
Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy

 ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Saliva Sampling
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bildt, M.M.; Bloemen, M.; Kuijpers-Jagtman, A.M.; Von den Hoff, J.W. Matrix metalloproteinases and tissue inhibitors of metalloproteinases in gingival crevicular fluid orthodontic tooth movement. Eur. J. Orthod. 2009, 31, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Meeran, N.A. Cellular response within the periodontal ligament on application of orthodontic forces. J. Indian Soc. Periodontol. 2013, 17, 16–20. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Cordasco, G.; Perillo, L.; Ramaglia, L. Mechanobiology of the tooth movement during the orthodontic treatment: A literature review. Minerva Stomatol. 2016, 65, 299–327. [Google Scholar]
- Xu, X.; Zhang, Q.; Lv, Y.; Yu, T.; Chen, J.; Zeng, P.; Wang, L.; Liu, T.; Diao, H. Levels of matrix metalloproteinases in saliva during orthodontic tooth movement. Int. J. Clin. Exp. Med. 2020, 13, 1564–1571. [Google Scholar]
- Snoek-Van Beurden, P.A.M.; Von den Hoff, J.W. Zymographic techniques for the analysis of matrix metalloproteinases and their inhibitors. Biotechniques 2005, 38, 73–83. [Google Scholar] [CrossRef]
- Ejeil, A.-L.; Igondjo-Tchen, S.; Ghomrasseni, S.; Pellat, B.; Godeau, G.; Gogly, B. Expression of Matrix Metalloproteinases (MMPs) and Tissue Inhibitors of Metalloproteinases (TIMPs) in Healthy and Diseased Human Gingiva. J. Periodontol. 2003, 74, 188–195. [Google Scholar] [CrossRef]
- Ingman, T.; Apajalahti, S.; Mäntylä, P.; Savolainen, P.; Sorsa, T. Matrix metalloproteinase-1 and -8 in gingival crevicular fluid during orthodontic tooth movement: A pilot study during 1 month of follow-up after fixed appliance activation. Eur. J. Orthod. 2005, 27, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Holliday, L.S.; Vakani, A.; Archer, L.; Dolce, C. Effects of matrix metalloproteinase inhibitors on bone resorption and orthodontic tooth movement. J. Dent. Res. 2003, 82, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Apajalahti, S.; Sorsa, T.; Ingman, T. Matrix Metalloproteinase-2, -8, -9, and -13 in Gingival Crevicular Fluid of Short Root Anomaly Patients. Eur. J. Orthod. 2003, 25, 365–369. [Google Scholar] [CrossRef][Green Version]
- Hanemaaijer, R.; Sorsa, T.; Konttinen, Y.T.; Ding, Y.; Sutinen, M.; Visser, H.; van Hinsbergh, V.W.; Helaakoski, T.; Kainulainen, T.; Rönkä, H.; et al. Matrix metalloproteinase-8 Is Expressed in Rheumatoid Synovial Fibroblasts and Endothelial Cells. Regulation by Tumor Necrosis Factor-Alpha and Doxycycline. J. Biol. Chem. 1997, 272, 31504–31509. [Google Scholar] [CrossRef] [PubMed]
- Hasty, K.A.; Jeffrey, J.J.; Hibbs, M.S.; Welgus, H.G. The collagen substrate specificity of human neutrophil collagenase. J. Biol. Chem. 1987, 262, 10048–10052. [Google Scholar] [CrossRef]
- Haas, A.N.; Pannuti, C.M.; Andrade, A.K.P.; Escobar, E.C.; de Almeida, E.R.; Costa, F.O.; Cortelli, J.R.; Cortelli, S.C.; Rode, S.d.M.; Pedrazzi, V.; et al. Mouthwashes for the control of supragingival biofilm and gingivitis in orthodontic patients: Evidence-based recommendations for clinicians. Braz. Oral Res. 2014, 28, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Botero, J.E.; Rösing, C.K.; Duque, A.; Jaramillo, A.; Contreras, A. Periodontal Disease in Children and Adolescents of Latin America. Periodontology 2000 2015, 67, 34–57. [Google Scholar] [CrossRef] [PubMed]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar] [PubMed]
- Mühlemann, H.R.; Son, S. Gingival sulcus bleeding-a leading symptom in initial gingivitis. Helv. Odontol. Acta 1971, 15, 107–113. [Google Scholar] [PubMed]
- Greenstein, G.; Caton, J.; Polson, A.M. Histologic characteristics associated with bleeding after probing and visual signs of inflammation. J. Periodontol. 1981, 52, 420–425. [Google Scholar] [CrossRef]
- Schätzle, M.; Löe, H.; Bürgin, W.; Anerud, A.; Boysen, H.; Lang, N.P. Clinical course of chronic periodontitis. I. Role of gingivitis. J. Clin. Periodontol. 2003, 30, 887–901. [Google Scholar] [CrossRef] [PubMed]
- Al-Anezi, S.A. The effect of orthodontic bands or tubes upon periodontal status during the initial phase of orthodontic treatment. Saudi Dent. J. 2014, 27, 120–124. [Google Scholar] [CrossRef]
- Sebbar, M.; Abidine, Z.; Laslami, N.; Bentahar, Z. Periodontal Health and Orthodontics. In Emerging Trends in Oral Health Sciences and Dentistry; Virdi, M.S., Ed.; IntechOpen: London, UK, 2015; Volume 32, pp. 717–732. [Google Scholar] [CrossRef]
- Lijian, L. Periodontic-orthodontic interactions—Rationale, sequence and clinical implications. Hong Kong Dent. J. 2007, 4, 60–64. [Google Scholar]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Clin. Periodontol. 2018, 45, S44–S67. [Google Scholar] [CrossRef]
- Dannan, A. An update on periodontic-orthodontic interrelationships. J. Indian Soc. Periodontol. 2010, 14, 66–71. [Google Scholar] [CrossRef]
- Preoteasa, C.T.; Ionescu, E.; Preoteasa, E. Risks and Complications Associated with Orthodontic Treatment. In Orthodontics-Basic Aspects and Clinical Considerations; Bourzgui, F., Ed.; IntechOpen: London, UK, 2012; Volume 18, pp. 403–428. [Google Scholar] [CrossRef][Green Version]
- Van Gastel, J.; Quirynen, M.; Teughels, W.; Coucke, W.; Carels, C. Longitudinal changes in microbiology and clinical periodontal parameters after removal of fixed orthodontic appliances. Eur. J. Orthod. 2011, 33, 15–21. [Google Scholar] [CrossRef]
- Mattingly, J.A.; Sauer, G.J.; Yancey, J.M.; Arnold, R.R. Enhancement of Streptococcus Mutans Colonization by Direct Bonded Orthodontic Appliances. J. Dent. Res. 1983, 62, 1209–1211. [Google Scholar] [CrossRef]
- Perinetti, G.; Paolantonio, M.; Serra, E.; D’Archivio, D.; D’Ercole, S.; Festa, F.; Spoto, G. Longitudinal Monitoring of Subgingival Colonization by Actinobacillus Actinomycetemcomitans, and Crevicular Alkaline Phosphatase and Aspartate Aminotransferase Activities Around Orthodontically Treated Teeth. J. Clin. Periodontol. 2004, 31, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C. Periodontal disease diagnosis: Current status and future developments. J. Dent. 1997, 25, 3–15. [Google Scholar] [CrossRef]
- Lang, N.P.; Adler, R.; Joss, A.; Nyman, S. Absence of bleeding on probing. An indicator of periodontal stability. J. Clin. Periodontol. 1990, 17, 714–721. [Google Scholar] [CrossRef]
- Daly, C.G.; Mitchell, D.H.; Highfield, J.E.; Grossberg, D.E.; Stewart, D. Bacteremia Due to Periodontal Probing: A Clinical and Microbiological Investigation. J. Periodontol. 2001, 72, 210–214. [Google Scholar] [CrossRef]
- Galgut, P. A comparison of different indices used in the clinical assessment of plaque and gingival bleeding. Clin. Oral Investig. 1999, 3, 96–99. [Google Scholar] [CrossRef]
- Lang, N.P.; Joss, A.; Orsanic, T.; Gusberti, F.A.; Siegrist, B.E. Bleeding on probing. A predictor for the progression of periodontal disease. J. Clin. Periodontol. 1986, 13, 590–596. [Google Scholar] [CrossRef]
- Giannobile, W.V.; Beikler, T.; Kinney, J.S.; Ramseier, C.A.; Morelli, T.; Wong, D.T. Saliva as a diagnostic tool for periodontal disease: Current state and future directions. Periodontology 2000 2009, 50, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Buduneli, N.; Kinane, D.F. Host-derived diagnostic markers related to soft tissue destruction and bone degradation in periodontitis. J. Clin. Periodontol. 2011, 38, 85–105. [Google Scholar] [CrossRef] [PubMed]
- Armitage, C.G. The complete periodontal examination. Periodontology 2000 2004, 34, 22–23. [Google Scholar] [CrossRef] [PubMed]
- Bardal, P.A.P.; Olympio, K.P.K.; Bastos, J.R.M.; Henriques, J.F.C.; Buzalaf, M.A.R. Education and motivation in oral health-preventing disease and promoting health in patients undergoing orthodontic treatment. Dent. Press J. Orthod. 2011, 16, 95–102. [Google Scholar] [CrossRef]
- Sorsa, T.; Tjäderhane, L.; Konttinen, Y.T.; Lauhio, A.; Salo, T.; Lee, H.; Golub, L.M.; Brown, D.L.; Mäntylä, P. Matrix metalloproteinases: Contribution to pathogenesis, diagnosis and treatment of periodontal inflammation. Ann. Med. 2006, 38, 306–321. [Google Scholar] [CrossRef]
- Sorsa, T.; Gürsoy, U.K.; Nwhator, S.; Hernandez, M.; Tervahartiala, T.; Leppilahti, J.; Gursoy, M.; Könönen, E.; Emingil, G.; Pussinen, P.J.; et al. Analysis of Matrix Metalloproteinases, Especially MMP-8, in Gingival Creviclular Fluid, Mouthrinse and Saliva for Monitoring Periodontal Diseases. Periodontology 2000 2016, 70, 142–163. [Google Scholar] [CrossRef]
- Boșca, A.B.; Miclăuş, V.; Raţiu, C.; Melincovici, C. Matrix metalloproteinase-8—A Salivary diagnostic biomarker related to soft tissue destruction in chronic periodontitis. Ann. Rom. Soc. Cell Biol. 2012, 17, 251–257. [Google Scholar]
- Rai, B.; Kharb, S.; Jain, R.; Anand, S.C. Biomarkers of periodontitis in oral fluids. J. Oral Sci. 2008, 50, 53–56. [Google Scholar] [CrossRef]
- Sexton, W.M.; Lin, Y.; Kryscio, R.J.; Dawson, D.R., III; Ebersole, J.L.; Miller, C.S. Salivary biomarkers of periodontal disease in response to treatment. J. Clin. Periodontol. 2011, 38, 434–441. [Google Scholar] [CrossRef]
- Kushlinskii, N.E.; Solovykh, E.A.; Karaoglanova, T.B. Content of matrix metalloproteinase-8 and matrix metalloproteinase-9 in oral fluid of patients with chronic generalized periodontitis. Bull. Exp. Biol. Med. 2011, 152, 240–244. [Google Scholar] [CrossRef]
- Gursoy, U.K.; Kononen, E.; Pradhan-Palikhe, P.; Tervahartiala, T.; Pussinen, P.J.; Suominen-Taipale, L.; Sorsa, T. Salivary MMP-8, TIMP-1, and ICTP as markers of advanced periodontitis. J. Clin. Periodontol. 2010, 37, 487–493. [Google Scholar] [CrossRef]
- De Morais, E.F.; Pinheiro, J.C.; Leite, R.B.; Santos, P.P.A.; Barboza, C.A.G.; Freitas, R.A. Matrix metalloproteinase-8 levels in periodontal disease patients: A systematic review. J. Periodontal Res. 2018, 53, 156–163. [Google Scholar] [CrossRef]
- Mantyla, P.; Stenman, M.; Kinane, D.F.; Salo, T.; Suomalainen, K.; Tikanoja, S.; Sorsa, T. Monitoring periodontal disease status in smokers and nonsmokers using a gingival crevicular fluid matrix metalloproteinase-8-specific chair-side test. J. Periodontal Res. 2006, 41, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Rios, P.; Hernandez, M.; Garrido, M.; Tervahartiala, T.; Leppilahti, J.; Kuula, H.; Heikkinen, A.M.; Mäntylä, P.; Rathnayake, N.; Nwhator, S.; et al. Oral fluid matrix metalloproteinase (MMP)-8 as a diagnostic tool in chronic periodontitis. Met. Med. 2016, 3, 11–18. [Google Scholar] [CrossRef]
- Shirozaki, M.U.; da Silva, R.A.B.; Romano, F.L. Clinical, microbiological, and immunological evaluation of patients in corrective orthodontic treatment. Prog. Orthod. 2020, 21, 6. [Google Scholar] [CrossRef] [PubMed]
- Mantyla, P.; Stenman, M.; Kinane, D.F.; Tikanoja, S.; Luoto, H.; Salo, T.; Sorsa, T. Gingival crevicular fluid collagenase-2 (MMP-8) test stick for chair-side monitoring of periodontitis. J. Periodontal Res. 2003, 38, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Marcaccini, A.M.; Novaes, A.B., Jr.; Meschiari, C.A.; Souza, S.L.; Palioto, D.B.; Sorgi, C.A.; Faccioli, L.H.; Tanus-Santos, J.E.; Gerlach, R.F. Circulating matrix metalloproteinase-8 (MMP-8) and MMP-9 are increased in chronic periodontal disease and decrease after non-surgical periodontal therapy. Clin. Chim. Acta 2009, 409, 117–122. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean (±Standard Deviation) |
|---|---|
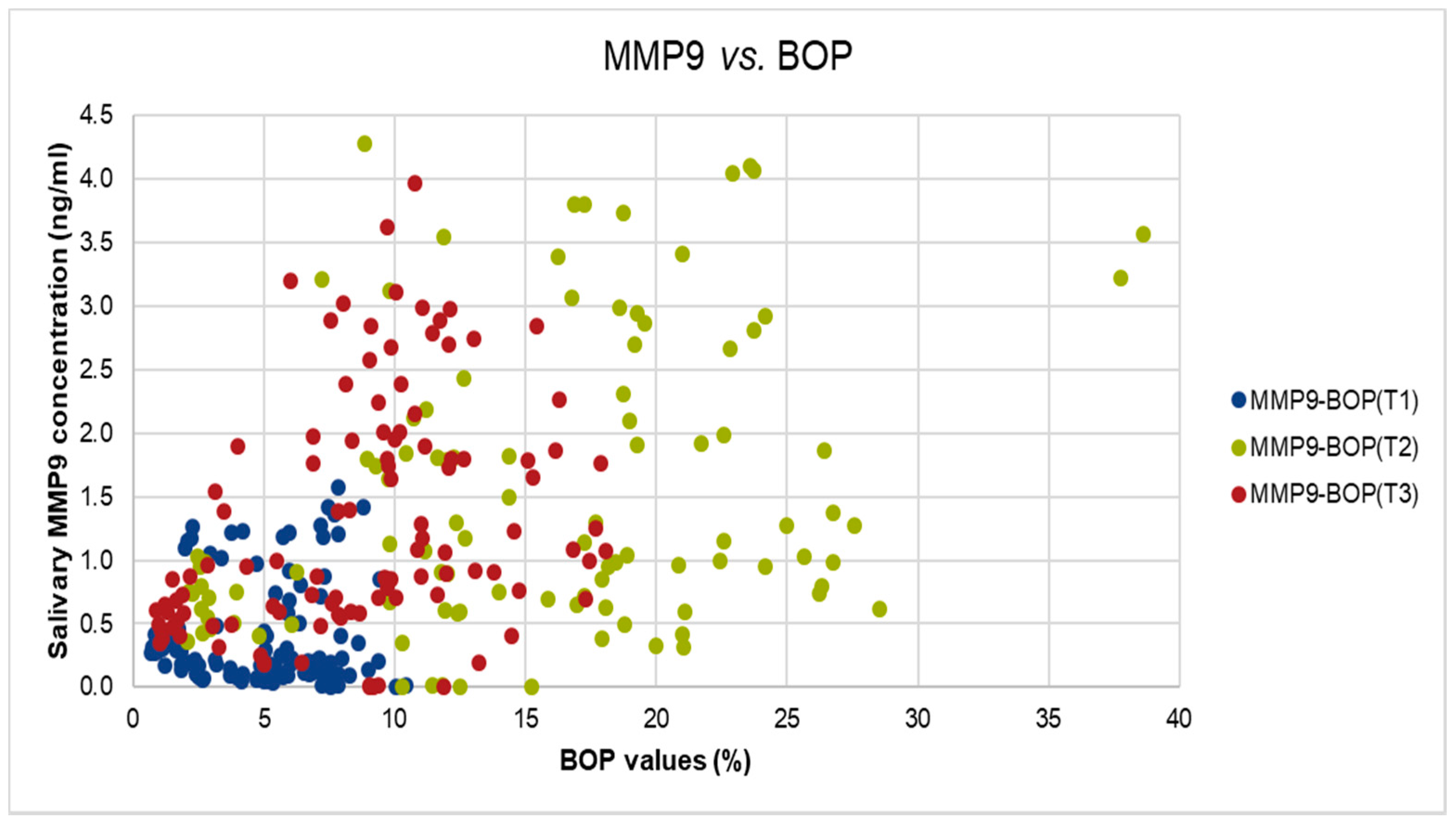
| MMP9(T1) | 0.450 ± (0.48) ng/mL |
| MMP9(T2) | 1.899 ± (1.82) ng/mL |
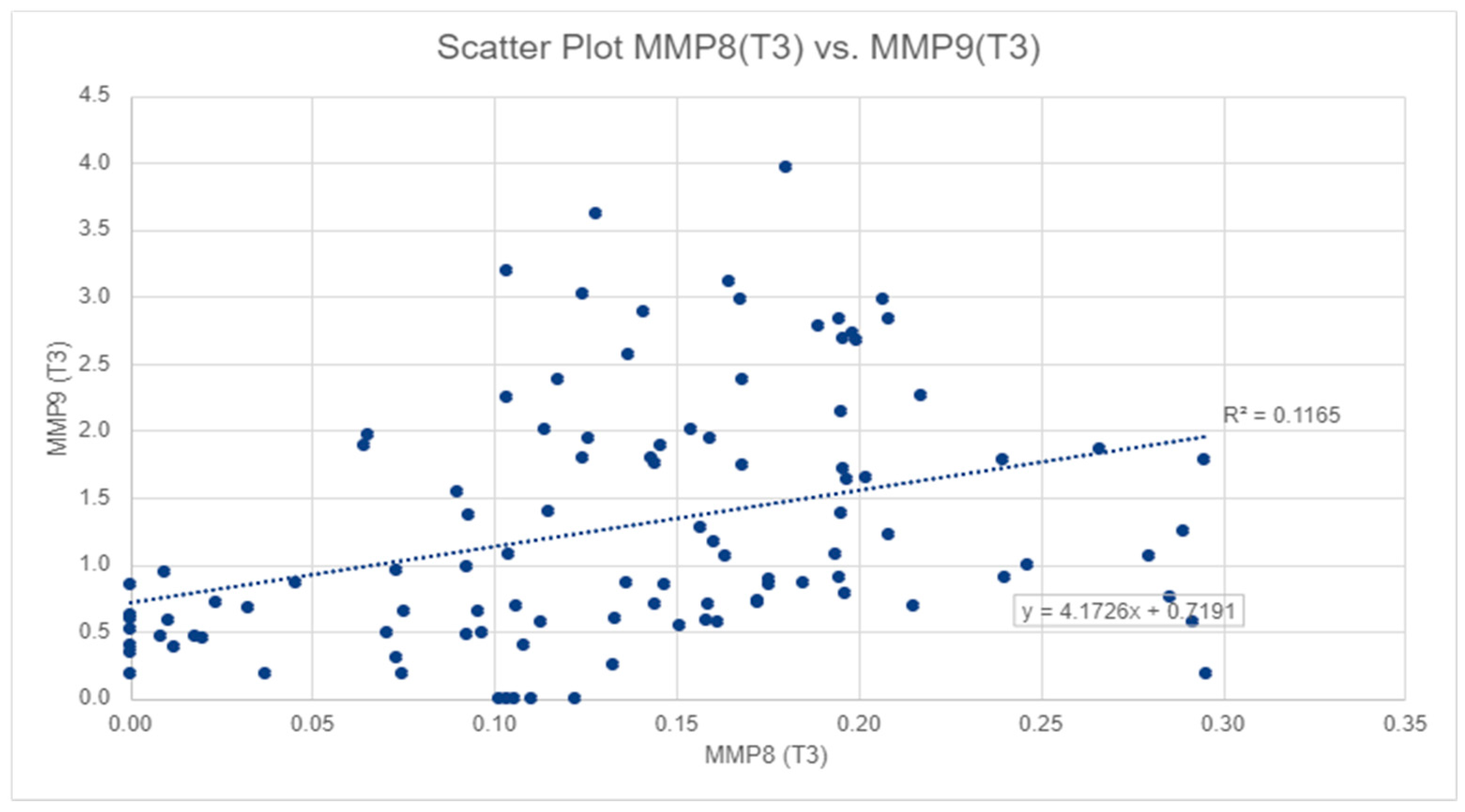
| MMP9(T3) | 0.100 ± (0.07) ng/mL *# |
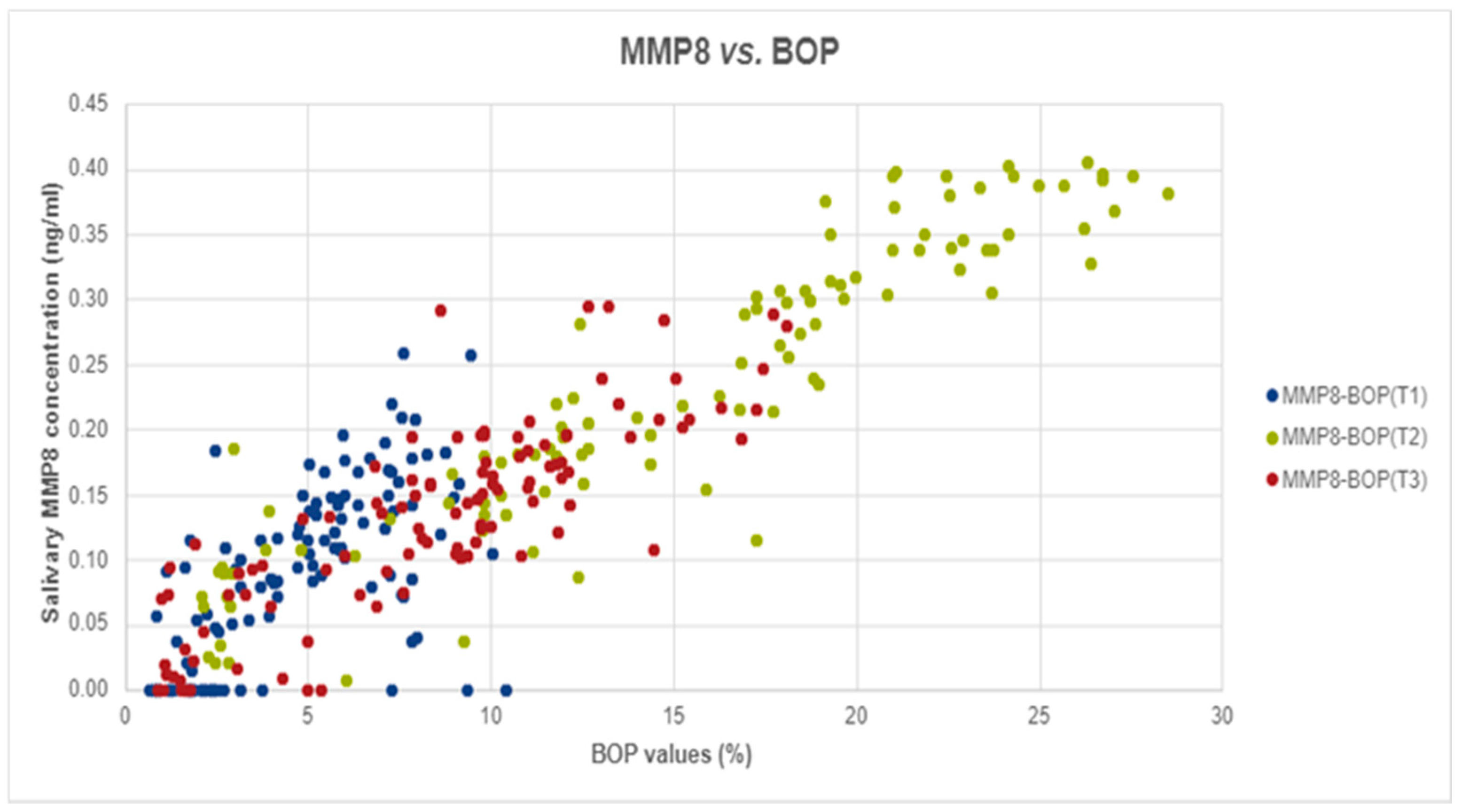
| MMP8(T1) | 0.100 ± (0.07) ng/mL |
| MMP8(T2) | 0.267 ± (0.20) ng/mL |
| MMP8(T3) | 0.140 ± (0.08) ng/mL *# |
| BOP(T1) | 5.088 ± (2.72)% |
| BOP(T2) | 16.224 ± (8.84)% |
| BOP(T3) | 8.761 ± (4.56)% **## |
| Parameter | Healthy Group (N = 201) | Localized Gingivitis Group (N = 127) | Generalized Gingivitis Group (N = 5) |
|---|---|---|---|
| MMP-9 (ng/mL) | 0.843 ± 1.11 | 1.842 ± 1.58 ** | 3.532 ± 0.50 ##** |
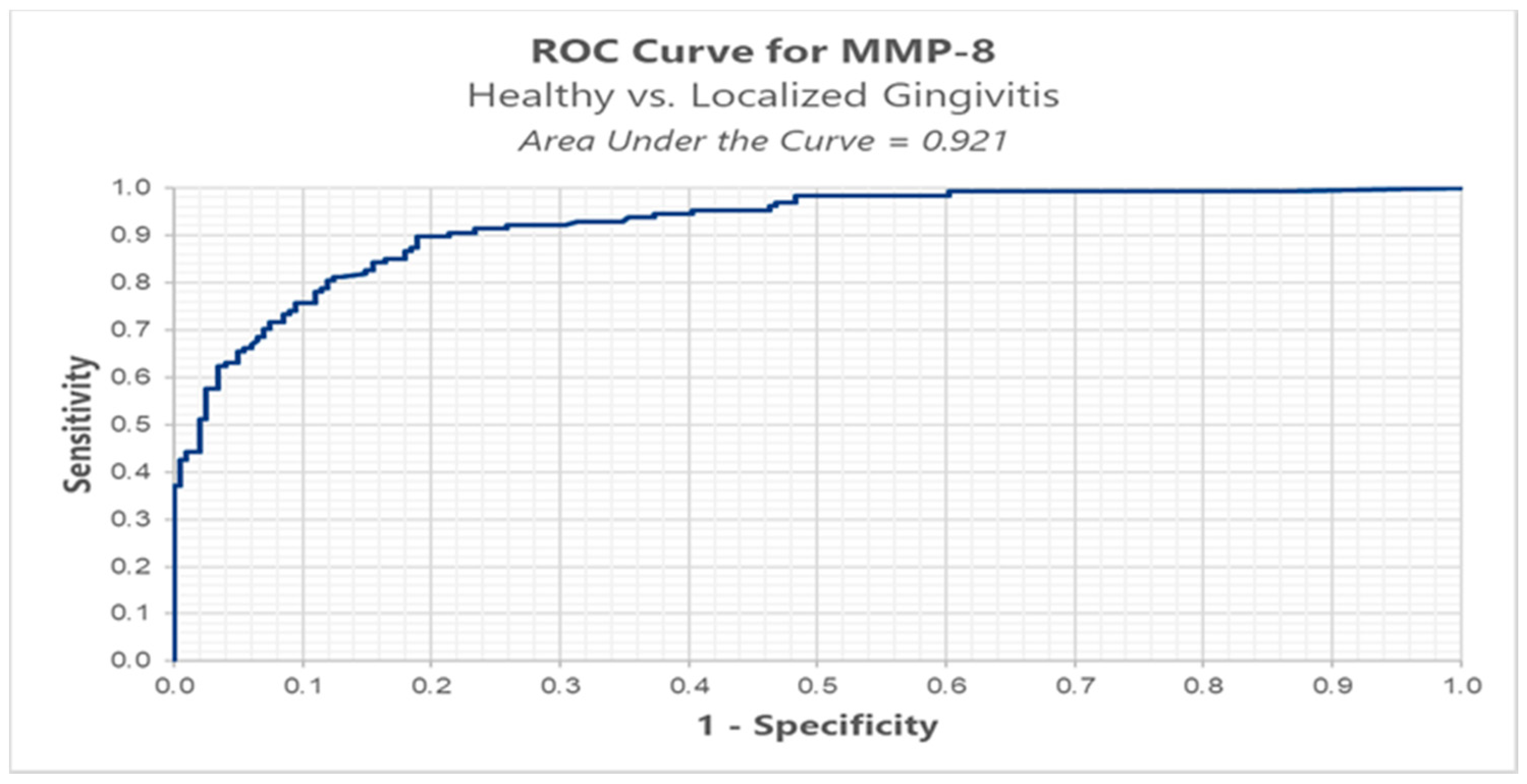
| MMP-8 (ng/mL) | 0.098 ± 0.06 | 0.249 ± 0.09 ** | 0.994 ± 0.26 ##** |
| Bleeding on probing (BOP, %) | 5.259 ± 2.80 | 16.411 ± 5.06 ** | 39.366 ± 1.17 ##** |
| Group | Optimal Cut-Off | Sensitivity | Specificity | FP | FN | AUC |
|---|---|---|---|---|---|---|
| MMP-8 (Healthy versus Localized Gingivitis) | 0.152 ng/mL | 0.898 | 0.811 | 0.189 | 0.102 | 0.924 |
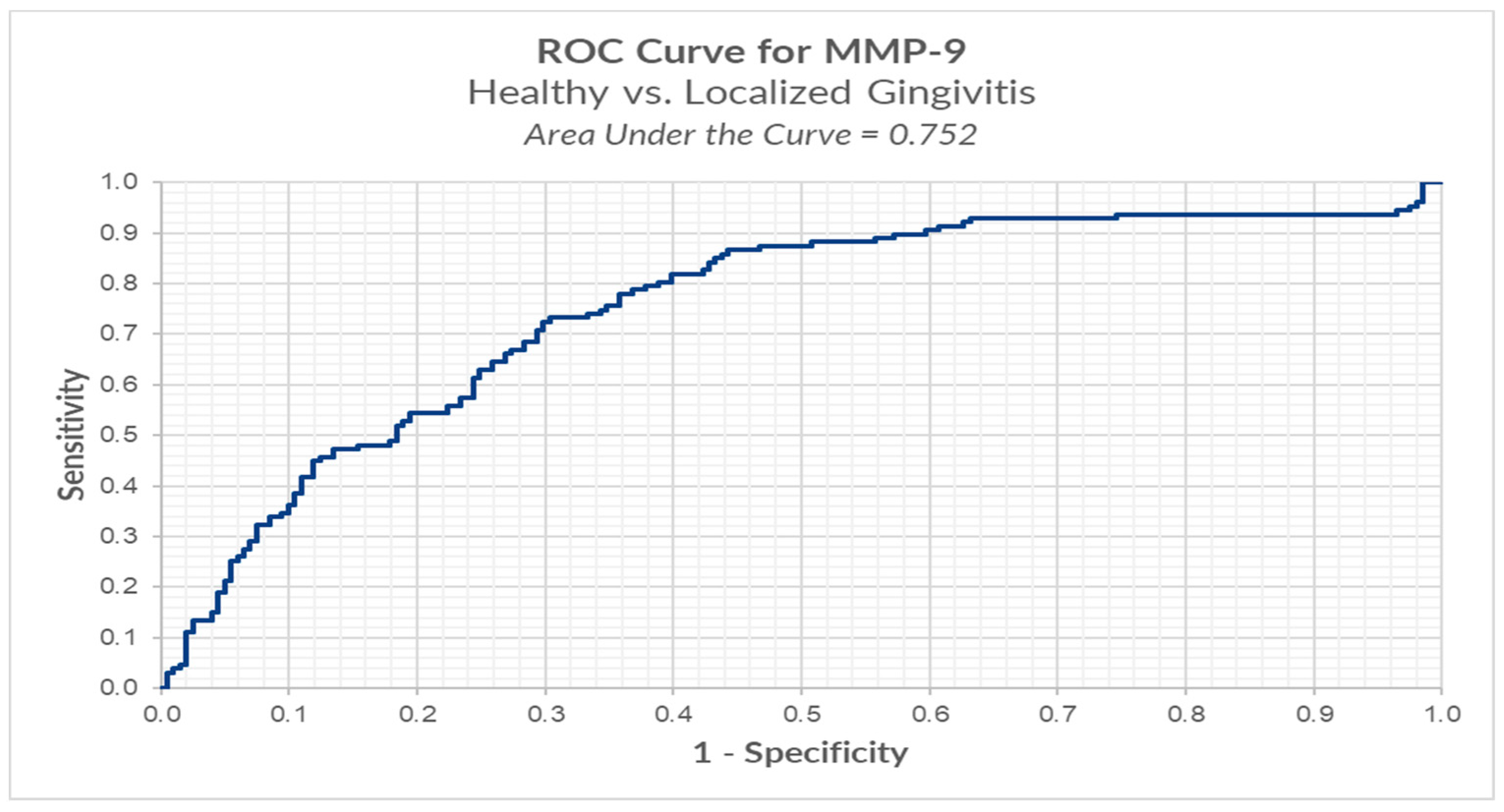
| Group | Optimal Cut-Off | Sensitivity | Specificity | FP | FN | AUC |
|---|---|---|---|---|---|---|
| MMP-9 (Healthy versus Localized Gingivitis) | 0.874 ng/mL | 0.732 | 0.697 | 0.303 | 0.268 | 0.752 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sioustis, I.-A.; Martu, M.-A.; Aminov, L.; Pavel, M.; Cianga, P.; Kappenberg-Nitescu, D.C.; Luchian, I.; Solomon, S.M.; Martu, S. Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy. Int. J. Environ. Res. Public Health 2021, 18, 1583. https://doi.org/10.3390/ijerph18041583
Sioustis I-A, Martu M-A, Aminov L, Pavel M, Cianga P, Kappenberg-Nitescu DC, Luchian I, Solomon SM, Martu S. Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy. International Journal of Environmental Research and Public Health. 2021; 18(4):1583. https://doi.org/10.3390/ijerph18041583
Chicago/Turabian StyleSioustis, Ioana-Andreea, Maria-Alexandra Martu, Liana Aminov, Mariana Pavel, Petru Cianga, Diana Cristala Kappenberg-Nitescu, Ionut Luchian, Sorina Mihaela Solomon, and Silvia Martu. 2021. "Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy" International Journal of Environmental Research and Public Health 18, no. 4: 1583. https://doi.org/10.3390/ijerph18041583
APA StyleSioustis, I.-A., Martu, M.-A., Aminov, L., Pavel, M., Cianga, P., Kappenberg-Nitescu, D. C., Luchian, I., Solomon, S. M., & Martu, S. (2021). Salivary Metalloproteinase-8 and Metalloproteinase-9 Evaluation in Patients Undergoing Fixed Orthodontic Treatment before and after Periodontal Therapy. International Journal of Environmental Research and Public Health, 18(4), 1583. https://doi.org/10.3390/ijerph18041583