The Role of Value Stream Mapping in Healthcare Services: A Scoping Review


Abstract
1. Introduction
2. Theoretical Framework
- How much research on VSM in healthcare has been published in the period 2015–2019?
- In which health areas has the VSM methodology been applied in the published articles?
- What sustainability indicators are considered when applying the VSM methodology?
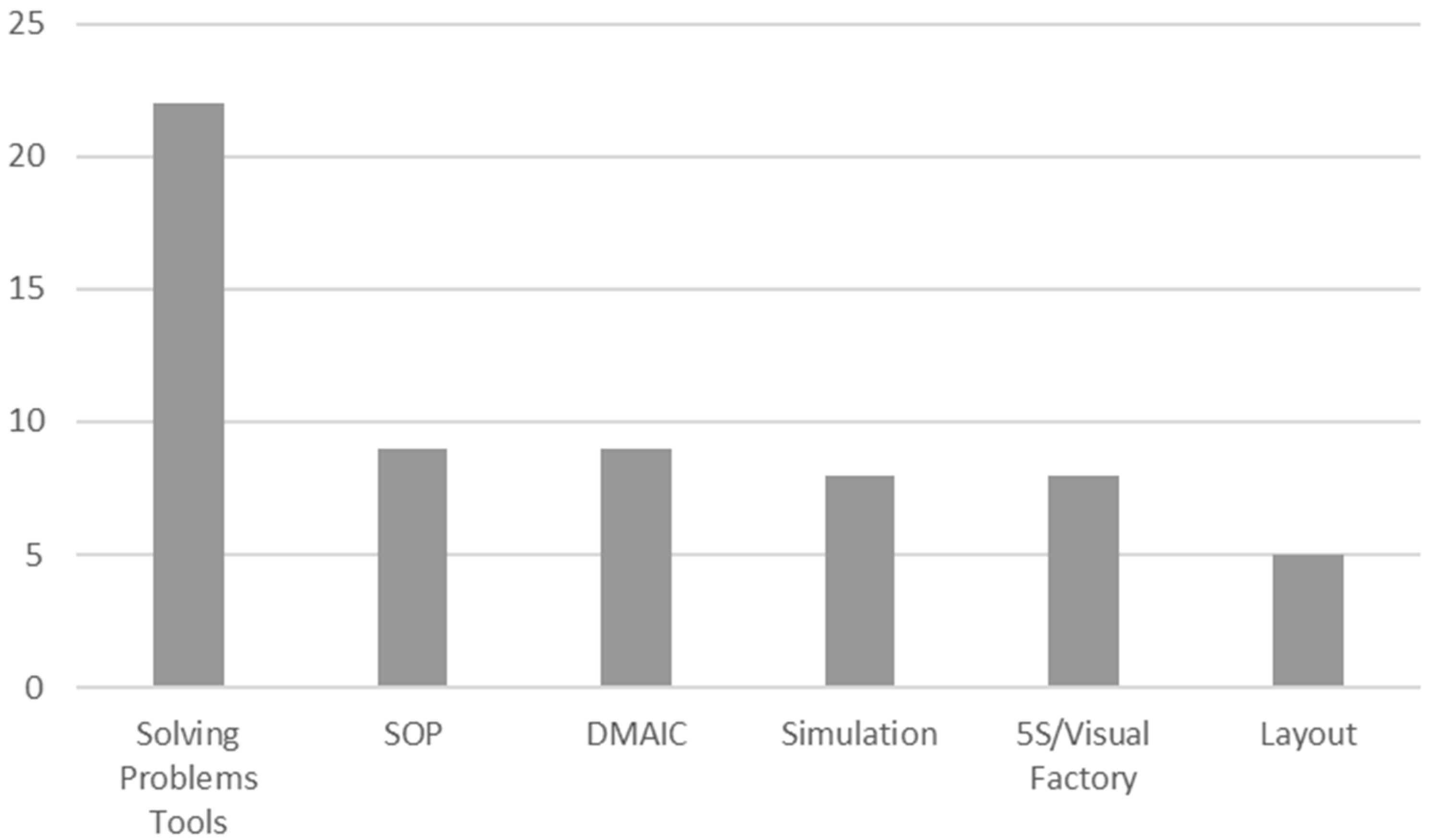
- Is VSM employed alone or along with other lean tools? If so, which ones?
- What is the common VSM version used in healthcare sector publications?
3. Materials and Methods
- ▪
- Inclusion criteria
- 1.
- Research works published between 2015 and 2019 in the journals or conferences indexed in Web of Science (WOS) databases
- 2.
- Research works that investigate applying VSM to public or private clinics or hospitals anywhere in the world.
- 3.
- Research works written in English, Spanish, French, German, Italian or Portuguese.
- ▪
- Exclusion criteria
- 4.
- Book chapters, dissertations and other sources that are not easy to access and with no guaranteed review process (e.g., consultant firms’ reports).
- 5.
- Applications in health areas that are not the object of our research, such as the pharmaceutical industry or official organizations or institutions (Red Cross, Ministry of Health, World Health Organization (WHO), Médecins Sans Frontières, etc.). For instance:
- Ha, C., Taylor, C., & Modi, J. R. (2016). Mass Vaccinations at the United States Naval Academy. HEALTH SECURITY, 14(6), 382–388. https://doi.org/10.1089/hs.2016.0030
- 6.
- The research work makes no clear contribution with VSM, but only appears indirectly as merely another lean manufacturing technique, or as a continuous improvement or processes improvement technique. For instance:
- Fung-Kee-Fung, M., Maziak, D. E., Pantarotto, J. R., Smylie, J., Taylor, L., Timlin, T., … Stewart, D. J. (2018). Regional process redesign of lung cancer care: a learning health system pilot project. CURRENT ONCOLOGY, 25(1), 59–66. https://doi.org/10.3747/co.25.3719
- Furterer, S. L. (2018). Applying Lean Six Sigma methods to reduce length of stay in a hospital’s emergency department. QUALITY ENGINEERING, 30(3), 389–404. https://doi.org/10.1080/08982112.2018.1464657
- Al Owad, A., Samaranayake, P., Karim, A., & Ahsan, K. B. (2018). An integrated lean methodology for improving patient flow in an emergency department—case study of a Saudi Arabian hospital. PRODUCTION PLANNING & CONTROL, 29(13), 1058–1081. https://doi.org/10.1080/09537287.2018.1511870
- Basta, Y. L., Zwetsloot, I. M., Klinkenbijl, J. H. G., Rohof, T., Monster, M. M. C., Fockens, P., & Tytgat, K. M. A. J. (2016). Decreasing the dispatch time of medical reports sent from hospital to primary care with Lean Six Sigma. JOURNAL OF EVALUATION IN CLINICAL PRACTICE, 22(5), 690–698. https://doi.org/10.1111/jep.12518
- 7.
- Articles containing only one page or two, with barely any information to be subsequently analyzed. For instance:
- Rodrigues, D. M., Sadeghi, M., Bernstein, M., & Yong, E. (2017). Utilization of quality improvement strategies in the inpatient endoscopy setting at a tertiary care educational hospital. GASTROENTEROLOGY, 152(5, 1), S221–S222. https://doi.org/10.1016/S0016-5085(17)31037-5
- ▪
- Search strategy
- Citation: specifying the author, year and titles of the article (e.g., “Dogan, N. O., & Unutulmaz, O. (2016). Lean production in healthcare: simulation-based value stream mapping in the physical therapy and rehabilitation department of a public hospital. Total Quality Management and Business Excellence, 27(1–2), 64–80. https://doi.org/10.1080/14783363.2014.945312”).
- Objectives: A brief description of the article’s objectives.
- Research type: literature review, survey/interview (cross-sectional), longitudinal (intervention or observation).
- Population: country or geographic region of which the data sample is representative.
- Sample (for surveys or multiple cases): if they are longitudinal, the hospital’s name.
- Year: indicating the year when the data or data sources employed in the research were collected.
- Questions: identify the main ideas set out in the articles.
- Healthcare sector: primary care consultation, consultation with a specialist, hospital, geriatric, others.
- Unit: emergency services, cardiology, traumatology, etc.
- Current state VSM (Yes/No).
- Future state VSM (Yes/No).
- Suggest improvement actions.
- Other TQM or lean interventions used with VSM.
- Indicators Baseline Value (Yes/No), Post Value (Yes/No).
- Indicators: operational/social–human resources/environmental.
- Limitations that the article indicates.
4. Results
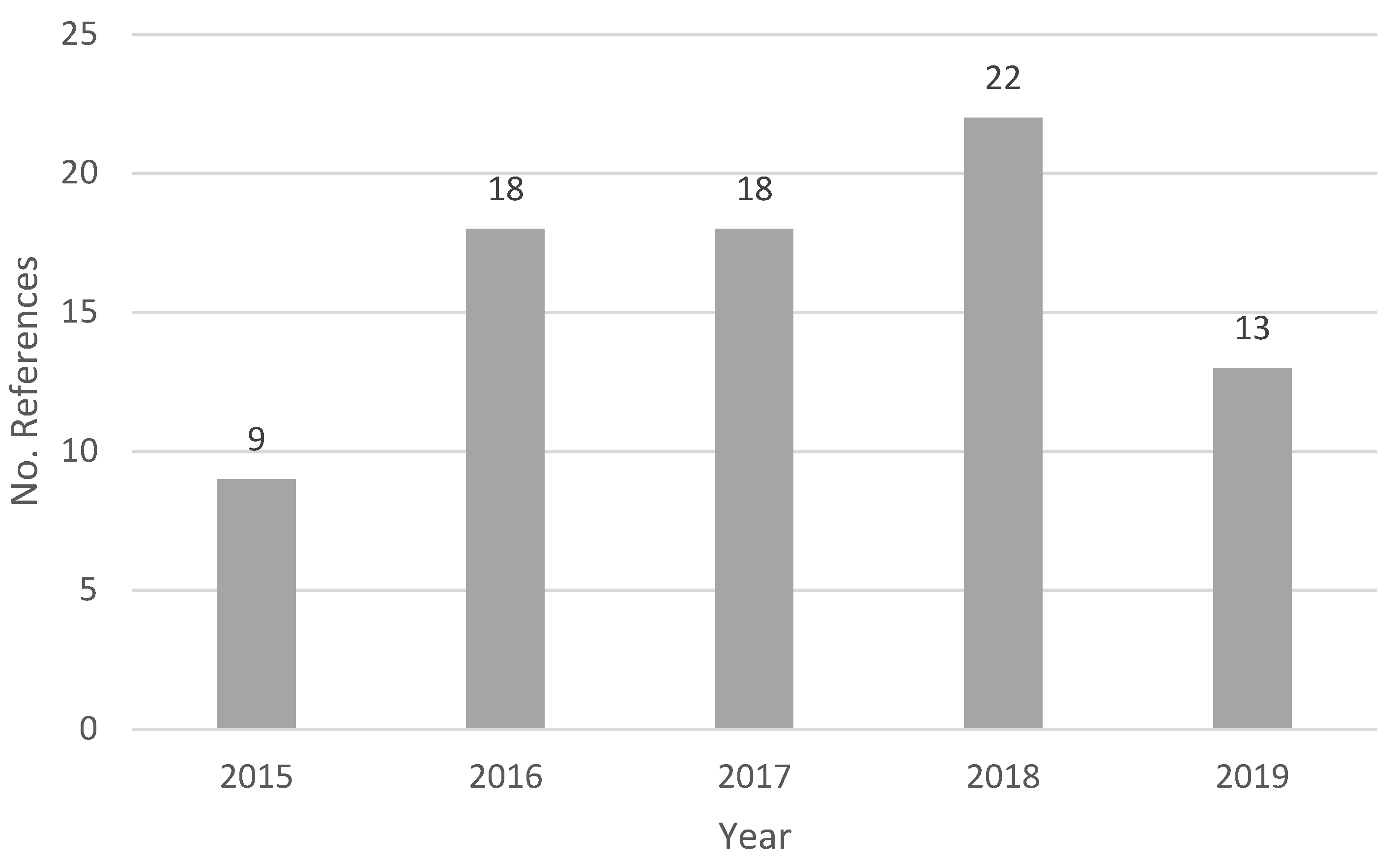
4.1. RQ1: How Much VSM Research in the Healthcare Sector Has Been Published?
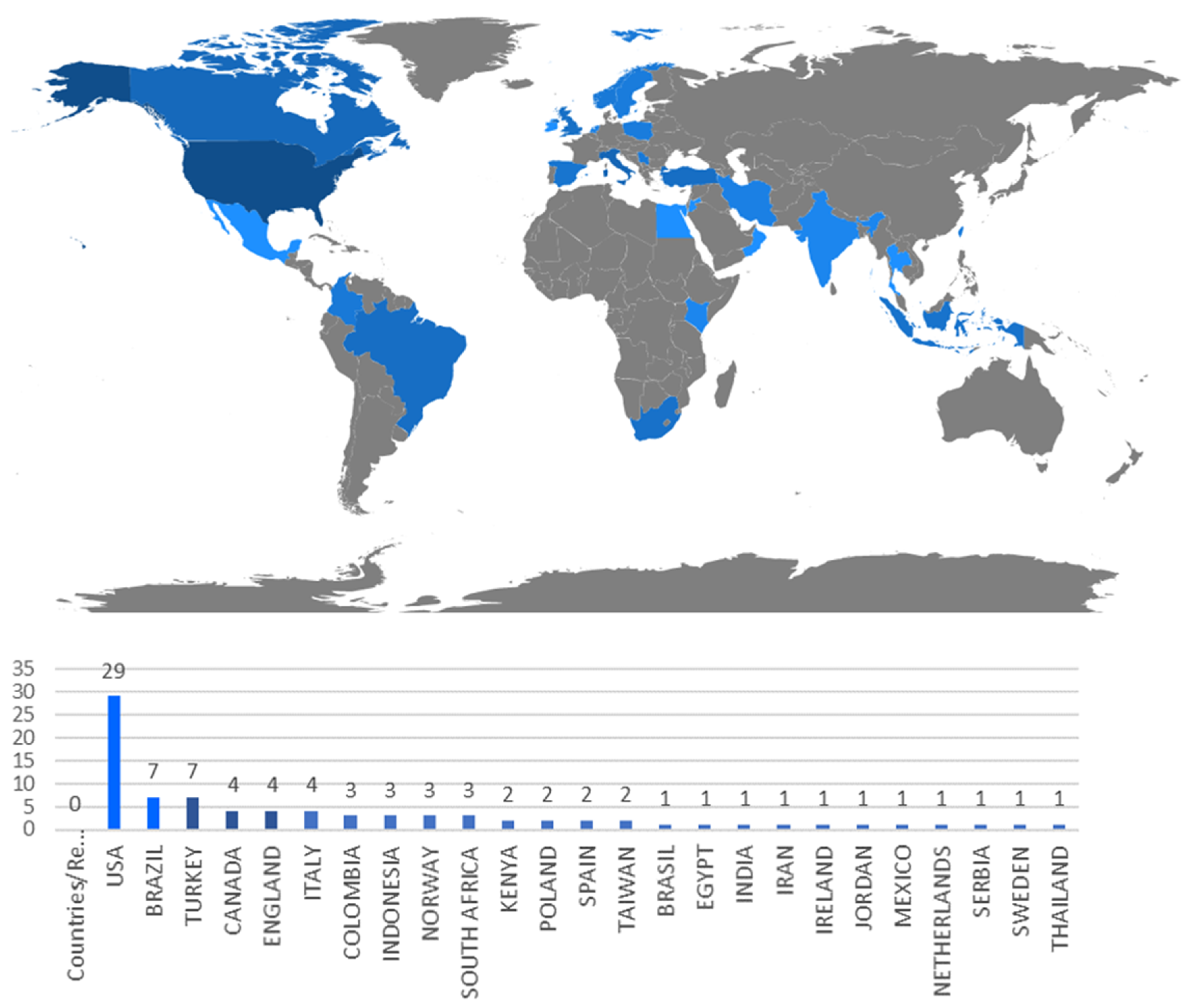
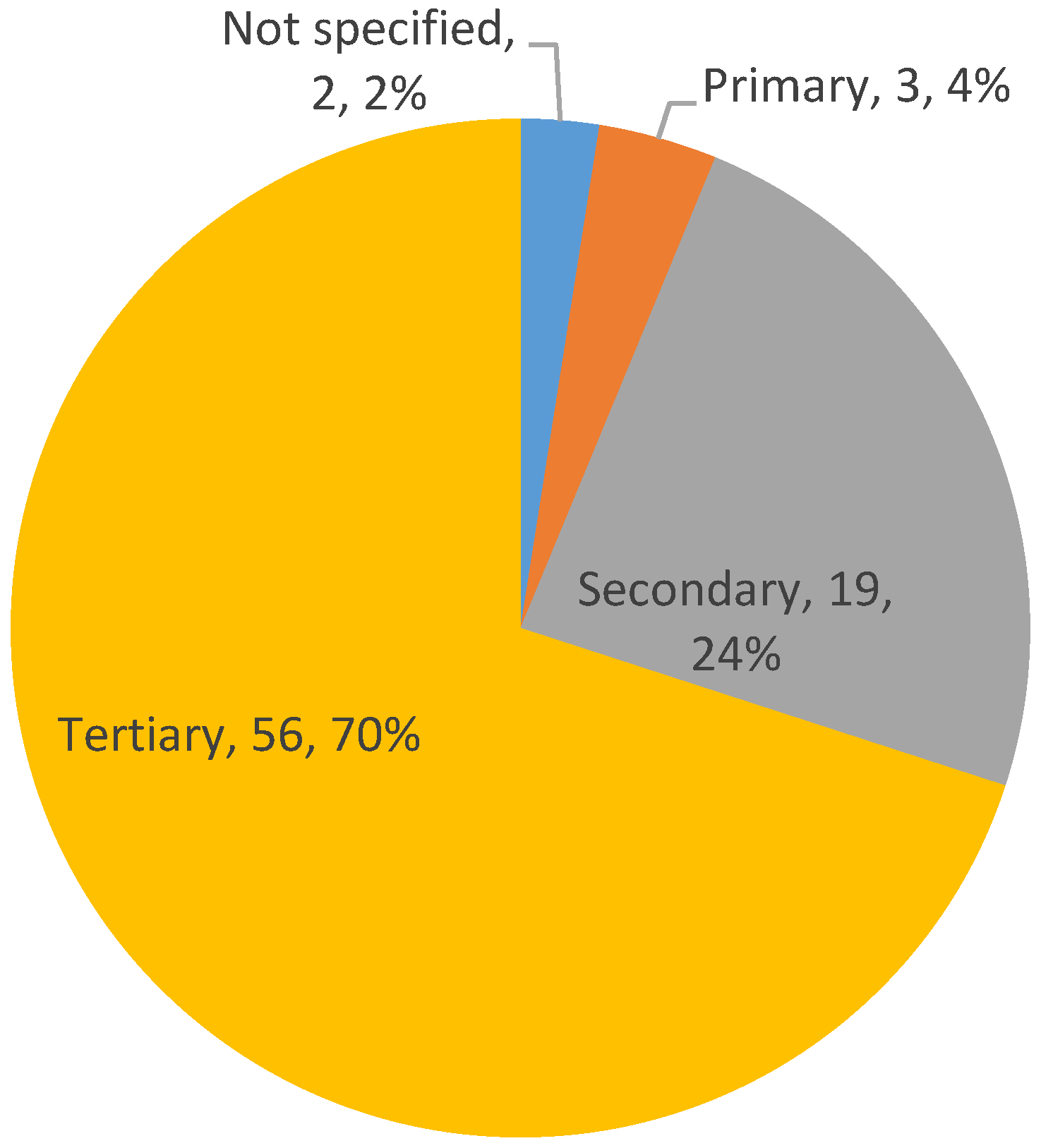
4.2. RQ2:Where Has the VSM Methodology Been Applied since 2015?
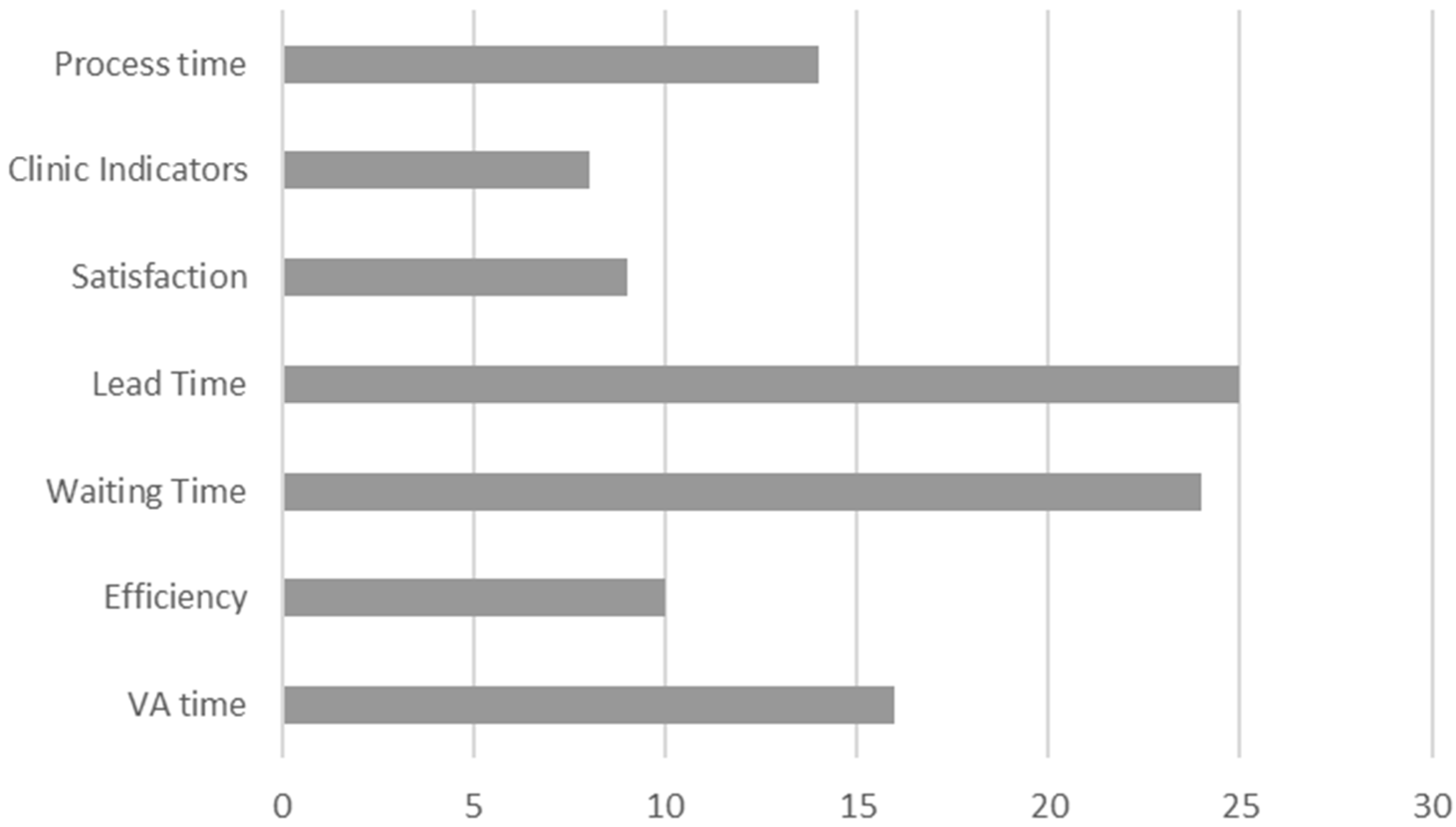
4.3. RQ3: What Is the Impact of VSM on Sustainability?
4.4. RQ4: Is VSM Applied Alone or Combined with Other Lean Tools?
4.5. RQ5: What Is the Most Common VSM Version in the Healthcare Sector Publications?
5. Discussion
6. Conclusions
Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Souza Gomes dos Santos, A.C.; da Cunha Reis, A.; de Dos, S.G.; Santos, C.; Ferreria, I.L.; Figueiredo, L.A. The first evidence about conceptual vs analytical lean healthcare research studies. J. Health Organ. Manag. 2020, 34, 789–806. [Google Scholar] [CrossRef] [PubMed]
- Dahlgaard, J.J.; Pettersen, J.; Dahlgaard-Park, S.M. Quality and lean health care: A system for assessing and improving the health of healthcare organisations. Total Qual. Manag. Bus. Excell. 2011, 22, 673–689. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Bonavia, T. Strategic Priorities and Lean Manufacturing Practices in Automotive Suppliers. Ten Years After. In New Trends and Developments in Automotive Engineering; Chiaberge, M., Ed.; InTech: London, UK, 2011; Available online: http://www.intechopen.com/articles/show/title/strategic-priorities-and-lean-manufacturing-practices-in-automotive-suppliers-ten-years-after (accessed on 10 December 2020).
- Marin-Garcia, J.A.; Carneiro, P. Desarrollo y validación de un modelo multidimensional de la producción ajustada. Intang. Cap. 2010, 6, 78–127. [Google Scholar]
- Marin-Garcia, J.A.; Carneiro, P.; Miralles, C. Effect of Lean Manufacturing practices on non-financial performance results: Empirical study in Spanish sheltered work centers. In Production Systems and Supply Chain Management in Emerging Countries: Best Practices; Mejia, G., Velasco, N., Eds.; Springer: Berlin, Germany, 2012; pp. 3–24. ISBN 978-3-642-26003-2. [Google Scholar]
- Scott, G. Customer Satisfaction: Six Strategies for Continuous Improvement. J. Healthc. Manag. 2001, 46, 82. [Google Scholar] [CrossRef] [PubMed]
- Marin-Garcia, J.A.; Mateo Martínez, R. Barreras y facilitadores de la implantación del TPM. Intang. Cap. 2013, 9, 823–853. [Google Scholar] [CrossRef]
- Vidal-Carreras, P.I.; Garcia-Sabater, J.J.; Marin-Garcia, J.A.; Garcia-Sabater, J.P. Value Stream Mapping on Healthcare. In 2015 International Conference on Industrial Engineering and Systems Management (IESM); Framinan, J.M., Gonzalez, P.P., Artiba, A., Eds.; IEEE: Piscataway, NJ, USA, 2015; pp. 272–276. [Google Scholar]
- Coetzee, R.; van der Merwe, K.; van Dyk, L. Lean implementation strategies: How are the Toyota Way principles addressed? S. Afr. J. Ind. Eng. 2016, 27, 79–91. [Google Scholar] [CrossRef]
- Shou, W.; Wang, J.; Wu, P.; Wang, X.; Chong, H.-Y. A cross-sector review on the use of value stream mapping. Int. J. Prod. Res. 2017, 55, 3906–3928. [Google Scholar] [CrossRef]
- Rother, M.; Shook, J. Learning to See: Value Stream Mapping to Create Value and Eliminate Muda; Lean Enterprise Institute: Boston, MA, USA, 1998; p. 102. [Google Scholar]
- Muñoz-Villamizar, A.; Santos, J.; Garcia-Sabater, J.J.; Lleo, A.; Grau, P. Green value stream mapping approach to improving productivity and environmental performance. Int. J. Product. Perform. Manag. 2019, 68, 608–625. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-analysis; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Nowak, M.; Pfaff, H.; Karbach, U. Does Value Stream Mapping affect the structure, process, and outcome quality in care facilities? A systematic review. Syst. Rev. 2017, 6, 11. [Google Scholar] [CrossRef]
- Dinis-Carvalho, J.; Guimaraes, L.; Sousa, R.M.; Leao, C.P. Waste identification diagram and value stream mapping: A comparative analysis. Int. J. Lean Six Sigma 2019, 10, 767–783. [Google Scholar] [CrossRef]
- Hines, P.; Rich, N. The seven value stream mapping tools. Int. J. Oper. Prod. Manag. 1997, 17, 46–64. [Google Scholar] [CrossRef]
- Lucherini, F.; Rapaccini, M. Exploring the impact of lean manufacturing on flexibility in SMEs. J. Ind. Eng. Manag. 2017, 10, 919–945. [Google Scholar] [CrossRef]
- Bevilacqua, M.; Ciarapica, F.E.; Germani, M.; Mazzuto, G.; Paciarotti, C. Relation of project managers’ personality and project performance: An approach based on value stream mapping. J. Ind. Eng. Manag. 2014, 7, 857–890. [Google Scholar] [CrossRef]
- Tapping, D. La Nueva Guia Lean de Bolsillo (Produccion Lean). Herramientas Para Eliminar el Desperdicio; MCS Media, Inc.: Finksburg, MD, USA, 2007. [Google Scholar]
- Tapping, D.; Luyster, T.; Shuker, T. Value Stream Management Eight Steps to Planning, Mapping, and Sustaining Lean Improvements, 1st ed.; Productivity Press: New York, NY, USA, 2002; ISBN 1-56327-245-8. [Google Scholar]
- Tapping, D.; Shuker, T. Value Stream Management for the Lean Office; Productivity Press: New York, NY, USA, 2003; ISBN 1-56327-246-6. [Google Scholar]
- Cringles, M.C. Developing an integrated care pathway to manage cancer pain across primary, secondary and tertiary care. Int. J. Palliat. Nurs. 2002, 8, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Grumbach, K.; Bodenheimer, T. The Organization of Health Care. JAMA 1995, 273, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, S.C.; Damberg, C.L.; Silverman, M.; Motala, A.; Shekelle, P.G. What Defines a High-Performing Health Care Delivery System: A Systematic Review. Jt. Comm. J. Qual. Patient Saf. 2017, 43, 450–459. [Google Scholar] [CrossRef]
- Sanchez-Ruiz, L.; Blanco, B.; Marin-Garcia, J.A.; Diez-Busto, E. Scoping Review of Kaizen and Green Practices: State of the Art and Future Directions. Int. J. Environ. Res. Public Health 2020, 17, 8258. [Google Scholar] [CrossRef]
- Urdan, M.S.; Luoma, P. Designing Effective Sustainability Assignments: How and Why Definitions of Sustainability Impact Assignments and Learning Outcomes. J. Manag. Educ. 2020, 44, 794–821. [Google Scholar] [CrossRef]
- Gaikwad, L.; Sunnapwar, V. An integrated Lean, Green and Six Sigma strategies: A systematic literature review and directions for future research. TQM J. 2020, 32, 201–225. [Google Scholar] [CrossRef]
- Lorenzon dos Santos, D.; Giglio, R.; Helleno, A.L.; Campos, L.M.S. Environmental aspects in VSM: A study about barriers and drivers. Prod. Plan. Control 2019, 30, 1239–1249. [Google Scholar] [CrossRef]
- Helleno, A.L.; de Moraes, A.J.I.; Simon, A.T. Integrating sustainability indicators and Lean Manufacturing to assess manufacturing processes: Application case studies in Brazilian industry. J. Clean. Prod. 2017, 153, 405–416. [Google Scholar] [CrossRef]
- Farias, L.M.S.; Santos, L.C.; Gohr, C.F.; de Oliveira, L.C.; da Silva Amorim, M.H. Criteria and practices for lean and green performance assessment: Systematic review and conceptual framework. J. Clean. Prod. 2019, 218, 746–762. [Google Scholar] [CrossRef]
- Antony, J.; Sunder M, V.; Sreedharan, R.; Chakraborty, A.; Gunasekaran, A. A systematic review of Lean in healthcare: A global prospective. Int. J. Qual. Reliab. Manag. 2019, 36, 1370–1391. [Google Scholar] [CrossRef]
- Abdallah, A.B.; Alkhaldi, R.Z. Lean bundles in health care: A scoping review. J. Health Organ. Manag. 2019, 33, 488–510. [Google Scholar] [CrossRef] [PubMed]
- Podgorodnichenko, N.; Akmal, A.; Edgar, F.; Everett, A.M. Sustainable HRM: Toward addressing diverse employee roles. Empl. Relat. 2020. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Bonavia, T.; Losilla, J.-M. Changes in the Association between European Workers’ Employment Conditions and Employee Well-being in 2005, 2010 and 2015. Int. J. Environ. Res. Public Health 2020, 17, 1048. [Google Scholar] [CrossRef]
- Saunders, M.; Lewis, P.; Thornhill, A. Research Methods for Business Students, 7/e; Pearson Education: Essex, UK, 2016; ISBN 978-1-292-01662-7. [Google Scholar]
- Makwana, A.D.; Patange, G.S. A methodical literature review on application of Lean & Six Sigma in various industries. Aust. J. Mech. Eng. 2019. [Google Scholar] [CrossRef]
- Romero, L.F.; Arce, A. Applying Value Stream Mapping in Manufacturing: A Systematic Literature Review. IFAC-PapersOnLine 2017, 50, 1075–1086. [Google Scholar] [CrossRef]
- Singh, B.; Garg, S.K.; Sharma, S.K. Value stream mapping: Literature review and implications for Indian industry. Int. J. Adv. Manuf. Technol. 2011, 53, 799–809. [Google Scholar] [CrossRef]
- Augusto, B.P.; Tortorella, G.L. Literature review on lean healthcare implementation: Assessment methods and practices. Int. J. Serv. Oper. Manag. 2019, 32, 285–306. [Google Scholar] [CrossRef]
- Syltevik, S.; Karamperidis, S.; Antony, J.; Taheri, B. Lean for airport services: A systematic literature review and agenda for future research. Int. J. Qual. Reliab. Manag. 2018, 35, 34–49. [Google Scholar] [CrossRef]
- Rafique, M.Z.; Ab Rahman, M.N.; Saibani, N.; Arsad, N. A systematic review of lean implementation approaches: A proposed technology combined lean implementation framework. Total Qual. Manag. Bus. Excell. 2019, 30, 386–421. [Google Scholar] [CrossRef]
- Poksinska, B. The current state of lean implementation in health care: Literature review. Qual. Manag. Health Care 2010, 19, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Gitlow, H.; Zuo, Q.; Ullmann, S.G.; Zambrana, D.; Campo, R.E.; Lubarsky, D.; Birnbach, D.J. The causes of never events in hospitals. Int. J. Lean Six Sigma 2013, 4, 338–344. [Google Scholar] [CrossRef]
- Heinzen, M.; Mettler, S.; Coradi, A.; Boutellier, R. A new application of value-stream mapping in new drug development: A case study within Novartis. Drug Discov. Today 2015, 20, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Marin-Garcia, J.A.; Garcia-Sabater, J.J.; Maheut, J. Protocol: Action planning for action research about kaizen in public organizations. The case of higher education. WPOM-Work. Pap. Oper. Manag. 2018, 9, 1. [Google Scholar] [CrossRef]
- Alrashed, I.A.; Kang, P.S. Applying lean principles to health economics transactional flow process to improve the healthcare delivery. In Proceedings of the 2017 IEEE International Conference on Industrial Engineering and Engineering Management (IEEM); IEEE: Piscataway, NJ, USA, 2017; pp. 879–883. [Google Scholar]
- Bhat, S.; Antony, J.; Gijo, E.V.; Cudney, E.A. Lean Six Sigma for the healthcare sector: A multiple case study analysis from the Indian context. Int. J. Qual. Reliab. Manag. 2019, 37, 90–111. [Google Scholar] [CrossRef]
- Costa, L.B.M.; Filho, M.G.; Rentes, A.F.; Bertani, T.M.; Mardegan, R. Lean healthcare in developing countries: Evidence from Brazilian hospitals. Int. J. Health Plann. Manag. 2017, 32, e99–e120. [Google Scholar] [CrossRef]
- Bucci, S.; De Belvis, A.G.; Marventano, S.; De Leva, A.C.; Tanzariello, M.; Specchia, M.L.; Ricciardi, W.; Franceschi, F. Emergency Department crowding and hospital bed shortage: Is Lean a smart answer? A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 4209–4219. [Google Scholar]
- Moraros, J.; Lemstra, M.; Nwankwo, C. Lean interventions in healthcare: Do they actually work? A systematic literature review. Int. J. Qual. Heal. Care 2016, 28, 150–165. [Google Scholar] [CrossRef]
- Cobo, M.J.; López-Herrera, A.G.; Herrera-Viedma, E.; Herrera, F. SciMAT: A new science mapping analysis software tool. J. Am. Soc. Inf. Sci. Technol. 2012, 63, 1609–1630. [Google Scholar] [CrossRef]
- Aria, M. bibliometrix: An R-tool for comprehensive science mapping analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Aguinis, H.; Ramani, R.S.; Alabduljader, N. Best-Practice Recommendations for Producers, Evaluators, and Users of Methodological Literature Reviews. Organ. Res. Methods 2020. [Google Scholar] [CrossRef]
- Andreu Andres, M.A.; Garcia-Carbonell, A.; González-Ladrón-de-Guevara, F.; Watts, F. Contrasting innovation competence FINCODA model in software engineering: Narrative review. J. Ind. Eng. Manag. 2018, 11, 715–734. [Google Scholar] [CrossRef]
- Fadahunsi, K.P.; Akinlua, J.T.; O’Connor, S.; Wark, P.A.; Gallagher, J.; Carroll, C.; Majeed, A.; O’Donoghue, J. Protocol for a systematic review and qualitative synthesis of information quality frameworks in eHealth. BMJ Open 2019, 9, e024722. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Alfalla-Luque, R. Protocol: How to deal with Partial Least Squares (PLS) research in Operations Management. A guide for sending papers to academic journals. WPOM-Work. Pap. Oper. Manag. 2019. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Betancour, E.; Giraldo-OMeara, M. Protocol: Literature review on the psychometric properties of the short versions of the scales of social desirability in the answers to competency self-assessment questionnaires. WPOM-Work. Pap. Oper. Manag. 2018, 9, 14–29. [Google Scholar] [CrossRef]
- Martínez Jurado, P.J.; Moyano Fuentes, J. Aprendiendo a Enseñar Lean Management mediante Juegos: Revisión Sistemática de la Literatura Learning to Teach Lean Management through Games: Systematic Literature Review. WPOM-Work. Pap. Oper. Manag. 2017, 8, 164–170. [Google Scholar] [CrossRef]
- Medina-López, C.; Marin-Garcia, J.A.; Alfalla Luque, R. Una propuesta metodológica para la realización de búsquedas sistemáticas de bibliografía (A methodological proposal for the systematic literature review). WPOM 2010, 1, 13–30. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Martinez-Tomas, J. Protocol: What does the wage structure depend on? Evidence from the INE salary national survey (pilot study with 2006 data). WPOM-Work. Pap. Oper. Manag. 2019, 10, 70–103. [Google Scholar] [CrossRef]
- Marin-Garcia, J.A.; Vidal-Carreras, P.I.; Garcia Sabater, J.J.; Escribano-Martinez, J. Protocol: Value Stream Maping in Healthcare. A systematic literature review. WPOM-Work. Pap. Oper. Manag. 2019, 10, 36. [Google Scholar] [CrossRef]
- Aloini, D.; Cannavacciuolo, L.; Gitto, S.; Lettieri, E.; Malighetti, P.; Visintin, F. Evidence-Based Management for Performance Improvement in HealthCare. Manag. Decis. 2018, 56, 2063–2068. [Google Scholar] [CrossRef]
- Reijula, J.; Nevala, N.; Lahtinen, M.; Ruohomäki, V.; Reijula, K. Lean design improves both health-care facilities and processes: A literature review. Intell. Build. Int. 2014, 6, 170–185. [Google Scholar] [CrossRef]
- Gonzalez-Aleu, F.; Van Aken, E.M.; Cross, J.; Glover, W.J. Continuous improvement project within Kaizen: Critical success factors in hospitals. TQM J. 2018, 30, 335–355. [Google Scholar] [CrossRef]
- Losilla, J.-M.; Oliveras, I.; Marin-Garcia, J.A.; Vives, J. Three risk of bias tools lead to opposite conclusions in observational research synthesis. J. Clin. Epidemiol. 2018, 101, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Marin-Garcia, J.A.; Martinez Tomas, J. Deconstructing AMO framework: A systematic review. Intang. Cap. 2016, 12, 1040. [Google Scholar] [CrossRef]
- Sanchez, L.; Blanco, B. Three decades of continuous improvement. Total Qual. Manag. Bus. Excell. 2014, 25, 986–1001. [Google Scholar] [CrossRef]
- Sanchez-Ruiz, L.; Marin-Garcia, J.A.; Blanco, B. Protocol: A Meta-Review on continuous improvement to know the state of this research field. WPOM-Working Pap. Oper. Manag. 2018, 9, 88. [Google Scholar] [CrossRef]
- Knight, C.; Patterson, M.; Dawson, J. Work engagement interventions can be effective: A systematic review. Eur. J. Work Organ. Psychol. 2019, 28, 348–372. [Google Scholar] [CrossRef]
- Lummus, R.R.; Vokurka, R.J.; Rodeghiero, B. Improving quality through value stream mapping: A case study of a physician’s clinic. Total Qual. Manag. Bus. Excell. 2006, 17, 1063–1075. [Google Scholar] [CrossRef]
- Dogan, N.O.; Unutulmaz, O. Lean production in healthcare: A simulation-based value stream mapping in the physical therapy and rehabilitation department of a public hospital. Total Qual. Manag. Bus. Excell. 2016, 27, 64–80. [Google Scholar] [CrossRef]
- Vandborg, M.P.; Edwards, K.; Kragstrup, J.; Vedsted, P.; Hansen, D.G.; Mogensen, O. A New Method for Analyzing Diagnostic Delay in Gynecological Cancer. Int. J. Gynecol. Cancer 2012, 22, 712–717. [Google Scholar] [CrossRef] [PubMed]
- Wulff Barreiro, E. El uso del software HistCite para identificar artículos significativos en búsquedas por materias en la Web of Science. Doc. las Ciencias la Inf. 2007, 30, 45–64. [Google Scholar]
- Swancutt, D.; Joel-Edgar, S.; Allen, M.; Thomas, D.; Brant, H.; Benger, J.; Byng, R.; Pinkney, J. Not all waits are equal: An exploratory investigation of emergency care patient pathways. BMC Health Serv. Res. 2017, 17, 436. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, G.L.; Fogliatto, F.S.; Anzanello, M.; Marodin, G.A.; Garcia, M.; Reis Esteves, R. Making the value flow: Application of value stream mapping in a Brazilian public healthcare organisation. Total Qual. Manag. Bus. Excell. 2017, 28, 1544–1558. [Google Scholar] [CrossRef]
- Hicks, C.; McGovern, T.; Prior, G.; Smith, I. Applying lean principles to the design of healthcare facilities. Int. J. Prod. Econ. 2015, 170, 677–686. [Google Scholar] [CrossRef]
- Henrique, D.B.; Rentes, A.F.; Godinho Filho, M.; Esposto, K.F. A new value stream mapping approach for healthcare environments. Prod. Plan. Control 2016, 27, 24–48. [Google Scholar] [CrossRef]
- Improta, G.; Balato, G.; Romano, M.; Carpentieri, F.; Bifulco, P.; Alessandro Russo, M.; Rosa, D.; Triassi, M.; Cesarelli, M. Lean Six Sigma: A new approach to the management of patients undergoing prosthetic hip replacement surgery. J. Eval. Clin. Pract. 2015, 21, 662–672. [Google Scholar] [CrossRef]
- Duska, L.R.; Mueller, J.; Lothamer, H.; Pelkofski, E.B.; Novicoff, W.M. Lean methodology improves efficiency in outpatient academic Gynecologic Oncology clinics. Gynecol. Oncol. 2015, 138, 707–711. [Google Scholar] [CrossRef]
- Improta, G.; Balato, G.; Romano, M.; Ponsiglione, A.M.; Raiola, E.; Russo, M.A.; Cuccaro, P.; Santillo, L.C.; Cesarelli, M. Improving performances of the knee replacement surgery process by applying DMAIC principles. J. Eval. Clin. Pract. 2017, 23, 1401–1407. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Steenwyk, B.L.; Watson, C.; Sparrow, J.; Belopolsky, V.; Townsley, M.; Lyerly, R.; Downing, M.; Bryant, A.; Gurley, W.Q.; et al. Decreasing the Preincision Time for Pulmonary Lobectomy: The Process of Lean and Value Stream Mapping. Ann. Thorac. Surg. 2016, 101, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- White, B.A.; Yun, B.J.; Lev, M.H.; Raja, A.S. Applying Systems Engineering Reduces Radiology Transport Cycle Times in the Emergency Department. West. J. Emerg. Med. 2017, 18, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Towbin, A.J.; Perry, L.A.; Larson, D.B. Improving efficiency in the radiology department. Pediatr. Radiol. 2017, 47, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Sampalli, T.; Desy, M.; Dhir, M.; Edwards, L.; Dickson, R. Improving wait times to care for individuals with multimorbidities and complex conditions using value stream mapping. Int. J. Heal. Policy Manag. 2015, 4, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Bal, A.; Ceylan, C.; Taçoğlu, C. Using value stream mapping and discrete event simulation to improve efficiency of emergency departments. Int. J. Healthc. Manag. 2017, 10, 196–206. [Google Scholar] [CrossRef]
- Sirvent, J.M.; Gil, M.; Alvarez, T.; Martin, S.; Vila, N.; Colomer, M.; March, E.; Loma-Osorio, P.; Metje, T. Técnicas «Lean» para la mejora del flujo de los pacientes críticos de una región sanitaria con epicentro en el servicio de medicina intensiva de un hospital de referencia. Med. Intensiva 2016, 40, 266–272. [Google Scholar] [CrossRef]
- Krupp, N.L.; Fiscus, C.; Webb, R.; Webber, E.C.; Stanley, T.; Pettit, R.; Davis, A.; Hollingsworth, J.; Bagley, D.; McCaskey, M.; et al. Multifaceted quality improvement initiative to decrease pediatric asthma readmissions. J. Asthma 2017, 54, 911–918. [Google Scholar] [CrossRef]
- Haddad, M.G.; Zouein, P.P.; Salem, J.; Otayek, R. Case Study of Lean in Hospital Admissions to Inspire Culture Change. Eng. Manag. J. 2016, 28, 209–223. [Google Scholar] [CrossRef]
- Robinson, F.G.; Cunningham, L.L.; Turner, S.P.; Lindroth, J.; Ray, D.; Khan, T.; Yates, A. Improving a Dental School’s Clinic Operations Using Lean Process Improvement. J. Dent. Educ. 2016, 80, 1170–1179. [Google Scholar] [CrossRef]
- Cheung, Y.Y.; Goodman, E.M.; Osunkoya, T.O. No More Waits and Delays: Streamlining Workflow to Decrease Patient Time of Stay for Image-guided Musculoskeletal Procedures. RadioGraphics 2016, 36, 856–871. [Google Scholar] [CrossRef]
- Martínez, P.; Martínez, J.L.; Cavazos, J.; Nuño, J.P. Mejora en el tiempo de atención al paciente en una Unidad de urgencias por medio de Lean Manufacturing. Nov. Sci. 2016, 8, 17–40. [Google Scholar] [CrossRef][Green Version]
- Martínez, P.; Martínez, J.; Nuño, P.; Cavazos, J. Mejora en el tiempo de atención al paciente en una unidad de urgencias gineco-obstétricas mediante la aplicación de Lean Manufacturing. Rev. Lasallista Investig. 2016, 13, 46–56. [Google Scholar] [CrossRef]
- Marisdina, S.; Junadi, P. Utilizing Lean Management Techniques to Improve Head CT Scan Turnaround Time of Ischemic Stroke Patients in the Emergency Department of Dr. Mohammad Hoesin Hospital, Palembang. KnE Life Sci. 2018, 4, 305. [Google Scholar] [CrossRef]
- Sánchez, M.; Suárez, M.; Asenjo, M.; Bragulat, E. Improvement of emergency department patient flow using lean thinking. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2018, 30, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Firman, F.; Koentjoro, T.; Widodo, K.H.; Utarini, A. The effect of lean six sigma toward maternal emergency lead time in penembahan senopati hospital, bantul, yogyakarta. BALI Med. J. 2019, 8, 435–443. [Google Scholar] [CrossRef]
- Improta, G.; Romano, M.; Di Cicco, M.V.; Ferraro, A.; Borrelli, A.; Verdoliva, C.; Triassi, M.; Cesarelli, M. Lean thinking to improve emergency department throughput at AORN Cardarelli hospital. BMC Health Serv. Res. 2018, 18, 914. [Google Scholar] [CrossRef] [PubMed]
- Damle, A.; Andrew, N.; Kaur, S.; Orquiola, A.; Alavi, K.; Steele, S.R.; Maykel, J. Elimination of waste: Creation of a successful Lean colonoscopy program at an academic medical center. Surg. Endosc. 2016, 30, 3071–3076. [Google Scholar] [CrossRef]
- Lisiecka-Biełanowicz, M.; Biechowska, D.; Brzozowski, S.; Hermanowski, T. Mapping process of the stroke treatment at the Institute of Psychiatry and Neurology in Warsaw. Postępy Psychiatr. Neurol. 2018, 27, 172–179. [Google Scholar] [CrossRef]
- Al Hroub, A.; Obaid, A.; Yaseen, R.; El-Aqoul, A.; Zghool, N.; Abu-Khudair, H.; Al Kakani, D.; Alloubani, A. Improving the Workflow Efficiency of an Outpatient Pain Clinic at a Specialized Oncology Center by Implementing Lean Principles. Asia-Pacific J. Oncol. Nurs. 2019, 6, 381. [Google Scholar] [CrossRef]
- Al-Balushi, M.M.; Al-Mandhari, Z. Implementing Lean Management Techniques at a Radiation Oncology Department. Sultan Qaboos Univ. Med. J. 2018, 18, e362. [Google Scholar] [CrossRef]
- Gjolaj, L.N.; Campos, G.G.; Olier-Pino, A.I.; Fernandez, G.L. Delivering Patient Value by Using Process Improvement Tools to Decrease Patient Wait Time in an Outpatient Oncology Infusion Unit. J. Oncol. Pract. 2016, 12, E95–E100. [Google Scholar] [CrossRef] [PubMed]
- Akdag, H.C.; Cantürk, N.Z. Improvement of Breast Cancer Patient Pathway Using EUSOMA Standards and European Guidelines. Chirurgia 2017, 112, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Camgoz-Akdag, H.; Beldek, T.; Konyalioglu, A.K. Process improvement in a radiology department with value stream mapping and its linkage to industry 4.0. Iioab J. 2018, 9, 36–41. [Google Scholar]
- Camgöz-Akdağ, H.; Çalişkan, E.; Toma, S. Lean process design for a radiology department. Bus. Process Manag. J. 2017, 23, 779–791. [Google Scholar] [CrossRef]
- de Oliveira, K.B.; dos Santos, E.F.; Junior, L.V.G. Lean Healthcare as a Tool for Improvement: A Case Study in a Clinical Laboratory. In Advances in Human Factors and Ergonomics in Healthcare; (Advances in Intelligent Systems and Computing; Vol. 482); Duffy, V.G., Lightner, N., Eds.; Advances in Intelligent Systems and Computing; Springer: Berlin, Germany, 2017; pp. 129–140, ISBN 978-3-319-41652-6; 978-3-319-41651-9. [Google Scholar]
- Alkher, M.; Radosevic, M.; Beker, I.; Cabarkapa, V.; Toljaga-nikolic, D.; Caric, M.; Moraca, S. Case Study of Healthcare Organization Improvement with Lean Concept. Teh. Vjesn. Tech. Gaz. 2019, 26, 845–851. [Google Scholar] [CrossRef]
- Roy, A.; Colpitts, J.; Becker, K.; Brewer, J.; van Lutterveld, R. Improving efficiency in neuroimaging research through application of Lean principles. PLoS ONE 2018, 13, e0205232. [Google Scholar] [CrossRef]
- Gupta, S.; Kapil, S.; Sharma, M. Improvement of laboratory turnaround time using lean methodology. Int. J. Health Care Qual. Assur. 2018, 31, 295–308. [Google Scholar] [CrossRef]
- Monroe-Wise, A.; Reisner, E.; Sherr, K.; Ojakaa, D.; Mbau, L.; Kisia, P.; Muhula, S.; Farquhar, C. Using lean manufacturing principles to evaluate wait times for HIV-positive patients in an urban clinic in Kenya. Int. J. STD AIDS 2017, 28, 1410–1418. [Google Scholar] [CrossRef]
- Hoffmann, C.J.; Milovanovic, M.; Kinghorn, A.; Kim, H.-Y.; Motlhaoleng, K.; Martinson, N.A.; Variava, E. Value stream mapping to characterize value and waste associated with accessing HIV care in South Africa. PLoS ONE 2018, 13, e0201032. [Google Scholar] [CrossRef]
- Mabuto, T.; Hansoti, B.; Kerrigan, D.; Mshweshwe-Pakela, N.; Kubeka, G.; Charalambous, S.; Hoffmann, C. HIV testing services in healthcare facilities in South Africa: A missed opportunity. J. Int. AIDS Soc. 2019, 22, e25367. [Google Scholar] [CrossRef]
- van der Sluijs, A.F.; van Slobbe-Bijlsma, E.R.; Goossens, A.; Vlaar, A.P.; Dongelmans, D.A. Reducing errors in the administration of medication with infusion pumps in the intensive care department: A lean approach. SAGE Open Med. 2019, 7, 205031211882262. [Google Scholar] [CrossRef] [PubMed]
- Ersson, A.; Beckman, A.; Jarl, J.; Borell, J. Effects of a multifaceted intervention QI program to improve ICU performance. BMC Health Serv. Res. 2018, 18, 838. [Google Scholar] [CrossRef] [PubMed]
- Durur, F.; Akbulut, Y. Lean methodology for pathology laboratories: A case study from a public hospital. Turkish J. Pathol. 2019, 35, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Sugianto, J.Z.; Stewart, B.; Ambruzs, J.M.; Arista, A.; Park, J.Y.; Cope-Yokoyama, S.; Luu, H.S. Applying the Principles of Lean Production to Gastrointestinal Biopsy Handling: From the Factory Floor to the Anatomic Pathology Laboratory. Lab. Med. 2015, 46, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Cromwell, S.; Chiasson, D.A.; Cassidy, D.; Somers, G.R. Improving Autopsy Report Turnaround Times by Implementing Lean Management Principles. Pediatr. Dev. Pathol. 2018, 21, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Ankrum, A.L.; Neogi, S.; Morckel, M.A.; Wilhite, A.W.; Li, Z.; Schaffzin, J.K. Reduced isolation room turnover time using Lean methodology. Infect. Control Hosp. Epidemiol. 2019, 40, 1151–1156. [Google Scholar] [CrossRef]
- Fields, E.; Neogi, S.; Schoettker, P.J.; Lail, J. Using Lean methodologies to streamline processing of requests for durable medical equipment and supplies for children with complex conditions. Healthcare 2018, 6, 245–252. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Ferrari-Light, D.; Ren-Fielding, C.; Fielding, G.; Perry, N.; Rabinovich, A.; Saraceni, M.; Fitzpatrick, M.; Jain, S.; Pachter, H.L. Improving Operating Room Turnover Time in a New York City Academic Hospital via Lean. Ann. Thorac. Surg. 2019, 107, 1011–1016. [Google Scholar] [CrossRef]
- Lebina, L.; Alaba, O.; Ringane, A.; Hlongwane, K.; Pule, P.; Oni, T.; Kawonga, M. Process evaluation of implementation fidelity of the integrated chronic disease management model in two districts, South Africa. BMC Health Serv Res. 2019, 19, 965. [Google Scholar] [CrossRef]
- Ramaswamy, R.; Rothschild, C.; Alabi, F.; Wachira, E.; Muigai, F.; Pearson, N. Using Value Stream Mapping to improve quality of care in low-resource facility settings. Int. J. Qual. Health Care 2017, 29, 961–965. [Google Scholar] [CrossRef]
- Smith, I. Operationalising the Lean principles in maternity service design using 3P methodology. BMJ Qual. Improv. Rep. 2016, 5, u208920.w5761. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Da Costa, D.G.; Pasin, S.S.; de Magalhães, A.M.M.; de Moura, G.M.S.S.; Rosso, C.B.; Saurin, T.A. Análise do preparo e administração de medicamentos no contexto hospitalar com base no pensamento Lean. Esc. Anna Nery Rev. Enferm. 2018, 22, e20170402. [Google Scholar]
- Pazeti, M.; Calache, L. Application of Lean Six Sigma Concepts to Medicine Dispensation of Public Health Centers. In Advances in Human Factors and Ergonomics in Healthcare; (Advances in Intelligent Systems and Computing; Vol. 482); Duffy, V.G., Lightner, N., Eds.; Springer: Berlin, Germany, 2017; pp. 119–127, ISBN 978-3-319-41652-6; 978-3-319-41651-9. [Google Scholar]
- Johannessen, K.A.; Alexandersen, N. Improving accessibility for outpatients in specialist clinics: Reducing long waiting times and waiting lists with a simple analytic approach. BMC Health Serv. Res. 2018, 18, 827. [Google Scholar] [CrossRef] [PubMed]
- Sayyida, G.; Fahma, F.; Iftadi, I. Process Improvement in Outpatient Installation RSUD dr. Soediran Mangun Sumarso Using Lean Hospital Approach. IOP Conf. Ser. Mater. Sci. Eng. 2018, 319, 012077. [Google Scholar] [CrossRef]
- Deniz, N.; Özçelik, F. Improving healthcare service processes by lean thinking. Pamukkale Univ. J. Eng. Sci. 2018, 24, 739–748. [Google Scholar] [CrossRef]
- Henrique, H.A.; Carolina, B.A.; Priscilla, L. Application of Engineering Concepts in the Sterile Processing Department. In World Congress on Medical Physics and Biomedical Engineering; (IFMBE Proceedings; Vol. 68); Lhotska, L., Sukupova, L., Lackovic, I., Ibbott, G., Eds.; Springer: Berlin, Germany, 2018; Volume 3, pp. 355–360. [Google Scholar]
- Wannemuehler, T.J.; Elghouche, A.N.; Kokoska, M.S.; Deig, C.R.; Matt, B.H. Impact of Lean on surgical instrument reduction: Less is more. Laryngoscope 2015, 125, 2810–2815. [Google Scholar] [CrossRef] [PubMed]
- Hung, S.-H.; Wang, P.-C.; Lin, H.-C.; Chen, H.-Y.; Su, C.-T. Integration of Value Stream Map and Healthcare Failure Mode and Effect Analysis into Six Sigma Methodology to Improve Process of Surgical Specimen Handling. J. Healthc. Eng. 2015, 6, 377–398. [Google Scholar] [CrossRef] [PubMed]
- Lot, L.T.; Sarantopoulos, A.; Min, L.L.; Perales, S.R.; de Fatima Santana Ferreira Boin, I.; de Ataide, E.C. Using Lean tools to reduce patient waiting time. Leadersh. Health Serv. 2018, 31, 343–351. [Google Scholar] [CrossRef]
- Barakauskas, V.E.; Bradshaw, T.A.; Smith, L.D.; Lehman, C.M.; Johnson-Davis, K.L. Process Optimization to Improve Immunosuppressant Drug Testing Turnaround Time. Am. J. Clin. Pathol. 2016, 146, 182–190. [Google Scholar] [CrossRef]
- Khodambashi, S. Alignment of an intra-operating management process to a health information system: A Lean analysis approach. Pers. UBIQUITOUS Comput. 2015, 19, 689–698. [Google Scholar] [CrossRef]
- Huddle, M.G.; Tirabassi, A.; Turner, L.; Lee, E.; Ries, K.; Lin, S.Y. Application of Lean Sigma to the Audiology Clinic at a Large Academic Center. Otolaryngol. NECK Surg. 2016, 154, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Antosz, K.; Stadnicka, D.; Ratnayake, R.M.C. Use of lean management philosophy in health sector: A VSM based case study. In Proceedings of the 2016 IEEE International Conference on Industrial Engineering and Engineering Management (IEEM); IEEE: Piscataway, NJ, USA, 2016; pp. 1523–1528. [Google Scholar]
- Mascarella, M.A.; Lahrichi, N.; Cloutier, F.; Kleiman, S.; Payne, R.J.; Rosenberg, L. High efficiency endocrine operation protocol: From design to implementation. Surgery 2016, 160, 1118–1124. [Google Scholar] [CrossRef] [PubMed]
- Anisi, S.; Marzban, S.; Zarei, E.; Sepehri, M.M. Identifying process improvement opportunities in gynecology clinic by value stream mapping. Iioab J. 2017, 8, 27–32. [Google Scholar]
- Newman-Casey, P.A.; Musser, J.A.; Niziol, L.M.; Heisler, M.M.; Kamat, S.S.; Shah, M.M.; Patel, N.; Cohn, A.M. Integrating Patient Education Into the Glaucoma Clinical Encounter. J. Glaucoma 2019, 28, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Drayton Jackson, M.; Bartman, T.; McGinniss, J.; Widener, P.; Dunn, A.L. Optimizing patient flow in a multidisciplinary haemophilia clinic using quality improvement methodology. Haemophilia 2019, hae.13768. [Google Scholar] [CrossRef]
- Gleich, S.J.; Nemergut, M.E.; Stans, A.A.; Haile, D.T.; Feigal, S.A.; Heinrich, A.L.; Bosley, C.L.; Tripathi, S. Improvement in patient transfer process from the operating room to the PICU using a Lean and Six Sigma--based quality improvement project. Hosp. Pediatr. 2016, 6, 483–489. [Google Scholar] [CrossRef]
- Gray, M.L.; Chen, S.; Kinberg, E.; Colley, P.; Malkin, B.D. Using Lean to Improve Patient Safety and Resource Utilization After Pediatric Adenotonsillectomy. J. Patient Saf. 2019, 1. [Google Scholar] [CrossRef]
- Ortíz-Barrios, M.A.; Escorcia-Caballero, J.P.; Sánchez-Sánchez, F.; De Felice, F.; Petrillo, A. Efficiency Analysis of Integrated Public Hospital Networks in Outpatient Internal Medicine. J. Med. Syst. 2017, 41, 163. [Google Scholar] [CrossRef]
- Ajdari, A.; Boyle, L.N.; Kannan, N.; Rowhani-Rahbar, A.; Wang, J.; Mink, R.; Ries, B.; Wainwright, M.; Groner, J.I.; Bell, M.J.; et al. Examining Emergency Department Treatment Processes in Severe Pediatric Traumatic Brain Injury. J. Healthc. Qual. 2017, 39, 334–344. [Google Scholar] [CrossRef]
- Özcan-Top, Ö.; McCaffery, F. A hybrid assessment approach for medical device software development companies. J. Softw. Evol. Process 2018, 30, e1929. [Google Scholar] [CrossRef]
- Schmidt, S.; Shay, L.A.; Saygin, C.; Wan, H.; Schulz, K.; Clark, R.A.; Shireman, P.K. Improving pilot project application and review processes: A novel application of lean six sigma in translational science. J. Clin. Transl. Sci. 2018, 2, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-H.; Chiu, M.-C. A Mathematical Model to Evaluate and Improve Lean Management of Healthcare System: A Case Study of Health Examination Center. In Transdisciplinary Engineering: A Paradigm Shift; (Advances in Transdisciplinary Engineering; Vol. 5); Chen, C.H., Trappey, A.C., Peruzzini, M., Stjepandic, J., Wognum, N., Eds.; IOS Press: Amsterdam, The Netherlands, 2017; pp. 530–537. [Google Scholar]
- Afsar-manesh, N.; Lonowski, S.; Namavar, A.A. Leveraging lean principles in creating a comprehensive quality program: The UCLA health readmission reduction initiative. Healthcare 2017, 5, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Martinez, D.A.; Tsalatsanis, A.; Yalcin, A.; Zayas-Castro, J.L.; Djulbegovic, B. Activating clinical trials: A process improvement approach. Trials 2016, 17, 106. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, S.L.; Joseph, P.L.; Cavaliere, I.J.; Bayley, M.T.; Lo, A. Optimising the mandatory reporting process for drivers admitted to an inpatient stroke rehabilitation unit. BMJ Open Qual. 2018, 7, e000203. [Google Scholar] [CrossRef] [PubMed]
- Valdez, M.M.; Liwanag, M.; Mount, C.; Rodriguez, R.; Avalos-Reyes, E.; Smith, A.; Collette, D.; Starsiak, M.; Green, R. Utilizing Lean Six Sigma Methodology to Improve the Authored Works Command Approval Process at Naval Medical Center San Diego. Mil. Med. 2018, 183, e405–e410. [Google Scholar] [CrossRef] [PubMed]
- Vilasdechanon, S.; Sopadang, A. Business Process Reengineering for the Saline Management in Hospitals. In 2018 5th International Conference on Industrial Engineering and Applications (ICIEA), Singapore, 26–28 April 2018; IEEE-Inst Electrical Electronics Engineers Inc.: New York, NY, USA, 2018; pp. 84–88. [Google Scholar]
- Ahmed, M.; Jones, E.; Redmond, E.; Hewedi, M.; Wingert, A.; Gad El Rab, M. Food production and service in UK hospitals. Int. J. Health Care Qual. Assur. 2015, 28, 40–54. [Google Scholar] [CrossRef] [PubMed]
- Marin-Garcia, J.A.; Garcia-Sabater, J.P.; Ruiz, A.; Maheut, J.; Garcia-Sabater, J.J. Operations Management at the Service of Health Care Management: Example of a Proposal for Action Research to Plan and Schedule Health Resources in Scenarios Derived from the COVID-19 Outbreak. J. Ind. Eng. Manag. 2020, 13, 213–227. [Google Scholar] [CrossRef]
- Nicolay, C.R.; Purkayastha, S.; Greenhalgh, A.; Benn, J.; Chaturvedi, S.; Phillips, N.; Darzi, A. Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. Br. J. Surg. 2012, 99, 324–335. [Google Scholar] [CrossRef]
- Sharma, G.V.S.S.; Prasad, C.L.V.R.S.; Srinivasa Rao, M. Industrial engineering into healthcare—A comprehensive review. Int. J. Healthc. Manag. 2020. [Google Scholar] [CrossRef]
- Akmal, A.; Greatbanks, R.; Foote, J. Lean thinking in healthcare—Findings from a systematic literature network and bibliometric analysis. Health Policy 2020, 124, 615–627. [Google Scholar] [CrossRef]
- Zepeda-Lugo, C.; Tlapa, D.; Baez-Lopez, Y.; Limon-Romero, J.; Ontiveros, S.; Perez-Sanchez, A.; Tortorella, G. Assessing the Impact of Lean Healthcare on Inpatient Care: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 5609. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Barraza, M.F.; Miguel-Davila, J.A. Kaizen–Kata, a Problem-Solving Approach to Public Service Health Care in Mexico. A Multiple-Case Study. Int. J. Environ. Res. Public Health 2020, 17, 3297. [Google Scholar] [CrossRef] [PubMed]
- Nagi, A.; Altarazi, S. Integration of value stream map and strategic layout planning into DMAIC approach to improve carpeting process. J. Ind. Eng. Manag. 2017, 10, 74–97. [Google Scholar] [CrossRef]
- Montoya-Reyes, M.; Gonzalez-Angeles, A.; Mendoza-Munoz, I.; Gil-Samaniego-Ramos, M.; Ling-Lopez, J. Method Engineering to Increase Labor Productivity and Eliminate Downtime. J. Ind. Eng. Manag. 2020, 13, 321–331. [Google Scholar] [CrossRef]
- Rodriguez-Garcia, M.; McLean-Carranza, A.A.; Carlos Prado-Prado, J.; Dominguez-Caamano, P. Managing Waiting Times to Predict No-shows and Cancelations at a Children’s Hospital. J. Ind. Eng. Manag. 2016, 9, 1107–1118. [Google Scholar] [CrossRef]
- Assis Ferreira, G.S.; Silva, U.R.; Costa, A.L.; de Dallavalle Padua, S.I. The promotion of BPM and lean in the health sector: Main results. Bus. Process Manag. J. 2018, 24, 400–424. [Google Scholar] [CrossRef]
- Tlapa, D.; Zepeda-Lugo, C.A.; Tortorella, G.L.; Baez-Lopez, Y.A.; Limon-Romero, J.; Alvarado-Iniesta, A.; Rodriguez-Borbon I., M. Effects of Lean Healthcare on Patient Flow: A Systematic Review. Value Health 2020, 23, 260–273. [Google Scholar] [CrossRef]
- Frichi, Y.; Jawab, F.; Boutahari, S. Modeling the Impact of Hospital Logistics on Quality of Care and Patient Satisfaction: Results of a Survey in Three Public Healthcare Facilities in Fez—Morocco. J. Ind. Eng. Manag. 2020, 13, 296–320. [Google Scholar] [CrossRef]
- Abdelfattah, F.A.; Rahman, M.S.; Osman, M. Assessing the antecedents of customer loyalty on healthcare insurance products: Service quality; perceived value embedded model. J. Ind. Eng. Manag. 2015, 8, 1639–1660. [Google Scholar] [CrossRef]
- Mahmoud, A.S.; Ahmad, M.H.; Yatim, Y.M.; Dodo, Y.A. Key Performance Indicators (KPIs) to Promote Building Developers Safety Performance in the Construction Industry. J. Ind. Eng. Manag. 2020, 13, 371–401. [Google Scholar] [CrossRef]
- Crema, M.; Verbano, C. Safety improvements from health lean management implementation Evidences from three cases. Int. J. Qual. Reliab. Manag. 2016, 33, 1150–1178. [Google Scholar] [CrossRef]
- Singh, P. Lean in healthcare organization: An opportunity for environmental sustainability. Benchmarking Int. J. 2019, 26, 205–220. [Google Scholar] [CrossRef]
- Hallam, C.R.A.; Contreras, C. Lean healthcare: Scale, scope and sustainability. Int. J. Health Care Qual. Assur. 2018, 31, 684–696. [Google Scholar] [CrossRef]
- Kovacevic, M.; Jovicic, M.; Djapan, M.; Zivanovic-Macuzic, I. Lean thinking in healthcare: Review of implementation results. Int. J. Qual. Res. 2016, 10, 219–229. [Google Scholar] [CrossRef]
- Macedo Gomes, A.; Senna, P.; Monteiro, A.; Pinha, D. Study on techniques and tools used in lean healthcare implementation: A literature review. Braz. J. Oper. Prod. Manag. 2016, 13, 406–420. [Google Scholar] [CrossRef]
- Swarnakar, V.; Singh, A.R.; Tiwari, A.K. Evaluating the effect of critical failure factors associated with sustainable Lean Six Sigma framework implementation in healthcare organization. Int. J. Qual. Reliab. Manag. 2020. [Google Scholar] [CrossRef]
- Al Hammadi, F.; Hussain, M. Sustainable organizational performance: A study of health-care organizations in the United Arab Emirates. Int. J. Organ. Anal. 2019, 27, 169–186. [Google Scholar] [CrossRef]
- Jones, D.; Womack, J.; Brunt, D.; Lovejoy, M.; Shook, J. Seeing the Whole Value Stream; Lean enterprise institute: Cambridge, MA, USA, 2011; ISBN 1934109355. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Results |
|---|---|
| Documents | 80 |
| Article | 71 |
| Editorial material | 1 |
| Proceedings paper | 8 |
| Sources (Journals, Books, etc.) | 67 |
| Keywords Plus | 164 |
| Author’s Keywords | 218 |
| Period | 2015–2019 |
| Average citations per documents | 4.784 |
| Authors | 408 |
| Author Appearances | 424 |
| Authors of multi-authored documents | 406 |
| Single-authored documents | 2 |
| Documents per Author | 0.196 |
| Authors per Document | 5.1 |
| Collaboration Index | 5.21 |
| Authors | Articles |
|---|---|
| Cesarelli M | 3 |
| Improta G | 3 |
| Romano M | 3 |
| Balato G | 2 |
| Camgöz-Akdağ H | 2 |
| Cerfolio R. J | 2 |
| Neogi S | 2 |
| Russo M. A | 2 |
| Triassi M | 2 |
| Martínez P | 2 |
| Martínez J | 2 |
| Nuño P | 2 |
| Cavazos J | 2 |
| Paper | Total Citations | TC per Year |
|---|---|---|
| Hicks C, 2015, Int J Prod Econ [76] | 43 | 7.167 |
| Henrique D. B, 2016, Prod Plan Control [77] | 38 | 7.600 |
| Improta G, 2015, J Eval Clin Pract [78] | 22 | 3.667 |
| Tortorella G. L, 2017, Total Qual Manag Bus [75] | 18 | 4.500 |
| Duska L. R, 2015, Gynecol Oncol [79] | 15 | 2.500 |
| Dogan N. O, 2016, Total Qual Manag Bus [71] | 14 | 2.800 |
| Improta G, 2017, J Eval Clin Pract [80] | 13 | 3.250 |
| Cerfolio R. J, 2016, Ann Thorac Surg [81] | 13 | 2.600 |
| White B. A, 2017, West J Emerg Med [82] | 12 | 3.000 |
| Towbin A. J, 2017, Pediatr Radiol [83] | 10 | 2.500 |
| Sampalli T, 2015, Int J Health Policy [84] | 10 | 1.667 |
| Bal A, 2017, Int J Healthcare Man [85] | 8 | 2.000 |
| Sirvent J. M, 2016, Med Intensiva [86] | 8 | 1.600 |
| Swancutt D, 2017, BMC Health Serv Res [74] | 7 | 1.750 |
| Krupp N. L, 2017, J Asthma [87] | 7 | 1.750 |
| Haddad M. G, 2016, Eng Manag J [88] | 7 | 1.400 |
| Robinson F. G, 2016, J Dent Educ [89] | 7 | 1.400 |
| Cheung Y. Y, 2016, Radiographics [90] | 7 | 1.400 |
| Healthcare Field | Articles | No. |
|---|---|---|
| Emergency | [74,82,85,91,92,93,94,95,96,97,98] | 11 |
| Oncology | [77,79,99,100,101] | 5 |
| Radiology | [83,90,102,103,104] | 5 |
| Laboratory | [105,106,107,108] | 4 |
| HIV | [109,110,111] | 3 |
| Intensive Care Unit | [86,112,113] | 3 |
| Pathology | [114,115,116] | 3 |
| Pediatrics | [87,117,118] | 3 |
| Cardiothoracic Surgery and Anesthesiology | [81,119] | 2 |
| Chronic Service | [84,120] | 2 |
| Maternity Unit | [121,122] | 2 |
| Medicine dispensation | [123,124] | 2 |
| Orthopedics and Traumatology | [78,80] | 2 |
| Outpatient Services | [125,126] | 2 |
| Physical Therapy and Rehabilitation | [71,127] | 2 |
| Sterilization | [75,128] | 2 |
| Surgical Unit | [129,130] | 2 |
| Transplants | [131,132] | 2 |
| Anesthesia | [133] | 1 |
| Audiology | [134] | 1 |
| Cardiology | [135] | 1 |
| Dental | [89] | 1 |
| Endocrine | [136] | 1 |
| Endoscopy | [76] | 1 |
| Gynecology | [137] | 1 |
| Glaucoma | [138] | 1 |
| Hemophilia | [139] | 1 |
| Orthopedics | [140] | 1 |
| Otolaryngology | [141] | 1 |
| Outpatient Internal Medicine | [142] | 1 |
| Trauma | [143] | 1 |
| Others | Articles | No. |
| Not specified | [144,145,146,147] | 4 |
| Administrative | [148,149] | 2 |
| Clinical Publications | [150] | 1 |
| Hospital Admissions | [88] | 1 |
| Internal saline process | [151] | 1 |
| Food services | [152] | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marin-Garcia, J.A.; Vidal-Carreras, P.I.; Garcia-Sabater, J.J. The Role of Value Stream Mapping in Healthcare Services: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 951. https://doi.org/10.3390/ijerph18030951
Marin-Garcia JA, Vidal-Carreras PI, Garcia-Sabater JJ. The Role of Value Stream Mapping in Healthcare Services: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(3):951. https://doi.org/10.3390/ijerph18030951
Chicago/Turabian StyleMarin-Garcia, Juan A., Pilar I. Vidal-Carreras, and Julio J. Garcia-Sabater. 2021. "The Role of Value Stream Mapping in Healthcare Services: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 3: 951. https://doi.org/10.3390/ijerph18030951
APA StyleMarin-Garcia, J. A., Vidal-Carreras, P. I., & Garcia-Sabater, J. J. (2021). The Role of Value Stream Mapping in Healthcare Services: A Scoping Review. International Journal of Environmental Research and Public Health, 18(3), 951. https://doi.org/10.3390/ijerph18030951