Abstract
An increase in the global surface temperature and changes in urban morphologies are associated with increased heat stress especially in urban areas. This can be one of the contributing factors underlying an increase in heat strokes. We examined the impact of summer minimum air temperatures, which often represent nighttime temperatures, as well as a maximum temperature on a heat stroke. We collected data from the records of daily ambulance transports for heat strokes and meteorological data for July and August of 2017–2019 in the Tottori Prefecture, Japan. A time-stratified case-crossover design was used to determine the association of maximum/minimum air temperatures and the incidence of heat strokes. We used a logistic regression to identify factors associated with the severity of heat strokes. A total of 1108 cases were identified with 373 (33.7%) calls originating in the home (of these, 59.8% were the age of ≥ 75). A total of 65.8% of cases under the age of 18 were related to exercise. Days with a minimum temperature ≥ 25 °C had an odds ratio (95% confidence interval) of 3.77 (2.19, 6.51) for the incidence of an exercise-related heat stroke (reference: days with a minimum temperature < 23 °C). The odds ratio for a heat stroke occurring at home or for calls for an ambulance to the home was 6.75 (4.47, 10.20). The severity of the heat stroke was associated with older age but not with air temperature. Minimum and maximum air temperatures may be associated with the incidence of heat strokes and in particular the former with non-exertional heat strokes.
1. Introduction
Multiple factors contribute to the incidence of heat strokes; for example, environmental factors such as high temperatures and humidity, human factors such as dehydration, the presence of comorbidities, delayed heat acclimatization, aging and activity factors such as exercise and work in a hot environment [1]. In particular, climate change including global warming has contributed to the recent increase in the incidence of heat strokes. In 2018, the number of people transported to emergency rooms for a heat stroke in Japan was 95,137, the highest number on record. The number of deaths was 1581, the second highest on record [2,3]. Continued warming over time is expected [4] and up to 1.2 billion people worldwide will be at risk of a heat stroke each year by the year 2100 if global warming continues at this rate [5].
A number of studies have been conducted on the relationship between maximum temperatures and heat strokes, reporting a strong correlation [6,7,8,9,10,11]. We previously noted a strong correlation between maximum temperatures and the number of emergency transports for heat strokes and were able to quantify the risk by temperature [12]. However, to date, most studies have focused on the maximum temperature.
An urban heat island is a phenomenon wherein urban areas are warmer than the surrounding suburban and rural areas typically because of urban geometry and material properties, human activity and reduced natural vegetation. This phenomenon can intensify extreme climatic events [13]. Direct health effects involve elevated body temperatures particularly during heat waves [14,15]. Urbanization is associated with higher temperatures and the number of nights in Japan where the minimum temperature does not fall below 25 °C is increasing [16] not only in cities but also in rural areas [17].
Although large daily differences in temperatures exert negative effects on the human body [18], this may not apply in midsummer. During the summer months, the risk of a stroke and a transient ischemic stroke may increase if minimum temperatures remain high [19]. However, there are no reports on the association of minimum temperatures with the incidence of heat strokes. An association between persistent high temperature environments and the incidence of non-exertional heat strokes resulting from impaired physiological adaptation to heat stress, the so-called classical heat stroke, has been noted [1,20]. However, research on non-exertional heat strokes has received less attention than on exertional heat strokes [21,22]. Therefore, in this study, we used data on emergency transports to investigate the association between maximum and minimum temperatures and heat strokes. In addition, we examined the relationships of temperature for both non-exertional and exertional heat strokes.
2. Materials and Methods
2.1. Study Design and Sites
This study focused on the Tottori Prefecture, which is located on the Sea of Japan side of the Chugoku region in western Japan (Figure 1). The Tottori Prefecture is 3507 km2 in area and the population was 555,663 in October 2019. The percentage area and population of densely inhabited districts in the Tottori Prefecture (2005) are 1.35% (national average, 3.32%) and 34.1% (66.0%), respectively [23]. The Tottori Prefecture is sunny and warm in the summer and snowy in the winter because of the monsoon from the northwest. The penetration rate of air conditioners in the Tottori Prefecture (2014) was 87.1% (the national average, 86.4%) [24]. Out of 47 prefectures, the Tottori Prefecture had the highest number of heat stroke emergency transports per 100,000 population (May–September) in 2019 (76.69) and ranked eighth in 2018 (101.49) and 2017 (68.88) [25,26,27].
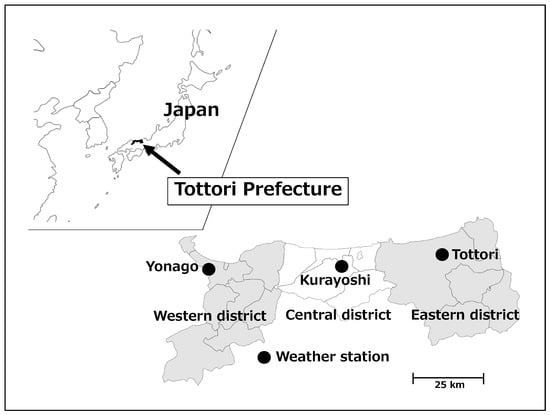
Figure 1.
Location of the Tottori Prefecture and meteorological observation sites. The eastern district (right dark area) includes five, the central district (light area) includes five and the western district (left dark area) includes nine municipalities.
2.2. Ambulance Transport Data
We obtained data on daily ambulance transports for heat strokes from all 26 fire stations in the Tottori Prefecture for July and August of 2017, 2018 and 2019. These data were collected through the Department of Health and Welfare of the Tottori Prefecture, which identified a total of 1187 cases. We did not include the June and September data because the percentage of days with a minimum temperature of 25 °C or higher in these months was 2.8% and the number of heat stroke transports was 13.3% of the total. Each case record contained information on age and sex, the municipality to which the ambulance was called, the date and time of ambulance transport, the medical condition and the initial diagnosis. Furthermore, the record specified the situation surrounding the heat stroke; at home, at work (excluding farm work), exercise (both indoors and outdoors), outside excluding work, farm work, while watching an outside event, during tourist activities or other circumstances. The medical condition and initial diagnosis were determined by the emergency room physician based on the International Classification of Diseases 10th revision (T67: Effects of heat and light) [28] when the patient arrived at the hospital. The medical condition was classified as mild (cases not requiring hospitalization), moderate (non-mild or non-severe cases), severe (cases expected to be hospitalized for more than three weeks) or death. It should be noted that this severity classification is specific to emergency departments and differs from that of the Japanese Association for Acute Medicine Committee [29]. Cases included persons living outside the Tottori Prefecture and these were excluded from the study for reasons described below. The final count of cases included in the analysis was 1108.
2.3. Meteorological Data
Data on daily ambient air temperatures and the average relative humidity in the Tottori Prefecture were provided by the Japan Meteorological Agency. We used data from meteorological observation sites located in three areas; Tottori City as the eastern district (Iwami Town, Yazu Town, Wakasa Town and Chizu Town), Kurayoshi City as the central district (Hokuei Town, Misasa Town, Kotoura Town and Yurihama Town) and Yonago City as the western district (Sakaiminato City, Daisen Town, Hoki Town, Nanbu Town, Kofu Town, Nichinan Town, Hino Town and Hiezu Village) (Figure 1). We selected three of the nine regional weather stations in the Tottori Prefecture because the three cities where these stations are located account for 83.3% of the population and the location of heat stroke incidence is only known on a municipal scale. We used meteorological data from the observation point nearest the location to which the ambulance was called. As the Kurayoshi observation site did not provide relative humidity data, we used data from the Tottori observation site, which is closer in distance, as a substitute.
2.4. Statistical Analysis
We first performed descriptive analyses. Ambulance transport cases were grouped by sex and by age (children (<18 years), adults (18–64 years), semi-elderly (65–74 years) and elderly (≥75 years)). We also tallied cases by time and circumstances of ambulance transport.
We then analyzed the association of maximum air temperature on heat strokes using the time-stratified case-crossover approach. The case-crossover method is useful for assessing the association of transient exposures on the short-term risk of disease when only case data are available [30,31,32]. This design has also been used in recent years in studies such as those estimating the association between temperature factors and adverse health events [33,34]. In the case-crossover design, each case acts as its own control and exposure factors (in this study, the maximum and minimum ambient temperature of the day) are compared between cases and controls. The same days of all other weeks in the same month were selected as the control days (up to four control days per case were used) with the day of transport for the heat stroke as the event day. The reason for this was to eliminate as many confounding factors as possible by assuming that an individual’s life pattern was mostly determined by the day of the week [34,35,36,37]. Seventy-nine subjects living outside the Tottori Prefecture were excluded from the study because they were likely to be outside the Tottori Prefecture on the control days. We used a conditional logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for the association of maximum and minimum air temperatures on heat strokes for all cases and for each subgroup of age/gender. Furthermore, because heat strokes are broadly classified into exertional [38] and non-exertional (classical) [39] heat strokes, we classified cases occurring at home as a non-exertional heat stroke and cases associated with exercise as an exertional heat stroke.
Finally, we quantified the severity of mild, moderate, severe and death in order from 1 to 4 and conducted an ordered logistic regression analysis to identify factors associated with severity. p < 0.05 was considered significant. Analyses were conducted in SPSS version 24.0 (IBM-SPSS, Armonk, NY, USA).
2.5. Ethical Approval
The study was approved by the Tottori University Ethics Committee (No. 180626-069).
3. Results
3.1. Minimum, Average and Maximum Air Temperatures at the Study Sites
Table 1 summarizes the daily minimum, average and maximum air temperatures at observation sites located in the three cities of the Tottori Prefecture during the study period (three year average for 2017–2019). All values were higher than the cumulative annual average calculated for 1981–2010. Table 2 lists the total number of days with a minimum temperature of ≥25 °C, a maximum temperature of ≥30 °C and ≥35 °C at three observation sites (2017–2019).

Table 1.
Daily minimum, average and maximum air temperatures (°C) in three districts of the Tottori Prefecture during the study period (three year average for 2017–2019).
Table 2.
Days with a minimum temperature of ≥25 °C, a maximum temperature of ≥ 0 °C and ≥35 °C (2017–2019).
3.2. Ambulance Transport Data
Table 3 lists the number of heat stroke cases by sex and age group. The mean age of the cases was 59.8 years and the median age was 69.0 years. The number of cases per 1000 residents was highest among elderly men (6.155), a 10-fold increase from the number among adult women (0.596).
Table 3.
Number of heat stroke cases (2017–2019).
An ambulance pickup for a heat stroke occurred mainly at home (33.7% of cases), work (20.9%), during outings (17.9%) and while exercising (15.6%). Ninety-seven percent of cases were mild or moderate with only four deaths (Table 4). A total of 59.8% of the heat stroke cases picked up at home were over 75 years of age and 70.4% of those were of moderate or greater severity.
Table 4.
Location or activity reported by heat stroke cases and stratified by age and severity.
Heat stroke cases were picked up the most in the hour from 11 am. Although not in large numbers, heat stroke cases were also transported at night and early in the morning. 64% of all heat stroke cases in the 12 h after 8 pm were picked up at home (Figure 2).
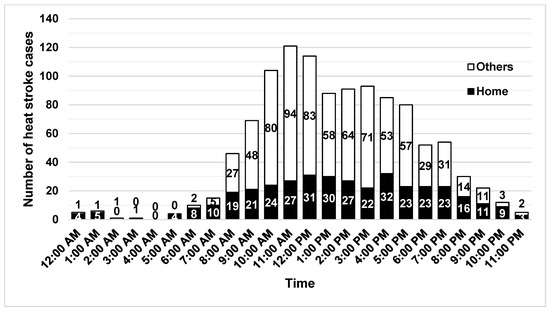
Figure 2.
Pickup time for heat stroke cases. Black bars indicate the number of pickups at home and white bars indicate the others.
3.3. Case-Crossover Analysis
3.3.1. Maximum Air Temperature
We investigated the risk of a heat stroke on days when the maximum air temperature exceeded 30 °C. The risk of a heat stroke increased when the maximum air temperature exceeded the reference temperature (<30 °C; Figure 3). The overall OR (95% CI) was 6.26 (4.67, 8.38) for 30–34.9 °C, 12.24 (8.85, 16.93) for 35–36.9 °C and 17.55 (12.16, 25.32) for ≥ 37 °C. The risk of a heat stroke was higher in individuals aged <18 years than in other age groups and in women. Engaging in exercise was more likely to result in a heat stroke than other activities.
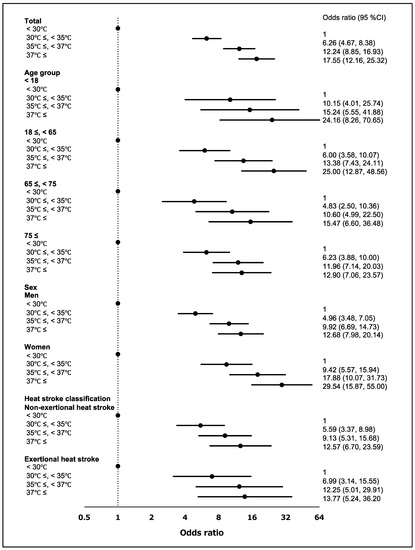
Figure 3.
Risk of developing a heat stroke by maximum air temperature and stratified by age, sex and heat stroke classification. The black dots mean the odds ratio. Numbers in parentheses are the 95% confidence intervals (95% CI).
3.3.2. Minimum Air Temperature
We investigated the risk of a heat stroke on days when the minimum air temperature exceeded 23 °C. The risk of a heat stroke increased when minimum air temperatures exceeded the reference temperature (<23 °C; Figure 4). The overall OR (95% CI) was 3.22 (2.58, 4.01) for 23–24.9 °C and 5.36 (4.30, 6.69) for ≥25 °C. When air temperatures were 23–25 °C, the risk of a heat stroke was higher in individuals aged 18–64 years and in women. The risk was higher in individuals who were at home at the time that the ambulance was called.
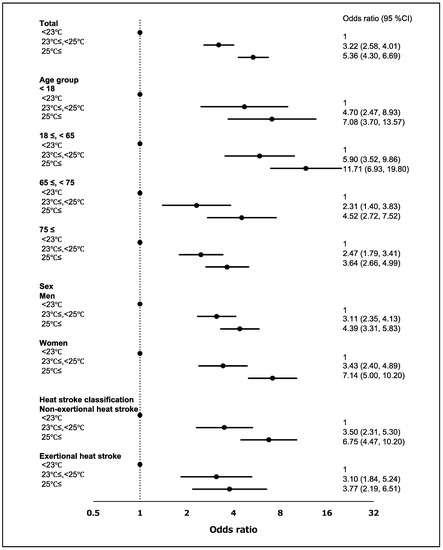
Figure 4.
Risk of developing a heat stroke by minimum air temperature and stratified by age, sex and heat stroke classification. The black dots mean the odds ratio. Numbers in parentheses are the 95% confidence intervals (95% CI).
3.4. Relationship between Air Temperature and Heat Stroke Severity
We investigated the risk analyzed heat stroke severity using two models (Table 5). In the first model, we used age, sex, maximum air temperature, relative humidity, a heat stroke occurring at home and a heat stroke associated with exercise as independent variables. In the second model, we replaced the maximum air temperature with a minimum air temperature. Only age was associated with the severity in either model (p < 0.001). Being at home when calling for medical transport showed a tendency toward association but did not reach statistical significance in either model (p = 0.070 and 0.098). Likewise, minimum temperatures showed a tendency toward association but did not reach statistical significance (p = 0.086).
Table 5.
Ordered logistic regression factors affecting the severity of a heat stroke.
4. Discussion
In the present study, we found that the daily minimum air temperature during summer may influence the incidence of a heat stroke. This effect does not exceed that of maximum temperatures but is probably not negligible. Typically, the lowest temperature of the day is often recorded around dawn and therefore high minimum temperatures are indicative of a hot night [40]. Higher nighttime temperatures have been reported to lead to sleep deprivation with the greatest impact seen in the summer months among low-income and elderly individuals [41]. Sleep deprivation has been cited as a risk factor for a heat stroke and research on the health effects of nighttime temperatures associated with global warming and the heat island phenomenon will become increasingly important [38].
We found that the risk of a non-exertional heat stroke when the minimum temperature was 25 °C or higher was approximately twice the risk associated with exercise. In general, a large temperature gradient during the day can exert adverse health effects such as mortality from cardiovascular disease, respiratory disease and stroke [18,42]. In contrast, cerebrovascular events in the summer have been reported to increase on days with smaller differences in air temperature or higher minimum air temperatures [19]. In the present study, we did not find a clear relationship between the temperature and the severity of the heat stroke, perhaps because the initial diagnosis could change and we had no information on the medical history and pre-existing conditions of cases. Although the number of cases in this study was small, the findings suggest that hot nights may be associated with the severity of heat strokes especially non-exertional heat strokes.
Japan has one of the highest percentages of older individuals in the world [43] and just over half (58%) of cases were aged 65 years and above in the present study. Therefore, we stratified those aged 65 years and over into two groups. The elderly are at a higher risk for heat strokes because of declining physiological and cognitive functions [43,44,45,46,47] and also in this study, the severity of the heat stroke was associated with older age. Furthermore, a non-exertional heat stroke is common in the elderly [48] who may not use air conditioning even if it is available [45,46,47]. The risk of a heat stroke associated with increasing temperatures was not as high as in the younger group presumably because the elderly are more vulnerable to environmental exposures even at temperatures below 30 °C.
We found that women were more susceptible to heat strokes than men especially when the maximum temperature was 37 °C or higher. This finding is supported by the literature [49]. A high body mass index is a risk factor for heat stroke [50] and women tend to have a higher body mass index than men [50,51]. However, there are no physical data on the subjects’ height or weight in our study and further research is needed to determine the relationship between heat strokes and body composition.
We only used the air temperature as a meteorological indicator in the case-crossover analysis and did not include relative humidity. Our previous study did not find an association with heat stroke transport [12] and we also found no association with heat stroke severity in the present study. One of the reasons is that the relative humidity in the target area remained extremely high in July and August. In fact, according to official data from the Japan Meteorological Agency, the average relative humidity ± standard deviation for the study period was 75.2 ± 8.6% at the Tottori observation site and 75.0 ± 9.2% at the Yonago observation site. Therefore, the effect of humidity may not have diminished. Although wet-bulb globe temperature (WBGT) [52] and apparent temperature (AT) [9,53] are standardized general indicators in the studies of heat strokes we did not use both because these calculations require data on relative humidity. In addition, radiant heat values are necessary for WBGT calculations [51] and wind-speed data for AT [54] but these values are very localized [55].
Several limitations should be noted. First, we have data on the location and time of the emergency transport; however, we do not know the exact location and time that the heat stroke developed. The heat stroke could have developed hours earlier and elsewhere in a few cases. We also did not use time series data of air temperatures but simply the daily minimum and maximum temperature data for analysis. It is likely that some of the highest temperatures may have been recorded after a heat stroke event. Moreover, the meteorological data were collected at representative locations, perhaps even 30 km from the location of the case, and therefore may not reflect the actual temperatures in each individual case. Second, ambulance transport data do not include heat stroke cases that arrived at emergency departments on their own. Third, the diagnosis of a heat stroke was made by a clinician at the time of the initial examination and may have ultimately been changed. Fourth, we had no access to the medical histories of cases, precluding the analysis of the influence of pre-existing conditions. As older individuals have more comorbidities, the risk in the elderly may be overestimated. However, ambulance transport data are frequently used because they are available and may be suitable for establishing a real-time surveillance system [56]. Finally, the use of a case-crossover design for statistical analysis may also be problematic [57,58]. It has been pointed out that this design has less power when compared with a Poisson regression analysis [57]. However, because the case-crossover design was thought to clear up the results of the subgroup analysis, we used this method in current study [57]. For a more detailed and universal assessment of environmental influences on the incidence of heat strokes, the effect of a lag in the day or two days before calling an ambulance, actual morbidity and post-hospitalization outcomes as well as the socioeconomic background of patients should be included in analyses.
5. Conclusions
Higher minimum and maximum daily temperatures are associated with the incidence of heat strokes in the summer, especially non-exertional heat strokes.
Author Contributions
Conceptualization, S.O. and Y.K.; methodology, S.O. and Y.K.; validation, S.O., Y.K., S.F.I., T.M. and H.A.; formal analysis, S.O.; investigation, S.F.I., T.M. and H.A.; resources, S.O.; data curation, S.O.; writing (original draft preparation), S.O.; writing (review and editing), S.O.; visualization, S.O.; supervision, Y.K.; project administration, S.O. and Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Tottori University Ethics Committee (No. 180626-069, 16 October 2019).
Informed Consent Statement
Informed consent was obtained in the form of opt-out on the web-site/posting in Tottori Prefectural Office.
Data Availability Statement
The data presented in this study are available on request from authors.
Acknowledgments
Ambulance transport data in this study were provided by the Department of Health and Welfare of the Tottori Prefectural Government.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Epstein, Y.; Yanovich, R. Heatstroke. N. Engl. J. Med. 2019, 380, 2449–2459. [Google Scholar] [CrossRef]
- Ministry of the Environment, Guidelines for Heat Stroke Prevention at Summer Events 2020. Available online: https://www.wbgt.env.go.jp/pdf/gline/heatillness_guideline_full.pdf (accessed on 22 September 2020). (In Japanese)
- Kodera, S.; Nishimura, T.; Rashed, E.A.; Hasegawa, K.; Takeuchi, I.; Egawa, R.; Hirata, A. Estimation of heat-related morbidity from weather data: A computational study in three prefectures of Japan over 2013–2018. Environ. Int. 2019, 130, 104907. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC), Climate Change 2014: Synthesis Report. Available online: https://www.ipcc.ch/report/ar5/syr/ (accessed on 22 September 2020).
- Li, D.W.; Yuan, J.C.; Kopp, R.E. Escalating global exposure to compound heat-humidity extremes with warming. Environ. Res. Lett. 2020, 15. [Google Scholar] [CrossRef]
- Miyatake, N.; Nakao, M.; Sakano, N.; Suna, S.; Suzue, T.; Hirao, T. Higher Temperatures Were Closely Associated with Higher Ambulance Transports in Takamatsu Area, Japan. J. Environ. Prot. 2011, 2, 72–75. [Google Scholar] [CrossRef]
- Miyatake, N.; Sakano, N.; Murakami, S. The relation between ambulance transports stratified by heat stroke and air temperature in all 47 prefectures of Japan in August, 2009: Ecological study. Environ. Health Prev. Med. 2012, 17, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Miyatake, N.; Sakano, N.; Murakami, S. The relation between ambulance transports due to heat stroke and air temperature using daily data in Okayama prefecture, Japan. Open J. Prev. Med. 2012, 2, 112–115. [Google Scholar] [CrossRef]
- Ng, C.F.; Ueda, K.; Ono, M.; Nitta, H.; Takami, A. Characterizing the effect of summer temperature on heatstroke-related emergency ambulance dispatches in the Kanto area of Japan. Int. J. Biometeorol. 2014, 58, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Akahane, M.; Imamura, T. Impact of Temperature in Summer on Emergency Transportation for Heat-Related Diseases in Japan. Chin. Med. J. 2018, 131, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, C.; Luo, S.; He, J.; Cheng, Y.; Jin, Y. Impacts of extremely high temperature and heatwave on heatstroke in Chongqing, China. Environ. Sci. Pollut. Res. Int. 2017, 24, 8534–8540. [Google Scholar] [CrossRef]
- Fujitani, Y.; Otani, S.; Majbauddin, A.; Amano, H.; Masumoto, T.; Kurozawa, Y. Impact of Maximum Air Temperature on Ambulance Transports Owing to Heat Stroke During Spring and Summer in Tottori Prefecture, Japan: A Time-stratified Case-crossover Analysis. Yonago Acta Med. 2019, 62, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Patz, J.A.; Campbell-Lendrum, D.; Holloway, T.; Foley, J.A. Impact of regional climate change on human health. Nature 2005, 438, 310–317. [Google Scholar] [CrossRef]
- Mohajerani, A.; Bakaric, J.; Jeffrey-Bailey, T. The urban heat island effect, its causes, and mitigation, with reference to the thermal properties of asphalt concrete. J. Environ. Manag. 2017, 197, 522–538. [Google Scholar] [CrossRef] [PubMed]
- Heaviside, C.; Macintyre, H.; Vardoulakis, S. The Urban Heat Island: Implications for Health in a Changing Environment. Curr. Environ. Health Rep. 2017, 4, 296–305. [Google Scholar] [CrossRef]
- Japan Meteorological Agency, Heat Island Monitoring Report 2017. Available online: https://www.data.jma.go.jp/cpdinfo/himr/h30/himr_2017.pdf (accessed on 22 September 2020). (In Japanese)
- Ministry of the Environment, Heat Island Measures Manual. Available online: https://www.env.go.jp/air/life/heat_island/manual_01/01_chpt1-1.pdf (accessed on 22 September 2020).
- Cheng, J.; Xu, Z.; Zhu, R.; Wang, X.; Jin, L.; Song, J.; Su, H. Impact of diurnal temperature range on human health: A systematic review. Int. J. Biometeorol. 2014, 58, 2011–2024. [Google Scholar] [CrossRef]
- Vered, S.; Paz, S.; Negev, M.; Tanne, D.; Zucker, I.; Weinstein, G. High ambient temperature in summer and risk of stroke or transient ischemic attack: A national study in Israel. Environ. Res. 2020, 187, 109678. [Google Scholar] [CrossRef]
- Hausfater, P.; Megarbane, B.; Dautheville, S.; Patzak, A.; Andronikof, M.; Santin, A.; Andre, S.; Korchia, L.; Terbaoui, N.; Kierzek, G.; et al. Prognostic factors in non-exertional heatstroke. Intensive Care Med. 2010, 36, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Alele, F.O.; Malau-Aduli, B.S.; Malau-Aduli, A.E.O.; Crowe, M.J. Epidemiology of Exertional Heat Illness in the Military: A Systematic Review of Observational Studies. Int. J. Environ. Res. Public Health 2020, 17, 7037. [Google Scholar] [CrossRef]
- Yeargin, S.W.; Dompier, T.P.; Casa, D.J.; Hirschhorn, R.M.; Kerr, Z.Y. Epidemiology of Exertional Heat Illnesses in National Collegiate Athletic Association Athletes During the 2009–2010 Through 2014–2015 Academic Years. J. Athl. Train. 2019, 54, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Portal Site of Official Statistic of Japan, Population Concentration Areas of Each Prefecture, Ministry of Internal Affairs and Communications. Available online: https://www.e-stat.go.jp/dbview?sid=0003413758 (accessed on 18 October 2020). (In Japanese)
- Portal Site of Official Statistic of Japan, Number and percentage of consumer goods owned per 1,000 households by prefecture, Ministry of Internal Affairs and Communications. Available online: https://www.e-stat.go.jp/dbview?sid=0003108720 (accessed on 18 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2019. Available online: https://www.fdma.go.jp/disaster/heatstroke/items/heatstroke004_houdou01.pdf (accessed on 16 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2018. Available online: https://www.fdma.go.jp/disaster/heatstroke/item/heatstroke003_houdou01.pdf (accessed on 16 October 2020). (In Japanese)
- Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, Heat Stroke Emergency Report for 2017. Available online: https://www.fdma.go.jp/disaster/heatstroke/item/heatstroke001_houdou_01.pdf (accessed on 16 October 2020). (In Japanese)
- World Health Organization, ICD-10 Version: 2019. Available online: https://icd.who.int/browse10/2019/en#/T67.0 (accessed on 17 October 2020).
- Yamamoto, T.; Fujita, M.; Oda, Y.; Todani, M.; Hifumi, T.; Kondo, Y.; Shimazaki, J.; Shiraishi, S.; Hayashida, K.; Yokobori, S.; et al. Evaluation of a Novel Classification of Heat-Related Illnesses: A Multicentre Observational Study (Heat Stroke STUDY 2012). Int. J. Environ. Res. Public Health 2018, 15, 1962. [Google Scholar] [CrossRef]
- Luo, X.; Sorock, G.S. Analysis of recurrent event data under the case-crossover design with applications to elderly falls. Stat. Med. 2008, 27, 2890–2901. [Google Scholar] [CrossRef] [PubMed]
- Byrwa-Hill, B.M.; Venkat, A.; Presto, A.A.; Rager, J.R.; Gentile, D.; Talbott, E. Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region. Int. J. Environ. Res. Public Health 2020, 17, 8619. [Google Scholar] [CrossRef] [PubMed]
- Contiero, P.; Boffi, R.; Tagliabue, G.; Scaburri, A.; Tittarelli, A.; Bertoldi, M.; Borgini, A.; Favia, I.; Ruprecht, A.A.; Maiorino, A.; et al. A Case-Crossover Study to Investigate the Effects of Atmospheric Particulate Matter Concentrations, Season, and Air Temperature on Accident and Emergency Presentations for Cardiovascular Events in Northern Italy. Int. J. Environ. Res. Public Health 2019, 16, 4627. [Google Scholar] [CrossRef]
- Parry, M.; Green, D.; Zhang, Y.; Hayen, A. Does Particulate Matter Modify the Short-Term Association between Heat Waves and Hospital Admissions for Cardiovascular Diseases in Greater Sydney, Australia? Int. J. Environ. Res. Public Health 2019, 16, 3270. [Google Scholar] [CrossRef]
- Zhang, P.; Wiens, K.; Wang, R.; Luong, L.; Ansara, D.; Gower, S.; Bassil, K.; Hwang, S.W. Cold Weather Conditions and Risk of Hypothermia Among People Experiencing Homelessness: Implications for Prevention Strategies. Int. J. Environ. Res. Public Health 2019, 16, 3259. [Google Scholar] [CrossRef] [PubMed]
- Yorifuji, T.; Suzuki, E.; Kashima, S. Hourly differences in air pollution and risk of respiratory disease in the elderly: A time-stratified case-crossover study. Environ. Health 2014, 13, 67. [Google Scholar] [CrossRef]
- Basu, R.; Dominici, F.; Samet, J.M. Temperature and mortality among the elderly in the United States: A comparison of epidemiologic methods. Epidemiology 2005, 16, 58–66. [Google Scholar] [CrossRef]
- Spector, J.T.; Bonauto, D.K.; Sheppard, L.; Busch-Isaksen, T.; Calkins, M.; Adams, D.; Lieblich, M.; Fenske, R.A. A Case-Crossover Study of Heat Exposure and Injury Risk in Outdoor Agricultural Workers. PLoS ONE 2016, 11, e0164498. [Google Scholar] [CrossRef]
- Westwood, C.S.; Fallowfield, J.L.; Delves, S.K.; Nunns, M.; Ogden, H.B.; Layden, J.D. Individual risk factors associated with exertional heat illness: A systematic review. Exp. Physiol. 2020. [Google Scholar] [CrossRef]
- Iriki, M.; Simon, E. Heat disorder in Yamanashi Prefecture during the summer from 1995 to 2004. Ind. Health 2006, 44, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Japan Meteorological Agency, Terms Used in Weather Forecasting, etc. Available online: https://www.jma.go.jp/jma/kishou/know/yougo_hp/kion.html (accessed on 22 September 2020). (In Japanese)
- Obradovich, N.; Migliorini, R.; Mednick, S.C.; Fowler, J.H. Nighttime temperature and human sleep loss in a changing climate. Sc.i Adv. 2017, 3, e1601555. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhou, M.; Li, M.; Yin, P.; Wang, B.; Pilot, E.; Liu, Y.; van der Hoek, W.; van Asten, L.; Krafft, T.; et al. Diurnal temperature range in relation to death from stroke in China. Environ. Res 2018, 164, 669–675. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Ageing 2019. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf (accessed on 23 September 2020).
- Leyk, D.; Hoitz, J.; Becker, C.; Glitz, K.J.; Nestler, K.; Piekarski, C. Health Risks and Interventions in Exertional Heat Stress. Dtsch. Arztebl. Int. 2019, 116, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Kondo, M.; Ono, M.; Nakazawa, K.; Kayaba, M.; Minakuchi, E.; Sugimoto, K.; Honda, Y. Population at high-risk of indoor heatstroke: The usage of cooling appliances among urban elderlies in Japan. Environ. Health Prev. Med. 2013, 18, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Khare, S.; Hajat, S.; Kovats, S.; Lefevre, C.E.; de Bruin, W.B.; Dessai, S.; Bone, A. Heat protection behaviour in the UK: Results of an online survey after the 2013 heatwave. BMC Public Health 2015, 15, 878. [Google Scholar] [CrossRef]
- Kravchenko, J.; Abernethy, A.P.; Fawzy, M.; Lyerly, H.K. Minimization of heatwave morbidity and mortality. Am. J. Prev. Med. 2013, 44, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Aruga, T.; Inoue, K.; Okudera, H.; KItahara, T.; Shimazaki, S.; Tsuruta, R.; Maekawa, T.; Yokota, H. The characteristics of classical heatstroke in Japan. Jpn. J. Intensive Care Med. 2009, 33, 309–315. (In Japanese) [Google Scholar]
- Alele, F.; Malau-Aduli, B.; Malau-Aduli, A.; Crowe, M. Systematic review of gender differences in the epidemiology and risk factors of exertional heat illness and heat tolerance in the armed forces. BMJ Open 2020, 10, e031825. [Google Scholar] [CrossRef] [PubMed]
- Chung, N.K.; Pin, C.H. Obesity and the occurrence of heat disorders. Mil. Med. 1996, 161, 739–742. [Google Scholar] [CrossRef] [PubMed]
- Nutong, R.; Mungthin, M.; Hatthachote, P.; Ukritchon, S.; Imjaijit, W.; Tengtrakulcharoen, P.; Panichkul, S.; Putwatana, P.; Prapaipanich, W.; Rangsin, R. Personal risk factors associated with heat-related illness among new conscripts undergoing basic training in Thailand. PLoS ONE 2018, 13, e0203428. [Google Scholar] [CrossRef] [PubMed]
- Budd, G.M. Wet-bulb globe temperature (WBGT—Its history and its limitations. J. Sci. Med. Sport 2008, 11, 20–32. [Google Scholar] [CrossRef]
- Harlan, S.L.; Chowell, G.; Yang, S.; Petitti, D.B.; Morales Butler, E.J.; Ruddell, B.L.; Ruddell, D.M. Heat-related deaths in hot cities: Estimates of human tolerance to high temperature thresholds. Int. J. Environ. Res. Public Health 2014, 11, 3304–3326. [Google Scholar] [CrossRef] [PubMed]
- Steadman, R.G. The Assessment of Sultriness. Part I: A Temperature-Humidity Index Based on Human Physiology and Clothing Science. J. Appl. Meteorol. 1979, 18, 861–873. [Google Scholar] [CrossRef]
- Parsons, K. Heat stress Standard ISO 7243 and its global application. Ind. Health 2006, 44, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Zauli Sajani, S.; Scotto, F.; Miglio, R.; Marchesi, S.; Lauriola, P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia-Romagna, Italy. Environ. Res. 2011, 111, 1192–1200. [Google Scholar] [CrossRef]
- Peters, A.; von Klot, S.; Berglind, N.; Hormann, A.; Lowel, H.; Nyberg, F.; Pekkanen, J.; Perucci, C.A.; Stafoggia, M.; Sunyer, J.; et al. Comparison of different methods in analyzing short-term air pollution effects in a cohort study of susceptible individuals. Epidemiol. Perspect. Innov. 2006, 3, 10. [Google Scholar] [CrossRef] [PubMed]
- Lumley, T.; Levy, D. Bias in the case-crossover design: Implications for studies of air pollution. Environmetrics 2000, 11, 689–704. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).