
Oral Manifestations of Rett Syndrome—A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
Research Question
2. Methodology
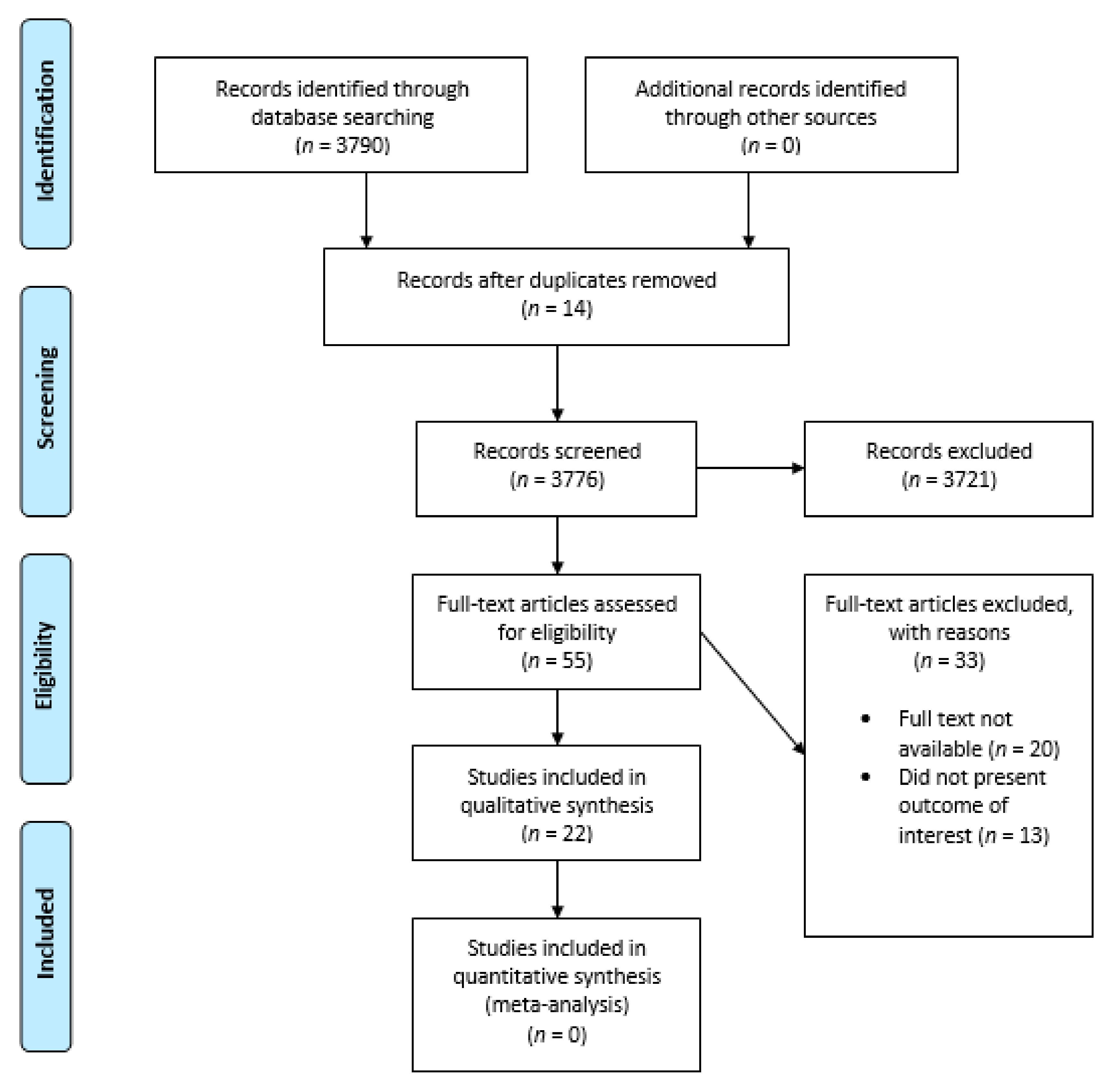
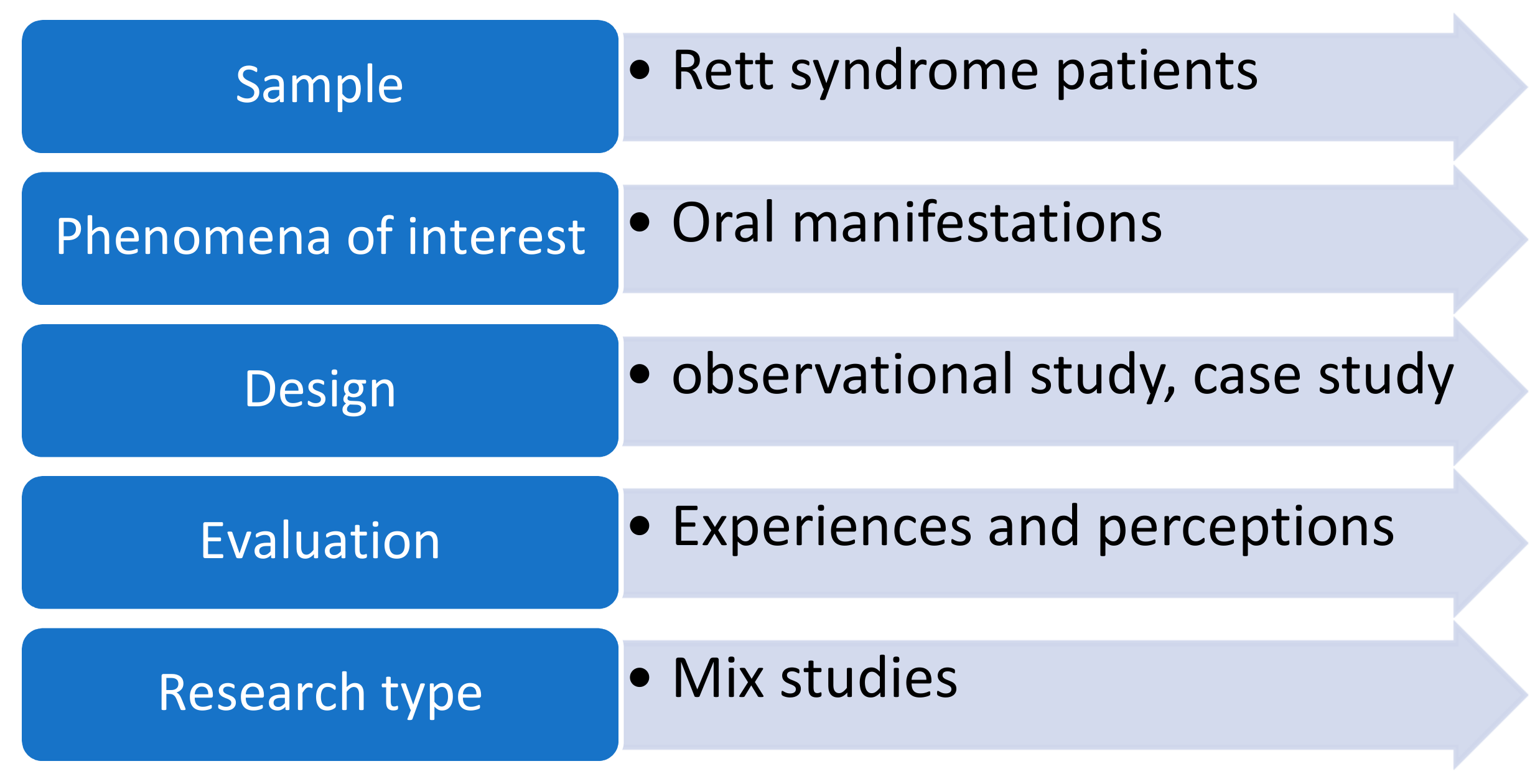
2.1. Search Strategy and Study Selection
2.2. Quality Assessment
3. Results
4. Discussion
4.1. Oral Clinical Manifestations of Rett Syndrome
4.2. Management of Oral Manifestations in Rett Syndrome Patients
4.3. Behavioral and Pharmacological Management of Rett Syndrome Patients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arora, N.K.; Nair, M.K.C.; Gulati, S.; Deshmukh, V.; Mohapatra, A.; Mishra, D.; Patel, V.; Pandey, R.M.; Das, B.C.; Divan, G.; et al. Neurodevelopmental disorders in children aged 2–9 years: Population-based burden estimates across five regions in India. PLoS Med. 2018, 15, e1002615. [Google Scholar] [CrossRef] [PubMed]
- Bromley, R.; Mawer, G.E.; Briggs, M.; Cheyne, C.; Clayton-Smith, J.; García-Fiñana, M.; Kneen, R.; Lucas, S.B.; Shallcross, R.; Baker, G.A.; et al. The prevalence of neurodevelopmental disorders in children prenatally exposed to antiepileptic drugs. J. Neurol. Neurosurg. Psychiatry 2013, 84, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Nerli, E.; Roggero, O.M.; Baj, G.; Tongiorgi, E. In vitro modeling of dendritic atrophy in Rett syndrome: Determinants for phenotypic drug screening in neurodevelopmental disorders. Sci. Rep. 2020, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Percy, A.K. The American History of Rett Syndrome. Pediatr. Neurol. 2014, 50, 1–3. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hagberg, B.; Aicardi, J.; Dias, K. Ramos OJAoNOJotANA, Society tCN. A progressive syndrome of autism, dementia, ataxia, and loss of purposeful hand use in girls: Rett’s syndrome: Report of 35 cases. Ann. Neurol. 1983, 14, 471–479. [Google Scholar] [CrossRef]
- Cocca, S.; Viviano, M.; Loglisci, M.; Parrini, S.; Monciatti, G.; Paganelli, I.I.; Livi, W.; Mezzedimi, C. Correlation Between Dysphagia and Malocclusion in Rett Syndrome: A preliminary study. Sultan Qaboos Univ. Med. J. 2019, 18, e489–e493. [Google Scholar] [CrossRef]
- Leonard, H.; Ravikumara, M.; Baikie, G.; Naseem, N.; Ellaway, C.; Percy, A.; Abraham, S.; Geerts, S.; Lane, J.; Jones, M.; et al. Assessment and Management of Nutrition and Growth in Rett Syndrome. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 451–460. [Google Scholar] [CrossRef]
- Meireles, P.T.; Soares, M.B.; Lacerda, D.R.N.B.; Gomes, B.B.M.; De Carvalho, E.E.V.; Salge, A.K.M.; Abdalla, G.K.; Abdalla, D.R. Rett Syndrome in a Peruvian Patient: A Case Report/Síndrome de Rett em um Paciente Peruano: Um Relato de Caso. Braz. J. Dev. 2020, 6, 63967–63974. [Google Scholar] [CrossRef]
- Krajnc, N. Management of epilepsy in patients with Rett syndrome: Perspectives and considerations. Ther. Clin. Risk Manag. 2015, 11, 925–932. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- West, S.; King, V.; Carey, T.S.; Lohr, K.N.; McKoy, N.; Sutton, S.F.; Lux, L. Systems to rate the strength of scientific evidence. Évid. Rep. Assess. 2002, 47, 1–11. [Google Scholar]
- Morrison, A.; Polisena, J.; Husereau, D.; Moulton, K.; Clark, M.; Fiander, M.; Mierzwinski-Urban, M.; Clifford, T.; Hutton, B.; Rabb, D. The Effect of English-Language Restriction on Systematic Review-Based Meta-Analyses: A Systematic Review of Empirical Studies. Int. J. Technol. Assess. Health Care 2012, 28, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2013. [Google Scholar]
- Peak, J.; Eveson, J.W.; Scully, C. Oral manifestation of Rett’s syndrome. Br. Dent. J. 1992, 172, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, R.; Romano, A.R.; Birman, E.G.; Mayer, M.P. Oral manifestations in Rett syndrome: A study of 17 cases. Pediatr. Dent. 1997, 19, 349–352. [Google Scholar]
- Alpoz, A.R.; Ergul, N.; Oncag, O. Bruxism in Rett syndrome: A case report. J. Clin. Pediatr Dent. 1999, 23, 161–163. [Google Scholar]
- Kohyama, J.; Ohinata, J.; Hasegawa, T. Disturbance of phasic chin muscle activity during rapid-eye-movement sleep. Brain Dev. 2001, 23, S104–S107. [Google Scholar] [CrossRef]
- Magalhães, M.H.C.G.; Kawamura, J.Y.; Araújo, L.C.A. General and oral characteristics in Rett syndrome. Spéc. Care Dent. 2002, 22, 147–150. [Google Scholar] [CrossRef]
- Khalil, S.N.; Hanna, E.; Farag, A.; Armendartz, G. Rett syndrome: Anaesthesia management. Pediatr. Anesth. 2002, 12, 375. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Yagiela, J.; Paterno, V.; Mahler, M. The pathophysiology, medical management and dental implications of fragile X, Rett, and Prader-Willi syndromes. J. Calif. Dent. Assoc. 2003, 31, 693–702. [Google Scholar]
- Lavås, J.; Slotte, A.; Jochym-Nygren, M.; Van Doorn, J.; Engerström, I.W. Communication and eating proficiency in 125 females with Rett syndrome: The Swedish Rett Center Survey. Disabil. Rehabil. 2006, 28, 1267–1279. [Google Scholar] [CrossRef]
- Escribano Hernández, A.; Hernández Corral, T.; Ruiz-Martín, E.; Porteros Sánchez, J.A. Results of a dental care protocol for mentally handicapped patients set in a primary health care area in Spain. Med. Oral Patol. Oral Cir. Bucal 2007, 12, E492–E495. [Google Scholar] [PubMed]
- Green, D.; Flanagan, D. Understanding the autistic dental patient. Gen. Dent. 2008, 56, 167–171. [Google Scholar] [PubMed]
- Bathla, M.; Chandna, S.; Bathla, J.C. Rett’s Syndrome: Diagnostic and therapeutic dilemma. Ger. J. Psychiatry 2010, 13, 157. [Google Scholar]
- Nho, J.-S.; Shin, D.-S.; Moon, J.-Y.; Yi, J.-W.; Kang, J.-M.; Lee, B.-J.; Kim, D.-O.; Chung, J.-Y. Anesthetic management of an adult patient with Rett syndrome and limited mouth opening—A case report. Korean J. Anesthesiol. 2011, 61, 428–430. [Google Scholar] [CrossRef] [PubMed]
- González, M.C.F.; Silvestre, F.-J.; Silla, J.M.A. Oral findings in Rett syndrome: A systematic review of the dental literature. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e37–e41. [Google Scholar] [CrossRef][Green Version]
- Morgan, A.T.; Dodrill, P.; Ward, E.C. Interventions for oropharyngeal dysphagia in children with neurological impairment. Cochrane Database Syst. Rev. 2012, 10, CD009456. [Google Scholar] [CrossRef]
- Fuertes-González, M.-C.; Silvestre, F.J. Oral health in a group of patients with Rett syndrome in the regions of Valencia and Murcia (Spain): A case-control study. Med. Oral Patol. Oral Cir. Bucal 2014, 19, 598. [Google Scholar] [CrossRef]
- Djukic, A.; Rose, S.A.; Jankowski, J.J.; Feldman, J.F. Rett Syndrome: Recognition of Facial Expression and Its Relation to Scanning Patterns. Pediatr. Neurol. 2014, 51, 650–656. [Google Scholar] [CrossRef]
- Janas, A.; Osica, P. Dental issues in Rett syndrome. Dev. Period. Med. 2015, 19, 478–481. [Google Scholar]
- Berman, M.H. Autism Open Access. 2015. Available online: https://www.longdom.org/open-access/autism-spectrum-disordera-paediatric-dentists-perspective-2165-7890-1000158.pdf (accessed on 27 January 2021).
- Karaca, O.; Pinar, H.U.; Ekmekcioglu, S.E.; Doğan, R. Rett syndrome and anaesthetic management: A case report. Med. Sci. Int. Med. J. 2017, 6, 1. [Google Scholar] [CrossRef]
- Mezzedimi, C.; Livi, W.; De Felice, C.; Cocca, S. Dysphagia in Rett Syndrome: A Descriptive Study. Ann. Otol. Rhinol. Laryngol. 2017, 126, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.; King, N.; Downs, J.; Leonard, H. Management of oral and dental problems in Rett syndrome: A narrative review of the literature. J. Disabil. Oral Health 2018, 19, 2. [Google Scholar]
- Bernardo, P.; Raiano, E.; Cappuccio, G.; Dubbioso, R.; Bravaccio, C.; Vergara, E.; Peluso, S.; Manganelli, F.; Esposito, M. The Treatment of Hypersalivation in Rett Syndrome with Botulinum Toxin: Efficacy and Clinical Implications. Neurol. Ther. 2019, 8, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Temudo, T.; Santos, M.; Dias, K.; Calado, E.; Carrilho, I.; Oliveira, G.; Barbot, C.; Fonseca, M.; Cabral, A.; Dias, A.; et al. Stereotypies in Rett syndrome: Analysis of 83 patients with and without detected MECP2 mutations. Neurology 2007, 68, 1183–1187. [Google Scholar] [CrossRef]
- Da Silva, T.R.; Canto, G.D.L. Integração odontologia-fonoaudiologia: A importância da formação de equipes interdisciplinares. Rev. CEFAC 2014, 16, 598–603. [Google Scholar] [CrossRef][Green Version]
- Motil, K.J.; Caeg, E.; Barrish, J.O.; Geerts, S.; Lane, J.B.; Percy, A.K.; Annese, F.; McNair, L.; Skinner, S.A.; Lee, H.-S.; et al. Gastrointestinal and Nutritional Problems Occur Frequently Throughout Life in Girls and Women with Rett Syndrome. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 292–298. [Google Scholar] [CrossRef]
- Li, Y.; Yu, F.; Niu, L.-N.; Hu, W.; Long, Y.; Tay, F.R.; Chen, J.-H. Associations among Bruxism, Gastroesophageal Reflux Disease, and Tooth Wear. J. Clin. Med. 2018, 7, 417. [Google Scholar] [CrossRef]
- Jordão, H.W.; Coleman, H.G.; Kunzmann, A.T.; McKenna, G. The association between erosive toothwear and gastro-oesophageal reflux-related symptoms and disease: A systematic review and meta-analysis. J. Dent. 2020, 95, 103284. [Google Scholar] [CrossRef]
- Bianco, E.; Rota, D. Oral findings in Rett syndrome: An update and review of the literature. Dent. Med Probl. 2018, 55, 441–445. [Google Scholar] [CrossRef]
- Chattopadhyay, S.; Arora, R. The ironies of human mind: A case of Rettsyndrome. Ethiop. J. Health Sci. 2014, 24, 171–174. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Rett Syndrome | 3790 |
| Rett Syndrome and Oral Health | 17 |
| Dental Health of Rett Syndrome patients | 13 |
| Rett syndrome and dentistry | 29 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Article published after 1990 | Articles published prior to 1990 |
| English language only | Articles not in English language |
| Original studies, review articles, case reports, case series | Editorials, opinions, correspondences |
| Only articles published in peer reviewed and indexed journals | Non peer reviewed/non indexed journals |
| Data bases examined (PubMed, CINAHL, Scopus, Medline, embase) | Little or no focus on dental aspects |
| Selection | Comparability | Outcome | Overall | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study & Year | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Score (*) |
| Peak, 1992 | * | * | * | * | * | * | * | 7 | |||
| Ribeiro, 1997 | * | * | * | * | * | * | * | 7 | |||
| Alpoz, 1999 | * | * | * | * | * | * | 6 | ||||
| Kohyama, 2001 | * | * | * | * | * | * | 6 | ||||
| Magalhães, 2002 | * | * | * | * | * | 5 | |||||
| Khalil, 2002 | * | * | * | * | * | * | * | 7 | |||
| Friedlander, 2003 | * | * | * | * | * | * | * | 7 | |||
| Lavas, 2006 | * | * | * | * | * | * | * | * | 8 | ||
| Alfonso, 2007 | * | * | * | * | * | * | * | * | 8 | ||
| Green, 2008 | * | * | * | * | * | 5 | |||||
| Manish, 2010 | * | * | * | * | * | * | 6 | ||||
| Ji-sung, 2011 | * | * | * | * | * | * | * | 7 | |||
| Fuertes, 2011 | * | * | * | * | * | * | * | * | 8 | ||
| Morgan, 2012 | * | * | * | * | * | * | 6 | ||||
| Fuertes, 2014 | * | * | * | * | * | * | * | * | 8 | ||
| Aleksandra, 2014 | * | * | * | * | * | * | * | * | 8 | ||
| Janas, 2015 | * | * | * | * | * | * | 6 | ||||
| Marvin, 2015 | * | * | * | * | 4 | ||||||
| Omer, 2016 | * | * | * | * | * | * | * | 7 | |||
| Mezzedimi, 2017 | * | * | * | * | * | * | * | 7 | |||
| Lai YYL, 2018 | * | * | * | * | * | * | * | 7 | |||
| Pia, 2019 | * | * | * | * | * | * | * | * | * | 9 | |
| Level | First Author, Date, Reference |
|---|---|
| 4 | Peak, 1992 [14] |
| 4 | Ribeiro, 1997 [15] |
| 5 | Alpoz, 1999 [16] |
| 5 | Kohyama, 2001 [17] |
| 4 | Magalhães, 2002 [18] |
| 4 | Khalil, 2002 [19] |
| 5 | Friedlander, 2003 [20] |
| 2b | Lavas, 2006 [21] |
| 5 | Alfonso, 2007 [22] |
| 5 | Green, 2008 [23] |
| 4 | Manish, 2010 [24] |
| 4 | Ji-sung, 2011 [25] |
| 3a | Fuertes, 2011 [26] |
| 1a | Morgan, 2012 [27] |
| 3b | Fuertes, 2014 [28] |
| 5 | Aleksandra, 2014 [29] |
| 5 | Janas, 2015 [30] |
| 4 | Marvin, 2015 [31] |
| 4 | Omer, 2016 [32] |
| 4 | Mezzedimi, 2017 [33] |
| 4 | Lai YYL, 2018 [34] |
| 1b | Pia, 2019 [35] |
| First Author, Date, Reference | Type of Article | Sample Size | Article Key Points | Barriers and Limitations |
|---|---|---|---|---|
| Peak, 1992 [14] | Case report | 5 year old girl | Severe bruxism-gross attrition of canines and incisors, Bilateral masseteric hypertrophy, No caries Patient education, Relaxation techniques, Lower polythene occlusal splint, Sedation or GA recommended. | None |
| Ribeiro, 1997 [15] | Case series | 17 patients with mean age of 7.33 | Bruxism (n = 14/17) Non-physiological dental attrition Digit/hand sucking or biting, mouth breathing, drooling, tongue thrusting. Palatal shelving, anterior open bite Gingivitis 76% (n = 13/17) 2.7% tooth surfaces had dental caries. | None |
| Alpoz, 1999 [16] | Case Report | 5 year old girl | A girl with daytime bruxism. Dental wear, with near complete loss of the dental crown, albeit without exposure to pulp. The patient was offered nitrous oxide sedation and alginate samples were obtained to create a flexible splint for the upper jaw, to be used only when the parents were up and watched, because the patient was not bruxed at night. | Single case study |
| Kohyama, 2001 [17] | Review article | Review | Disturbance in phasic chin muscle activity during rapid-eye-movement sleep (REMS); an elevation of phasic inhibition index (PII), without disturbing of tonic inhibition index (TII) due to functional impairment of the pontine tegmentum. | Reports on autistic tendency in SMEI (severe nocturnal enuresis, autism) patients were not found. |
| Magalhães, 2002 [18] | Case series | 13 patients age 9 years. | Update on the oral (bruxism) and general aspect (stereotyped hand movements, scoliosis) of the disorder. Oral hygiene instruction Dental prophylaxis. Application of topical fluoride. Construction of bite-plane. Acupuncture | Do not have the measure of the efficacy of bruxism treatment in Rett syndrome patients. |
| Khalil, 2002 [19] | Case report | 7 year old girl | The girl weighed 14 kg, was weak, grinding her teeth constantly, and had a poor ability to open her mouth and stretch her neck. Importance of BIS monitor in inducing and maintaining level of anesthesia in children sensitive to drugs | Did not measure the wear on the teeth so do not have the measure of the efficacy of bruxism treatment in Rett syndrome patients. |
| Friedlander, 2003 [20] | Review | Review | Dentists caring for individuals with Rett, fragile X must be familiar with the manifestations of these diseases. They must also be familiar with the medications (anticonvulsants, anti-hypertensives, etc.) used to treat the associated behaviors as they might cause adverse reactions. | None |
| Lavas, 2006 [21] | Original Research | 125 females with mean age of 19.6 years. | This study provides data describing Rett syndrome female difficulties from parents/caregivers aspect regarding eating, communication, functional and oral and dental problems. | The information from the study has been compromised to a small extent by the variation in the number of answers for different questions. |
| Alfonso, 2007 [22] | Original research | 108 patients with mean age 31 years. | Protocol was planned and implemented coordinating with health care levels and workers, it provides necessary dental treatment to a large number of disabled people, who would not have received it otherwise. | It remains to be studied, the success or failure of treatments. A patient satisfaction and a cost analysis is still to be done. |
| Green, 2008 [23] | Review article | Review | Early interventions make the symptoms of the disorder less obvious. Management strategies for pediatric ASD population (Rett syndrome) describing behavioral and drug therapy. | Communication problem, dentists should have patience understanding of this neurological condition. Educating parents and patients in preventive care is imperative. |
| Manish, 2010 [24] | Case report | 8 year old girl | Four stages of Rett’s syndrome have been defined to help characterize the disorder and improve its recognition and diagnosis. Kids with Rett’s syndrome frequently display autistic-like symptoms at an early stage. Certain signs may include jumping on the knees, sleeping problems, a wide-spread gait, teeth grinding and chewing difficulty, slow growth, hallucinations, cognitive disabilities, and breathing difficulties when waking up, such as hyperventilation, apnea, and air swallowing. | Limited case study |
| Ji-sung, 2011 [25] | Case report | 19 year old girl | Many difficulties and issues for anesthetic management of RS patients, such as scoliosis and muscular tonicity and breathing abnormalities, ranging from centrally mediated hyperventilation to apnea, should be considered. Ante grade fiber optic-guided oro-tracheal intubation was possible to perform by an experienced anesthesiologist in patient with limited mouth opening. | Management could not be carried out in an effective and comprehensive manner. |
| Fuertes, 2011 [26] | Review article | 35 cases of RS patients from 1985 to 2007 | Drug-related oral manifestations include xerostomia, stomatitis, glossitis, erythema multiform, sialorrhea, gingivitis, dysphagia etc. Oral findings more prevalent in RS are bruxism, open bite, a high arched palate and gingivitis. | Patient communication capacity. Controversy in bruxism treatment, Sample being too small. |
| Morgan, 2012 [27] | Review article | Review | This review examined the effectiveness of interventions for oropharyngeal dysphagia in children with neurological impairment. The three studies included in the review examined oral sensorimotor treatments and lip strengthening interventions. | Insufficient randomized trials to evaluate the effectiveness of interventions for oropharyngeal dysphagia. |
| Fuertes, 2014 [28] | Case control study | RS Patients = 41 Mean age [13.37 (±) 3.19 years], Control match group = 82 | Observational case-control study, followed the protocol of WHO for conducting health surveys. Data recorded by questionnaire and oral examination used to document caries indicators, CPI (Community Periodontal Index) and oral manifestations. Patients with RS: caries score was lower than the control group, they had increased frequency of periodontal problems, dental wear, drooling, high arched palate and anterior open bite. Oral habits of RS patients: diurnal bruxism, followed by stereotyped tongue movements and oral breathing. | Limited case study. |
| Aleksandra, 2014 [29] | Original research | 37 RS female patients of 2–31 years and 34 Gender- matched Control group of 2–30 years | RTT participants have more difficulty reading emotional expressions and these problems are linked to atypicalities in scanning. | Single problem for each pairing of familiar/novel expressions and secondly, use of a single familiarization time for each problem. |
| Janas, 2015 [30] | Case report | 18 year old girl |
RS patients shall be sent to a medical center where appropriate medical and testing services and qualified personnel are available. Intra oral examination: teeth grinding—bruxism, difficulties in chewing and swallowing, neglect of oral cavity hygiene, oral inflammation with hypertrophic gingiva also many cavities in teeth. Extra oral examination showed hand wringing and washing movements, sudden lurching of the head towards the shoulder. | No specific recommendations on behavior guidance for the dental examination of RS patients. |
| Marvin, 2015 [31] | Review article | Review | Dentists may be the first healthcare providers to recognize that a 1- or 2-year-old child has some type of extraordinary pervasive behavioral disorder. | Treatment modalities are wide and tend to be of much error and no cure is present as these pervasive disorders present various entities. No reliable empirical biological tests (e.g., blood tests or brain scans) for ASD are reliable. |
| Omer, 2016 [32] | Case report | 4.5 years old girl | Regional anesthesia should be preferred for suitable operations in patients with Rett syndrome since it reduces opioids, anesthetic requirements and postoperative respiratory depression. Patients with RS had a lower anesthetic dose requirement compared to the control group and suffered prolonged apnea at the postoperative period. | Utilization of BIS monitored not done to follow anesthetic depth and to titrate the effect of anesthetic agent. |
| Mezzedimi, 2017 [33] | Case study | 61 female patients with mean age of 13.6 years. |
Oral apraxia, dyskinetic tongue movements, prolonged oral stage, and poor bolus formation were the most common findings in all patients and progressive dysphagia was noted by caregivers. Useful instructions and suggestions for preventing dysphagia that facilitates in eating. | Single case reported. |
| Lai YYL, 2018 [34] | Case study | 242 females. |
Dental problems reported in severe genotype RS patients included gingival bleeding; and dental trauma from falls, bruxism or malocclusion. The incidence of restoration and extraction of teeth decreased with higher levels of income although extractions were more common than restorations. | Limited patient collaboration. |
| Pia, 2019 [35] | RCT | 5 female patients. | Treatment with botulinum toxin (BTX) for hyper salivation is effective in reducing saliva production that may help in oral motor functions such as eating and bruxism. | Missing data in income level analysis, the allocated age for the incidence calculations had varied implications for analysis and comparison of the data and finally unclear formal diagnosis of GORD were made. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahdi, S.S.; Jafri, H.A.; Allana, R.; Amenta, F.; Khawaja, M.; Qasim, S.S.B. Oral Manifestations of Rett Syndrome—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1162. https://doi.org/10.3390/ijerph18031162
Mahdi SS, Jafri HA, Allana R, Amenta F, Khawaja M, Qasim SSB. Oral Manifestations of Rett Syndrome—A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(3):1162. https://doi.org/10.3390/ijerph18031162
Chicago/Turabian StyleMahdi, Syed Sarosh, Hafsa Abrar Jafri, Raheel Allana, Francesco Amenta, Mariam Khawaja, and Syed Saad B. Qasim. 2021. "Oral Manifestations of Rett Syndrome—A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 3: 1162. https://doi.org/10.3390/ijerph18031162
APA StyleMahdi, S. S., Jafri, H. A., Allana, R., Amenta, F., Khawaja, M., & Qasim, S. S. B. (2021). Oral Manifestations of Rett Syndrome—A Systematic Review. International Journal of Environmental Research and Public Health, 18(3), 1162. https://doi.org/10.3390/ijerph18031162