
The Effects of the Modified Transtheoretical Theory of Stress and Coping (TTSC) Program on Dementia Caregivers’ Knowledge, Burden, and Quality of Life

Abstract
:1. Introduction
2. Materials and Methods
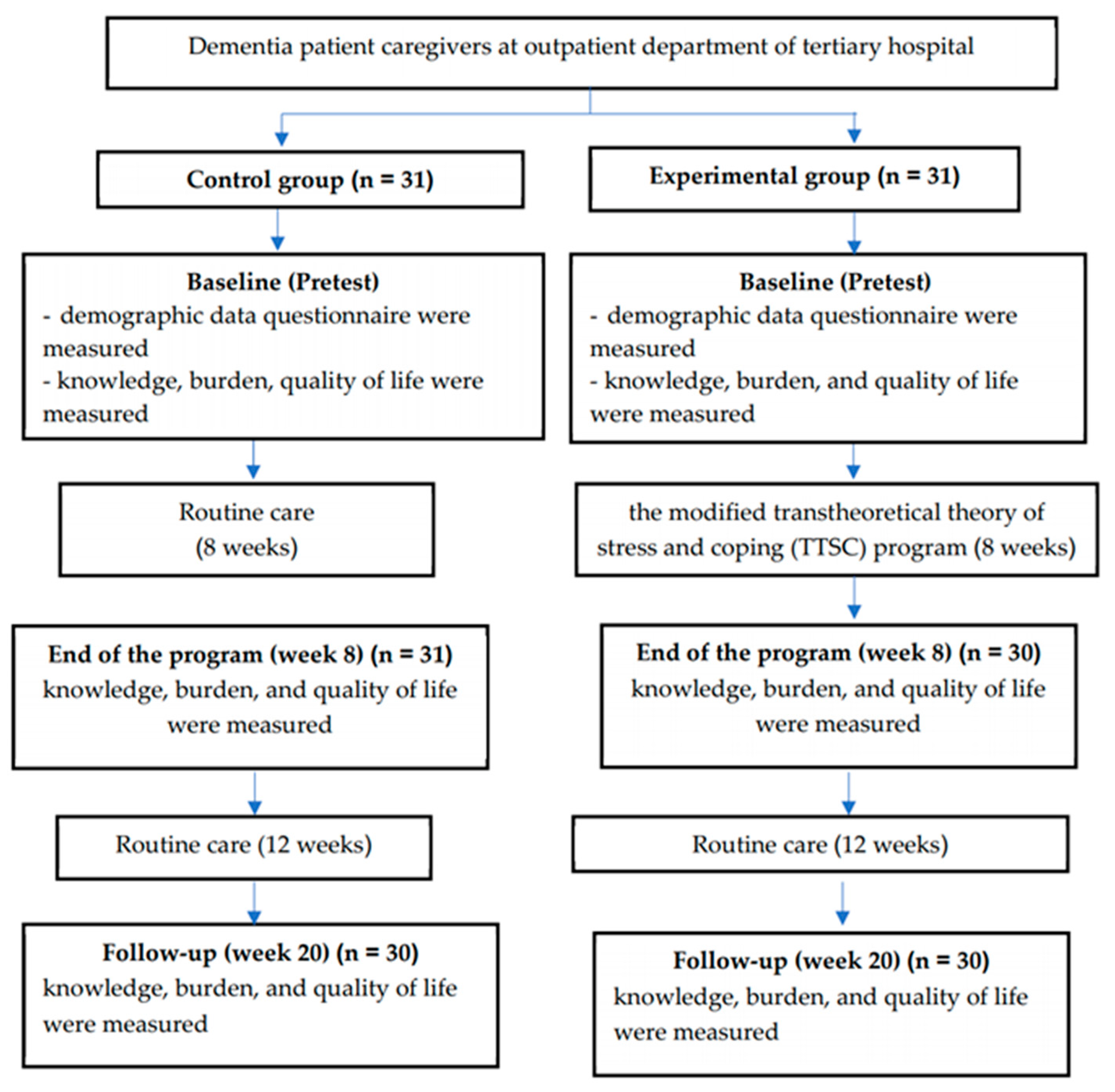
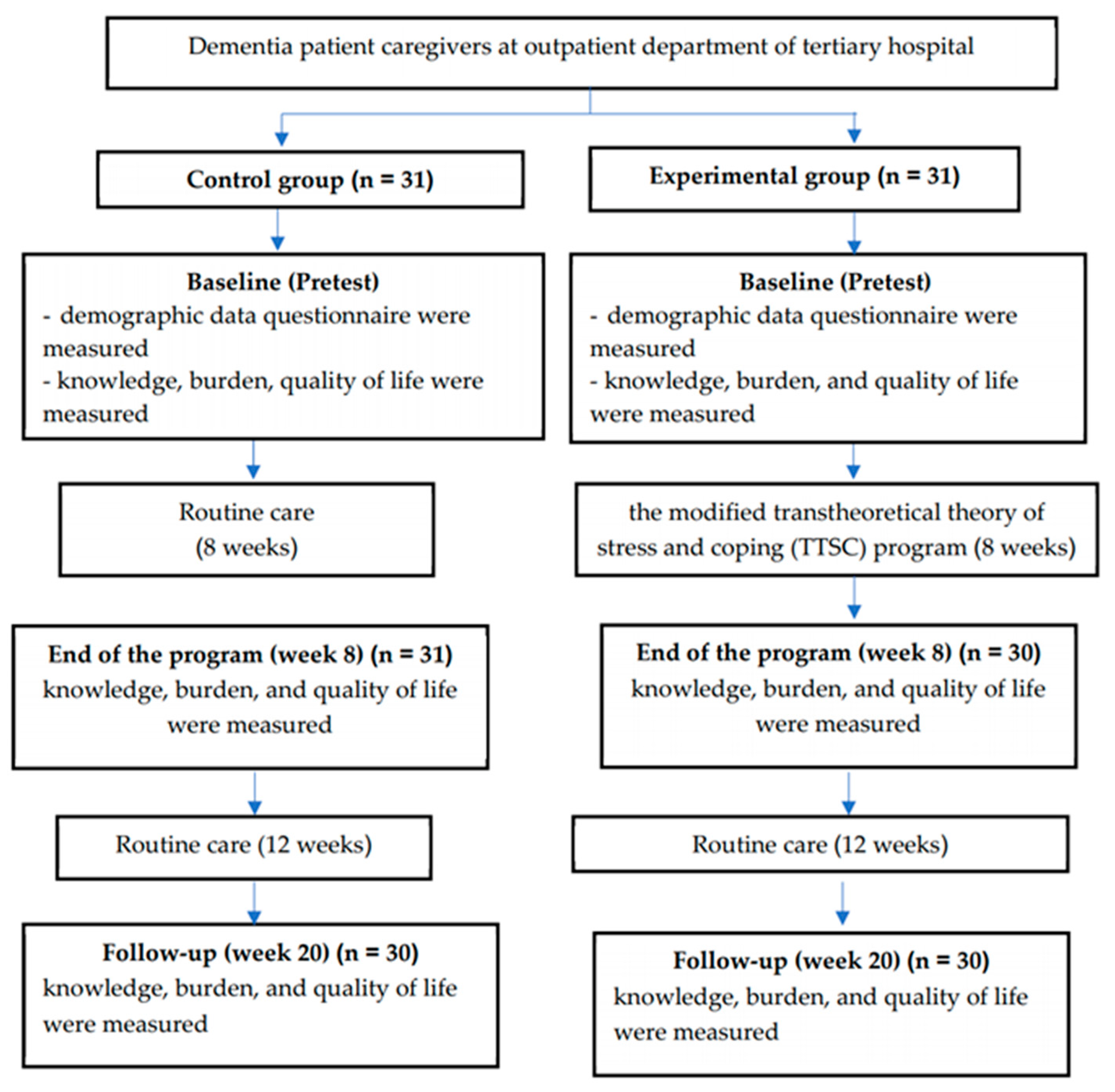
2.1. Study Design
2.2. Study Population and Sample Size
2.3. Intervention
2.4. Instruments
2.5. Data Collection
2.6. Data Analysis
3. Results
Sociodemographic and Characteristic Variables
4. Discussion
Strengths, Limitations, and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ray, S.; Davidson, S. Dementia and Congitive Decline: A Review of the Evidence. 2014. Available online: https://www.ageuk.org.uk/globalassets/age-uk/documents/reports-and-publications/reports-and-briefings/health--wellbeing/rb_oct14_cognitive_decline_and_dementia_evidence_review_age_uk.pdf (accessed on 10 January 2018).
- Wichai, A. Thailand National Health and Examination Survey 2014; Health Systems Research Institute: Nonthaburi, Thailand, 2016. [Google Scholar]
- World Health Organization. Dementia: A Public Health Priority; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Vaingankar, J.A.; Chong, S.A.; Abdin, E.; Picco, L.; Jeyagurunathan, A.; Zhang, Y.; Sambasivam, R.; Chua, B.Y.; Ng, L.L.; Prince, M.; et al. Care participation and burden among informal caregivers of older adults with care needs and associations with dementia. Int. Psychogeriatr. 2016, 28, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, B.; Harary, E.; Kurzman, R.; Mould-Quevedo, J.F.; Pan, S.; Yang, J.; Qiao, J. Clinical Characterization and the Caregiver Burden of Dementia in China. Value Health Reg. Issues 2013, 2, 118–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tulek, Z.; Baykal, D.; Erturk, S.; Bilgic, B.; Hanagasi, H.; Gurvit, I.H. Caregiver Burden, Quality of Life and Related Factors in Family Caregivers of Dementia Patients in Turkey. Issues Ment. Health Nurs. 2020, 41, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Andreakou, M.I.; Papadopoulos, A.A.; Panagiotakos, D.B.; Niakas, D. Assessment of Health-Related Quality of Life for Caregivers of Alzheimer’s Disease Patients. Int. J. Alzheimers Dis. 2016, 2016, 9213968. [Google Scholar] [CrossRef] [Green Version]
- Mekawichai, P.; Saetang, S. Caregiver Burden among Thai Dementia Patients’ Caregivers. J. Psychiatr. Assoc. Thail. 2013, 58, 101–110. [Google Scholar]
- Rosdinom, R.; Zarina, M.Z.N.; Zanariah, M.S.; Marhani, M.; Suzaily, W. Behavioural and psychological symptoms of dementia, cognitive impairment and caregiver burden in patients with dementia. Prev. Med. 2013, 57, S67–S69. [Google Scholar] [CrossRef]
- Innes, A.; Morgan, D.; Kostineuk, J. Dementia care in rural and remote settings: A systematic review of informal/family caregiving. Maturitas 2011, 68, 34–46. [Google Scholar] [CrossRef]
- Schindler, M.; Engel, S.; Rupprecht, R. The Impact of Perceived Knowledge of Dementia on Caregiver Burden. GeroPsych J. Gerontopsychol. Geriatr. Psychiatr. 2012, 25, 127. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Yamada, K.; Iseki, M.; Karasawa, Y.; Murakami, Y.; Enomoto, T.; Kikuchi, N.; Chiba, S.; Hara, A.; Yamaguchi, K.; et al. Insomnia and caregiver burden in chronic pain patients: A cross-sectional clinical study. PLoS ONE 2020, 15, e0230933. [Google Scholar] [CrossRef]
- Alfakhri, A.S.; Alshudukhi, A.W.; Alqahtani, A.A.; Alhumaid, A.M.; Alhathlol, O.A.; Almojali, A.I.; Alotaibi, M.A.; Alaqeel, M.K. Depression among Caregivers of Patients with Dementia. Inquiry 2018, 55, 46958017750432. [Google Scholar] [CrossRef] [Green Version]
- Sittironnarit, G.; Emprasertsuk, W.; Wannasewok, K. Quality of life and subjective burden of primary dementia caregivers in Bangkok, Thailand. Asian J. Psychiatr. 2020, 48, 101913. [Google Scholar] [CrossRef]
- Srivastava, G.; Tripathi, R.; Tiwari, S.; Singh, B.; Tripathi, S. Caregiver burden and quality of life of key caregivers of patients with dementia. Indian J. Psychol. Med. 2016, 38, 133–136. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing: New York, NY, USA, 1984. [Google Scholar]
- Muangpaisan, W.; Praditsuwan, R.; Assanasen, J.; Srinonprasert, V.; Assantachai, P.; Intalapaporn, S.; Chatthanawaree, W.; Dajpratham, P.; Kuptniratsaikul, V.; Pisansalakij, D. Caregiver Burden and Needs of Dementia Caregivers in Thailand: A Cross-Sectional Study. J. Med. Assoc. Thail. 2010, 93, 601–607. [Google Scholar]
- Huis in het Veld, J.G.; Verkaik, R.; Mistiaen, P.; van Meijel, B.; Francke, A.L. The effectiveness of interventions in supporting self-management of informal caregivers of people with dementia; a systematic meta review. BMC Geriatr. 2015, 15, 147. [Google Scholar] [CrossRef] [Green Version]
- Whitlatch, C.J.; Orsulic-Jeras, S. Meeting the Informational, Educational, and Psychosocial Support Needs of Persons Living with Dementia and Their Family Caregivers. Gerontologist 2018, 58, S58–S73. [Google Scholar] [CrossRef]
- Department of Older Persons. Elderly Statistics, Thailand. Available online: http://www.dop.go.th/download/knowledge/th1533055363-125_1.pdf (accessed on 17 January 2018).
- Department of Highways. DOH Travel. Available online: http://www.doh.go.th/content/page/page/8076 (accessed on 17 January 2018).
- Thasana, P. Community Context under the Semi-Urban, Semi-Rural Society. Far East. Univ. Acad. J. 2015, 9, 7–15. [Google Scholar]
- Office of the Education Council. Education Statistic; Office of the Education Council: Bangkok, Thailand, 2020; Available online: http://www.onec.go.th/index.php/page/category/CAT0000058 (accessed on 10 February 2020).
- National Statistical Office. Average Monthly Income Per Household: 1998–2015. Available online: http://www.nso.go.th/sites/2014 (accessed on 20 August 2016).
- Yimyam, U.; Yamsakul, N. A survey of Dementia in the elderly in Damnoensaduak district, Ratchaburi providence. Prim. Health Care Div. J. 2013, 9, 29–37. [Google Scholar]
- Thailand Data Journalism Network. TDJ Dementia in Thailand. Available online: http://www.tja.or.th/media-law/5199--1 (accessed on 23 September 2019).
- Tremont, G.; Davis, J.D.; Bishop, D.S.; Fortinsky, R.H. Telephone-Delivered Psychosocial Intervention Reduces Burden in Dementia Caregivers. Dementia 2008, 7, 503–520. [Google Scholar] [CrossRef] [Green Version]
- Toye, C.; Lester, L.; Popescu, A.; McInerney, F.; Andrews, S.; Robinson, A.L. Dementia Knowledge Assessment Tool Version Two: Development of a tool to inform preparation for care planning and delivery in families and care staff. Dementia 2014, 13, 248–256. [Google Scholar] [CrossRef] [Green Version]
- Toonsiri, C.; Sunsern, R.; Lawang, W. Development of the Burden Interview for Caregivers of Patients with Chronic Illness. J. Nurs. Educ. 2011, 4, 62–75. [Google Scholar]
- Mahuntnirunkul, S.; Tantipiwattanasakool, W.; Poompisanchai, V.; Wongsuwan, K.; Prommanajirangkool, R. Comparison of the WHOQOL-100 and the WHOQOL-BREF (26 items). J. Ment. Health Thail. 1998, 5, 4–15. [Google Scholar]
- Tan, Z.S.; Jennings, L.; Ramirez, K.; Kofman, Y.B.; Ercoli, L. Caregiver Knowledge and Perceived Competence Following an Intensive Dementia Caregiving Training Course. Alzheimers Dement. 2016, 12, P266. [Google Scholar] [CrossRef]
- Tan, Z.S.; Soh, M.; Knott, A.; Ramirez, K.; Ercoli, L.; Caceres, N.; Yuan, S.; Long, M.; Jennings, L.A. Impact of an Intensive Dementia Caregiver Training Model on Knowledge and Self-Competence: The Improving Caregiving for Dementia Program. J. Am. Geriatr. Soc. 2019, 67, 1306. [Google Scholar] [CrossRef]
- Shata, Z.N.; Amin, M.R.; El-Kady, H.M.; Abu-Nazel, M.W. Efficacy of a multi-component psychosocial intervention program for caregivers of persons living with neurocognitive disorders, Alexandria, Egypt: A randomized controlled trial. Avicenna J. Med. 2017, 7, 54–63. [Google Scholar] [CrossRef]
- Kwok, T.; Lam, L.; Chung, J. Case management to improve quality of life of older people with early dementia and to reduce caregiver burden. Hong Kong Med. J. 2012, 18 (Suppl. 6), 4–6. [Google Scholar]
- Arango-Lasprilla, J.C.; Panyavin, I.; Merchán, E.J.; Perrin, P.B.; Arroyo-Anlló, E.M.; Snipes, D.J.; Arabia, J. Evaluation of a group cognitive-behavioral dementia caregiver intervention in Latin America. Am. J. Alzheimers Dis. Other Dement. 2014, 29, 548–555. [Google Scholar] [CrossRef]
- Ransmayr, G.; Hermann, P.; Sallinger, K.; Benke, T.; Seiler, S.; Dal-Bianco, P.; Marksteiner, J.; Defrancesco, M.; Sanin, G.; Struhal, W.; et al. Caregiving and Caregiver Burden in Dementia Home Care: Results from the Prospective Dementia Registry (PRODEM) of the Austrian Alzheimer Society. J. Alzheimers Dis. 2018, 63, 103–114. [Google Scholar] [CrossRef]
- Cheng, S.-T. Dementia Caregiver Burden: A Research Update and Critical Analysis. Curr. Psychiatr. Rep. 2017, 19, 64. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-M.; Huang, M.-F.; Yeh, Y.-C.; Huang, W.-H.; Chen, C.-S. Effectiveness of coping strategies intervention on caregiver burden among caregivers of elderly patients with dementia. Psychogeriatrics 2015, 15, 20–25. [Google Scholar] [CrossRef]
- Kuo, L.M.; Huang, H.L.; Liang, J.; Kwok, Y.T.; Hsu, W.C.; Su, P.L.; Shyu, Y.L. A randomized controlled trial of a home-based training programme to decrease depression in family caregivers of persons with dementia. J. Adv. Nurs. 2017, 73, 585–598. [Google Scholar] [CrossRef]
- Ying, J.; Wang, Y.; Zhang, M.; Wang, S.; Shi, Y.; Li, H.; Li, Y.; Xing, Z.; Sun, J. Effect of multicomponent interventions on competence of family caregivers of people with dementia: A systematic review. J. Clin. Nurs. 2018, 27, 1744–1758. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Week | Objective | Activities and Content | Evaluate |
|---|---|---|---|
| 1 | To share additional requirements, problems, and methods to solve the problems | Group health education at dementia clinic (30–40 min) (researcher and research assistants per 5–6 participants per group) Step 1: Introduction and building confidence: The researcher introduces the details of the program and builds caregivers’ confidence that their problems will be heard and handled. Caregivers cannot avoid the problems; however, we can handle the problems. Step 2: Caregivers share about the caring experience.
| Sharing additional requirements, caregiver’s problems, and methods to solve the problems |
| 2 | To explore self-assessment and home arrangement | Home visit (45–90 min) Major concept: Stress
The researcher helps the caregivers overcome stress by using coping strategies.
|
|
| 3–7 | To re-explore self-assessment and support a positive appraisalTo help the caregiver overcome stress by using coping strategies | Telephone follow-up (once a week) (15–30 min) The caregivers receive telephone contact once a week. This telephone tracking focuses on providing education that is tailored to the specific needs of the caregiver. Moreover, the intervention guides the dementia caregivers to use specific coping strategies based on the transtheoretical model. Major concept: Stress
The researcher helps the caregivers overcome stress by using coping strategies.
|
|
| 8 | To re-explore self-assessment and support positive appraisal To help the caregivers overcome stress by continuing to develop and utilize adaptive coping strategies To inform caregivers regarding termination of the intervention | Home visit (45–90 min) Major concept: Stress
|
|
| 9–20 | Reappraisal | none |
|
| Characteristics | Experimental Group (n = 31) | Control Group (n = 31) | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Gender | |||||
| Male | 8 | 25.8 | 4 | 12.9 | |
| Female | 23 | 74.2 | 27 | 87.1 | 0.19 a |
| Age | |||||
| 20–40 years | 2 | 6.5 | 3 | 9.7 | |
| 41–60 years | 24 | 77.4 | 24 | 77.4 | |
| ≥60 years | 5 | 16.1 | 4 | 12.9 | 0.86 b |
| Marital status | |||||
| Single | 11 | 35.5 | 7 | 22.6 | |
| Married | 17 | 54.8 | 17 | 54.8 | |
| Divorced/Separated/Widowed | 3 | 9.7 | 7 | 22.6 | 0.41 a |
| Relationship to care recipient | |||||
| Spouse | 5 | 16.1 | 5 | 16.1 | |
| Son (blood relatives) | 6 | 19.4 | 3 | 9.7 | |
| Daughter (blood relatives) | 15 | 48.4 | 18 | 58.1 | |
| Relative | 3 | 9.7 | 2 | 6.5 | |
| Friend/Adopted child/Neighbor | 2 | 6.5 | 3 | 9.7 | 0.87 b |
| Education level | |||||
| Primary school | 12 | 38.7 | 8 | 25.8 | |
| High school | 11 | 35.5 | 15 | 48.4 | |
| Bachelor’s degree | 8 | 25.8 | 8 | 25.8 | 0.49 a |
| Employment Status | |||||
| Full time | 17 | 54.8 | 17 | 54.8 | |
| Part time | 3 | 9.7 | 4 | 12.9 | |
| Not Employed/Retired | 11 | 35.5 | 10 | 32.3 | 0.91 b |
| Length of time as a caregiver | |||||
| 0–3 years | 13 | 41.9 | 6 | 19.4 | |
| 3.1–6 years | 10 | 32.3 | 10 | 32.3 | |
| 6.1–9 years | 5 | 16.1 | 11 | 35.5 | |
| More than 9 years | 3 | 9.7 | 4 | 12.9 | 0.17 b |
| Time for caring (hour/day) | |||||
| 6–12 h | 29 | 93.6 | 31 | 100 | |
| More than 12 h | 2 | 6.4 | 0 | 0 | 0.26 b |
| Clinical Dementia Rating (CDR) c | |||||
| Mild dementia | 8 | 25.8 | 8 | 25.8 | |
| Moderate dementia | 18 | 58.1 | 17 | 54.8 | |
| Severe dementia | 5 | 16.1 | 6 | 19.4 | 0.94 a |
| Outcome | Time | Experimental Group | Control Group | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Caregiver burden | Baseline | 45.67 | 12.0 | 47.33 | 13.52 |
| Week 8 | 43.27 | 10.75 | 49.37 | 11.84 | |
| Week 20 | 44.00 | 9.99 | 50.07 | 11.44 | |
| Outcome | Baseline | Week 8 | Week 20 | Test Stat | df | p | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| Knowledge | |||||||||
| Experimental group | 10.23 | 1.99 | 13.63 | 1.65 | 13.77 | 1.63 | 55.802 | 2 | <0.05 * |
| Control group | 10.35 | 1.89 | 10.97 | 2.06 | 11.13 | 2.11 | 17.148 | 2 | <0.05 * |
| Quality of life | |||||||||
| Experimental group | 85.03 | 9.80 | 88.13 | 8.83 | 87.07 | 8.82 | 43.130 | 2 | <0.05 * |
| Control group | 86.52 | 9.21 | 79.65 | 7.84 | 77.87 | 6.66 | 46.308 | 2 | <0.05 * |
| Outcome | Group | Time (Within Group) | Test Stat | Sd. Error | Sd. Test Stat | p-Value |
|---|---|---|---|---|---|---|
| Knowledge | Intervention | Baseline–Week 8 | −1.383 | 0.258 | −5.358 | <0.05 * |
| Baseline–Week 20 | −1.517 | 0.258 | −5.874 | <0.05 * | ||
| Week 8–Week 20 | −0.133 | 0.258 | −0.516 | 1.000 | ||
| Control | Baseline–Week 8 | −0.583 | 0.258 | −2.259 | 0.072 | |
| Baseline–Week 20 | −0.717 | 0.258 | −2.776 | 0.017 * | ||
| Week 8–Week 20 | −0.133 | 0.258 | −0.516 | 1.000 | ||
| Quality of life | Intervention | Baseline–Week 8 | −1.467 | 0.258 | −5.680 | <0.05 * |
| Baseline–Week 20 | −0.933 | 0.258 | −3.615 | <0.05 * | ||
| Week 8–Week 20 | 0.533 | 0.258 | 2.066 | 0.117 | ||
| Control | Baseline–Week 8 | −0.933 | 0.258 | 3.615 | 0.001 * | |
| Baseline–Week 20 | 1.517 | 0.258 | 5.874 | <0.05 * | ||
| Week 8–Week 20 | 0.583 | 0.258 | 2.259 | 0.072 |
| Outcome | Time | Experimental Group | Control Group | Mann-Whitney U | df | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||||
| Knowledge | Baseline | 10.23 | 1.99 | 10.35 | 1.89 | 458.00 | 1 | 0.748 |
| Week 8 | 13.63 | 1.65 | 10.97 | 2.06 | 140.00 | 1 | <0.05 * | |
| Week 20 | 13.77 | 1.63 | 11.13 | 2.11 | 146.50 | 1 | <0.05 * | |
| Quality of life | Baseline | 85.03 | 9.80 | 86.52 | 9.21 | 427.00 | 1 | 0.451 |
| Week 8 | 88.13 | 8.83 | 79.65 | 7.84 | 218.50 | 1 | <0.05 * | |
| Week 20 | 87.07 | 8.82 | 77.87 | 6.66 | 171.50 | 1 | <0.05 * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magteppong, W.; Yamarat, K. The Effects of the Modified Transtheoretical Theory of Stress and Coping (TTSC) Program on Dementia Caregivers’ Knowledge, Burden, and Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 13231. https://doi.org/10.3390/ijerph182413231
Magteppong W, Yamarat K. The Effects of the Modified Transtheoretical Theory of Stress and Coping (TTSC) Program on Dementia Caregivers’ Knowledge, Burden, and Quality of Life. International Journal of Environmental Research and Public Health. 2021; 18(24):13231. https://doi.org/10.3390/ijerph182413231
Chicago/Turabian StyleMagteppong, Worarat, and Khemika Yamarat. 2021. "The Effects of the Modified Transtheoretical Theory of Stress and Coping (TTSC) Program on Dementia Caregivers’ Knowledge, Burden, and Quality of Life" International Journal of Environmental Research and Public Health 18, no. 24: 13231. https://doi.org/10.3390/ijerph182413231
APA StyleMagteppong, W., & Yamarat, K. (2021). The Effects of the Modified Transtheoretical Theory of Stress and Coping (TTSC) Program on Dementia Caregivers’ Knowledge, Burden, and Quality of Life. International Journal of Environmental Research and Public Health, 18(24), 13231. https://doi.org/10.3390/ijerph182413231