
Evaluation of the Use of Sterilized and Non-Sterilized Peruibe Black Mud in Patients with Knee Osteoarthritis


Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
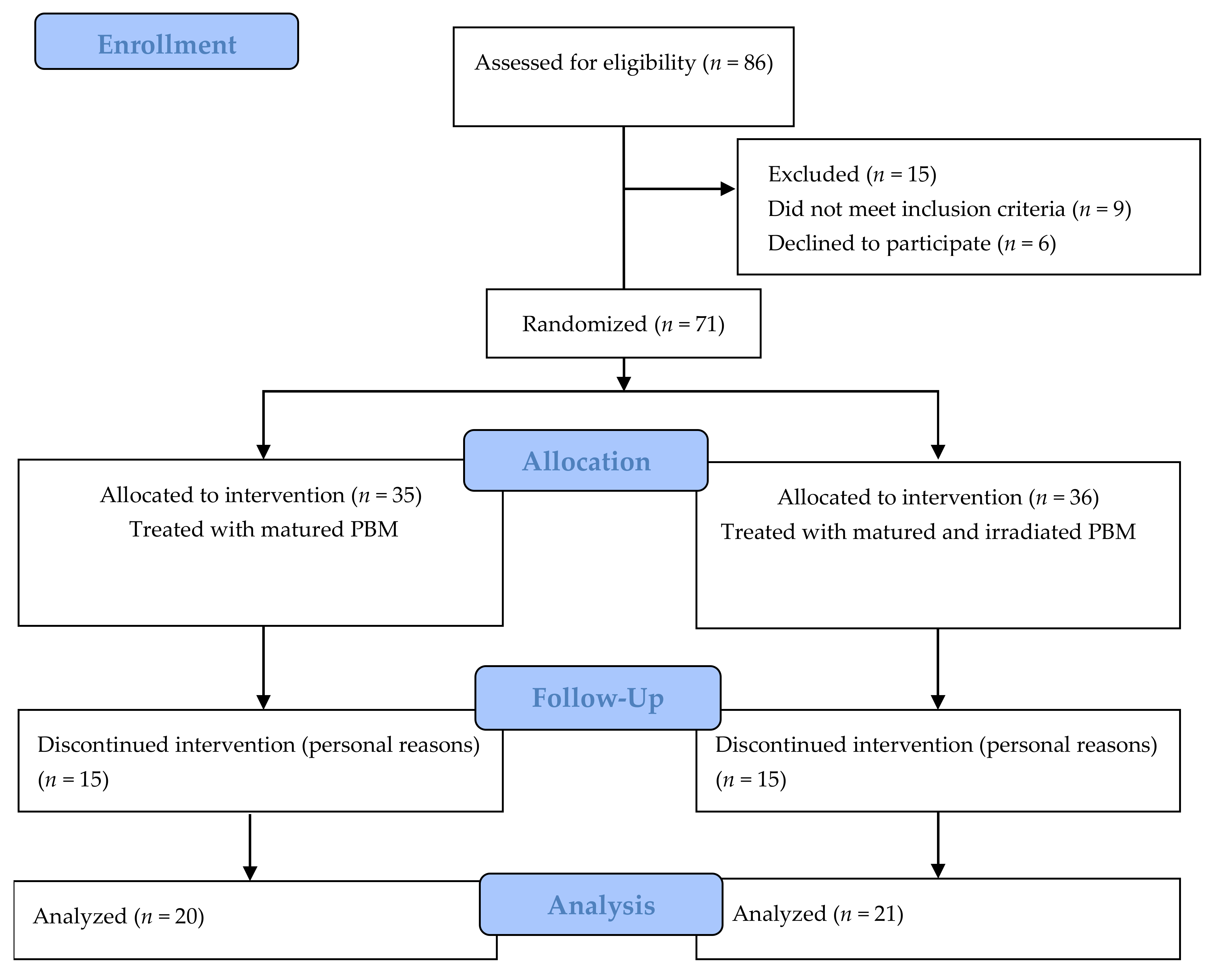
2.2. Experimental Design
2.3. Intervention
2.4. Evaluation Parameters
2.4.1. Analysis of Pain, Discomfort, and Quality of Life
2.4.2. Radiographic Evaluation
2.4.3. Determination of Serum Concentrations of Cytokines and PGE2
2.5. Statistical Analysis
3. Results
3.1. WOMAC Evaluation
3.2. SF-36 Evaluation
3.3. Radiographic Evaluation
3.4. Serum Levels of Inflammatory Mediators
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Fazaa, A.; Souabni, L.; Ben Abdelghani, K.; Kassab, S.; Chekili, S.; Zouari, B.; Hajri, R.; Laatar, A.; Zakraoui, L. Comparison of the clinical effectiveness of thermal cure and rehabilitation in knee osteoarthritis. A randomized therapeutic trial. Ann. Phys. Rehabil. Med. 2014, 57, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, A.; Tenti, S.; Giannitti, C.; Fortunati, N.A.; Galeazzi, M. Short- and long-term effects of mud-bath treatment on hand osteoarthritis: A randomized clinical trial. Int. J. Biometeorol. 2014, 58, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Riyaz, N.; Arakkal, F.R. Spa therapy in dermatology. Indian J. Dermatol. Venereol. Leprol. 2011, 77, 128–134. [Google Scholar] [CrossRef]
- Maeda, T.; Kudo, Y.; Horiuchi, T.; Makino, N. Clinical and anti-aging effect of mud-bathing therapy for patients with fibromyalgia. Mol. Cell. Biochem. 2018, 444, 87–92. [Google Scholar] [CrossRef]
- Quintela, A.; Terroso, D.; Ferreira da Silva, E.; Rocha, F. Certification and quality criteria of peloids used for therapeutic purposes. Clay Miner. 2012, 47, 441–451. [Google Scholar] [CrossRef]
- Bellometti, S.; Cecchettin, M.; Galzigna, L. Mud pack therapy in osteoarthrosis. Changes in serum levels of chondrocyte markers. Clin. Chim. Acta 1997, 268, 101–106. [Google Scholar] [CrossRef]
- Caraglia, M.; Beninati, S.; Giuberti, G.; D’Alessandro, A.M.; Lentini, A.; Abbruzzese, A.; Bove, G.; Landolfi, F.; Rossi, F.; Lampa, E.; et al. Alternative therapy of earth elements increases the chondroprotective effects of chondroitin sulfate in mice. Exp. Mol. Med. 2005, 37, 476–481. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pascarelli, N.A.; Cheleschi, S.; Bacaro, G.; Guidelli, G.M.; Galeazzi, M.; Fioravanti, A. Effect of Mud-Bath Therapy on Serum Biomarkers in Patients with Knee Osteoarthritis: Results from a Randomized Controlled Trial. Isr. Med. Assoc. J. 2016, 18, 232–237. [Google Scholar]
- Galzigna, L.; Moretto, C.; Lalli, A. Physical and biochemical changes of thermal mud after maturation. Biomed. Pharmacother. 1996, 50, 306–308. [Google Scholar] [CrossRef]
- Levinger, I.; Levinger, P.; Trenerry, M.K.; Feller, J.A.; Bartlett, J.R.; Bergman, N.; McKenna, M.J.; Cameron-Smith, D. Increased inflammatory cytokine expression in the vastus lateralis of patients with knee osteoarthritis. Arthritis. Rheum. 2011, 63, 1343–1348. [Google Scholar] [CrossRef]
- Cecchettin, M.; Bellometti, S.; Lalli, A.; Galzigna, L. Serum interleukin 1 changes in arthrosic patients after mud-pack treatment. Phys. Rheabil. Kur. Med. 1995, 5, 92–93. [Google Scholar] [CrossRef]
- Bellometti, S.; Cecchettin, M.; Lalli, A.; Galzigna, L. Mud pack treatment increases serum antioxidant defenses in osteoarthrosic patients. Biomed. Pharmacother. 1996, 50, 50–57. [Google Scholar] [CrossRef]
- Saladino, R.; Chiocchini, U.; Botta, G.; Delfino, M.; Conigliaro, R.; Mosesso, P. Free radical scavenging capacity and protective effect of natural substances in peloids from the thermal spring pool Bagnaccio (Viterbo, Italy). J. Cosmet. Sci. 2016, 67, 71–92. [Google Scholar]
- Cozzi, F.; Raffeiner, B.; Beltrameb, V.; Cipriana, L.; Coranb, A.; Botsios, C.; Perissinotto, E.; Grisan, E.; Ramonda, R.; Oliviero, F.; et al. Effects of mud-bath therapy in psoriatic arthritis patients treated with TNF inhibitors. Clinical evaluation and assessment of synovial inflammation by contrast-enhanced ultrasound (CEUS). Jt. Bone Spine 2015, 82, 104–108. [Google Scholar] [CrossRef]
- Argenziano, G.; Delfino, M.; Russo, N. Mud and baththerapy in the acne cure. Clin. Ter. 2004, 155, 121–125. [Google Scholar]
- Clijsen, R.; Taeymans, J.; Duquet, W.; Barel, A.; Clarys, P. Changes of skin characteristics during and after local Parafango therapy as used in physiotherapy. Skin. Res. Technol. 2008, 14, 237–242. [Google Scholar] [CrossRef]
- Ciprian, L.; Lo Nigro, A.; Rizzo, M.; Gava, A.; Ramonda, R.; Punzi, L.; Cozzi, F. The effects of combined spa therapy and rehabilitation on patients with ankylosing spondylitis being treated with TNF inhibitors. Rheumatol. Int. 2013, 33, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Karagülle, M.; Karagülle, M.Z. Effectiveness of balneotherapy and spa therapy for the treatment of chronic low back pain: A review on latest evidence. Clin. Rheumatol. 2015, 34, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.S.C.; Torrecilha, J.K.; Gouvea, P.F.M.; Máduar, M.F.; Oliveira, S.M.B.; Scapin, M.A. Chemical and radiological characterization of Peruíbe Black Mud. Appl. Clay Sci. 2015, 118, 221–230. [Google Scholar] [CrossRef]
- Britschka, Z.M.N.; Teodoro, W.R.; Velosa, A.P.; de Mello, S.B. The efficacy of Brazilian black mud treatment in chronic experimental arthritis. Rheumatol. Int. 2007, 28, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Chaganti, R.K.; Lane, N. Risk factors for incident osteoarthritis of the hip and knee. Curr. Rev. Musculoskelet. Med. 2011, 4, 99–104. [Google Scholar] [CrossRef]
- Plotnikoff, R.; Karunamuni, N.; Lytvyak, E.; Penfold, C.; Schopflocher, D.; Imayama, I.; Johnson, S.T.; Raine, K. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health 2015, 15, 1195. [Google Scholar] [CrossRef]
- Bellometti, S.; Galzigna, L.; Richelmi, P.; Gregotti, C.; Bertè, F. Both serum receptors of tumor necrosis factor are influenced by mud pack treatment in osteoarthrotic patients. Int. J. Tissue React. 2002, 24, 57–64. [Google Scholar]
- Ortega, E.; Gálvez, I.; Hinchado, M.D.; Guerrero, J.; Martín-Cordero, L.; Torres-Piles, S. Anti-inflammatory effect as a mechanism of effectiveness underlying the clinical benefits of pelotherapy in osteoarthritis patients: Regulation of the altered inflammatory and stress feedback response. Int. J. Biometeorol. 2017, 29, 1–9. [Google Scholar] [CrossRef]
- ANSI/AAMI ST32. Guideline for Gamma Radiation Sterilization; AAMI: Arlington, VA, USA, 1991. [Google Scholar]
- Bellamy, N.; Buchaman, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar] [PubMed]
- Pollard, B.; Johnston, M.; Dixon, D. Exploring differential item functioning in the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). BMC Musculoskelet. Disord. 2012, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 2015, 16, 494–502. [Google Scholar] [CrossRef]
- Miettinem, O.S. Quality of life from the epidemiologic perspective. J. Chron. Dis. 1987, 40, 641–643. [Google Scholar] [CrossRef]
- Fioravanti, A.; Cantarini, L.; Guidelli, G.M.; Galeazzi, M. Mechanisms of action of spa therapies in rheumatic diseases: What scientific evidence is there? Rheumatol. Int. 2011, 31, 1–8. [Google Scholar] [CrossRef]
- Sánchez-Espejo, R.; Aguzzi, C.; Cerezo, P.; Salcedo, I.; López-Galindo, A.; Viseras, C. Folk pharmaceutical formulations in western Mediterranean: Identification and safety of clays used in pelotherapy. J. Ethnopharmacol. 2014, 155, 810–814. [Google Scholar] [CrossRef]
- Giacomino, M.I.; de Michele, D.F. Is mud an anti-inflammatory? An. Med. Interna 2007, 24, 352–353. [Google Scholar]
- Espejo-Antúnez, L.; Cardero-Durán, M.A.; Garrido-Ardila, E.M.; Torres-Piles, S.; Caro-Puártolas, B. Clinical effectiveness of mud pack therapy in knee osteoarthritis. Rheumatology 2013, 52, 659–668. [Google Scholar] [CrossRef]
- Maraver, F.; Fernández-Torán, M.A.; Corvillo, I.; Morer, C.; Váquez, I.; Aguillera, L.; Armijo, F. Peloterapia, una revisión. Medicina Naturista 2015, 9, 38–46. [Google Scholar]
- Cherkin, D. Spa therapy: Panacea or placebo? Med. Care 1998, 36, 1303–1305. [Google Scholar] [CrossRef] [PubMed]
- Sukenik, S.; Flusser, D.; Balint, G.P.; Abu-Shakra, M. The Role of Spa Therapy in Various Diseases. Rheum. Dis. Clin. N. Am. 1999, 25, 883–897. [Google Scholar] [CrossRef]
- Gungüen, G.; Ardic, F.; Gulin, F.; Rota, S. The effect of mud pack therapy on serum YKL-40 and hsCRP levels in patients with knee osteoarthritis. Rheumatol. Int. 2012, 32, 1235–1244. [Google Scholar] [CrossRef]
- Bellometti, S.; Galzigna, L. Function of the hypothalamic adrenal axis in patients with fibromyalgia syndrome undergoing mud-pack treatment. Int. J. Clin. Pharmacol. Res. 1999, 19, 27–33. [Google Scholar]
- Pizzoferrato, A.; Garzia, I.; Cenni, E.; Pratelli, L.; Tarabusi, C. Beta-endorphin and stress hormones in patients affected by osteoarthritis undergoing thermal mud therapy. Minerva Med. 2000, 91, 239–245. [Google Scholar] [PubMed]
- Basili, S.; Martini, F.; Ferroni, P.; Grassi, M.; Scavalli, A.S.; Streva, P.; Cusumano, G.; Musca, A.; Rini, G.B. Effects of mud-pack treatment on plasma cytokine and soluble adhesion molecule levels in healthy volunteers. Clin. Chim. Acta 2001, 314, 209–214. [Google Scholar] [CrossRef]
- Oláh, M.; Konz, A.; Fehér, J.; Kalmánczhey, J.; Oláh, C.; Nagy, G.; Bender, T. The effect of balneotherapy on antioxidant, inflammatory, and metabolic indices in patients with cardiovascular risk factors (hypertension and obesity) A randomised, controlled, follow-up study. Contemp. Clin. Trials 2011, 32, 793–801. [Google Scholar]
- Stier-Jarmer, M.; Kus, S.; Frisch, D.; Sabariega, C.; Schuh, A. Health resort medicine in non-musculoskeletal disorders: Is there evidence of its effectiveness? Int. J. Biometeorol. 2015, 59, 1523–1544. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total | Mean | Median |
|---|---|---|---|
| Number of patients (group A) | 20 | ||
| Number of patients (group B) | 21 | ||
| Age—group A (years; mean ± SD) | 62 ± 11 | 62 | |
| Age—group B (years; mean ± SD) | 63 ± 9 | 67 | |
| Gender—group A (M/F) | 5 (25%)/15 (75%) | ||
| Gender—group B (M/F) | 6 (29%)/15 (71%) | ||
| Time since first complaint—group A (years; mean ± SD) | 6 ± 4 | 7.5 | |
| Time since first complaint—group B (years; mean ± SD) | 6 ± 5 | 2.5 | |
| Radiographic scores—group A | |||
| II | 14 | ||
| III | 5 | ||
| IV | 1 | ||
| Radiographic scores—group B | |||
| II | 13 | ||
| III | 7 | ||
| IV | 1 |
| Group A (n = 20) | Group B (n = 21) | p Values of Mean Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Ai | Af | Bi | Bf | ||||||
| Domain | Mean ± sd | Mean ± sd | Mean ± sd | Mean ± sd | 1 Ti × Tf | Ai × Bi | 2 Ai × Af | 3 Bi × Bf | Af × Bf |
| PA | 9 ± 4 | 4 ± 4 | 9 ± 5 | 5 ± 3 | 1.3 × 10−7 | 0.82 | 2.0 × 10−4 | 2.0 × 10−4 | 0.41 |
| JS | 3 ± 2 | 2 ± 2 | 3 ± 2 | 2 ± 2 | 1.5 × 10−5 | 0.78 | 2.2 × 10−3 | 6.0 × 10−4 | 0.64 |
| PF | 28 ± 16 | 16 ± 16 | 32 ± 14 | 19 ± 13 | 8.0 × 10−8 | 0.58 | 2.0 × 10−4 | 1.1 × 10−5 | 0.26 |
| Group A (n = 20) | Group B (n = 21) | p Values of Mean Comparisons | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Ai | Af | Bi | Bf | ||||||
| Domains | Mean ± sd | Mean ± sd | Mean ± sd | Mean ± sd | 1 Ti × Tf | Ai × Bi | 2 Ai × Af | 3 Bi × Bf | Af × Bf |
| PF | 41 ± 26 | 62 ± 31 | 44 ± 30 | 56 ± 26 | 9.7 × 10−7 | 0.72 | 8.3 × 10−4 | 4.3 × 10−3 | 0.56 |
| RP | 30 ± 24 | 53 ± 41 | 26 ± 33 | 62 ± 35 | 2.9 × 10−5 | 0.028 | 0.010 | 1.1 × 10−3 | 0.52 |
| BP | 35 ± 20 | 58 ± 25 | 35 ± 26 | 53 ± 28 | 2.5 × 10−5 | 0.96 | 2.6 × 10−5 | 8.6 × 10−3 | 0.55 |
| GH | 58 ± 19 | 73 ± 24 | 68 ± 17 | 78 ± 15 | 1.5 × 10−5 | 0.10 | 1.6 × 10−3 | 3.4 × 10−3 | 0.86 |
| VT | 52 ± 25 | 73 ± 21 | 52 ± 26 | 72 ± 17 | 3.3 × 10−7 | 0.87 | 7.2 × 10−4 | 2.0 × 10−4 | 0.92 |
| SF | 69 ± 29 | 76 ± 30 | 67 ± 26 | 77 ± 23 | 0.034 | 0.86 | 0.23 | 0.070 | 0.81 |
| RE | 37 ± 35 | 62 ± 42 | 41 ± 40 | 62 ± 40 | 6.7 × 10−4 | 0.75 | 0.019 | 0.023 | 1.0 |
| MH | 61 ± 24 | 71 ± 27 | 65 ± 22 | 70 ± 19 | 6.4 × 10−3 | 0.49 | 3.0 × 10−3 | 0.25 | 0.43 |
| Ti | Tf | Ai | Af | Bi | Bf | |
|---|---|---|---|---|---|---|
| Grade 0—no signs | 0 | 4 | 0 | 3 | 0 | 1 |
| Grade I—doubtful | 0 | 5 | 0 | 2 | 0 | 3 |
| Grade II—minimal | 27 | 20 | 14 | 11 | 13 | 9 |
| Grade III—moderate | 12 | 10 | 5 | 3 | 7 | 7 |
| Grade IV—severe | 2 | 2 | 1 | 1 | 1 | 1 |
| Mediators | Ai | Af | Bi | Bf |
|---|---|---|---|---|
| IL-1β | 1.7 ± 0.3 | 1.2 ± 0.5 | 1.2 ± 0.3 | 0.6 ± 0.3 |
| TNF-α | 6.4 ± 1.3 | 5.3 ± 2.0 | 6.1 ±1.4 | 2.4 ± 0.9 |
| IL-6 | 2.8 ± 0.3 | 3.0 ± 0.5 | 3.0 ± 0.3 | 3.2 ± 0.5 |
| IL-8 | 12.5 ± 2.5 | 10.4 ± 2.0 | 8.4 ± 1.3 | 10.7 ± 2.0 |
| IL-10 | 1.8 ± 0.7 | 1.6 ± 1.0 | 2.5 ± 1.1 | 4.1 ± 1.8 |
| PGE2 | 737 ± 124 | 633 ± 176 | 650 ± 158 | 772 ± 178 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gouvêa, P.F.M.; Britschka, Z.M.N.; Gomes, C.d.O.M.S.; Queiroz, N.G.T.d.; Salvador, P.A.V.; Silva, P.S.C. Evaluation of the Use of Sterilized and Non-Sterilized Peruibe Black Mud in Patients with Knee Osteoarthritis. Int. J. Environ. Res. Public Health 2021, 18, 1666. https://doi.org/10.3390/ijerph18041666
Gouvêa PFM, Britschka ZMN, Gomes CdOMS, Queiroz NGTd, Salvador PAV, Silva PSC. Evaluation of the Use of Sterilized and Non-Sterilized Peruibe Black Mud in Patients with Knee Osteoarthritis. International Journal of Environmental Research and Public Health. 2021; 18(4):1666. https://doi.org/10.3390/ijerph18041666
Chicago/Turabian StyleGouvêa, Paulo Fávio Macedo, Zélia Maria Nogueira Britschka, Cristina de Oliveira Massoco Salles Gomes, Nicolle Gilda Teixeira de Queiroz, Pablo Antonio Vásquez Salvador, and Paulo Sergio Cardoso Silva. 2021. "Evaluation of the Use of Sterilized and Non-Sterilized Peruibe Black Mud in Patients with Knee Osteoarthritis" International Journal of Environmental Research and Public Health 18, no. 4: 1666. https://doi.org/10.3390/ijerph18041666
APA StyleGouvêa, P. F. M., Britschka, Z. M. N., Gomes, C. d. O. M. S., Queiroz, N. G. T. d., Salvador, P. A. V., & Silva, P. S. C. (2021). Evaluation of the Use of Sterilized and Non-Sterilized Peruibe Black Mud in Patients with Knee Osteoarthritis. International Journal of Environmental Research and Public Health, 18(4), 1666. https://doi.org/10.3390/ijerph18041666