
Impact of DST (Daylight Saving Time) on Major Trauma: A European Cohort Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
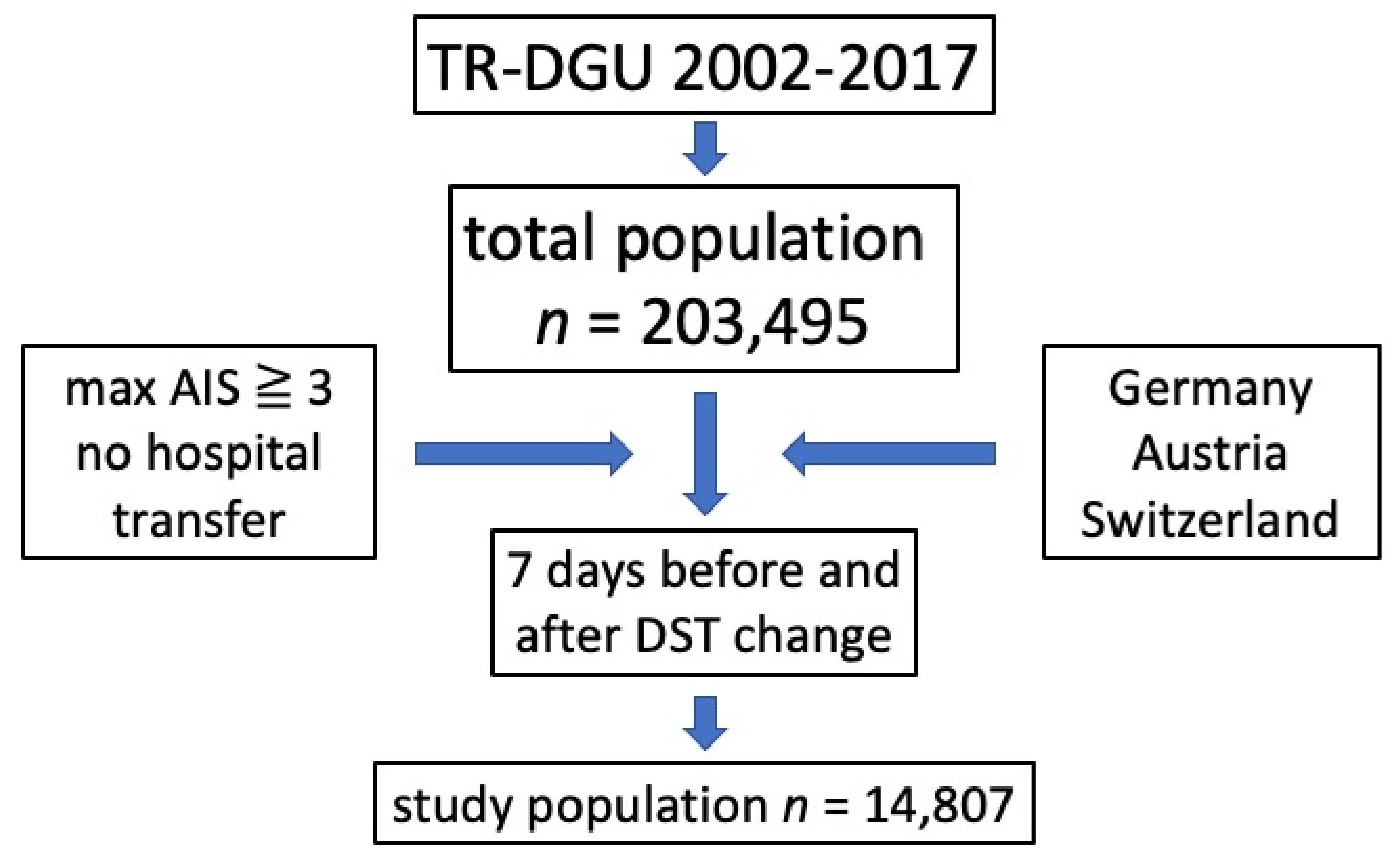
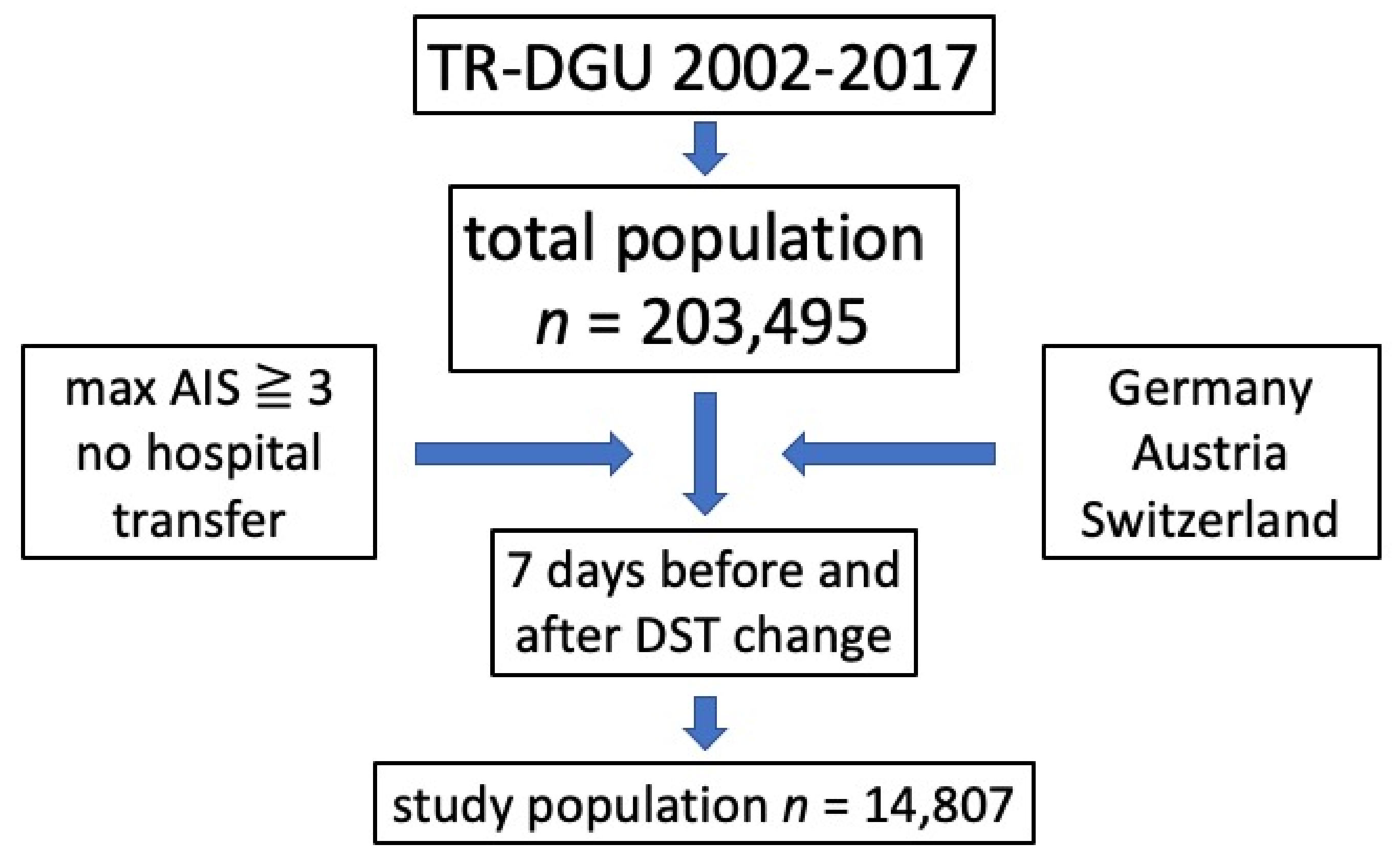
2.1. Data Set
- -
- Demographics;
- -
- Injury patterns;
- -
- Comorbidities;
- -
- Prehospital data;
- -
- Course of hospital treatment, including intensive care unit, relevant laboratory findings, transfusions, and interventions;
- -
- Outcome.
2.2. Statistics
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIS | abbreviated injury scale |
| DST | daylight saving time |
| ICU | intensive care unit |
| ISS | Injury Severity Score |
| IQR | interquartile range |
| RISC II | Revised Injury Severity Classification II |
References
- Summertime Consultation: 84% Want Europe to Stop Changing the Clock. Available online: https://ec.europa.eu/commission/presscorner/detail/en/IP_18_5302 (accessed on 8 December 2021).
- Varughese, J.; Allen, R.P. Fatal Accidents Following Changes in Daylight Savings Time: The American Experience. Sleep Med. 2001, 2, 31–36. [Google Scholar] [CrossRef]
- Kantermann, T.; Juda, M.; Merrow, M.; Roenneberg, T. The Human Circadian Clock’s Seasonal Adjustment Is Disrupted by Daylight Saving Time. Curr. Biol. CB 2007, 17, 1996–2000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janszky, I.; Ljung, R. Shifts to and from Daylight Saving Time and Incidence of Myocardial Infarction. N. Engl. J. Med. 2008, 359, 1966–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MONK, T.H.; APLIN, L.C. Spring and Autumn Daylight Saving Time Changes: Studies of Adjustment in Sleep Timings, Mood, and Efficiency. Ergonomics 1980, 23, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.C. Spring Forward at Your Own Risk: Daylight Saving Time and Fatal Vehicle Crashes. Am. Econ. J. Appl. Econ. 2016, 8, 65–91. [Google Scholar] [CrossRef] [Green Version]
- Czeisler, C.A.; Wickwire, E.M.; Barger, L.K.; Dement, W.C.; Gamble, K.; Hartenbaum, N.; Ohayon, M.M.; Pelayo, R.; Phillips, B.; Strohl, K.; et al. Sleep-Deprived Motor Vehicle Operators Are Unfit to Drive: A Multidisciplinary Expert Consensus Statement on Drowsy Driving. Sleep Health 2016, 2, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Ziebarth, N.R. Sleep, Health, and Human Capital: Evidence from Daylight Saving Time. J. Econ. Behav. Organ. 2020, 170, 174–192. [Google Scholar] [CrossRef]
- Toro, W.; Tigre, R.; Sampaio, B. Daylight Saving Time and Incidence of Myocardial Infarction: Evidence from a Regression Discontinuity Design. Econ. Lett. 2015, 136, 1–4. [Google Scholar] [CrossRef]
- Fritz, J.; VoPham, T.; Wright, K.P.; Vetter, C. A Chronobiological Evaluation of the Acute Effects of Daylight Saving Time on Traffic Accident Risk. Curr. Biol. 2020, 30, 729–735.e2. [Google Scholar] [CrossRef] [PubMed]
- Lahti, T.; Sysi-Aho, J.; Haukka, J.; Partonen, T. Work-Related Accidents and Daylight Saving Time in Finland. Occup. Med. 2011, 61, 26–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, R.N.; Sarma, K.M. Impact of Daylight Saving Time on Road Traffic Collision Risk: A Systematic Review. BMJ Open 2017, 7, e014319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKenzie, E.J. Epidemiology of Injuries: Current Trends and Future Challenges. Epidemiol. Rev. 2000, 22, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Pape-Köhler, C.I.A.; Simanski, C.; Nienaber, U.; Lefering, R. External Factors and the Incidence of Severe Trauma: Time, Date, Season and Moon. Injury 2014, 45, S93–S99. [Google Scholar] [CrossRef] [PubMed]
- AUC: TraumaRegister. Available online: https://www.traumaregister-dgu.de/ (accessed on 12 May 2021).
- Lefering, R.; Huber-Wagner, S.; Nienaber, U.; Maegele, M.; Bouillon, B. Update of the Trauma Risk Adjustment Model of the TraumaRegister DGUTM: The Revised Injury Severity Classification, Version II. Crit. Care 2014, 18, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dauerzählstellen | Straßen.NRW. Available online: https://www.strassen.nrw.de/de/wir-bauen-fuer-sie/verkehr/verkehrsbelastung/dauerzaehlstellen.html (accessed on 8 December 2021).
- Robb, D.; Barnes, T. Accident Rates and the Impact of Daylight Saving Time Transitions. Accid. Anal. Prev. 2018, 111, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Prats-Uribe, A.; Tobías, A.; Prieto-Alhambra, D. Excess Risk of Fatal Road Traffic Accidents on the Day of Daylight Saving Time Change. Epidemiology 2018, 29, e44. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, M.; Hautzinger, H.; Pfeiffer, M. Motorräder: Mobilitätsstrukturen und Expositionsgrößen = Motorcycles: Mobility structure and exposition data. 2020. Available online: https://bast.opus.hbz-nrw.de/opus45-bast/frontdoor/deliver/index/docId/2457/file/M301_barrfreiPDF.pdf; (accessed on 8 December 2021).

{kind=link}
| Accident History, n = 14,488 | |||||
|---|---|---|---|---|---|
| Pre-Week | Post-Week | Total | |||
| DST standard to summer time | car/lorry, n (%) | 758 (21.9) | 778 (20.8) | 1534 (21.3) | |
| motorcycle, n (%) | 349 (10.1) | 529 (14.1) | 878 (12.2) | ||
| bicycle, n (%) | 245 (7.1) | 280 (7.5) | 525 (7.3) | ||
| pedestrians, n (%) | 218 (6.3) | 209 (5.6) | 427 (5.9) | ||
| high fall > 3 m, n (%) | 589 (17.0) | 610 (16.3) | 1199 (16.6) | ||
| low fall < 3 m, n (%) | 869 (25.1) | 870 (23.2) | 1739 (24.1) | ||
| others, n (%) | 430 (12.4) | 472 (12.6) | 902 (12.5) | ||
| total, n | 3456 | 3748 | 7204 | ||
| DST summer to standard time | car/lorry, n (%) | 863 (23.0) | 830 (23.5) | 1693 (23.2) | |
| motorcycle, n (%) | 412 (11.0) | 319 (9.0) | 731 (10.0) | ||
| bicycle, n (%) | 288 (7.7) | 244 (6.9) | 532 (7.3) | ||
| pedestrians, n (%) | 243 (6.5) | 303 (8.6) | 546 (7.5) | ||
| high fall > 3 m, n (%) | 653 (17.4) | 638 (18.1) | 1291 (17.7) | ||
| low fall < 3 m, n (%) | 866 (23.1) | 803 (22.8) | 1669 (22.9) | ||
| others, n (%) | 430 (11.5) | 392 (11.1) | 822 (11.3) | ||
| total, n | 3755 | 3529 | 7284 | ||
| Total | car/lorry, n (%) | 1619 (22.5) | 1608 (22.1) | 3227 (22.3) | |
| motorcycle, n (%) | 761 (10.6) | 848 (11.7) | 1609 (11.1) | ||
| bicycle, n (%) | 533 (7.4) | 524 (7.2) | 1057 (7.3) | ||
| pedestrians, n (%) | 461 (6.4) | 512 (7.0) | 973 (6.7) | ||
| fall > 3 m, n (%) | 1242 (17.2) | 1248 (17.1) | 2490 (17.2) | ||
| fall < 3 m, n (%) | 1735 (24.1) | 1673 (23.1) | 3408 (23.5) | ||
| others, n (%) | 860 (11.9) | 864 (11.9) | 1724 (11.9) | ||
| total, n (%) | 7211 | 7277 | 14,488 | ||
| Impact of DST in Major Trauma | ||||
|---|---|---|---|---|
| Pre-DST | Post-DST | p-Value | ||
| Traffic accident, n (%) | no | 3752 (52.0) | 3695 (50.8) | p = 0.131 |
| yes | 3459 (48.0) | 3582 (49.2) | ||
| Blunt/penetrating trauma, n (%) | blunt | 6749 (95.8) | 6808 (95.6) | p = 0.595 |
| penetrating | 295 (4.2) | 311 (4.4) | ||
| Sex, n (%) | female | 2172 (29.6) | 2066 (27.8) | p = 0.017 |
| male | 5175 (70.4) | 5367 (72.2) | ||
| Age 70+ years, n (%) | <70 | 5459 (74.4) | 5502 (74.2) | p = 0.778 |
| >70 | 1877 (25.6) | 1912 (25.8) | ||
| Died, n (%) | no | 6482 (87.8) | 6495 (87.2) | p = 0.325 |
| yes | 900 (12.2) | 950 (12.8) | ||
| AIS head ≥ 3, n (%) | <3 | 3968 (58.9) | 3993 (53.6) | p = 0.746 |
| ≥3 | 3394 (46.1) | 3452 (46.4) | ||
| AIS thorax ≥ 3, n (%) | <3 | 3898 (52.9) | 3942 (52.9) | p = 0.999 |
| ≥3 | 3464 (47.1) | 3503 (47.1) | ||
| AIS abdomen ≥ 3, n (%) | <3 | 6384 (86.7) | 6473 (86.9) | p = 0.681 |
| ≥3 | 978 (13.3) | 972 (13.1) | ||
| AIS extremities ≥ 3, n (%) | <3 | 5166 (70.2) | 5106 (68.6) | p = 0.036 |
| ≥3 | 2196 (29.8) | 2339 (31.4) | ||
| Pre-DST | Post-DST | p-Value | |
|---|---|---|---|
| Age, mean (SD) | 51 (22) | 51 (22) | 0.501 |
| ISS, mean (SD) | 21.8 (11.7) | 22.3 (12.1) | 0.052 |
| Prognosis based on RISC II, mean % | 13.2 | 13.4 | 0.439 |
| ICU days, median (IQR) | 2 (1–8) | 3 (1–8) | 0.035 |
| Hospital days, median (IQR) | 13 (5–23) | 13 (6–23) | 0.457 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nohl, A.; Seelmann, C.; Roenick, R.; Ohmann, T.; Lefering, R.; Brune, B.; Weichert, V.; Dudda, M.; The TraumaRegister DGU. Impact of DST (Daylight Saving Time) on Major Trauma: A European Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 13322. https://doi.org/10.3390/ijerph182413322
Nohl A, Seelmann C, Roenick R, Ohmann T, Lefering R, Brune B, Weichert V, Dudda M, The TraumaRegister DGU. Impact of DST (Daylight Saving Time) on Major Trauma: A European Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(24):13322. https://doi.org/10.3390/ijerph182413322
Chicago/Turabian StyleNohl, André, Christine Seelmann, Robert Roenick, Tobias Ohmann, Rolf Lefering, Bastian Brune, Veronika Weichert, Marcel Dudda, and The TraumaRegister DGU. 2021. "Impact of DST (Daylight Saving Time) on Major Trauma: A European Cohort Study" International Journal of Environmental Research and Public Health 18, no. 24: 13322. https://doi.org/10.3390/ijerph182413322
APA StyleNohl, A., Seelmann, C., Roenick, R., Ohmann, T., Lefering, R., Brune, B., Weichert, V., Dudda, M., & The TraumaRegister DGU. (2021). Impact of DST (Daylight Saving Time) on Major Trauma: A European Cohort Study. International Journal of Environmental Research and Public Health, 18(24), 13322. https://doi.org/10.3390/ijerph182413322