.5) |
| Past year externalizing problems | |||
| Low | 0.4 (0.2–0.9) | 0.6 (0.4–1.0) | 1.1 (0.8–1.6) |
| Moderate | 1.1 (0.6–2.0) | 0.8 (0.4–1.6) | 1.2 (0.8–1.9) |
| High | 2.5 (1.7–3.6) | 1.5 (0.9–2.4) | 2.2 (1.6–2.9) |
| Model 1 | Model 2 | |
|---|---|---|
| No Interaction | With Interaction | |
| aOR (95% CI) | aOR (95% CI) | |
| P30D e-cigarette use | ||
| Yes | 3.90 (2.51–6.08) | 1.93 (0.79–4.71) |
| No | Ref. | Ref. |
| Sex | ||
| Male | 1.24 (1.03–1.49) | 1.19 (0.98–1.43) |
| Female | Ref. | Ref. |
| P30D e-cigarette use # Sex | ||
| Yes # Male | 3.18 (2.21–4.57) | |
| No # Female | Ref. | |
| Age group | ||
| 12–14 | Ref. | Ref. |
| 15–17 | 1.80 (1.44–2.26) | 1.81 (1.44–2.26) |
| Race/ethnicity | ||
| Non-Hispanic White | Ref. | Ref. |
| Non-Hispanic Black | 0.46 (0.30–0.70) | 0.46 (0.30–0.70) |
| Non-Hispanic Other | 0.66 (0.43–1.01) | 0.66 (0.43–1.01) |
| Hispanic | 0.66 (0.50–0.89) | 0.66 (0.50–0.89) |
| Parental education | ||
| Less than high school | Ref. | Ref. |
| High school graduate | 0.92 (0.66–1.29) | 0.92 (0.65–1.29) |
| Some college or associate degree | 0.76 (0.55–1.05) | 0.75 (0.54–1.04) |
| Bachelor’s degree or above | 0.50 (0.35–0.71) | 0.50 (0.35–0.71) |
| P30D use of other tobacco products 1 | ||
| Yes | 3.22 (1.23–8.46) | 3.45 (1.36–8.70) |
| No | Ref. | Ref. |
| Internalizing mental health problems | ||
| Low | Ref. | Ref. |
| Moderate | 1.33 (1.04–2.58) | 1.33 (1.05–1.69) |
| High | 1.90 (1.40–2.58) | 1.93 (1.42–2.63) |
| Externalizing mental health problems | ||
| Low | Ref. | Ref. |
| Moderate | 1.40 (1.01–1.95) | 1.41 (1.01–1.97) |
| High | 2.11 (1.55–2.88) | 2.09 (1.54–2.85) |
| Boys P30D Cigarette Smoking | Girls P30D Cigarette Smoking | |
|---|---|---|
| aOR (95% CI) | aOR (95% CI) | |
| P30D e-cigarette use | ||
| Yes | 6.17 (2.43–15.68) | 1.10 (0.14–8.33) |
| No | Ref. | Ref. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duan, Z.; Wang, Y.; Huang, J. Sex Difference in the Association between Electronic Cigarette Use and Subsequent Cigarette Smoking among U.S. Adolescents: Findings from the PATH Study Waves 1–4. Int. J. Environ. Res. Public Health 2021, 18, 1695. https://doi.org/10.3390/ijerph18041695
Duan Z, Wang Y, Huang J. Sex Difference in the Association between Electronic Cigarette Use and Subsequent Cigarette Smoking among U.S. Adolescents: Findings from the PATH Study Waves 1–4. International Journal of Environmental Research and Public Health. 2021; 18(4):1695. https://doi.org/10.3390/ijerph18041695
Chicago/Turabian StyleDuan, Zongshuan, Yu Wang, and Jidong Huang. 2021. "Sex Difference in the Association between Electronic Cigarette Use and Subsequent Cigarette Smoking among U.S. Adolescents: Findings from the PATH Study Waves 1–4" International Journal of Environmental Research and Public Health 18, no. 4: 1695. https://doi.org/10.3390/ijerph18041695
APA StyleDuan, Z., Wang, Y., & Huang, J. (2021). Sex Difference in the Association between Electronic Cigarette Use and Subsequent Cigarette Smoking among U.S. Adolescents: Findings from the PATH Study Waves 1–4. International Journal of Environmental Research and Public Health, 18(4), 1695. https://doi.org/10.3390/ijerph18041695