
Effectiveness of Horticultural Therapy in People with Schizophrenia: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection of Articles
2.4. Quality Evaluation
2.5. Statistical Methods
2.5.1. Data Extraction
2.5.2. Statistical Analysis
3. Results
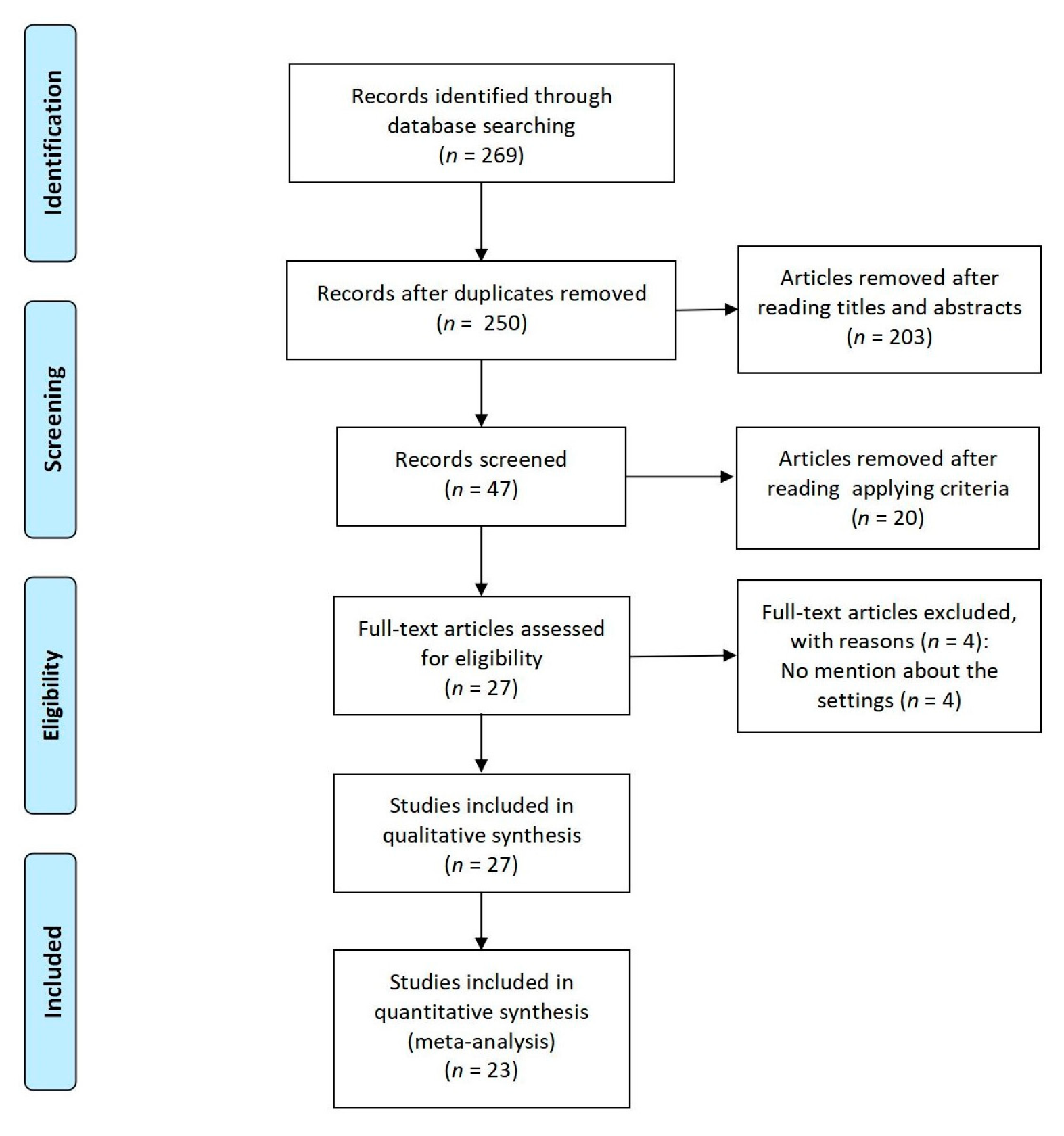
3.1. Search Outcomes
3.2. Study Characteristics
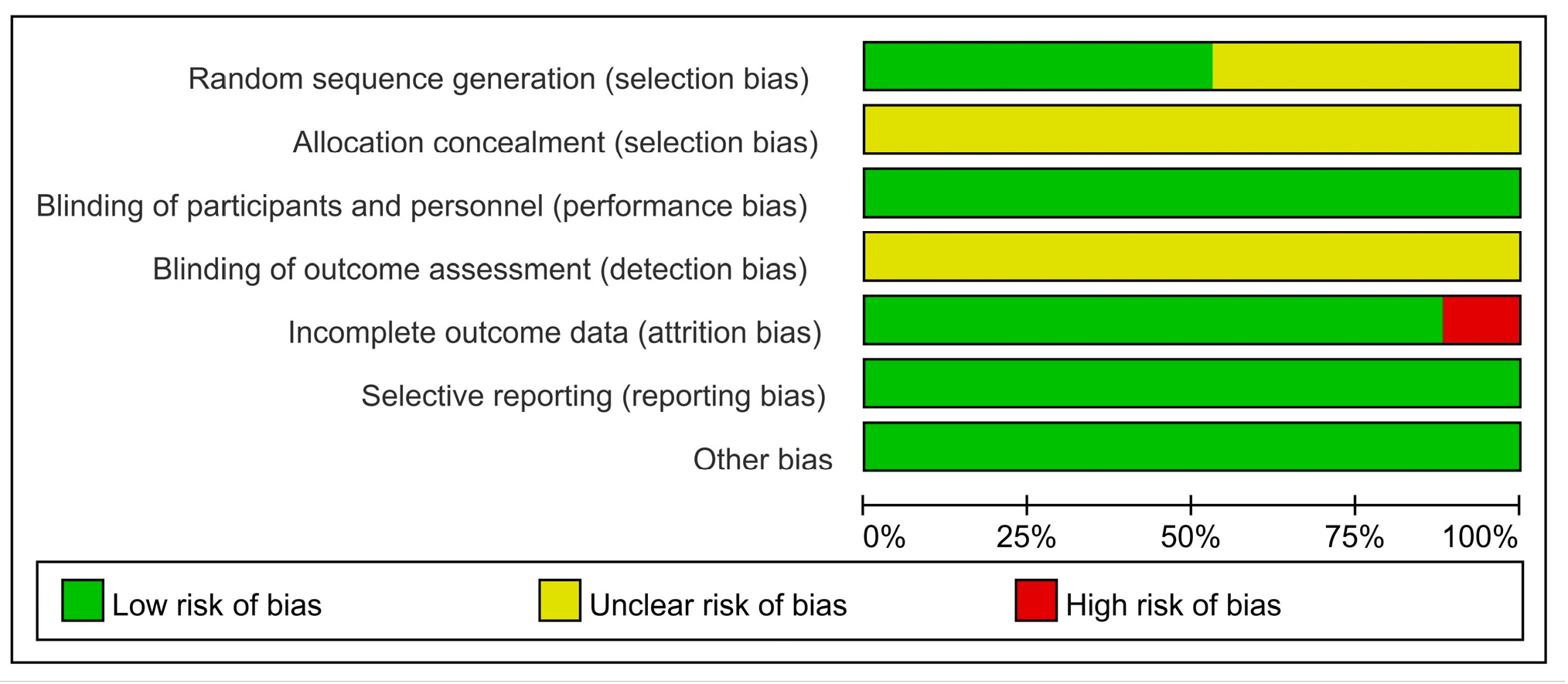
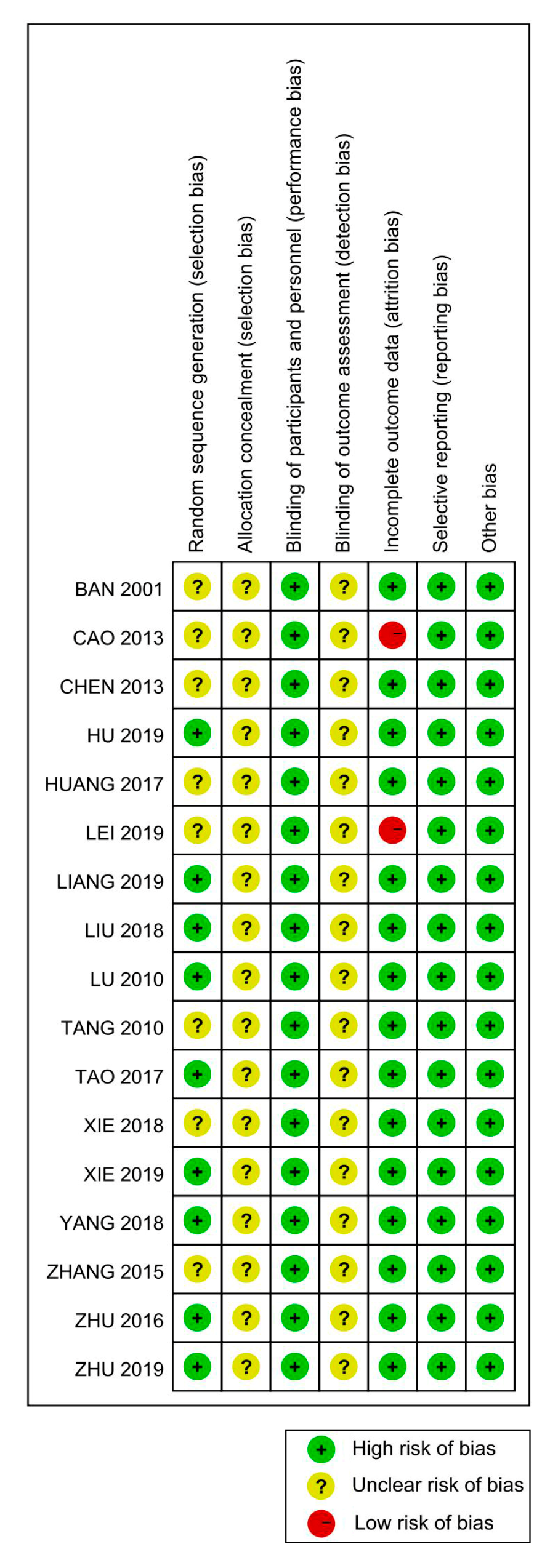
3.3. Methodological Quality
3.4. Meta-Analysis Results
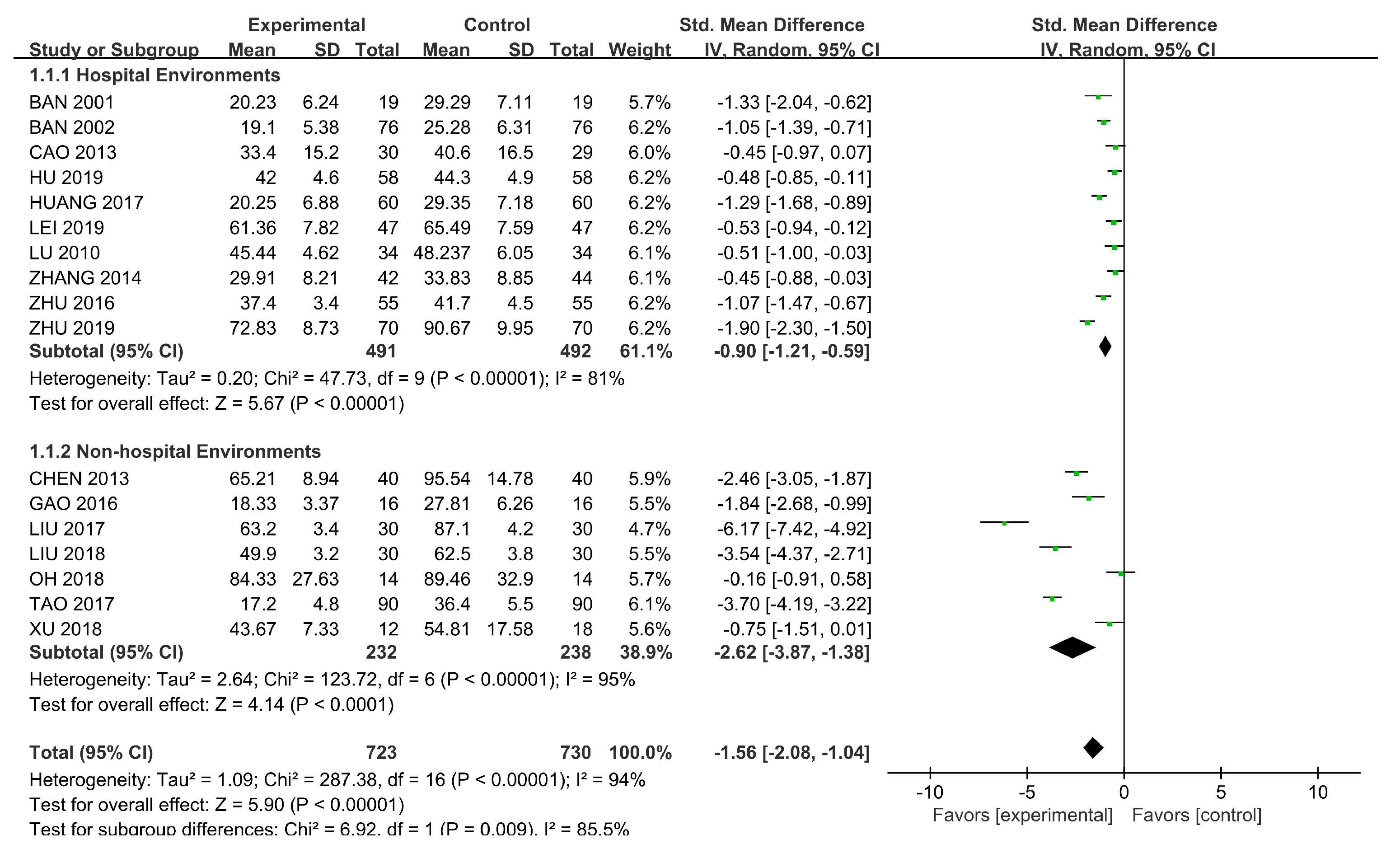
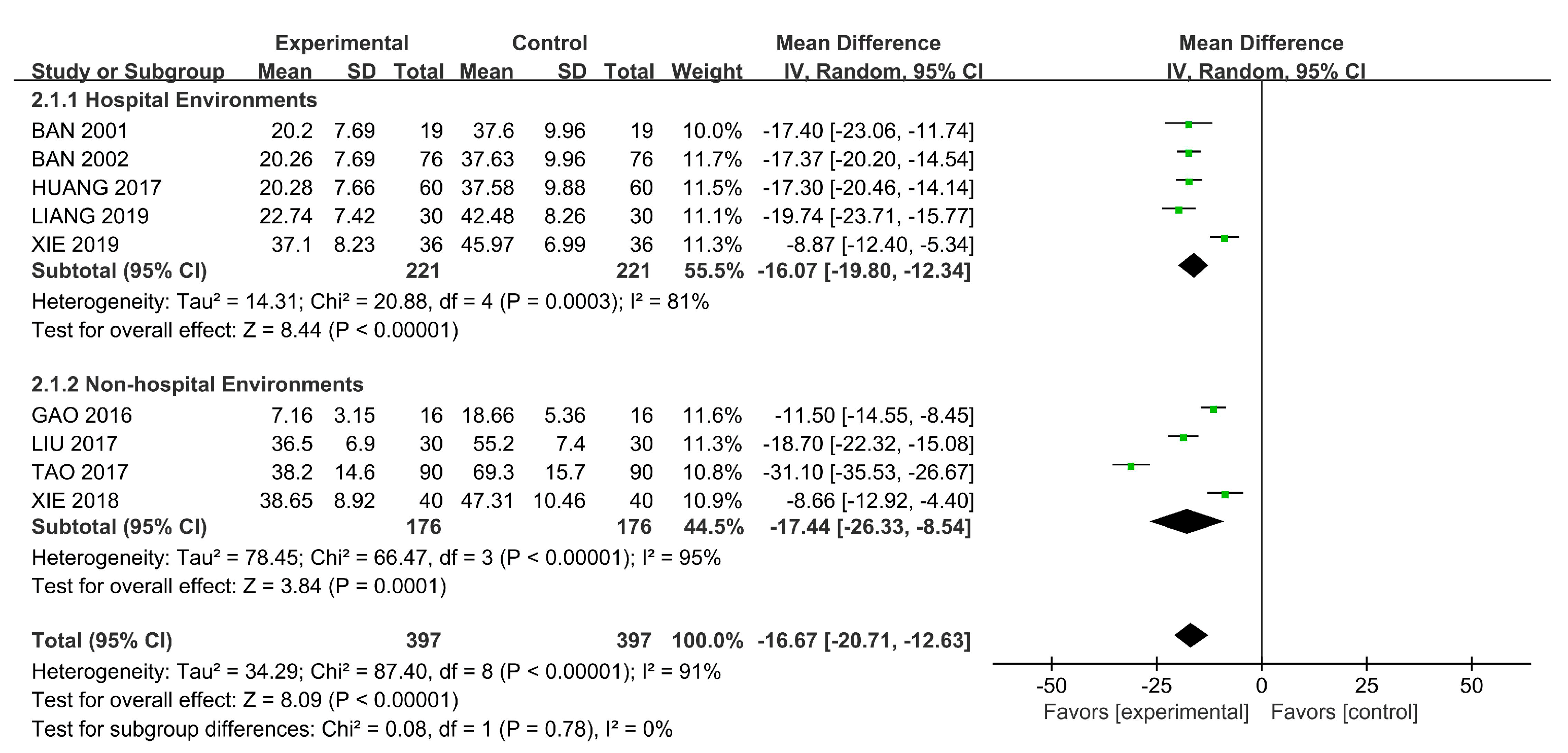
3.4.1. Symptoms
3.4.2. Rehabilitation Outcomes
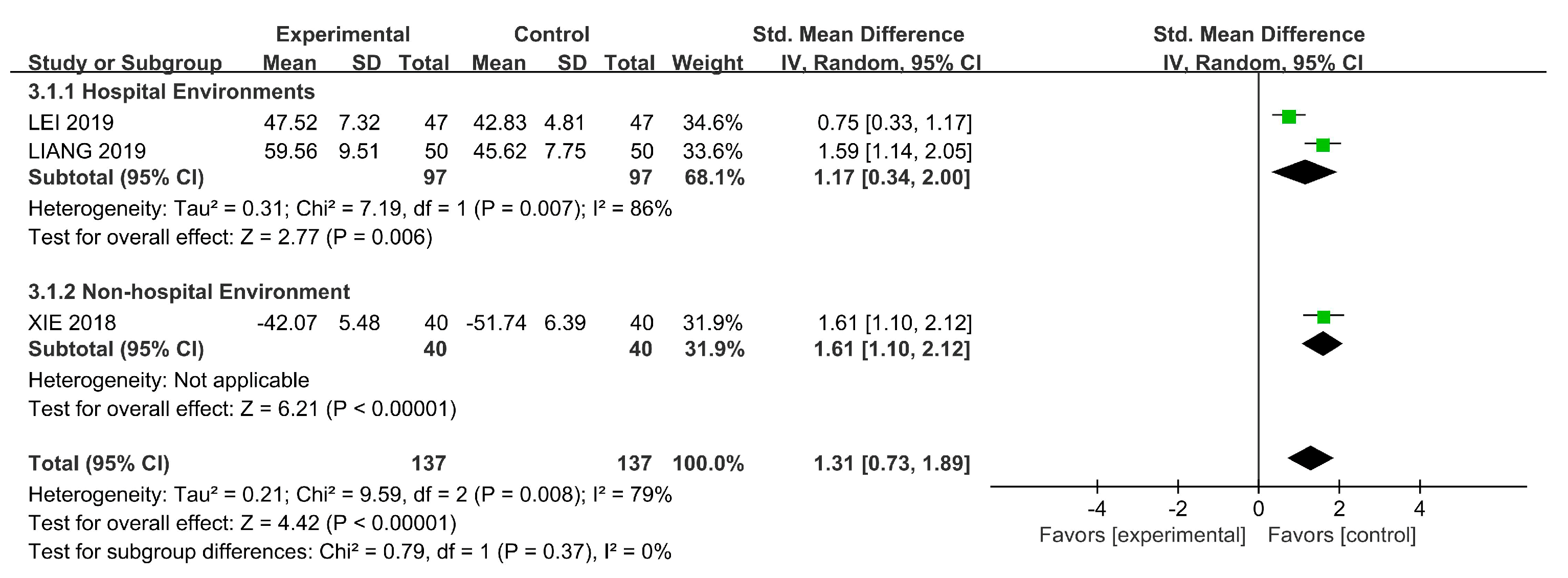
3.4.3. Quality of Life
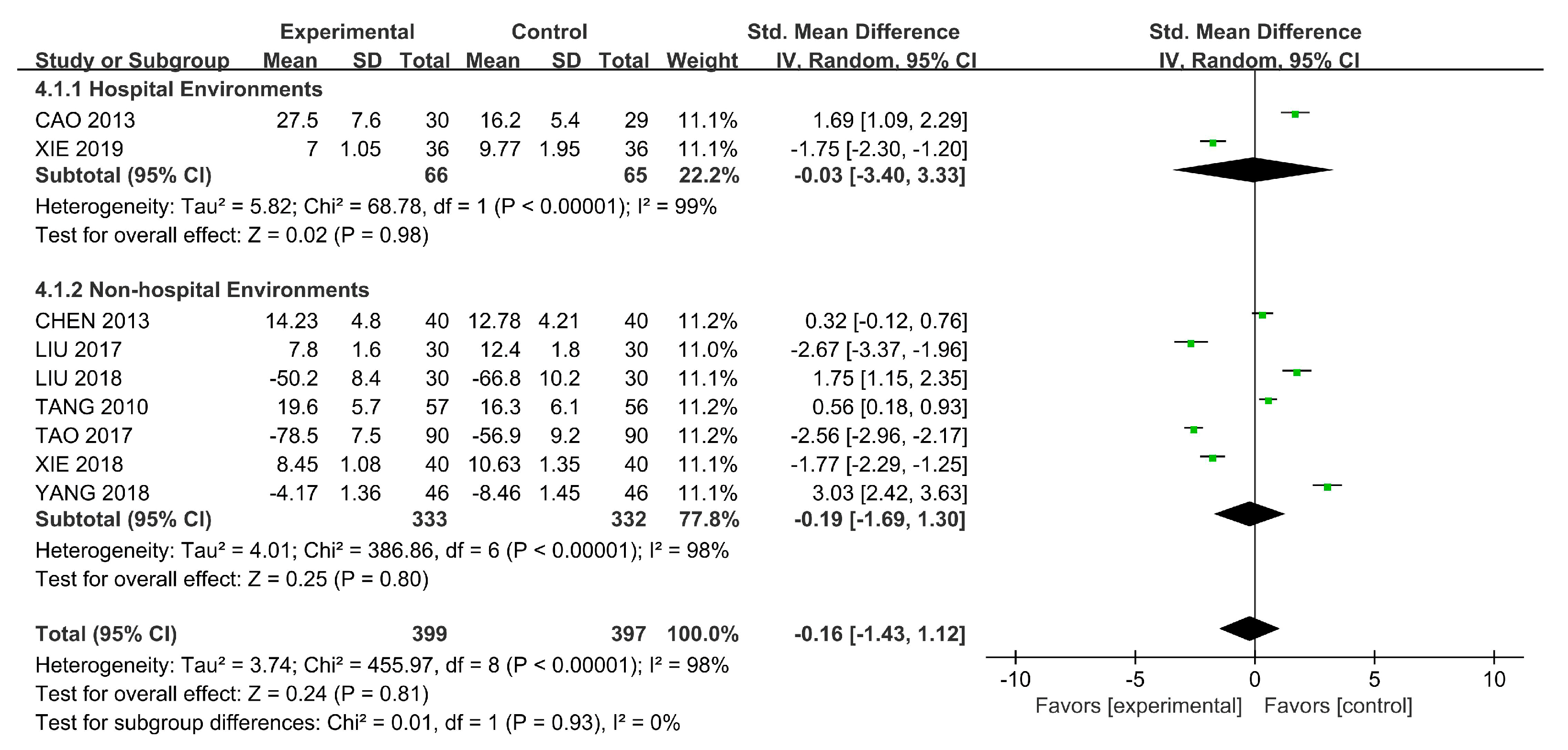
3.4.4. Social Functioning
4. Discussion
4.1. Outcomes and Processes of Horticultural Therapy
4.2. Contributions and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years Lived with Disability (YLDs) for 1160 Sequelae of 289 Diseases and Injuries 1990–2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Roberts, N.L.S.; Mountjoy-Venning, W.C.; Anjomshoa, M.; Banoub, J.A.M.; Yasin, Y.J. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study. Lancet 2019, 393, 44. [Google Scholar]
- Laursen, T.M.; Nordentoft, M.; Mortensen, P.B. Excess Early Mortality in Schizophrenia. In Annual Review of Clinical Psychology; Cannon, T.D., Widiger, T., Eds.; Annual Reviews: Palo Alto, CA, USA, 2014; Volume 10, pp. 425–448. ISBN 978-0-8243-3910-4. [Google Scholar]
- Xi, L.-Y.; Huang, X.-Q.; Zhu, F.-Y. Comparison of Psychiatric Symptoms of Schizophrenia Patients at Different Levels of Mental Disability. Chin. Gen. Pract. 2015, 18, 1208–1211. [Google Scholar] [CrossRef]
- Tsolaki, M.; Kounti, F.; Agogiatou, C.; Poptsi, E.; Bakoglidou, E.; Zafeiropoulou, M.; Soumbourou, A.; Nikolaidou, E.; Batsila, G.; Siambani, A.; et al. Effectiveness of Nonpharmacological Approaches in Patients with Mild Cognitive Impairment. Neurodegener. Dis. 2011, 8, 138–145. [Google Scholar] [CrossRef]
- Clatworthy, J.; Hinds, J.; Camic, P.M. Gardening as a Mental Health Intervention: A Review. Ment. Health Rev. J. 2014, 18, 214–225. [Google Scholar] [CrossRef]
- Aldridge, J.; Sempik, J. Social and Therapeutic Horticulture: Evidence and Messages from Research; Loughborough University: Loughborough, UK, 2002. [Google Scholar]
- Gaszner, P. Complex Therapy of Schizophrenia. Neuropsychopharmacol. Hung. Magy. Pszichofarmakol. Egyes. Lapja Off. J. Hung. Assoc. Psychopharmacol. 2009, 11, 41–45. [Google Scholar]
- Wichrowski, M.; Whiteson, J.; Haas, F.; Mola, A.; Rey, M.J. Effects of Horticultural Therapy on Mood and Heart Rate in Patients Participating in an Inpatient Cardiopulmonary Rehabilitation Program. J. Cardpulm. Rehabil. Prev. 2005, 25, 270–274. [Google Scholar] [CrossRef]
- Oh, Y.-A.; Park, S.-A.; Ahn, B.-E. Assessment of the Psychopathological Effects of a Horticultural Therapy Program in Patients with Schizophrenia. Complement. Ther. Med. 2018, 36, 54–58. [Google Scholar] [CrossRef]
- Zhu, S.-H.; Wan, H.-J.; Lu, Z.-D.; Wu, H.-P.; Zhang, Q.; Qian, X.-Q.; Ye, C.-Y. Treatment Effect of Antipsychotics in Combination with Horticultural Therapy on the Inpatients with Schizophrenia: A Randomized, Case-Controlled Study. Shanghai Arch. Psychiatry 2016, 28, 195–203. [Google Scholar] [CrossRef]
- Ban, Y.-R. Therapeutic Effects of Gardening Assisted Therapy in the Treatment of Chronic Schizophrenia. J. Nurs. Sci. 2001, 16, 518–520. [Google Scholar]
- Huang, Y.-Y. Effect of Horticultural Therapy on Long-Term Hospitalized Elderly Patients with Schizophrenia. Nurs. Pract. Res. 2017, 14, 150–151. [Google Scholar] [CrossRef]
- Gao, Y.; Huang, S.; Lu, Y.-Q. Effect of Horticultural Therapy on Rehabilitation of Chronic Schizophrenia. China Med. Pharm. 2016, 6, 202–205. [Google Scholar]
- Lei, Z.-J.; Li, H.-F.; Zhou, L. Effect of Agricultural Therapy on Rehabilitation of Patients with Chronic Schizophrenia. Health Vocat. Educ. 2019, 37, 144–145. [Google Scholar]
- Eum, E.-Y.; Sook, K.H. Effects of a Horticultural Therapy Program on Self-efficacy, Stress Response, and Psychiatric Symptoms in Patients with Schizophrenia. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2016, 25, 48–57. [Google Scholar] [CrossRef][Green Version]
- Kam, M.C.Y.; Siu, A.M.H. Evaluation of a Horticultural Activity Programme for Persons with Psychiatric Illness. Hong Kong J. Occup. Ther. 2010, 20, 80–86. [Google Scholar] [CrossRef]
- Hyun, M.Y. The Effects of Cognitive Behavioral Group Therapy Improving Social Cognition on the Self efficacy, Relationship Function and Social Skills for Chronic Schizophrenia. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2017, 26, 186. [Google Scholar] [CrossRef]
- Son, K.C.; Jung, H.J.; Bae, H.J.; Song, J.E. Comparison of the Effectiveness of Different Horticultural Therapy Programs for Individuals with Chronic Schizophrenia. Korean J. Hortic. Sci. Technol. 2004, 22, 135–142. [Google Scholar]
- Glass, G.V. 9: Integrating Findings: The Meta-Analysis of Research. Rev. Res. Educ. 1977, 5, 351–379. [Google Scholar] [CrossRef]
- Tu, H.-M.; Chiu, P.-Y. Meta-Analysis of Controlled Trials Testing Horticultural Therapy for the Improvement of Cognitive Function. Sci. Rep. 2020, 10, 14637. [Google Scholar] [CrossRef]
- Liu, Y.; Li, B.; Sampson, S.J.; Roberts, S.; Zhang, G.; Wu, W. Horticultural Therapy for Schizophrenia. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Zhao, Y.; Liu, Y.; Wang, Z. Effectiveness of Horticultural Therapy in People with Dementia: A Quantitative Systematic Review. J. Clin. Nurs. 2020. [Google Scholar] [CrossRef] [PubMed]
- Spano, G.; D’Este, M.; Giannico, V.; Carrus, G.; Elia, M.; Lafortezza, R.; Panno, A.; Sanesi, G. Are Community Gardening and Horticultural Interventions Beneficial for Psychosocial Well-Being? A Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 3584. [Google Scholar] [CrossRef] [PubMed]
- Jang, E.J.; Han, G.W.; Hong, J.W.; Yoon, S.E.; Pak, C.H. Meta-Analysis of Research Papers on Horticultural Therapy Program Effect. Korean J. Hortic. Sci. Technol. 2010, 28, 701–707. [Google Scholar]
- Soga, M.; Gaston, K.J.; Yamaura, Y. Gardening Is Beneficial for Health: A Meta-Analysis. Prev. Med. Rep. 2017, 5, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, R.S. Effects of Interior Design on Wellness: Theory and Recent Scientific Research. J. Health Care Inter. Des. 1991, 3, 97. [Google Scholar] [PubMed]
- Verderber, S.; Grice, S.; Gutentag, P. Wellness Health Care and the Architectural Environment. J. Community Health 1987, 12, 163–175. [Google Scholar] [CrossRef]
- Williams, M.A. The Physical Environment and Patient Care. Annu. Rev. Nurs. Res. 1988, 6. [Google Scholar] [CrossRef]
- Graven, S.N. Clinical Research Data Illuminating the Relationship between the Physical Environment & Patient Medical Outcomes. J. Healthc. Des. Proc. Symp. Healthc. Des. Symp. Healthc. Des. 1997, 9, 15. [Google Scholar]
- Perovic, Z.; Perovic, S. Influence of Hospital Room Environment on the Reduction of Anxiety and Depression in the Early Stage of Stroke. J. Environ. Prot. Ecol. 2017, 18, 710–719. [Google Scholar]
- Devlin, A.S.; Andrade, C.C. Quality of the Hospital Experience: Impact of the Physical Environment. In Handbook of Environmental Psychology and Quality of Life Research; FleuryBahi, G., Pol, E., Navarro, O., Eds.; Springer: Cham, Switzerland, 2017; pp. 421–440. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 1000097. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, 5928. [Google Scholar] [CrossRef] [PubMed]
- Critical-Appraisal-Tools—Critical Appraisal Tools. Joanna Briggs Institute. Available online: https://jbi.global/critical-appraisal-tools (accessed on 15 January 2021).
- Tang, J.-W.; He, D.-D.; Liu, J.-M.; Yang, Y.-Y.; Su, J.-G. Park Farm Rehabilitation on the Social Function of Patients with Chronic Schizophrenia. J. Clin. Psychiatry 2010, 20, 164–165. [Google Scholar]
- Ban, Y.-R. Effect of Horticultural Therapy on Rehabilitation of Patients with Chronic Schizophrenia. J. Pract. Nurs. 2002, 18, 50–51. [Google Scholar]
- Cao, M.-Y.; Wu, H. Effects of Agronomic Therapy on Social Function of Inpatients with Chronic Schizophrenia. Med. Inf. 2013, 26, 321–322. [Google Scholar]
- Chen, D.-R.; Jia, X.-S. Effect Of Farming Therapy For Rehabilitation Of Chronic Schizophrenic Patients. J. Nongken Med. 2013, 35, 199–201. [Google Scholar]
- Tao, F.; Sun, X.-F. Observation on the Efficacy of Agronomic Treatment in the Rehabilitation of Inpatients with Chronic Schizophrenia. China Gen. Pract. 2017, 20, 320–321. [Google Scholar]
- Hu, X.-L.; Liang, Z.; Zhang, Y.-H. Improvement of Happiness and Deficiency in Inpatients with Schizophrenia by Horticultural Therapy. Chin. J. Ment. Health 2019, 33, 498–503. [Google Scholar]
- Zhu, Y.; Zhang, S.-F. Effects of Teamwork Intervention on Social Function of Chronic Schizophrenia Patients during Rehabilitation Period. Contemp. Nurses 2019, 26, 119–121. [Google Scholar]
- Liu, S.-Z.; Liao, G.-J.; Huang, Z.-J.; Li, J.; Gao, L. Effect of Agricultural Therapy on Rehabilitation of Inpatients with Chronic Schizophrenia. Chin. Med. Innov. 2018, 15, 61–64. [Google Scholar] [CrossRef]
- Yang, C.-T.; Zhou, Z.-G.; Huang, Y.-Q.; He, Y.-X. Effect of Drug Therapy Combined with Agricultural Treatment on Social Function in Patients with Chronic Schizophrenia. Pract. Clin. Med. 2018, 19, 23–25. [Google Scholar]
- Xie, Z.-H. Effect of Systematic Agricultural Therapy on Social Function and Quality of Life of Inpatients with Chronic Schizophrenia during Rehabilitation Period. Jilin Med. 2018, 39, 733–734. [Google Scholar]
- Xu, Y.; Cai, J.; Zhou, Y.; Li, J.; Chen, W.-J.; Wu, L.; Xie, D.-H. Analysis of the Effect of Agricultural Training on Rehabilitation of Schizophrenic Patients in Community. Chin. Nurs. Res. 2018, 32, 1142–1143. [Google Scholar]
- Liu, S.-Z.; Gan, G.-R.; Liao, B.; Li, Y.; Wu, D. A Study of the Effect of Therapy on the Recovery of Hospitalized Patients with Chronic Schizophrenia. Contemp. Med. 2017, 23, 131–133. [Google Scholar] [CrossRef]
- Zhang, S.-Q.; Cui, W.-D.; Zhao, X.-F. The Social Function of Effect of Agricultural Rehabilitation Treatment in Team on Chronic Male Schizophrenics. China J. Health Psychol. 2015, 23, 967–970. [Google Scholar]
- Zhang, S.-Q.; Cui, W.-D.; Wang, L.; Zhao, X.-F. The Significance of Agricultural Rehabilitation Training in the Rehabilitation of Patients with Chronic Schizophrenia. J. Pract. Clin. Med. 2014, 18, 128–129. [Google Scholar] [CrossRef]
- Lu, A.-J. Rehabilitative Effects of Farming Cure on Hospitalized Patients with Chronic Schizophrenia. Shanghai Arch. Psychiatry 2010, 22, 236–238. [Google Scholar]
- Liang, Z.-X.; Qin, Y.-L.; Gao, Y.; Lu, Y.-Q.; Huang, S.-Y. Influence of Horticultural Therapy on Rehabilitation and Quality of Life of Schizophrenic Inpatients. Chin. Contemp. Med. 2019, 26, 58–60, 64. [Google Scholar]
- Xie, H.; Cao, X. Effects of Agricultural Therapy on Social Functioning in Long-Term Hospitalized Patients with Chronic Schizophrenia. World Latest Med. Inf. 2019, 19, 54–55. [Google Scholar] [CrossRef]
- Son, K.C.; Um, S.J.; Kim, S.Y.; Song, J.E.; Kwack, H.R. Effect of Horticultural Therapy on the Changes of Self-Esteem and Sociality of Individuals with Chronic Schizophrenia. Acta Hortic. 2004, 639, 185–191. [Google Scholar] [CrossRef]
- Lysaker, P.H.; Salyers, M.P. Anxiety Symptoms in Schizophrenia Spectrum Disorders: Associations with Social Function, Positive and Negative Symptoms, Hope and Trauma History. Acta Psychiatr. Scand. 2007, 116, 290–298. [Google Scholar] [CrossRef]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with Nature Improves Cognition and Affect for Individuals with Depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and Mental Health: An Ecosystem Service Perspective. Sci. Adv. 2019, 5, 0903. [Google Scholar] [CrossRef] [PubMed]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature Contact and Human Health: A Research Agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at Least 120 Minutes a Week in Nature Is Associated with Good Health and Wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef]
- Van den Berg, M.; Van Poppel, M.; Van Kamp, I.; Andrusaityte, S.; Balseviciene, B.; Cirach, M.; Danileviciute, A.; Ellis, N.; Hurst, G.; Masterson, D.; et al. Visiting Green Space Is Associated with Mental Health and Vitality: A Cross-Sectional Study in Four European Cities. Health Place 2016, 38, 8–15. [Google Scholar] [CrossRef]
- Kaplan, S. The Restorative Benefits of Nature—Toward an Integrative Framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S. Visual Landscapes and Psychological Well-being. Landsc. Res. 1979, 4, 17–23. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.-J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative Effects of Viewing Real Forest Landscapes, Based on a Comparison with Urban Landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Ottosson, J.; Grahn, P. The Role of Natural Settings in Crisis Rehabilitation: How Does the Level of Crisis Influence the Response to Experiences of Nature with Regard to Measures of Rehabilitation? Landsc. Res. 2008, 33, 51–70. [Google Scholar] [CrossRef]
- Han, K.-T. An Exploration of Relationships Among the Responses to Natural Scenes Scenic Beauty, Preference, and Restoration. Environ. Behav. 2010, 42, 243–270. [Google Scholar] [CrossRef]
- Henson, P.; Pearson, J.F.; Keshavan, M.; Torous, J. Impact of Dynamic Greenspace Exposure on Symptomatology in Individuals with Schizophrenia. PLoS ONE 2020, 15, 0238498. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategy | Details |
|---|---|
| Inclusion criteria | P: People with schizophrenia |
| I: Horticultural therapy | |
| C: Medication and conventional workshop training | |
| O: Symptoms, rehabilitation outcomes, quality of life, and social functioning | |
| S: Randomized controlled trials (RCTs) and quasi-experimental studies | |
| Exclusion criteria | S: Non-original papers (opinion papers, review articles, commentaries, letters, protocols, and reports without quantitative data) |
| Language filter | English or Chinese |
| Time filter | From January 2000 to December 2020 |
| Database | PubMed, Cochrane Library, Embase, Science Direct, and China National Knowledge Infrastructure |
| Author (Publication Year) | Country | Settings | Diagnostic Criteria | Subject | Intervention | Measurement and Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants E/C | Age E/C | Male (%) | Performer of Intervention | Intervention Duration | Intervention-E | Intervention-C | Follow-Up (Months) | |||||
| Ban (2001) [12] | China | Hospital | CCMD-2-R | 19/19 | 25–51 | 63.16 | Gardeners and nurses | 60 min per time/five times per week/12 weeks | Horticultural therapy: Planting flowers and making bonsai | Usual schizophrenia care: Medication and conventional work and entertainment treatment | 3 | BPRS and IPROS |
| Huang (2017) [13] | China | Hospital | Not mentioned | 60/60 | 60–81 | 53.33 | Gardeners and nurses | Not mentioned | Horticultural therapy: planting flowers | Usual schizophrenia care: medication and conventional work and entertainment treatment | 3 | BPRS and IPROS |
| Gao et al. (2016) [14] | China | The agricultural rehabilitation training institution | ICD-10 | 16/16 | 55.6 ± 2.3/56.3 ± 2.3 | 40.63 | Horticultural therapists | 60 min per time/four times/eight weeks | Horticultural therapy: Seed planting, plant appreciation, cutting propagation, flower pot planting, and taste grown vegetables | Usual schizophrenia care: Rehabilitation training, sanitation, self-care training and medication training | 2 | BPRS and IPROS |
| Tang et al. (2010) [36] | China | The agricultural rehabilitation training institution | ICD-10 | 57/56 36/36 | 29–64 | 65.41 | Therapeutic specialists | 120–180 min per time/five times per week/40 weeks | Horticultural therapy: Planting vegetables, flowers, and fruits | Usual schizophrenia care: Watching TV, listening to music, singing, reading books, playing chess, playing cards, playing table tennis, and cleaning the room | 10 | SSPI |
| Ban (2002) [37] | China | Hospital | CCMD-2-R | 76/76 | 40.0 ± 7.96/38.13 ± 9.24 | 63.16 | Gardeners and occupational staff | >300 min a week/12 weeks | Horticultural therapy: Planting flowers and making bonsai | Usual schizophrenia care: Medication | 3 | BPRS and IPROS |
| Cao and Wu (2013) [38] | China | Hospital | ICD-10 | 30/30 | 42.4 ± 9.3/43.7 ± 9.0 | 72.88 | Three agronomy therapists | 90 min per time/once per week/24 weeks | Horticultural therapy: Planting corn | Usual schizophrenia care: Medication | 6 | PANSS and SSPI |
| Chen and Jia (2013) [39] | China | The agricultural rehabilitation training institution | ICD-10 | 40/40 | 43.26 ± 10.26/45.21 ± 9.87 | 67.50 | Agricultural specialists | 8–12 h per week/96 weeks | Horticultural therapy | Usual schizophrenia care: Watching TV, listening to music, singing, reading books, playing chess, playing cards, playing table tennis, and cleaning the room | 24 | PANSS and SSPI |
| Tao and Sun (2017) [40] | China | The agricultural rehabilitation training institution | ICD-10 | 90/90 | 41.5 ± 6.8/40.4 ± 7.5 | Not mentioned | Agricultural specialists, doctors, and nurses | 60–120 min per time/5–8 times per week/24 weeks | Horticultural therapy: Planting vegetables and fruits | Usual schizophrenia care: Medication and conventional work and entertainment treatment | 6 | SANS, IPROS, and PSP |
| Oh et al. (2018) [10] | Korea | Farm | ICD-10 | 14/14 | 42.1 ± 13.0/33.4 ± 9.4 | 71.43 | Two horticultural therapists and one volunteer | 120 min per week/10 weeks | Horticultural therapy: Plant cultivating activities | Usual schizophrenia care: Medication, leisure activities, and exercise program | 2.5 | PANSS and BPRS |
| Zhu et al. (2016) [11] | China | Hospital | ICD-10 | 55/55 | 48.2 | 43.64 | Two rehabilitative therapists | 90 min per time/three times per week/12 weeks | Horticultural therapy: Seeding, watering, fertilizing, weeding, and catching pests | Usual schizophrenia care: Medication | 3 | PANSS |
| Hu et al. (2019) [41] | China | Hospital | ICD-10 | 58/58 | 45 ± 8/48 ± 7 | 64.66 | Horticultural specialists, doctors, and nurses | 60 min per session/twice a week/12 weeks | Horticultural therapy: Planting and making garden micro-landscape | Usual schizophrenia care | 3 | PANSS |
| Zhu and Zhang (2019) [42] | China | Hospital | ICD-10 | 70/70 | 46.97 ± 11.48/46.96 ± 9.54 | Not mentioned | Therapeutic specialists, doctors, nurses, and agricultural specialists | 60–90 min per time/5–7 h a week/24 weeks | Horticultural therapy: Planting vegetables and raising animals | Usual schizophrenia care | 6 | PANSS |
| Lei et al. (2019) [15] | China | Hospital | ICD-10 | 47/47 | 36.04 ± 9.52/35.45 ± 7.91 | 55.32 | Agricultural specialists and nurses | 60 min per time/once every two days/48 weeks | Horticultural therapy: Turning the ground, sowing, watering, and fertilizing, removing insects, weeding, picking vegetables | Usual schizophrenia care: Medication and conventional work and entertainment treatment, such as music therapy and physical training, group games | 12 | SANS and GQOLI-74 |
| Liu (2018) [43] | China | The agricultural rehabilitation training institution | ICD-10 | 30/30 | 41.4 ± 11.6/40.9 ± 11.3 | 75.00 | Staff | More than 60 min per time/5–8 h per week/24 weeks | Horticultural therapy | Usual schizophrenia care: Medication | 6 | PANSS and PSP |
| Yang et al. [44] | China | The agricultural rehabilitation training institution | DSM-IV-TR | 46/46 | 37.72 ± 6.16/38.44 ± 6.76 | Not mentioned | Agricultural specialists and staff | 60 min per time/seven times per week/24 weeks | Horticultural therapy: Watering, weeding, sowing vegetables, and fertilizing | Usual schizophrenia care: Medication | 6 | SDSS |
| Xie (2018) [45] | China | The agricultural rehabilitation training institution | ICD-10 | 40/40 | 44.89 ± 4.96/45.03 ± 4.82 | 56.25 | Therapeutic specialists | 120 min per time/24 weeks | Horticultural therapy: Planting, pulling weeds, hoeing, watering, and picking fruits | Usual schizophrenia care: Medication and rehabilitation knowledge training, life and social skills training, psychotherapy | 6 | SSPI, SQLS, and IPROS |
| Xu et al. (2018) [46] | China | Community | ICD-10 | 12/16 | 44.33 ± 9.71/44.19 ± 8.12 | Not mentioned | Psychiatrists, nurses, psychological counselors, public health physicians, rehabilitation specialists, social workers, disabled workers with agricultural skills, and family members | More than 60 min per time/twice per week/24 weeks | Horticultural therapy: Turning the ground, sowing, and maintaining and picking vegetables and fruits | Usual schizophrenia care: Medication and conventional work and entertainment treatment | 6 | PANSS |
| Liu et al. (2017) [47] | China | The agricultural rehabilitation training institution | ICD-10 | 30/30 | 46.4 ± 8.5/46.5 ± 8.2 | 65.00 | Agricultural specialists | More than 60 min per time/5–8 h per week/48 weeks | Horticultural therapy: Fertilizing, sowing, watering, weeding, planting, and harvesting | Usual schizophrenia care: Medication | 12 | PANSS, IPROS, and SSPI |
| Zhang et al. (2015) [48] | China | Hospital | DSM-IV | 45/38 | 42.25 ± 9.25/43.26 ± 8.91 | 100.00 | Therapeutic specialists and agricultural specialists | 120 min per time/once every two days/24 weeks | Horticultural therapy: Planting, weeding, and fertilizing | Usual schizophrenia care | 6 | PSP |
| Zhang et al. (2014) [49] | China | Hospital | ICD-10 | 42/44 | 35.42 ± 7.21/38.20 ± 5.41 | 100.00 | Nurses | One hour per day/48 weeks | Horticultural therapy: Breeding, planting vegetables, studying forest and fruit technology, and cultivating flowers | Usual schizophrenia care: Medication | 12 | PANSS |
| Lu and Wang (2010) [50] | China | Hospital | ICD-10 | 34/34 | 42 ± 12/40 ± 11 | 61.76 | Agricultural specialists | 60 min per time/once every two weeks/48 weeks | Horticultural therapy: Planting, weeding, and fertilizing | Usual schizophrenia care: Medication and conventional work and entertainment treatment | 12 | PANSS |
| Liang et al. (2019) [51] | China | Hospital | ICD-10 | 30/30 | 36.78 ± 8.50/36.73 ± 8.34 | 66.67 | Horticultural therapists | 120 min per time/five times per week/12 weeks | Horticultural therapy: Planting | Usual schizophrenia care: medication | 3 | IPROS and GQOLI-74 |
| Xie and Cao (2019) [52] | China | Hospital | Not mentioned | 36/36 | 45.43 ± 5.14/45.12 ± 5.23 | 56.94 | Agricultural specialists and nurses | Not mentioned | Horticultural therapy: | Usual schizophrenia care: Medication and social function exercise, and psychotherapy | 6 | SSPI and IPROS |
| Included Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Ban (2002) [37] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gao (2016) [14] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Liu et al. (2017) [47] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Oh et al. (2018) [10] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Xu et al. (2018) [46] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Zhang et al. (2014) [48] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, S.; Zhao, Y.; Liu, J.; Xu, F.; Wang, Z. Effectiveness of Horticultural Therapy in People with Schizophrenia: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 964. https://doi.org/10.3390/ijerph18030964
Lu S, Zhao Y, Liu J, Xu F, Wang Z. Effectiveness of Horticultural Therapy in People with Schizophrenia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(3):964. https://doi.org/10.3390/ijerph18030964
Chicago/Turabian StyleLu, Shan, Yajie Zhao, Jianjiao Liu, Feng Xu, and Zhiwen Wang. 2021. "Effectiveness of Horticultural Therapy in People with Schizophrenia: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 3: 964. https://doi.org/10.3390/ijerph18030964
APA StyleLu, S., Zhao, Y., Liu, J., Xu, F., & Wang, Z. (2021). Effectiveness of Horticultural Therapy in People with Schizophrenia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(3), 964. https://doi.org/10.3390/ijerph18030964