
Factors Associated with Successful Smoking Cessation According to Age Group: Findings of an 11-Year Korea National Survey


Abstract
1. Introduction
2. Materials and Methods
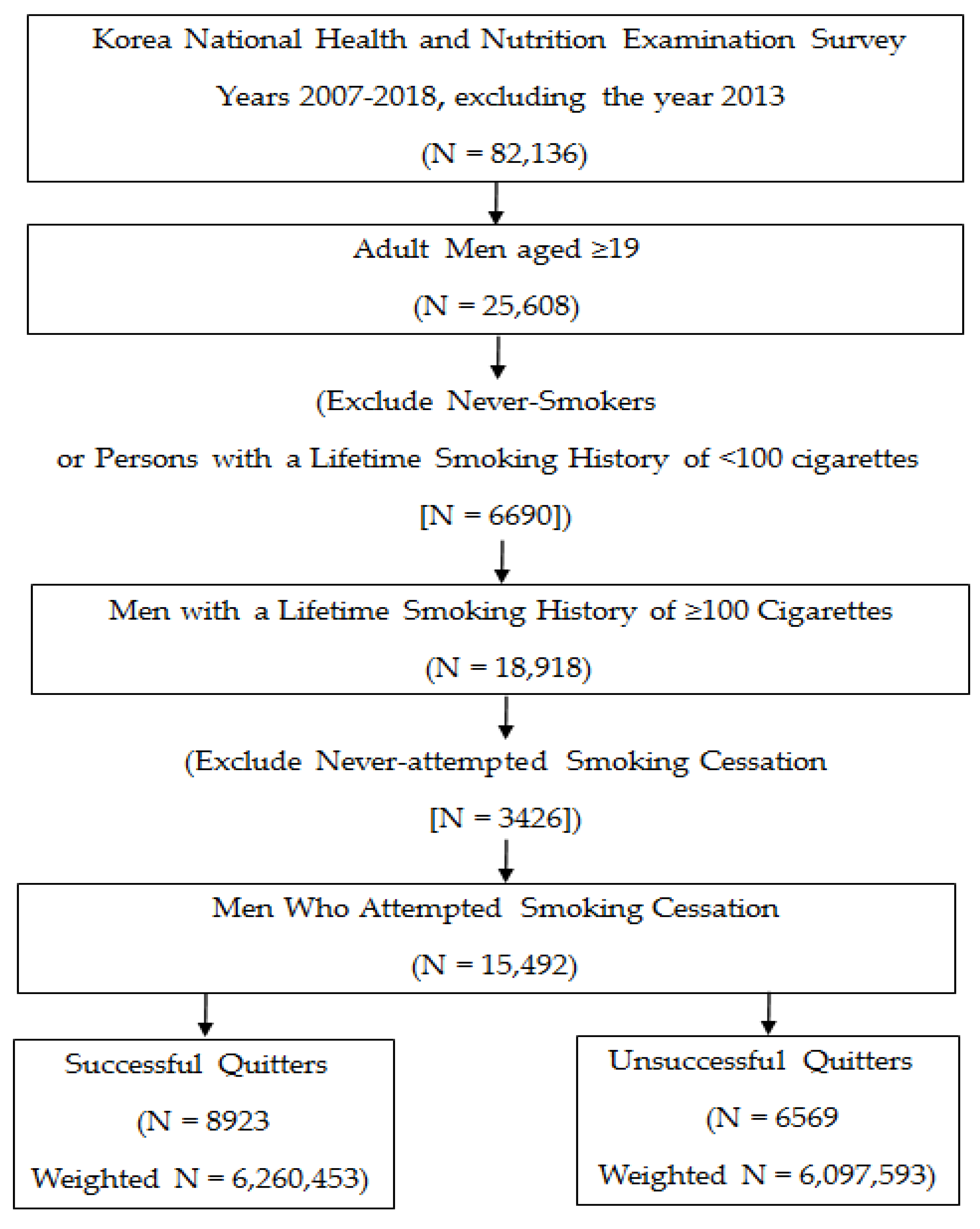
2.1. Study Design, Data Sources, and Inclusion/Exclusion Criteria
2.2. Ethical Considerations
2.3. Measurements and Definitions of Major Clinical and General Characteristics
2.4. Statistical Analysis
3. Results
3.1. Prevalence of Successful vs. Unsuccessful Quitters
3.2. Sociodemographic Characteristics and Smoking History of Study Participants
3.3. Clinical Characteristics, Health Behaviours, and Perceived Health Status of Study Participants
3.4. Factors Associated with Smoking Cessation According to Age Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Prevalence of Tobacco Smoking. Available online: https://www.who.int/gho/tobacco/use/en/ (accessed on 1 October 2020).
- Ockene, J.K.; Emmons, K.M.; Mermelstein, R.J.; Bonollo, D.S.; Perkins, K.A.; Voorhees, C.C.; Hollis, J.F. Relapse and maintenance issues for smoking cessation. Health Psychol. 2000, 19, 17–31. [Google Scholar] [CrossRef]
- Abrams, D.N.R.; Brown, R. The Tobacco Dependence Treatment Handbook: A Guide to Best Practices; Guilford: New York, NY, USA, 2003. [Google Scholar]
- London RCoPo. Nicotine Addiction in Britain: A Report of the Tobacco Advisory Group of the Royal College of Physicians; Royal College of Physicians of London: London, UK, 2000; Available online: http://bookshop.rcplondon.ac.uk/details.aspx?e=131 (accessed on 10 September 2020).
- Trotter, L.; Mullins, R.; Boulter, J.; Borland, R. Key findings of the 1996 and 1997 household surveys. In Quit Evaluation Studies 9; The Anti-Cancer Council of Victoria: Melbourne, Australia, 1998; pp. 1–26. [Google Scholar]
- Filozof, C.; Fernandez Pinilla, M.C.; Fernandez-Cruz, A. Smoking cessation and weight gain. Obes. Rev. 2004, 5, 95–103. [Google Scholar] [CrossRef]
- Korea Centers for Disease Control and Prevention KCfDCaP. The statistical report on health behaviors and chronic illnesses, 2019. Available online: https://knhanescdcgokr/knhanes/eng/indexdo (accessed on 9 July 2020).
- Kim, Y.; Cho, W.K. Factors associated with successful smoking cessation in Korean adult males: Findings from a National Survey. Iran J. Public Health 2014, 43, 1486–1496. [Google Scholar]
- Monso, E.; Campbell, J.; Tonnesen, P.; Gustavsson, G.; Morera, J. Sociodemographic predictors of success in smoking intervention. Tob. Control. 2001, 10, 165–169. [Google Scholar] [CrossRef]
- Lee, C.W.; Kahende, J. Factors associated with successful smoking cessation in the United States, 2000. Am. J. Public Health 2007, 97, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Hymowitz, N.; Cummings, K.M.; Hyland, A.; Lynn, W.R.; Pechacek, T.F.; Hartwell, T.D. Predictors of smoking cessation in a cohort of adult smokers followed for five years. Tob. Control. 1997, 6, S57–S62. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J. Predictors for successful smoking cessation in Korean adults. Asian Nurs. Res. 2014, 8, 1–7. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Quitting smoking among adults—United States, 2001–2010. MMWR Morb. Mortal. Wkly. Rep. 2011, 60, 1513–1519. [Google Scholar]
- Yong, H.H.; Borland, R.; Siahpush, M. Quitting-related beliefs, intentions, and motivations of older smokers in four countries: Findings from the International Tobacco Control Policy Evaluation Survey. Addict. Behav. 2005, 30, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Breslau, N.; Peterson, E.L. Smoking cessation in young adults: Age at initiation of cigarette smoking and other suspected influences. Am. J. Public Health 1996, 86, 214–220. [Google Scholar] [CrossRef]
- Hellman, R.; Cummings, K.M.; Haughey, B.P.; Zielezny, M.; O′Shea, R. Predictors of attempting and succeeding at smoking cessation. Health Educ. Res. 1991, 6, 77–86. [Google Scholar] [CrossRef]
- Walker, J.F.; Loprinzi, P.D. Longitudinal examination of predictors of smoking cessation in a national sample of U.S. adolescent and young adult smokers. Nicotine Tob. Res. 2014, 16, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Hyland, A.; Borland, R.; Li, Q.; Yong, H.-H.; McNeill, A.; Fong, G.T.; O’Connor, R.J.; Cummings, K.M. Individual-level predictors of cessation behaviours among participants in the International Tobacco Control (ITC) Four Country Survey. Tob. Control 2006, 15, iii83–iii94. [Google Scholar] [CrossRef]
- Kang, H.G.; Kwon, K.H.; Lee, I.W.; Jung, B.; Park, E.-C.; Jang, S.-I. Biochemically-verified smoking rate trends and factors associated with inaccurate self-reporting of smoking habits in Korean women. Asian Pac. J. Cancer Prev. 2013, 14, 6807–6812. [Google Scholar] [CrossRef] [PubMed]
- Jung-Choi, K.H.; Khang, Y.H.; Cho, H.J. Hidden female smokers in Asia: A comparison of self-reported with cotinine-verified smoking prevalence rates in representative national data from an Asian population. Tob. Control 2012, 21, 536–542. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (accessed on 12 September 2019).
- Pomerleau, C.S.; Pomerleau, O.F.; Snedecor, S.M.; Mehringer, A.M. Defining a never-smoker: Results from the nonsmokers survey. Addict. Behav. 2004, 29, 1149–1154. [Google Scholar] [CrossRef]
- Gideon, C.A. Adult development. In Encyclopedia of Aging and Public Health; Loue, S.J.D., Sajatovic, M., Eds.; Springer: Boston, MA, USA, 2008; pp. 90–91. [Google Scholar]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Smoking Cessation. A Report of the Surgeon General. Available online: https://www.cdc.gov/tobacco/data_statistics/sgr/2020-smoking-cessation/index.html (accessed on 21 September 2020).
- Babb, S.; Malarcher, A.; Schauer, G.; Asman, K.; Jamal, A. Quitting smoking among adults—United States, 2000–2015. Morb. Mortal. Wkly. Rep. 2017, 65, 1457–1464. [Google Scholar] [CrossRef]
- Wang, T.W.; Gentzke, A.S.; Creamer, M.R.; Cullen, K.A.; Holder-Hayes, E.; Sawdey, M.D.; Anic, G.M.; Portnoy, D.B.; Hu, S.; Homa, D.M.; et al. Tobacco product use and associated factors among middle and high school students—United States, 2019. MMWR Surveill. Summ. 2019, 68, 1–22. [Google Scholar] [CrossRef]
- Oshio, T. Association between successful smoking cessation and changes in marital and job status and health behaviours: Evidence from a 10-wave nationwide survey in Japan. BMC Public Health 2018, 18, 1051. [Google Scholar] [CrossRef]
- Pennanen, M.; Broms, U.; Korhonen, T.; Haukkala, A.; Partonen, T.; Tuulio-Henriksson, A.; Laatikainen, T.; Patja, K.; Kaprio, J. Smoking, nicotine dependence and nicotine intake by socio-economic status and marital status. Addict. Behav. 2014, 39, 1145–1151. [Google Scholar] [CrossRef]
- Faseru, B.; Richter, K.P.; Scheuermann, T.S.; Park, E.W. Enhancing partner support to improve smoking cessation. Cochrane Database Syst. Rev. 2018, 8, CD002928. [Google Scholar] [CrossRef]
- Lancaster, T.; Stead, L.F. Individual behavioural counselling for smoking cessation. Cochrane Database Syst. Rev. 2017, 3, CD001292. [Google Scholar] [CrossRef]
- Hartmann-Boyce, J.; Chepkin, S.C.; Ye, W.; Bullen, C.; Lancaster, T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst. Rev. 2018, 5, CD000146. [Google Scholar] [CrossRef] [PubMed]
- Cahill, K.; Lindson-Hawley, N.; Thomas, K.H.; Fanshawe, T.R.; Lancaster, T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database Syst Rev 2016, 5, CD006103. [Google Scholar] [CrossRef]
- Vangeli, E.; Stapleton, J.; Smit, E.S.; Borland, R.; West, R. Predictors of attempts to stop smoking and their success in adult general population samples: A systematic review. Addiction 2011, 106, 2110–2121. [Google Scholar] [CrossRef]
- Zhou, X.; Nonnemaker, J.; Sherrill, B.; Gilsenan, A.W.; Coste, F.; West, R. Attempts to quit smoking and relapse: Factors associated with success or failure from the ATTEMPT cohort study. Addict. Behav. 2009, 34, 365–373. [Google Scholar] [CrossRef]
- Van Zundert, R.M.; Nijhof, L.M.; Engels, R.C. Testing social cognitive theory as a theoretical framework to predict smoking relapse among daily smoking adolescents. Addict. Behav. 2009, 34, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.S.; Wick, J.A.; Nazir, N.; Cupertino, A.P.; Mussulman, L.M.; Ahluwalia, J.S.; Ellerbeck, E.F. Predictors of early versus late smoking abstinence within a 24-month disease management program. Nicotine Tob. Res. 2011, 13, 215–220. [Google Scholar] [CrossRef]
- Japuntich, S.J.; Leventhal, A.M.; Piper, M.E.; Bolt, D.M.; Roberts, L.J.; Fiore, M.C.; Baker, T.B. Smoker characteristics and smoking-cessation milestones. Am J. Prev. Med. 2011, 40, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Kalkhoran, S.; Kruse, G.R.; Chang, Y.; Rigotti, N.A. Smoking-cessation efforts by US adult smokers with medical comorbidities. Am. J. Med. 2018, 131, 318.e1–318.e8. [Google Scholar] [CrossRef] [PubMed]
- Croghan, I.T.; Schroeder, D.R.; Hays, J.T.; Eberman, K.M.; Patten, C.A.; Berg, E.J.; Hurt, R.D. Nicotine dependence treatment: Perceived health status improvement with 1-year continuous smoking abstinence. Eur. J. Public Health 2005, 15, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Piper, M.E.; Kenford, S.; Fiore, M.C.; Baker, T.B. Smoking cessation and quality of life: Changes in life satisfaction over 3 years following a quit attempt. Ann. Behav. Med. 2012, 43, 262–270. [Google Scholar] [CrossRef]
- Shang, C.; Chaloupka, F.J.; Fong, G.T.; Thompson, M.; Siahpush, M.; Ridgeway, W. Weight control belief and its impact on the effectiveness of tobacco control policies on quit attempts: Findings from the ITC 4 Country Survey. Tob. Control 2015, 24, iii41–iii47. [Google Scholar] [CrossRef]
- Stadler, M.; Tomann, L.; Storka, A.; Wolzt, M.; Peric, S.; Bieglmayer, C.; Pacini, G.; Dickson, S.L.; Brath, H.; Bech, P.; et al. Effects of smoking cessation on beta-cell function, insulin sensitivity, body weight, and appetite. Eur. J. Endocrinol. 2014, 170, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Fanshawe, T.R.; Halliwell, W.; Lindson, N.; Aveyard, P.; Livingstone-Banks, J.; Hartmann-Boyce, J. Tobacco cessation interventions for young people. Cochrane Database Syst. Rev. 2017, 11, CD003289. [Google Scholar] [CrossRef]
- Macy, J.T.; Seo, D.C.; Chassin, L.; Presson, C.C.; Sherman, S.J. Prospective predictors of long-term abstinence versus relapse among smokers who quit as young adults. Am. J. Public Health 2007, 97, 1470–1475. [Google Scholar] [CrossRef]
- Gunay, T.; Pekel, O.; Simsek, H.; Sahan, C.; Soysal, A.; Kilinc, O.; Ergör, G. Smoking habits and cessation success. What differs among adults and elderly? Saudi Med. J. 2014, 35, 585–591. [Google Scholar]



{kind=link}
{kind=link}
| Year | Age Group | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 19–39 Years (N = 3523) | 40–64 Years (N = 7380) | ≥65 Years (N = 4589) | All Age Groups (N = 15,492) | |||||||||
| Successful Quitters % (SE) (N = 1157) 1 | Unsuccessful Quitters % (SE) (N = 2366) 2 | p | Successful Quitters % (SE) (N = 4188) 3 | Unsuccessful Quitters % (SE) (N = 3192) 4 | p | Successful Quitters % (SE) (N = 3578) 5 | Unsuccessful Quitters % (SE) (N = 1011) 6 | p | Successful Quitters % (SE) (N = 8923) 7 | Unsuccessful Quitters % (SE) (N = 6569) 8 | p | |
| 0.012 | 0.001 | 0.022 | <0.001 | |||||||||
| 2007 | 32.1 (3.25) | 67.9 (3.25) | 57.8 (3.06) | 42.2 (3.06) | 75.3 (4.34) | 24.7 (4.34) | 49.3 (2.05) | 50.7 (2.05) | ||||
| 2008 | 30.0 (2.40) | 70.0 (2.40) | 56.2 (2.16) | 43.8 (2.16) | 72.1 (3.06) | 27.9 (3.06) | 48.7 (1.45) | 51.3 (1.45) | ||||
| 2009 | 27.7 (2.09) | 72.3 (2.09) | 49.9 (1.94) | 50.1 (1.94) | 79.6 (2.01) | 20.4 (2.01) | 46.3 (1.32) | 53.7 (1.32) | ||||
| 2010 | 28.2 (2.62) | 71.8 (2.62) | 50.1 (2.27) | 49.9 (2.27) | 74.9 (2.37) | 25.1 (2.37) | 46.6 (1.72) | 53.4 (1.72) | ||||
| 2011 | 26.6 (2.61) | 73.4 (2.61) | 53.3 (2.12) | 46.7 (2.12) | 73.9 (2.57) | 26.1 (2.57) | 47.6 (1.69) | 52.4 (1.69) | ||||
| 2012 | 31.2 (3.04) | 68.8 (3.04) | 54.7 (2.24) | 45.3 (2.24) | 76.5 (2.26) | 23.5 (2.26) | 51.3 (1.59) | 48.7 (1.59) | ||||
| 2014 | 30.2 (3.16) | 69.8 (3.16) | 47.0 (2.67) | 53.0 (2.67) | 79.1 (2.27) | 20.9 (2.27) | 48.9 (1.96) | 51.1 (1.96) | ||||
| 2015 | 32.8 (2.98) | 67.2 (2.98) | 57.2 (2.15) | 42.8 (2.15) | 80.7 (2.30) | 19.3 (2.30) | 55.0 (1.47) | 45.0 (1.47) | ||||
| 2016 | 32.4 (3.00) | 67.6 (3.00) | 58.4 (2.55) | 41.6 (2.55) | 79.8 (2.31) | 20.2 (2.31) | 55.2 (1.77) | 44.8 (1.77) | ||||
| 2017 | 38.8 (3.46) | 61.2 (3.46) | 58.4 (2.53) | 41.6 (2.53) | 80.3 (2.13) | 19.7 (2.13) | 57.7 (1.66) | 42.3 (1.66) | ||||
| 2018 | 41.6 (3.06) | 58.4 (3.06) | 59.1 (1.98) | 40.9 (1.98) | 84.3 (2.14) | 15.7 (2.14) | 59.6 (1.50) | 40.4 (1.50) | ||||
| Variables | Age 19–39 Years (N = 3523) | Age 40–64 Years (N = 7380) | Age ≥65 Years (N = 4589) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Successful Quitters (N = 1157) | Unsuccessful Quitters (N = 2366) | p | Successful Quitters (N = 4188) | Unsuccessful Quitters (N = 3192) | p | Successful Quitters (N = 3578) | Unsuccessful Quitters (N = 1011) | p | |
| Married (%) | 57.6 (1.69) | 44.9 (1.23) | <0.001 | 91.6 (0.52) | 83.9 (0.79) | <0.001 | 89.3 (0.64) | 86.4 (1.33) | 0.033 |
| Education level (%) | <0.001 | 0.009 | <0.001 | ||||||
| ≤High school | 40.9 (1.64) | 54.6 (1.18) | 61.9 (0.98) | 65.3 (1.06) | 84.1 (0.87) | 90.1 (1.14) | |||
| University or higher | 59.1 (1.64) | 45.4 (1.18) | 38.1 (0.98) | 34.7 (1.06) | 15.9 (0.87) | 9.9 (1.14) | |||
| Occupation | <0.001 | 0.198 | <0.001 | ||||||
| Manager/Professionals | 22.5 (1.37) | 18.5 (0.89) | 18.3 (0.79) | 16.7 (0.79) | 3.3 (0.38) | 3.0 (0.75) | |||
| Office worker | 20.6 (1.25) | 14.2 (0.77) | 13.2 (0.63) | 12.3 (0.71) | 1.4 (0.24) | 1.9 (0.50) | |||
| Service workers/Sellers | 11.6 (1.05) | 17.9 (0.92) | 13.6 (0.63) | 13.1 (0.71) | 2.9 (0.33) | 2.9 (0.56) | |||
| Agriculture/Fishery/Labour | 26.2 (1.42) | 28.9 (1.05) | 42.4 (0.95) | 45.6 (1.12) | 28.7 (1.03) | 38.4 (1.98) | |||
| None | 19.1 (1.41) | 20.5 (1.08) | 12.5 (0.60) | 12.3 (0.67) | 63.7 (1.09) | 53.8 (1.99) | |||
| Residence (% Rural) | 10.1 (1.19) | 12.5 (1.07) | 0.064 | 18.0 (1.04) | 22.3 (1.31) | 0.001 | 25.2 (1.37) | 29.9 (1.98) | 0.008 |
| Household income (Quartiles) | 0.062 | <0.001 | 0.001 | ||||||
| 1st (Lowest) | 23.1 (1.37) | 25.9 (1.06) | 21.2 (0.78) | 27.9 (0.97) | 23.6 (0.88) | 28.8 (1.73) | |||
| 2nd | 24.7 (1.39) | 24.9 (0.98) | 25.8 (0.82) | 27.0 (0.96) | 23.9 (0.85) | 26.1 (1.65) | |||
| 3rd | 24.8 (1.38) | 26.1 (1.02) | 25.9 (0.81) | 23.6 (0.89) | 24.5 (0.86) | 24.2 (1.60) | |||
| 4th (Highest) | 27.3 (1.48) | 23.1 (1.05) | 27.1 (0.87) | 21.5 (0.90) | 27.9 (0.97) | 20.9 (1.60) | |||
| Lifetime smoking amount (pack year) | 6.93 ± 0.22 | 8.67 ± 0.17 | <0.001 | 19.26 ± 0.30 | 24.87 ± 0.30 | <0.001 | 29.32 ± 0.54 | 30.51 ± 0.82 | 0.220 |
| Second-hand smoking (%) | |||||||||
| Workplace (yes) | 43.4 (1.72) | 46.4 (1.19) | 0.148 | 36.7 (0.89) | 44.1 (1.03) | <0.001 | 8.7 (0.57) | 13.4 (1.32) | <0.001 |
| Home (yes) | 4.6 (0.73) | 11.8 (0.82) | <0.001 | 1.8 (0.24) | 5.2 (0.44) | <0.001 | 2.4 (0.32) | 3.8 (0.68) | 0.026 |
| Smoking cessation methods (%) | |||||||||
| Willpower | 94.2 (0.72) | 87.1 (0.76) | <0.001 | 92.8 (0.47) | 82.3 (0.80) | <0.001 | 95.3 (0.44) | 81.9 (1.48) | <0.001 |
| Nicotine replacement therapy | 6.0 (0.75) | 16.8 (0.84) | <0.001 | 5.8 (0.42) | 17.5 (0.79) | <0.001 | 3.3 (0.35) | 11.4 (1.29) | <0.001 |
| Prescribed oral medicines | 1.0 (0.31) | 0.9 (0.22) | 0.809 | 1.2 (0.20) | 2.0 (0.28) | 0.020 | 0.8 (0.18) | 3.0 (0.68) | <0.001 |
| Education/Counselling | 4.1 (0.59) | 8.6 (0.62) | <0.001 | 5.4 (0.40) | 12.7 (0.67) | <0.001 | 3.9 (0.41) | 17.4 (1.42) | <0.001 |
| Smokers’ quit line | 0.4 (0.18) | 0.7 (0.17) | 0.296 | 0.8 (0.17) | 1.9 (0.27) | <0.001 | 0.4 (0.12) | 1.5 (0.44) | <0.001 |
| Variables | Age 19–39 Years (N = 3523) | Age 40–64 Years (N = 7380) | Age ≥65 Years (N = 4589) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Successful Quitters (N = 1157) | Unsuccessful Quitters (N = 2366) | p | Successful Quitters (N = 4188) | Unsuccessful Quitters (N = 3192) | p | Successful Quitters (N = 3578) | Unsuccessful Quitters (N = 1011) | p | |
| Systolic blood pressure (mmHg) | 114.96 ± 0.40 | 115.07 ± 0.28 | 0.820 | 121.76 ± 0.28 | 119.58 ± 0.32 | <0.001 | 127.37 ± 0.36 | 125.87 ± 0.65 | 0.035 |
| Diastolic blood pressure (mmHg) | 77.37 ± 0.36 | 77.09 ± 0.25 | 0.513 | 81.31 ± 0.19 | 79.89 ± 0.23 | <0.001 | 73.30 ± 0.22 | 71.49 ± 0.41 | <0.001 |
| Body mass index (kg/m2) | 24.60 ± 0.12 | 24.44 ± 0.09 | 0.272 | 24.76 ± 0.05 | 24.21 ± 0.06 | <0.001 | 23.57 ± 0.06 | 22.86 ± 0.12 | <0.001 |
| Waist circumference (cm) | 84.72 ± 0.32 | 84.20 ± 0.24 | 0.185 | 86.67 ± 0.15 | 85.60 ± 0.18 | <0.001 | 86.18 ± 0.18 | 84.36 ± 0.35 | <0.001 |
| Fasting blood sugar (mg/dL) | 94.18 ± 0.48 | 93.04 ± 0.39 | 0.065 | 104.78 ± 0.43 | 104.47 ± 0.55 | 0.660 | 107.31 ± 0.54 | 106.18 ± 1.12 | 0.368 |
| Total cholesterol (mg/dL) | 187.16 ± 1.09 | 187.26 ± 0.88 | 0.945 | 194.72 ± 0.67 | 194.55 ± 0.74 | 0.865 | 178.90 ± 0.77 | 178.08 ± 1.59 | 0.645 |
| Diabetes mellitus (%) | 13.0 (1.08) | 12.0 (0.78) | 0.493 | 38.2 (0.86) | 31.3 (0.97) | <0.001 | 58.4 (0.99) | 53.4 (1.94) | 0.020 |
| Hypertension (%) | 2.2 (0.48) | 2.5 (0.36) | 0.680 | 14.2 (0.62) | 14.3 (0.68) | 0.919 | 23.7 (0.89) | 23.8 (1.72) | 0.957 |
| Cardiovascular disease (%) | 0.4 (0.22) | 0.4 (0.12) | 0.747 | 4.7 (0.36) | 3.3 (0.34) | 0.005 | 16.0 (0.75) | 14.5 (1.34) | 0.339 |
| Cancer (%) | 0.4 (0.18) | 0.2 (0.09) | 0.255 | 3.5 (0.30) | 1.6 (0.26) | <0.001 | 10.2 (0.60) | 6.3 (0.94) | 0.002 |
| Trauma history (%) | 7.9 (0.94) | 11.0 (0.73) | 0.012 | 7.4 (0.48) | 8.4 (0.61) | 0.162 | 5.5 (0.49) | 9.1 (1.09) | 0.001 |
| Heavy drinker (%) | 22.4 (1.37) | 29.7 (1.03) | <0.001 | 22.2 (0.77) | 31.1 (0.93) | <0.001 | 8.2 (0.54) | 11.6 (1.26) | 0.007 |
| Regular exercise | 43.8 (1.63) | 39.7 (1.19) | 0.039 | 40.9 (0.96) | 32.8 (0.97) | <0.001 | 31.6 (1.02) | 26.2 (1.75) | 0.008 |
| Skipping meals (%) | |||||||||
| Skipping breakfast | 34.6 (1.60) | 45.6 (1.23) | <0.001 | 14.1 (0.68) | 21.6 (0.89) | <0.001 | 3.1 (0.37) | 8.9 (1.28) | <0.001 |
| Skipping lunch | 6.9 (0.84) | 11.3 (0.86) | 0.007 | 5.1 (0.43) | 6.9 (0.55) | 0.009 | 5.1 (0.46) | 10.7 (1.35) | <0.001 |
| Skipping dinner | 4.0 (0.61) | 6.2 (0.57) | 0.012 | 3.5 (0.35) | 4.2 (0.43) | 0.195 | 2.6 (0.33) | 3.8 (0.75) | 0.105 |
| Perceived health status (%) | <0.001 | <0.001 | <0.001 | ||||||
| Very good/Good | 48.7 (1.59) | 35.5 (1.13) | 37.3 (0.87) | 30.6 (0.95) | 30.1 (0.92) | 23.9 (1.58) | |||
| Fair | 41.5 (1.57) | 50.4 (1.15) | 48.4 (0.90) | 52.2 (1.03) | 43.2 (1.03) | 43.0 (1.90) | |||
| Poor/Very poor | 9.9 (1.00) | 14.1 (0.83) | 14.3 (0.60) | 17.2 (0.76) | 26.7 (0.90) | 33.0 (1.79) | |||
| Perceived psychological stress (%) | 28.7 (1.42) | 35.0 (1.09) | 0.001 | 21.8 (0.73) | 30.3 (0.90) | <0.001 | 12.9 (0.68) | 16.1 (1.32) | 0.023 |
| Variables | Age 19–39 Years | Age 40–64 Years | Age ≥65 Years | p for Interaction |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Marital status (Married) | 2.15 (1.78–2.60) | 1.97 (1.58–2.46) | 1.17 (0.83–1.64) | 0.007 |
| Education level (University) | 1.31 (1.08–1.69) | 0.98 (0.85–1.15) | 0.93 (0.65–1.33) | 0.043 |
| Occupation (Ref, None) | 0.013 | |||
| Manager/Professionals | 0.85 (0.62–1.16) | 0.75 (0.58–0.98) | 0.57 (0.26–1.24) | |
| Office workers | 0.98 (0.71–1.35) | 0.76 (0.58–1.00) | 0.30 (0.14–0.63) | |
| Service workers/Sellers | 0.56 (0.40–0.78) | 0.82 (0.63–1.07) | 0.60 (0.36–0.99) | |
| Agriculture/Fishery/Labour | 0.78 (0.58–1.06) | 0.83 (0.66–1.02) | 0.63 (0.50–0.79) | |
| Residence (Rural) | 0.84 (0.63–1.13) | 0.87 (0.73–1.03) | 0.85 (0.67–1.06) | 0.972 |
| Household income (Ref, Lowest) | 0.972 | |||
| 2nd | 1.21 (0.93–1.58) | 1.10 (0.91–1.33) | 1.11 (0.80–1.53) | |
| 3rd | 1.09 (0.84–1.42) | 1.15 (0.95–1.39) | 1.16 (0.85–1.59) | |
| 4th (Highest) | 1.35 (1.02–1.78) | 1.37 (1.13–1.67) | 1.26 (0.93–1.72) | |
| Lifetime smoking amount (Pack-year) | 0.96 (0.94–0.98) | 0.98 (0.98–0.99) | 1.00 (1.00–1.00) | <0.001 |
| Second-hand smoking | ||||
| Workplace (Yes) | 0.93 (0.76–1.13) | 0.89 (0.78–1.02) | 0.77 (0.54–1.10) | 0.665 |
| Home (Yes) | 0.39 (0.24–0.62) | 0.42 (0.28–0.62) | 0.75 (0.41–1.39) | 0.198 |
| Smoking cessation modes | ||||
| Willpower | 1.23 (0.87–1.75) | 1.43 (1.14–1.81) | 2.38 (1.59–3.58) | 0.034 |
| Nicotine replacement therapy | 0.37 (0.25–0.54) | 0.38 (0.30–0.48) | 0.42 (0.26–0.70) | 0.897 |
| Prescribed oral medicines | 1.16 (0.45–2.99) | 0.80 (0.46–1.39) | 0.24 (0.10–0.54) | 0.017 |
| Education or counselling | 0.69 (0.46–1.04) | 0.60 (0.46–0.78) | 0.33 (0.22–0.50) | 0.020 |
| Smokers’ quit line | 1.00 (0.22–4.55) | 0.76 (0.40–1.44) | 0.74 (0.21–2.64) | 0.944 |
| Systolic BP (per 10 mmHg increase) | 0.95 (0.87–1.05) | 1.07 (1.00–1.13) | 1.05 (0.98–1.12) | 0.053 |
| Diastolic BP (per 10 mmHg increase) | 0.96 (0.87–1.07) | 1.06 (0.97–1.16) | 1.16 (1.02–1.31) | 0.044 |
| Body mass index (kg/m2) | 1.01 (0.97–1.05) | 1.06 (1.02–1.10) | 1.06 (1.01–1.12) | 0.008 |
| Waist circumference (per 10 cm increase) | 0.93 (0.79–1.09) | 1.09 (0.95–1.25) | 1.07 (0.92–1.25) | 0.052 |
| Fasting blood sugar (per 10 mg/dL increase) | 1.06 (1.00–1.13) | 1.03 (0.99–1.06) | 1.02 (0.97–1.06) | 0.449 |
| Total cholesterol (per 10 mg/dL increase) | 0.99 (0.96–1.02) | 0.99 (0.97–1.01) | 1.01 (0.98–1.05) | 0.526 |
| Hypertension | 0.87 (0.64–1.18) | 1.23 (1.05–1.44) | 1.05 (0.84–1.31) | 0.071 |
| Diabetes mellitus | 0.75 (0.41–1.38) | 0.91 (0.72–1.15) | 0.83 (0.62–1.11) | 0.724 |
| Cardiovascular disease | 0.16 (0.02–1.33) | 1.55 (1.10–2.17) | 1.00 (0.73–1.36) | 0.027 |
| Cancer | 1.97 (0.44–8.79) | 2.22 (1.42–3.48) | 1.73 (1.09–2.74) | 0.735 |
| Trauma history | 0.74 (0.53–1.04) | 0.96 (0.75–1.23) | 0.62 (0.43–0.90) | 0.131 |
| Heavy drinker | 0.69 (0.56–0.86) | 0.64 (0.55–0.75) | 0.76 (0.52–1.10) | 0.661 |
| Exercise | 1.23 (1.02–1.49) | 1.34 (1.16–1.54) | 1.15 (0.90–1.47) | 0.539 |
| Perceived health status (Ref, Poor/Very poor) | 0.016 | |||
| Very good/Good | 1.62 (1.18–2.23) | 1.21 (0.99–1.49) | 1.46 (1.09–1.94) | |
| Fair | 0.97 (0.71–1.33) | 1.11 (0.91–1.34) | 1.18 (0.91–1.52) | |
| Perceived psychological stress | 0.79 (0.65–0.96) | 0.69 (0.60–0.80) | 0.81 (0.60–1.09) | 0.437 |
| Skipping meals | ||||
| Skipping breakfast | 0.67 (0.56–0.81) | 0.62 (0.52–0.75) | 0.36 (0.21–0.62) | 0.090 |
| Skipping lunch | 0.66 (0.45–0.97) | 0.75 (0.57–0.99) | 0.43 (0.28–0.66) | 0.089 |
| Skipping dinner | 0.49 (0.32–0.76) | 1.11 (0.79–1.55) | 0.80 (0.42–1.52) | 0.017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Lee, J.S.; Cho, W.-K. Factors Associated with Successful Smoking Cessation According to Age Group: Findings of an 11-Year Korea National Survey. Int. J. Environ. Res. Public Health 2021, 18, 1576. https://doi.org/10.3390/ijerph18041576
Kim Y, Lee JS, Cho W-K. Factors Associated with Successful Smoking Cessation According to Age Group: Findings of an 11-Year Korea National Survey. International Journal of Environmental Research and Public Health. 2021; 18(4):1576. https://doi.org/10.3390/ijerph18041576
Chicago/Turabian StyleKim, Youngmee, Ji Sung Lee, and Won-Kyung Cho. 2021. "Factors Associated with Successful Smoking Cessation According to Age Group: Findings of an 11-Year Korea National Survey" International Journal of Environmental Research and Public Health 18, no. 4: 1576. https://doi.org/10.3390/ijerph18041576
APA StyleKim, Y., Lee, J. S., & Cho, W.-K. (2021). Factors Associated with Successful Smoking Cessation According to Age Group: Findings of an 11-Year Korea National Survey. International Journal of Environmental Research and Public Health, 18(4), 1576. https://doi.org/10.3390/ijerph18041576