
Comparative Performance Testing of Respirator versus Surgical Mask Using a Water Droplet Spray Model

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Test Set-Up
2.2. TIL Testing Procedure
2.3. Statistical Analysis
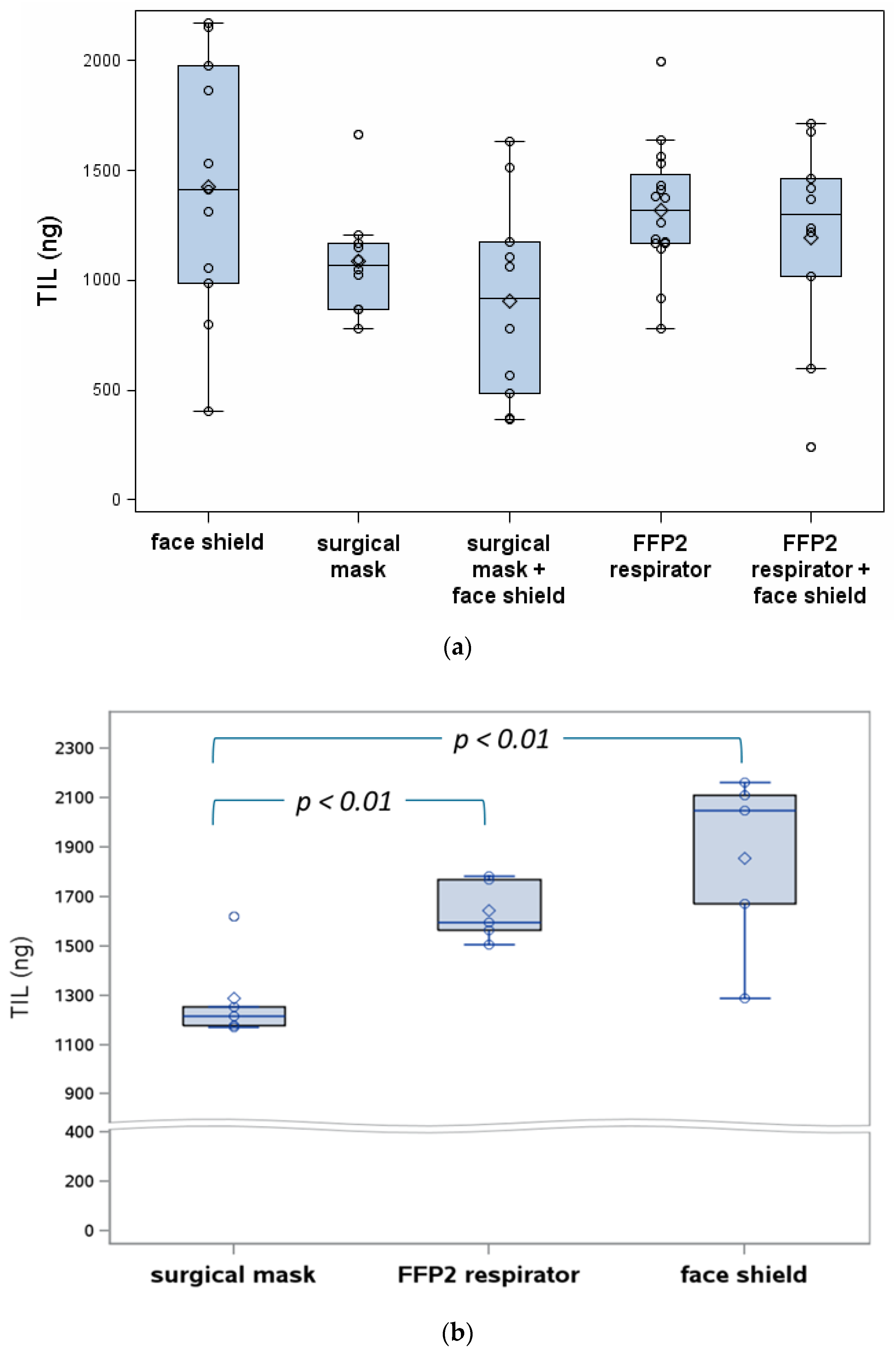
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Advice on the Use of Masks in the Context of COVID-19. Interim Guidance. 2020. Available online: https://www.who.int/publications/i/item/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak (accessed on 4 January 2021).
- Guo, Z.D.; Wang, Z.Y.; Zhang, S.F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.B.; Dong, Y.Z.; Chi, X.Y.; et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Qi, X.; Chen, H.; Li, X.; Zhang, Z.; Wang, H.; Sun, L.; Zhang, L.; Guo, J.; Morawska, L.; et al. COVID-19 patients in earlier stages exhaled millions of SARS-CoV-2 per hour. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Zhou, L.; Yao, M.; Zhang, X.; Hu., B.; Li., X.; Chen, H.; Zhang, L.; Liu, Y.; Du, M.; Sun, B.; et al. Breath-, air- and surface-borne SARS-CoV-2 in hospitals. J. Aerosol. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Fears, A.C.; Klimstra, W.B.; Duprex, P.; Hartman, A.; Weaver, S.C.; Plante, K.S.; Mirchandani, D.; Plante, J.A.; Aguilar, P.V.; Fernández, D.; et al. Persistence of Severe Acute Respiratory Syndrome Coronavirus 2 in Aerosol Suspensions. Emerg. Infect. Dis. 2020, 26, 2168–2171. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D. Is the coronavirus airborne? Experts can’t agree. Nature 2020, 580, 175. [Google Scholar] [CrossRef] [PubMed]
- Conly, J.; Seto, W.H.; Pittet, D.; Holmes, A.; Chu, M.; Hunter, P.R. WHO Infection Prevention and Control Research and Development Expert Group for COVID-19. Correction to: Use of medical face masks versus particulate respirators as a component of personal protective equipment for health care workers in the context of the COVID-19 pandemic. Antimicrob. Resist. Infect. Control 2020, 9, 151. [Google Scholar] [CrossRef] [PubMed]
- EN 149:2001+A1:2009 Respiratory Protective Devices—Filtering Half Masks to Protect against Particles—Requirements, Testing, Marking; European Committee for Standardization: Brussels, Belgium, 2009.
- Centers of Disease Control and Prevention (2019) Respiratory Protective Devices, NIOSH 42 CFR Part 84; The National Personal Protective Technology Laboratory (NPPTL): Atlanta, GA, USA, 2019.
- Bartoszko, J.J.; Farooqi, M.A.M.; Alhazzani, W.; Loeb, M. Medical masks vs. N95 respirators for preventing COVID-19 in healthcare workers: A systematic review and meta-analysis of randomized trials. Influ. Other Respir. Viruses 2020, 14, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Long, Y.; Hu, T.; Liu, L.; Chen, R.; Guo, Q.; Yang, L.; Cheng, Y.; Huang, J.; Du, L. Effectiveness of N95 respirators versus surgical masks against influenza: A systematic review and meta-analysis. J. Evid. Based Med. 2020, 13, 93–101. [Google Scholar] [CrossRef] [PubMed]
- EN 13274-7:2019 Respiratory Protective Devices—Methods of Test—Part 7: Determination of Particle Filter Penetration; European Committee for Standardization: Brussels, Belgium, 2019.
- EN 14683:2019 Medical Face Masks—Requirements and Test Methods; European Committee for Standardization: Brussels, Belgium, 2019.
- Scheepers, P.T.J.; Godderis, L. Detect and re-assess impact of chemicals on health and environment during post-market evaluation. Environ. Res. 2019, 178, 108728. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Type | European Standard | Testing Substance | Particle Size (µm) | Filter Penetration | Bacterial Filtration Efficiency |
|---|---|---|---|---|---|
| N95 | NIOSH 42 CFR Part 84 [10] | NaCl | 0.3 | <5% | - |
| FFP2 | EN 13274-7: 2019 [13] | NaCl | 0.6 | <6% | - |
| Paraffine | 0.3 | <6% | - | ||
| Surgical mask (IIR) 1 | EN 14683: 2019 [14] | Staphylococcus aureus | 3.0 ± 0.3 | - | ≥98% |
| Parameter | Particle Size Distribution by Volume (µm) | |
|---|---|---|
| 30 cm (N = 4) | 60 cm (N = 4) | |
| Minimum | 1.2 ± 0.2 | 1.0 ± 0.1 |
| 10th percentile (P10) | 29 ± 1.3 | 25 ± 0.5 |
| Median (P50) | 76 ± 12 | 53 ± 2.1 |
| 90th percentile (P90) | 226 ± 40 | 167 ± 52 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheepers, P.T.J.; Wertheim, H.F.L.; van Dael, M.; Anzion, R.; Holterman, H.J.; Teerenstra, S.; de Groot, M.; Voss, A.; Hopman, J. Comparative Performance Testing of Respirator versus Surgical Mask Using a Water Droplet Spray Model. Int. J. Environ. Res. Public Health 2021, 18, 1599. https://doi.org/10.3390/ijerph18041599
Scheepers PTJ, Wertheim HFL, van Dael M, Anzion R, Holterman HJ, Teerenstra S, de Groot M, Voss A, Hopman J. Comparative Performance Testing of Respirator versus Surgical Mask Using a Water Droplet Spray Model. International Journal of Environmental Research and Public Health. 2021; 18(4):1599. https://doi.org/10.3390/ijerph18041599
Chicago/Turabian StyleScheepers, Paul T. J., Heiman F. L. Wertheim, Maurice van Dael, Rob Anzion, Henk Jan Holterman, Steven Teerenstra, Martijn de Groot, Andreas Voss, and Joost Hopman. 2021. "Comparative Performance Testing of Respirator versus Surgical Mask Using a Water Droplet Spray Model" International Journal of Environmental Research and Public Health 18, no. 4: 1599. https://doi.org/10.3390/ijerph18041599
APA StyleScheepers, P. T. J., Wertheim, H. F. L., van Dael, M., Anzion, R., Holterman, H. J., Teerenstra, S., de Groot, M., Voss, A., & Hopman, J. (2021). Comparative Performance Testing of Respirator versus Surgical Mask Using a Water Droplet Spray Model. International Journal of Environmental Research and Public Health, 18(4), 1599. https://doi.org/10.3390/ijerph18041599