
Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage?




Abstract
1. Introduction
2. Materials and Methods
- Current health expenditure as % of GDP—this presents total spending on healthcare goods and services (excluding investment spending) by all types of financing arrangements (compulsory schemes, household out-of-pocket payments, voluntary health insurance, non-governmental organizations etc.) in relation to country GDP. Source of data: OECD Health Statistics (accessed on 20 July 2020) [33].
- Domestic general government health expenditure as % of general government expenditure—this compares the scale of current public health expenditure (by all financing agents holding public domestic funds) relative to the total scale of government expenditure. Thus, it indicates the government’s priority to spend on health out of its own domestic public resources. Source of data: World Health Organization Global Health Expenditure Database (accessed on 10 January 2021) [34].
- Government/compulsory scheme expenditure as % of current health expenditure—this presents the share of government (central and regional/local) and compulsory financing schemes (e.g., compulsory health insurance) in the total current expenditure. This mostly includes spending by government and social health insurance, though compulsory private health insurance is also included if present. Source of data: OECD Health Statistics (accessed on 20 July 2020) [33].
- Household out-of-pocket health expenditure as % of current health expenditure—out-of-pocket expenditures are payments borne directly by patients when using healthcare. They include direct payments for privately purchased healthcare (without involvement of third-party payers, e.g., an insurer) and patient cost sharing for goods and services covered by third-party payers. This also includes estimations of informal payments to healthcare providers when such data are available. Source of data: OECD Health Statistics (accessed on 20 July 2020) [33].
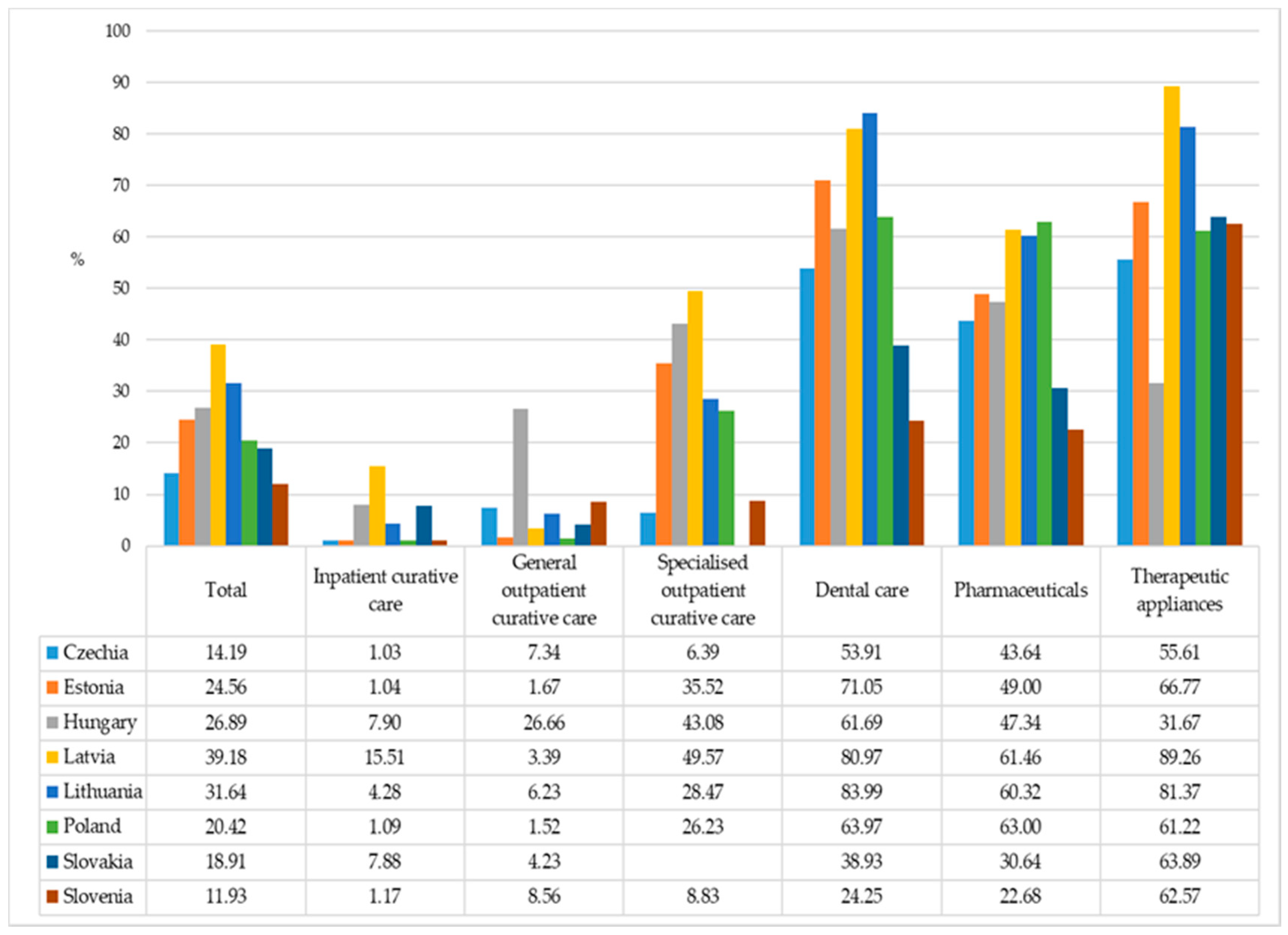
- Household out-of-pocket expenditure as % of health expenditure for given types of services—this gives more detailed information on household contributions to financing healthcare, and indicates the areas where public coverage is limited. Source of data: OECD Health Statistics (accessed on 20 July 2020) [33].
- Population coverage—population entitlement to a benefit package, financed from government or compulsory insurance schemes;
- Service coverage—the range of goods and services included in a benefit package. We focused on healthcare benefits (primary care, outpatient and inpatient specialist care, dental care, medical products, medicines), excluding sickness benefits or maternity benefits (even if in some countries they are financed though the obligatory health insurance fund). When analyzing service coverage, we also looked at the quality of services in a benefit package. Quality might be considered the fourth dimension of healthcare coverage, as gaps in this aspect might also lead to out-of-pocket patient payments.
- Cost coverage—patient cost-sharing obligations for healthcare in a benefit package. This might include a) flat-rate payments (co-payments) per good or service; b) percentage co-payments (sometimes referred to as co-insurance) when a patient pays a share of the price; c) deductibles, which require users to pay up to a fixed amount first, before the state/insurer will cover any costs. Patients might be also asked to cover any cost over the amount of money reimbursed by the insurer/state if the price of service or good exceeds the reimbursement amount (balance billing/extra billing/reference pricing).
- The Health Systems in Transition (HiT) country profiles by the European Observatory on Health Systems and Policies;
- The State of Health in the EU country profiles by the OECD and the European Observatory on Health Systems and Policies;
- Universal Health Coverage: Financial Protection Country Reviews by the WHO Regional Office for Europe;
- The Health at a Glance report series by the OECD and the EU.
3. Results
3.1. Healthcare Expenditure
3.2. Healthcare Coverage
3.2.1. Population Coverage
3.2.2. Service Coverage and Quality of Care
3.3. Patient Cost Sharing for Goods and Services in a Benefit Package
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fischer, S.; Gelb, A. The Process of Socialist Economic Transformation. J. Econ. Perspect. 1991, 5, 91–105. [Google Scholar] [CrossRef]
- Ekiert, G.; Hanson, S.E. (Eds.) Capitalism and Democracy in Central and Eastern Europe; Cambridge University Press: Cambridge, UK, 2003. [Google Scholar]
- Dobry, M. (Ed.) Democratic and Capitalist Transitions in Eastern Europe. Lessons for the Social Sciences; Kluwer Academic Publisher: Dordrecht, The Netherlands, 2000. [Google Scholar]
- Kollmorgen, R. Theories of Postcommunist Transformation. Approaches, Debates, and Problems of Theory Building in the Second Decade of Research. Stud. Transit. States Soc. 2013, 5, 89–105. [Google Scholar]
- Petsinis, V. Twenty years after 1989: Moving on from transitology. Contemp. Politics 2010, 16, 301–319. [Google Scholar] [CrossRef]
- Papava, V. On the Theory of Post-Communist Economic Transition to Market. Int. J. Soc. Econ. 2005, 32, 77–97. [Google Scholar] [CrossRef]
- Stiglitz, J.E. Another century of economic science. In The Future of Economics; Hey, J.D., Ed.; Blackwell: Oxford, UK, 1992; pp. 134–141. [Google Scholar]
- Kutzin, J.; Cashin, C.; Jakab, M. (Eds.) Implementing Health Financing Reform: Lessons from Countries in Transition; World Health Organization Regional Office for Europe, on behalf of the European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2010. [Google Scholar]
- Rechel, B.; McKee, M. Health reform in central and Eastern Europe and the former Soviet Union. Lancet 2009, 374, 1186–1195. [Google Scholar] [CrossRef]
- Preker, A.; Jakab, M.; Schneider, M. Health financing reforms in central and eastern Europe and the former Soviet Union. In Funding Health Care: Options for Europe; Mossialos, E., Dixon, A., Figueras, J., Kutzin, J., Eds.; Open University Press: Buckingham, UK, 2002; pp. 80–109. [Google Scholar]
- Marrée, J.; Groenewegen, P.P. Back to Bismarck: Eastern European Health Care Systems in Transition; Atheneum Press, Ltd.: Avebury, UK, 1997. [Google Scholar]
- Björkman, J.W.; Nemec, J. (Eds.) Health reforms in Central and Eastern Europe; Options, Obstacles, Limited Outcomes; Eleven International Publishing: The Hague, The Netherlands, 2013. [Google Scholar]
- Shakarishvili, G. Poverty and Equity in Healthcare Finance: Analyzing Post-Soviet Healthcare Reform; Local Government and Public Service Reform Initiative Open Society Institute: Budapest, Hungary, 2006. [Google Scholar]
- Tambor, M.; Pavlova, M.; Woch, P.; Groot, W. Diversity and dynamics of patient cost-sharing for physicians’ and hospital services in the 27 European Union countries. Eur. J. Public Health. 2010, 21, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Mossialos, E.; Dixon, A.; Figueras, J.; Kutzin, J. (Eds.) Funding Health Care: Options for Europe; Open University Press: Buckingham, UK, 2002. [Google Scholar]
- Davis, C. Understanding the legacy: Health financing systems in the USSR and central and eastern Europe prior to transition. In Implementing Health Financing Reform: Lessons from Countries in Transition; Kutzin, J., Cashin, C., Jakab, M., Eds.; World Health Organization Regional Office for Europe, on behalf of the European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2010; pp. 25–65. [Google Scholar]
- Thompson, R.; Witter, S. Informal payments in transitional economies: Implications for health sector reform. Int. J. Health Plann. Manag. 2000, 15, 169–187. [Google Scholar] [CrossRef]
- Stepurko, T.; Pavlova, M.; Gryga, I.; Groot, W. Empirical studies on informal patient payments for health care services: A systematic and critical review of research methods and instruments. BMC Health Serv. Res. 2010, 10, 273. [Google Scholar] [CrossRef]
- Thomson, S.; Evetovits, T.; Kluge, H. Universal health coverage and the economic crisis in Europe. Eurohealth 2016, 22, 18. [Google Scholar]
- World Health Organization. Strengthening health systems for universal health coverage and sustainable development. Bull. World Health Organ. 2017, 95, 537–539. [Google Scholar] [CrossRef]
- Golinowska, S.; Kocot, E.; Sowa, A. Development of Scenarios for Health Expenditure in the New EU Member States: Bulgaria, Estonia, Hungary, Poland and Slovakia; CASE Network Reports; CASE-Center for Social and Economic Research: Warsaw, Poland, 2008. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Czechia: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Estonia: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Hungary: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Latvia: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Lithuania: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Poland: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Slovakia: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Slovenia: Country Health Profile 2019; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2019. [Google Scholar]
- United Nations Development Programme. Human Development Report. Beyond Income, Beyond Averages, Beyond Today: Inequalities in Human Development in the 21st Century; RR Donnelley Company: New York, NY, USA, 2019. [Google Scholar]
- World Bank. Worldwide Governance Indicators. Available online: http://info.worldbank.org/governance/WGI (accessed on 10 January 2021).
- ISSP Research Group. International Social Survey Programme: Role of Government V—ISSP 2016. GESIS Data Archive. ZA6900 Data File Version 2.0.0. Cologne. 2018. Available online: https://dbk.gesis.org/dbksearch/sdesc2.asp?no=6900&db=e&doi=10.4232/1.13052 (accessed on 10 January 2021).
- OECD Health Statistics Online Database. Available online: https://stats.oecd.org/Index.aspx?ThemeTreeId=9 (accessed on 20 July 2020).
- WHO. Global Health Expenditure Database. Available online: https://apps.who.int/nha/database/Select/Indicators/en (accessed on 10 January 2021).
- Thomson, S.; Evetovits, T.; Cylus, J. Financial Protection in High-Income Countries. A comparison of the Czech Republic, Estonia and Latvia; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar]
- Alexa, J.; Rečka, L.; Votápková, J.; van Ginneken, E.; Spranger, A.; Wittenbecher, F. Czech Republic: Health system review. Health Syst. Transit. 2015, 17, 1–165. [Google Scholar] [PubMed]
- Health Insurance Bureau. Health Insurance System in the Check Republic. Available online: https://www.kancelarzp.cz/en/links-info-en/health-insurance-system-in-cz (accessed on 10 January 2021).
- Habicht, T.; Reinap, M.; Kasekamp, K.; Sikkut, R.; Aaben, L.; van Ginneken, E. Estonia: Health system review. Health Syst. Transit. 2018, 20, 1–193. [Google Scholar] [PubMed]
- Võrk, A.; Habicht, T. Can People Afford to Pay for Health Care? New Evidence on Financial Protection in Estonia; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Habicht, T.; Gaps in Health Insurance Coverage Gain Evidence Basis. Health Systems in Transition (HiT) Profile of Estonia. The Health Systems and Policy Monitor. European Observatory on Health Systems and Policies. 2018. Available online: https://www.hspm.org/countries/estonia05112013/livinghit.aspx?Section=3.3%20Overview%20of%20the%20statutory%20financing%20system&Type=Section#26Gapsinhealthinsurancecoveragegainevidencebasis (accessed on 30 July 2020).
- Gaál, P.; Szigeti, S.; Csere, M.; Gaskins, M.; Panteli, D. Hungary: Health system review. Health Syst. Transit. 2011, 13, 1–266. [Google Scholar] [PubMed]
- Szigeti, S.; Evetovits, T.; Kutzin, J.; Gaál, P. Tax-Funded Social Health Insurance: An Analysis of Revenue Sources. Bull. World Health Organ. 2019, 97, 335. [Google Scholar] [CrossRef] [PubMed]
- Behmane, D.; Dudele, A.; Villerusa, A.; Misins, J.; Kļaviņa, K.; Mozgis, D.; Scarpetti, G. Latvia: Health system review. Health Syst. Transit. 2019, 21, 1–165. [Google Scholar]
- Taube, M.; Vaskis, E.; Nesterenko, O. Can People Afford to Pay for Health Care? New Evidence from Latvia; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Murauskienė, L.; Thomson, S. Can People Afford to Pay for Health Care? New Evidence from Lithuania; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Murauskiene, L.; Janoniene, R.; Veniute, M.; van Ginneken, E.; Karanikolos, M. Lithuania: Health system review. Health Syst. Transit. 2013, 15, 1–150. [Google Scholar] [PubMed]
- Sowada, C.; Sagan, A.; Kowalska-Bobko, I.; Badora-Musiał, K.; Bochenek, T.; Domagała, A.; Dubas-Jakóbczyk, K.; Kocot, E.; Mrożek-Gąsiorowska, M.; Sitko, S.; et al. Poland: Health System Review. Health Syst. Transit. 2019, 21, 1–235. [Google Scholar]
- Tambor, M.; Pavlova, M. Can People Afford to Pay for Health Care? New Evidence from Poland; WHO Regional Office for Europe: Copenhagen, Demark, 2019. [Google Scholar]
- Smatana, M.; Pažitný, P.; Kandilaki, D.; Laktišová, M.; Sedláková, D.; Palušková, M.; van Ginneken, E.; Spranger, A. Slovakia: Health system review. Health. Syst. Transit. 2016, 18, 1–210. [Google Scholar]
- Löffler, L.; Pažitný, P.; Fluctuations in Revenues by a Flexible Contribution Base for State-Insured. Health Systems in Transition (HiT) Profile of Slovakia. The Health Systems and Policy Monitor. European Observatory on Health Systems and Policies. 2019. Available online: https://www.hspm.org/countries/slovakia24102017/livinghit.aspx?Section=3.3%20Overview%20of%20the%20statutory%20financing%20system&Type=Section#13Fluctuationsinrevenuesbyaflexiblecontributionbaseforstate-insured (accessed on 30 July 2020).
- Albreht, T.; Pribaković Brinovec, R.; Jošar, D.; Poldrugovac, M.; Kostnapfel, T.; Zaletel, M.; Panteli, D.; Maresso, A. Slovenia: Health system review. Health Syst. Transit. 2016, 18, 1–207. [Google Scholar]
- European Commission. Council Directive 89/105/EEC of 21 December 1988 Relating to the Transparency of Measures Regulating the Pricing of Medicinal Products for Human Use and Their Inclusion in the Scope of National Health Insurance Systems. Available online: https://ec.europa.eu/health/sites/health/files/files/eudralex/vol-1/dir_1989_105/dir_1989_105_en.pdf (accessed on 20 July 2020).
- OECD/EU. Health at a Glance: Europe 2020: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2020. [Google Scholar]
- Thomson, S.; Figueras, J.; Evetovits, T.; Jowett, M.; Mladovsky, P.; Maresso, A.; Kluge, H. Economic Crisis, Health Systems and Health in Europe: Impact and Implications for Policy; World Health Organization, Regional Office for Europe: Copenhagen, Demark, 2015. [Google Scholar]
- Kawalec, P.; Tesar, T.; Vostalova, L.; Draganic, P.; Manova, M.; Savova, A.; Petrova, G.; Rugaja, Z.; Männik, A.; Sowada, C.; et al. Pharmaceutical regulation in central and Eastern European countries: A current review. Front. Pharmacol. 2017, 8, 892. [Google Scholar] [CrossRef]
- Björnberg, A.; Yung Phang, A. Euro Health Consumer Index 2018 Report; Health Consumer Powerhouse: Stockholm, Sweden, 2019. [Google Scholar]
- World Health Organization. Universal Health Coverage. Available online: http://apps.who.int/gho/portal/uhc-cabinet-wrapper-v2.jsp?id=1010501 (accessed on 23 July 2020).
- OECD; European Observatory on Health Systems and Policies. Slovakia: Country Health Profile 2017; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2017. [Google Scholar]
- OECD; European Observatory on Health Systems and Policies. Slovenia: Country Health Profile 2017; State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2017. [Google Scholar]
- Fall, F.; Glocker, D. Improving the Czech Health Care System; OECD Economics Department Working Papers; OECD Publishing: Paris, France, 2018; Volume 1522. [Google Scholar]
- World Health Organization. Medicines Reimbursement Policies in Europe; WHO Regional Office for Europe: Copenhagen, Demark, 2018. [Google Scholar]
- Baji, P.; Pavlova, M.; Gulácsi, L.; Zsófia, H.C.; Groot, W. Informal payments for healthcare services and short-term effects of the introduction of visit fee on these payments in Hungary. Inter. J. Health Plann. Manag. 2012, 27, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Tambor, M.; Pavlova, M.; Golinowska, S.; Sowada, C.; Groot, W. The formal–informal patient payment mix in European countries. Governance, economics, culture or all of these? Health Policy 2013, 113, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Dieleman, J.L.; Sadat, N.; Chang, A.Y.; Fullman, N.; Abbafati, C.; Acharya, P.; Alkerwi, A.A. Trends in future health financing and coverage: Future health spending and universal health coverage in 188 countries, 2016–2040. Lancet 2018, 391, 1783–1798. [Google Scholar] [CrossRef]
- Lozano, R.; Fullman, N.; Mumford, J.E.; Knight, M.; Barthelemy, C.M.; Abbafati, C.; Abolhassani, H. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1250–1284. [Google Scholar] [CrossRef]
- Stepovic, M.; Rancic, N.; Vekic, B.; Dragojevic-Simic, V.; Vekic, S.; Ratkovic, N.; Jakovljevic, M. Gross Domestic Product and Health Expenditure Growth in Balkan and East European Countries—Three-Decade Horizon. Front. Public Health 2020, 8, 492. [Google Scholar] [CrossRef] [PubMed]
- Tambor, M.; Pavlova, M.; Golinowska, S.; Sowada, C.; Groot, W. Towards a stakeholders’ consensus on patient payment policy: The views of health-care consumers, providers, insurers and policy makers in six Central and Eastern European countries. Health Expect. 2015, 18, 475–488. [Google Scholar] [CrossRef]
- Eurostat Online Database. European Health Interview Survey. Available online: https://ec.europa.eu/eurostat/cache/metadata/fr/hlth_det_esms.htm (accessed on 28 July 2020).
- Stepurko, T. Informal Patient Payments in Central and Eastern European Countries. Ph.D. Thesis, Maastricht University, Maastricht, The Netherlands, 2013. Available online: https://cris.maastrichtuniversity.nl/en/publications/informal-patient-payments-in-central-and-eastern-european-countri (accessed on 28 June 2020).
- Riklikiene, O.; Jarasiunaite, G.; Starkiene, L. Informal patient payments in publicly financed healthcare facilities in Lithuania. Scand. J. Public Health. 2014, 42, 488–496. [Google Scholar] [CrossRef]
- European Commission. Special Eurobarometer 470, Corruption. Available online: http://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/Survey/getSurveyDetail/instruments/SPECIAL/surveyKy/2176 (accessed on 2 February 2021).
- Papp, M.; Kőrösi, L.; Sándor, J.; Nagy, C.; Juhász, A.; Ádány, R. Workforce crisis in primary healthcare worldwide: Hungarian example in a longitudinal follow-up study. BMJ Open 2019, 9, e024957. [Google Scholar] [CrossRef]
- European Union. ESPN Thematic Report on Inequalities in Access to Healthcare. Slovenia; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Domagała, A.; Klich, J. Planning of Polish physician workforce—Systemic inconsistencies, challenges and possible ways forward. Health Policy 2018, 122, 102–108. [Google Scholar] [CrossRef]
- European Commission. Eurostat. Income and Living Conditions. Available online: https://ec.europa.eu/eurostat/web/income-and-living-conditions/data/database (accessed on 27 July 2020).
- Mitenbergs, U.; Brigis, G.; Quentin, W. Healthcare financing reform in Latvia: Switching from social health insurance to NHS and back? Health Policy 2014, 118, 147–152. [Google Scholar] [CrossRef]
- World Health Organization. WHO Notes on Health System Financing Policy in Latvia: Opportunities and Challenges in Light of International Experience. July 2016. Available online: http://www.vm.gov.lv/images/files/Latvia_meeting_report_WHO_2016_final_13_July_%281%29.pdf (accessed on 27 July 2020).
- Thomson, S.; Mossialos, E. Private Health Insurance in the European Union; European Commission: Brussels, Belgium, 2009. [Google Scholar]


{kind=link}
| Czechia | Estonia | Hungary | Latvia | Lithuania | Poland | Slovakia | Slovenia | |
|---|---|---|---|---|---|---|---|---|
| Population (thousands) (2018) | 10,610 | 1319 | 9778 | 1934 | 2809 | 37,977 | 5443 | 2067 |
| Population density (persons per km2) (2018) | 137.7 | 30.4 | 107.1 | 30.4 | 44.7 | 123.6 | 111.8 | 102.9 |
| Life expectancy at birth, total (years) (2018) | 79.1 | 78.5 | 76.2 | 75.1 | 76.0 | 77.7 | 77.4 | 81.5 |
| Old-age dependency ratio (2018) | 29.6 | 30.6 | 28.5 | 31.4 | 30.1 | 25.3 | 22.5 | 29.6 |
| GDP per capita, PPP (current international $) (2018) | 41,036 | 36,222 | 32,086 | 30,736 | 36,011 | 31,851 | 32,538 | 38,841 |
| Human Development Index † (2018) | 0.898 | 0.889 | 0.850 | 0.863 | 0.876 | 0.877 | 0.858 | 0.912 |
| Government Effectiveness Index ‡ (2018) | 0.92 | 1.19 | 0.49 | 1.04 | 1.07 | 0.66 | 0.71 | 1.13 |
| Healthcare for the sick: percentage claiming it should be the government’s responsibility (2016) § | 95.8 | n.d. | 98.0 | 98.0 | 96.0 | n.d. | 98.2 | 98.9 |
| 2000 | 2018 | Min. Annual Growth Rate (Year) | Max. Annual Growth Rate (Year) | Regression Model | |
|---|---|---|---|---|---|
| Current health expenditure as % of GDP | |||||
| Czechia | 5.72 | 7.65 | −5.4 (2015) | 14.7 (2009) | y = 0.098x + 5.790, R2 = 0.758, p < 0.01 |
| Estonia | 5.16 | 6.66 | −8.0 (2011) | 14.6 (2008) | y = 0.111x + 4.553, R2 = 0.784, p < 0.01 |
| Hungary | 6.78 | 6.70 | −7.3 (2007) | 14.0 (2003) | y = −0.027x + 7.542, R2 = 0.129, p = 0.131 |
| Latvia | 5.45 | 6.21 | −9.3 (2011) | 13.4 (2004) | y = 0.011x + 5.661, R2 = 0.046, p = 0.376 |
| Lithuania | 6.19 | 6.57 | −10.9 (2004) | 17.0 (2009) | y = 0.037x + 5.891, R2 = 0.233, p < 0.05 |
| Poland | 5.30 | 6.33 | −3.2 (2018) | 8.5 (2008) | y = 0.050x + 5.643, R2 = 0.644, p < 0.01 |
| Slovakia | 5.30 | 6.69 | −8.2 (2014) | 18.7 (2004) | y = 0.090x + 5.828, R2 = 0.395, p < 0.01 |
| Slovenia | 7.80 | 8.33 | −4.0 (2007) | 8.7 (2009) | y = 0.043x + 7.787, R2 = 0.439, p < 0.01 |
| Domestic general government health expenditure as % of general government expenditure | |||||
| Czechia | 12.38 | 15.54 | −4.6% (2003) | 15.8 (2013) | y = 0.195x + 11.508, R2 = 0.824, p < 0.01 |
| Estonia | 10.80 | 12.54 | −6.6 (2002) | 5.6 (2003) | y = 0.119x + 10.191, R2 = 0.851, p < 0.01 |
| Hungary | 9.86 | 9.92 | −8.1 (2007) | 19.7 (2003) | y = −0.045x + 10.523, R2 = 0.154, p = 0.097 |
| Latvia | 7.43 | 9.60 | −9.2 (2008) | 23.7 (2004) | y = 0.037x + 8.468, R2 = 0.083, p = 0.232 |
| Lithuania | 10.57 | 12.70 | −25.9 (2004) | 11.8 (2002) | y = 0.067x + 10.947, R2 = 0.141, p = 0.113 |
| Poland | 8.59 | 10.83 | −5.2 (2010) | 8.1 (2008) | y = 0.132x + 8.561, R2 = 0.872, p < 0.01 |
| Slovakia | 8.89 | 12.65 | −7.6 (2015) | 17.0 (2001) | y = 0.129x + 11.112, R2 = 0.336, p < 0.01 |
| Slovenia | 11.72 | 13.80 | −18.5 (2013) | 15.7 (2014) | y = 0.053x + 11.774, R2 = 0.157, p = 0.093 |
| Government/compulsory scheme expenditure as % of current health expenditure | |||||
| Czechia | 89.80 | 83.03 | −3.1 (2008) | 1.4 (2009) | y = –0.472x + 89.835, R2 = 0.801, p < 0.01 |
| Estonia | 76.97 | 73.67 | −2.7 (2017) | 1.8 (2001) | y = −0.122x + 77.231, R2 = 0.312, p < 0.05 |
| Hungary | 69.65 | 69.45 | −2.7 (2007) | 2.0 (2002) | y = −0.129x + 69.903, R2 = 0.224, p < 0.05 |
| Latvia | 50.75 | 59.88 | −5.0 (2012) | 12.7 (2004) | y = 0.499x + 52.309, R2 = 0.393, p < 0.01 |
| Lithuania | 68.51 | 67.05 | −11.7 (2004) | 5.2 (2007) | y = −0.272x + 71.969, R2 = 0.280, p < 0.05 |
| Poland | 68.88 | 71.49 | −2.0 (2004) | 3.1 (2001) | y = 0.059x + 69.543, R2 = 0.085, p = 0.226 |
| Slovakia | 89.16 | 80.13 | −11.6 (2004) | 8.7 (2008) | y = −0.425x + 82.591, R2 = 0.135, p = 0.121 |
| Slovenia | 72.90 | 72.93 | −2.2 (2007) | 2.8 (2008) | y = −0.043x + 73.042, R2 = 0.083, p = 0.231 |
| Out-of-pocket health expenditure as % of current health expenditure | |||||
| Czechia | 10.20 | 14.19 | −11.2 (2013) | 18.4 (2008) | y = 0.300x + 10.242, R2 = 0.629, p < 0.01 |
| Estonia | 20.37 | 24.56 | −8.5 (2008) | 9.4 (2017) | y = 0.186x + 20.127, R2 = 0.516, p < 0.01 |
| Hungary | 27.33 | 26.89 | −4.5 (2002) | 5.4 (2001) | y = 0.053x + 26.637, R2 = 0.068, p = 0.280 |
| Latvia | 47.66 | 39.18 | −16.3 (2004) | 10.3 (2012) | y = −0.404x + 44.834, R2 = 0.258, p < 0.05 |
| Lithuania | 27.15 | 31.64 | −10.8 (2007) | 36.1 (2004) | y = 0.291x + 26.873, R2 = 0.338, p < 0.01 |
| Poland | 31.12 | 20.42 | −10.5% (2018) | 6.8 (2004) | y = −0.457x + 29.897, R2 = 0.867, p < 0.01 |
| Slovakia | 10.84 | 18.91 | −23.2 (2008) | 71.2 (2004) | y = 0.335x + 16.230, R2 = 0.134, p = 0.123 |
| Slovenia * | 12.47 | 11.93 | −7.3 (2008) | 11.1 (2007) | y = −0.033x + 12.905, R2 = 0.133, p = 0.165 |
| Current Health Expenditure as % of GDP | Domestic General Government Health Expenditure as % of General Government Expenditure | Government/Compulsory Scheme Expenditure as % of Current Health Expenditure | Out-of-Pocket Health Expenditure as % of Current Health Expenditure | |
|---|---|---|---|---|
| Coeff. (S.E.) | Coeff. (S.E.) | Coeff. (S.E.) | Coeff. (S.E.) | |
| Time | 0.052 *** (0.007) | 0.086 *** (0.012) | −0.113 * (0.048) | 0.037 (0.046) |
| Czechia | 1.105 *** (0.145) | 2.080 *** (0.254) | 9.109 *** (1.043) | −8.743 *** (0.973) |
| Estonia | ref. | ref. | ref. | ref. |
| Hungary | 1.607 *** (0.145) | −1.307 *** (0.254) | −7.394 *** (1.043) | 5.185 *** (0.963) |
| Latvia | 0.109 (0.145) | −2.541 *** (0.254) | −18.716 *** (1.043) | 18.812 *** (0.963) |
| Lithuania | 0.599 *** (0.145) | 0.234 (0.254) | −6.7574 *** (1.043) | 7.798 *** (0.963) |
| Poland | 0.472 ** (0.145) | −1.497 ***(0.254) | −5.879 *** (1.043) | 3.349 *** (0.963) |
| Slovakia | 1.064 *** (0.145) | 1.024 *** (0.254) | 2.329 * (1.043) | −2.399 * (0.963) |
| Slovenia | 2.547 *** (0.145) | 0.926 *** (0.254) | −3.396 ** (1.043) | −9.457 *** (0.963) |
| Constant | 5.149 *** (0.122) | 10.521 *** (0.213) | 77.141 *** (0.878) | 21.608 *** (0.825) |
| Observations | 152 | 152 | 152 | 149 |
| F test | F(8, 143) = 66.82 *** | F(8, 143) = 71.23 *** | F(8, 143) = 108.1 *** | F(8, 140) = 161.5 *** |
| R-squared | 0.789 | 0.799 | 0.858 | 0.897 |
| Adj. R-squared | 0.777 | 0.788 | 0.850 | 0.891 |
| Country | Basis for Entitlement | % of Population Covered | Noncovered Groups | Contribution Paid by the Government or Coverage without Contribution Paid on Behalf of Noncontributors | Additional Information |
|---|---|---|---|---|---|
| Czechia | Participation in insurance scheme [35]. | 100% [36,37]. | n/a | State-paid contribution for 17 population groups (58% of population), including children and students up to the age of 26, disabled people, pensioners, the unemployed, and informal caregivers [22,38]. | The contribution for state-insured groups is fixed and substantially lower than an average contribution from salary [22]. |
| Estonia | Participation in insurance scheme [39]. | 94–95% [36,39,40]. | Individuals working abroad and those inactive/unemployed or with nonstandard employment [23,40,41]. | State-paid contribution for 24% of the insured (e.g., pensioners, people on parental leave, caregivers). No contribution is paid for ~26% of the covered population (e.g., children, students up to the age of 24, the unemployed) [23,39,40]. | The government started paying contributions for pensioners in 2018 in order to increase the financial stability of the system [23,39]. Health coverage has been gradually extended, e.g., registered jobseekers were included in 2007 [39,40]. |
| Hungary | Participation in insurance scheme [24,42]. | 94–95% [24,36,42,43]. | Individuals working abroad or without a fixed address [24]. | State-paid contribution for selected groups, mainly pensioners, minors, students [42]. | The government pays for a significant share of the health insurance fund exceeding revenues from wage-based health insurance contributions [43]. In practice, noncovered individuals also receive necessary healthcare services [24,42]. |
| Latvia | Residence [25]. | 100% [25,36,44]. | n/a | n/a | Between 2018 and 2019, a mandatory health insurance system was in place. The full benefit package was available for individuals paying the insurance contribution and to those in one of 21 population groups covered by the state (e.g., children, pensioners). Others were granted access to a minimum benefit package financed by the state (emergency care, primary care, maternity care, psychiatric care, treatment of infectious diseases, and reimbursement of pharmaceuticals) [25,45]. |
| Lithuania | Participation in insurance scheme [46]. | 98% [26,36]. | Individuals not in regular employment, people working abroad [26]. | State-paid contribution for 55–60% of the population, including pensioners, social assistance beneficiaries, children under 18, students, registered unemployed, disabled individuals, patients suffering from certain communicable diseases [46,47]. | Emergency healthcare is provided free of charge to all permanent residents irrespective of their insurance status [26,47]. |
| Poland | Participation in insurance scheme [48,49]. | 91–93% [27,36,48,49]. | Individual working abroad, nonregistered family members, nonregistered homeless or unemployed people [27,49]. | State-paid contribution for farmers of small farms, registered jobseekers, recipients of income support, clergy, children, and students if they are not co-insured family members. No contribution is paid for co-insured family members (22% of the insured population) [48,49]. | For pregnant women and children under 18, the right to publicly financed healthcare can be granted irrespective of their insurance status. Since 2017, all people, regardless of insurance status, have had free access to primary care. Individuals not insured but eligible for public coverage can be insured retroactively avoiding out-of-pocket payments [27,48,49]. |
| Slovakia | Participation in insurance scheme [28,50]. | 94–96% [28,36,50]. | Mostly individuals working abroad [28,50]. | State-paid contribution for the economically inactive (dependent family members, students and pensioners) (in total >50% of population) [28,50]. | The insurance rate of the state-paid contribution has been fluctuating over the years, and now it is lower than the rate for the economically active, contributing to a financial deficit in healthcare system [51]. |
| Slovenia | Participation in insurance scheme [29,52]. | 99.5–100% [29,36,52]. | Ethnic minorities, undocumented migrants, and nonregistered homeless people [29,36,52]. | State-paid contribution for pensioners, the unemployed, individuals without income, prisoners, and war veterans [52]. | In addition to public coverage, about 95% of the population purchase voluntary health insurance to cover obligatory patient payments [29]. |
| Country | Benefit Package | Example of Included/Excluded Services | Quality and Access to Healthcare | Changes in the Benefit Package | Additional Information †,‡ |
|---|---|---|---|---|---|
| Czechia | Positive list of services, medicines, medical products. Negative list of services explicitly excluded [37]. | Included: in vitro fertilization, spa treatments, over-the-counter medicines (if prescribed), dental care (least expensive options) [22,37]. Excluded: cosmetic surgery, dental treatments, voluntary abortions, employer-requested health examinations, medical certificates, some medical aids, e.g., prescription glasses [22,37]. | There might be limitations on volume of services provided by specific providers [37]. No problems with waiting times [33]. Regional disparities in the distribution of physicians [22] 4.0 doctors and 8.1 nurses per 1000 population [54]. | During the economic crisis of 2008, dental benefits were restricted [55]. Periodic (several times a year) amendments of the medicine list [56]. | Services not included on the positive list may still be reimbursed, depending on the needs of individual patients. Also, there are exceptional cases in which items on the negative list may be reimbursed [37]. UHC service coverage index: 76 [57]. HCI: 731 points (14th place) [57]. |
| Estonia | Positive lists of services, medicines, medical products [39]. | Included: dental care for children, most essential dental services for adults [23,39,40]. Excluded: cosmetic surgery, alternative therapies, optician services [39,40]. | Maximum waiting time guarantees, however often not met for specialist services [23,40]. Medical professional shortages, particularly nurses [23]. 3.0 doctors and 6.3 nurses per 1000 population [54]. | Between 2002 and 2017, cash benefit instead of in-kind dental care benefits for adults). Coverage of dental care for adults restricted during the economic crisis of 2008, restored in 2017 [23,39]. Benefit package updated at least once a year [23]. | UHC service coverage index: 75 [58]. HCI: 729 points (15th place) [57]. |
| Hungary | Negative list of services. Positive and negative list of medicines [42,57]. | Included: spa treatment, infertility treatments (limits on number of benefits) [42]. Excluded: cosmetic surgery, medical certificates, abortion or sterilization without medical indication, selected dental services for adults [42]. | Performance volume limit set for each provider [24]. Long waiting times [42]. Shortages and uneven distribution of medical professionals [24]. 3.4 doctors and 6.6 nurses per 1000 population [54]. | Ad hoc revision of medicine lists [56]. | UHC service coverage index: 74 [58]. HCI: 565 points (33rd place) [57]. |
| Latvia | Positive list of medicines and certain services. Negative lists of services explicitly excluded [25]. | Included: dental care for children [39] Excluded: dental care for adults, some rehabilitation services, employer-requested health examinations, sight correction, hearing aids for adults, psychotherapy, spa treatment, abortion (if no medical or social indications) [44,45]. | Volume limits on contracted services. Lack of waiting time guarantees and long waiting times [25,44,45]. Shortages and uneven geographical distribution of medical professionals [25]. 3.3 doctors and 4.4 nurses per 1000 population [54]. | Reduction of benefit package after the economic crisis in 2008 [45]. Periodic (every 3 months) amendments of the medicine list [56]. | The scope of the benefit package is considered relatively limited, particularly for outpatient care, medicines, medical devices [25,45]. UHC service coverage index: 71 [58]. HCI: 605 points (30th place) [57]. |
| Lithuania | No explicitly defined list of services. Positive list of medicines and medical products [26,46]. | Included: dental care for children and individuals on income support, in vitro fertilization (since 2017) [26,46,47]. Excluded: dental care for adults, medical certificates, nonmedical cosmetics, over-the counter medicines, occupational health check-ups, abortions, substance abuse treatment [26,46,47]. | Long waiting times [46]. Uneven geographical distribution of medical professionals; shortages of nurses [26]. 4.6 doctors and 7.8 nurses per 1000 population [54]. | Periodic revision of medicine list since 2019 [26]. | Coverage of pharmaceuticals and medical products is limited [26,46]. UHC service coverage index: 73 [58]. HCI: 622 points (28th place) [57]. |
| Poland | Positive lists for services, medicines, medical products [48,49]. | Included: spa treatment, basic dental services for adults with more services for children [48,49]. Excluded: most dental care for adults, medical certificates and nonmedical cosmetics, over-the counter medicines, in vitro fertilization [48,49]. | Limits on the volume of services contracted. Lack of waiting time guarantees and long waiting times [27,49]. Sever shortages of medical professionals and their uneven distribution [27]. 2.4 doctors and 5.1 nurses per 1000 population [54]. | Periodic (every 2 months) amendments of the medicine list [56]. Ad hoc revision of the service list. In vitro fertilization was covered between 2013 and 2016, and then was excluded due to political reasons [48]. | Lists of guaranteed services in primary care, outpatient specialist care, and hospital care are fairly comprehensive. In the case of some services (rehabilitation, dental care, medical products), limits on the number of services to be provided per person [27,49]. UHC service coverage index: 75 [58]. HCI: 585 points (32nd place) [57]. |
| Slovakia | Positive list of services, medical products and medicines [50]. | Included: spa treatment, some dental services for adults [50]. Excluded: most dental care, patient-requested anesthesia, paternity tests, specialist visits without referral, treatment caused by substance abuse, cosmetic plastic surgery, abortion upon request of the patient, sterilization [50,59]. | Budget ceilings resulting in waiting times for specialists [59]. Shortages of healthcare professionals and their uneven distribution [28]. 3.5 doctors and 5.7 nurses per 1000 population [54]. | Periodic (every 3 months) amendments of the medicine list [56]. | The benefit package is broadly defined. Some attempts to define a narrower benefit package (2002–2004) were unsuccessful [59]. UHC service coverage index: 77 [58]. HCI: 722 points (17th place) [57]. |
| Slovenia | The list of covered services only broadly defined [52,60]. Positive and negative list of medicines [52]. | Included: dental care for children and adults, contraception, infertility treatment, artificial insemination, sterilization, abortion, costs of travel to health facilities. Excluded: cosmetic surgery [52]. | Maximum waiting times, but not always met for specialist care [29,52]. Low number of physicians [29]. 3.2 doctors and 10.1 nurses per 1000 population [54]. | Although the majority of services are covered, they might be subject to percentage co-payments (up to 90%) (see: section on patient cost sharing). UHC service coverage index: 79 [58]. HCI: 678 points (21st place) [57]. |
| Country | Cost Sharing for Outpatient Services (GPs and/or specialists) and Inpatient Hospital Services | Cost Sharing for Outpatient Medicines | Cost Sharing for other Goods and Services | Protection Mechanisms (Co-Payment Limits, Exemptions) | Additional Information |
|---|---|---|---|---|---|
| Czechia | None (except for ambulatory services outside standard office hours) [22,37,61]. | The difference between the price and the reimbursement amount [22]. | Payments for medical products and dental care beyond the standard package (cost above the reimbursement amounts) [22,37,61]. | A yearly payment limit of 5000 CZK (~€200) for payments for medicines. Lower limits apply to children up to 18 years of age and seniors (both since 2018), as well as disabled people (since 2020). Selected vulnerable groups are fully exempt [22,37]. | Between 2008 and 2015, there were co-payments for services: 30 CZK (€1.20) per doctor visit, 60 CZK (€2.40) (100 CZK since 2011) per hospital day. There was also cost sharing for medicines in the form of a flat fee of 30 CZK (€1.20) for each prescribed pharmaceutical (since 2012 per prescription). Due to the unpopularity of user fees, some local governments (controlled by the opposition) had reimbursed patients for the user charges before fees were fully abolished in 2015 [37,61]. |
| Estonia | Co-payments for outpatient specialist care (€5 per visit), inpatient care (€2.50 per day), and primary care home visits (€5 per visit) (otherwise primary care free-of-charge) [39,40]. | Co-payment for each prescription (€2.50), a percentage co-payment (0%, 25%, 50%), and any additional costs above the reference price [39,40]. | Dental care for adults: percentage co-payment of 50% with a benefit cap of €40 per year (15% and €85 respectively for some vulnerable groups) For medical products: percentage co-payments of 10% or 50% [39]. | A cap on payments for hospital stays (€25 per hospitalization). Caps on payments for outpatient medicines, i.e., if the total spending on prescription medications in a year reaches €100, then the insurance fund starts to reimburse 50% of the cost above €100. This reimbursement rate increases up to 90% for out-of-pocket spending above €300. Over the years, these spending thresholds have been decreasing [23,39,40]. Exemption or fee reduction for selected vulnerable groups (children, pregnant women, pensioners) [40]. | Cost sharing for services was first introduced in 1995. The system was modified by the 2002 Health Insurance Act, which set the maximum co-payment levels. In 2013, the maximum fee level was increased. Cost sharing for dental care was introduced in 2017, when in-kind dental care was included in the benefit package [39]. |
| Hungary | None [42]. | Percentage co-payments (up to 75%) or a fixed co-payment. The co-payment rate depends on the therapeutic value of the medicine, the severity and status of the disease (with lower rates for more severe or longer lasting disease) [24,56,62]. | Different flat and percentage co-payment rates for medical products. Cost sharing for dental care (adults) [42]. | A monthly personal budget of up to 12,000 HUF (€40) to cover co-payments for prescribed medicines for specific vulnerable groups (the disabled, low-income individuals). Limited exemption scheme for some vulnerable population groups [24]. | Between 2007 and 2008, patients paid a flat co-payment of 300 HUF (approx. €1) per outpatient visit and a per diem for inpatient care (for max. 20 visits/days of hospitalization per year). The fees were withdrawn as a consequence of a nation-wide referendum [14,63]. |
| Latvia | Co-payment of €1.42 per primary care visit, €4.28 per specialist visit, and €10 per day of hospitalization [44,45]. | A flat fee of €0.71 per prescription or percentage co-payments of 25% or 50%, and any additional costs above the reference price [44,45]. | For medical products: a flat fee of €0.71 per prescription or percentage co-payments of 25% or 50%, and any additional costs above the reference price [44,45]. | Caps on the total annual payments for inpatient and outpatient services (€569 per person per year) and on payments for inpatient stay (€356 per hospitalization) (but no cap on payments for medicines and medical products). Exceptions from payments for some population groups, including children, pregnant women, people suffering from certain diseases, and since 2009, for low-income individuals [44,45]. | Flat co-payments were first implemented in 1995, and in the late 90s, a percentage co-payment (up to 25% of service costs) was applied to selected services. Due to the complexity of the system, in 2004, it was simplified with only flat co-payments remaining [64]. In 2009, due to fiscal pressure, patient payments increased substantially, resulting in weakened financial protection. Thus, in the subsequent years, some fee reduction took place [45]. |
| Lithuania | None (except for visits to specialists without referrals) [46,47] | Patients pay the full price for medicines unless they fall into certain vulnerable groups (children, pensioners, the disabled, low-income individuals), for which full or partial reimbursement is applied (list B of medicines), or suffer from certain diseases, e.g., tuberculosis, cancers, schizophrenia, metabolic diseases, or asthma, for which medicines are now fully reimbursed (list A of medicines). Everyone pays the costs above the reference price [26,47,56]. | None The majority of population pay the full price for medical products and dental care [46,47]. | A 50% reimbursement rate for medicines on list B for pensioners, partially disabled and recipients of social benefits. Full reimbursement is available for children, the severely disabled, people with specific conditions, and since 2020, for low-income older adults [26,47,56]. | Providers might charge patients the difference between the price and the actual cost of a treatment if patients opt for a treatment that is more expensive. There are concerns regarding the poor regulation and lack of transparency in these charges [46,47]. Since 2017, there have been significant changes in the reimbursement policy aimed at decreasing out-of-pocket payments for medicines. Before April 2019, there was percentage co-payment (50%, 20%, or 10%) for medicines on a disease-specific list (list A) [26]. |
| Poland | None [48,49]. | Fixed co-payment of PLN 3.20 (€0.7) or percentage co-payments of 30% or 50%, and any cost above the reference price [48,56]. | For medical products: payments on top of the reimbursement price if patients opt for more expensive products, and percentage co-payments for some products. No cost sharing for dental care. The majority of the population pay the full price for dental care [48,49]. | Exemptions apply to only a few groups, i.e., veterans, organ or blood donors, people aged 75+ (since 2016, for a broad range of medicines), pregnant women (since 2020, for certain medicines) children (only for some medical products) [48,49]. | Until 2010, extra billing in dental care was allowed, i.e., patients had had the possibility of opting for more expensive materials within the publicly financed system and pay any extra cost [49]. |
| Slovakia | None [50]. | Different percentage co-payment rates (0–100%) Many medicines (1/3) provided free of charge. Flat fee for prescription €0.17 [50,56]. | Different percentage co-insurance rates for medical products. Cost sharing for some dental services [50]. | Maximum limits for co-payments for prescribed medicines. A wide range of medical devices with individually reduced cost sharing [50]. | Between 2003 and 2006, co-payments for physician consultation, prescriptions (approximately €0.7), hospitalization (approximately €1.7 per day), and emergency care visits (approximately €2) were in place. In 2006, co-payments for outpatient and inpatient care were abolished, while other co-payments were reduced. Yet, providers continued to collect payments for health and health-related services. In 2015, a regulation was introduced banning such practices [50,64]. |
| Slovenia | Percentage co-payments from 10% to 90% depending on the type of services [52]. | Percentage co-payments (max. 30% for medicines on the positive list and min. 75% for medicines on the intermediate list) [52]. | Percentage co-payments for dental care and medical products | Exempt from cost sharing are: children, students, unemployed individuals, low-income individuals, pregnant women, and chronically ill people [52,60]. | Cost sharing was introduced in 1992 along with the compulsory health insurance system [14]. A vast majority of the population has private complementary insurance to cover cost-sharing obligations [52,60]. The economic crisis of 2008 led to an increase in co-payments [29]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tambor, M.; Klich, J.; Domagała, A. Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage? Int. J. Environ. Res. Public Health 2021, 18, 1382. https://doi.org/10.3390/ijerph18041382
Tambor M, Klich J, Domagała A. Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage? International Journal of Environmental Research and Public Health. 2021; 18(4):1382. https://doi.org/10.3390/ijerph18041382
Chicago/Turabian StyleTambor, Marzena, Jacek Klich, and Alicja Domagała. 2021. "Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage?" International Journal of Environmental Research and Public Health 18, no. 4: 1382. https://doi.org/10.3390/ijerph18041382
APA StyleTambor, M., Klich, J., & Domagała, A. (2021). Financing Healthcare in Central and Eastern European Countries: How Far Are We from Universal Health Coverage? International Journal of Environmental Research and Public Health, 18(4), 1382. https://doi.org/10.3390/ijerph18041382