
Therapeutic Benefits of Balneotherapy on Quality of Life of Patients with Rheumatoid Arthritis: A Systematic Review


 ,
,  ,
, 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Elegibility
2.2. Outcomes
2.3. Information Sources
2.4. Search Strategy
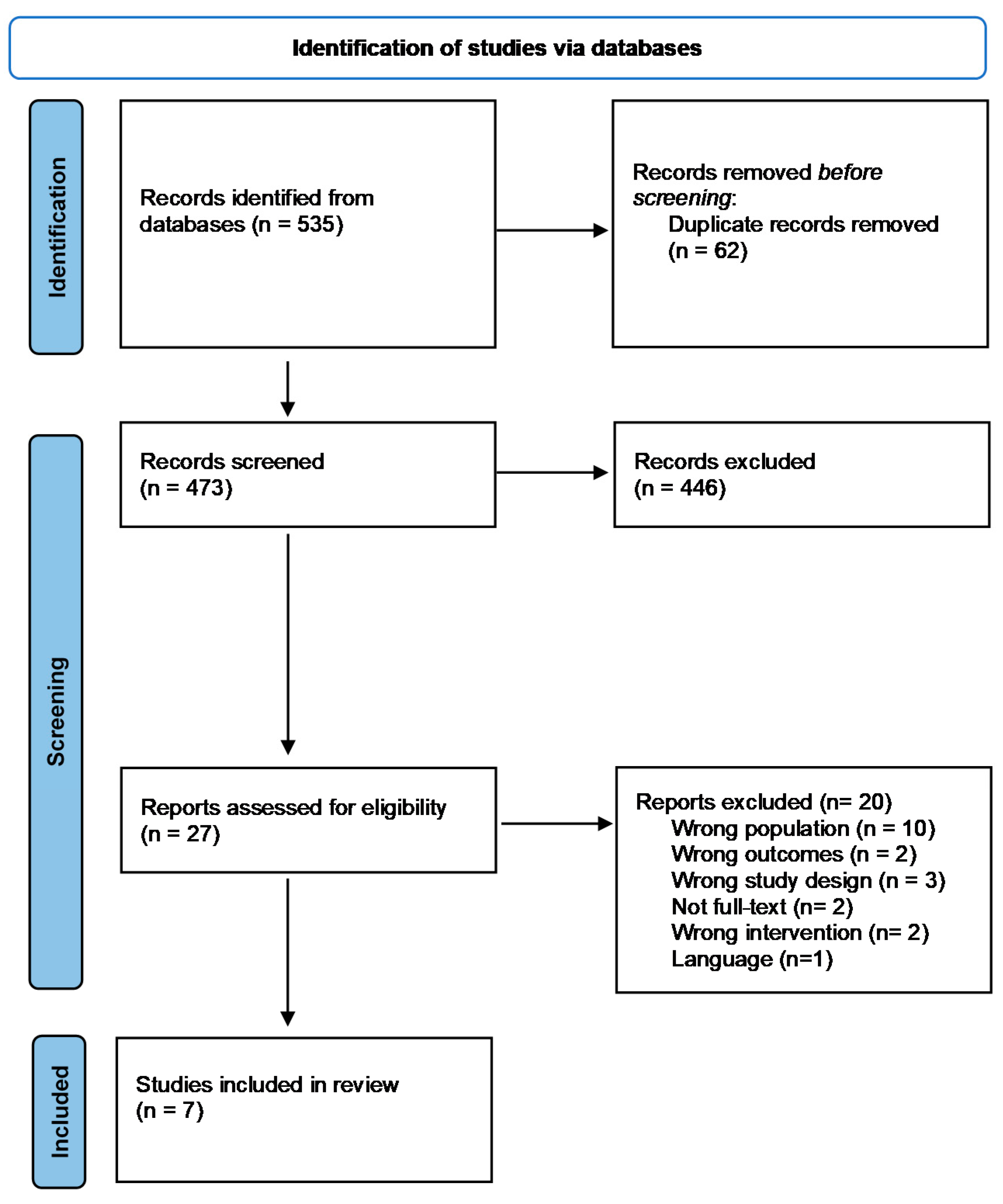
2.5. Selection Process
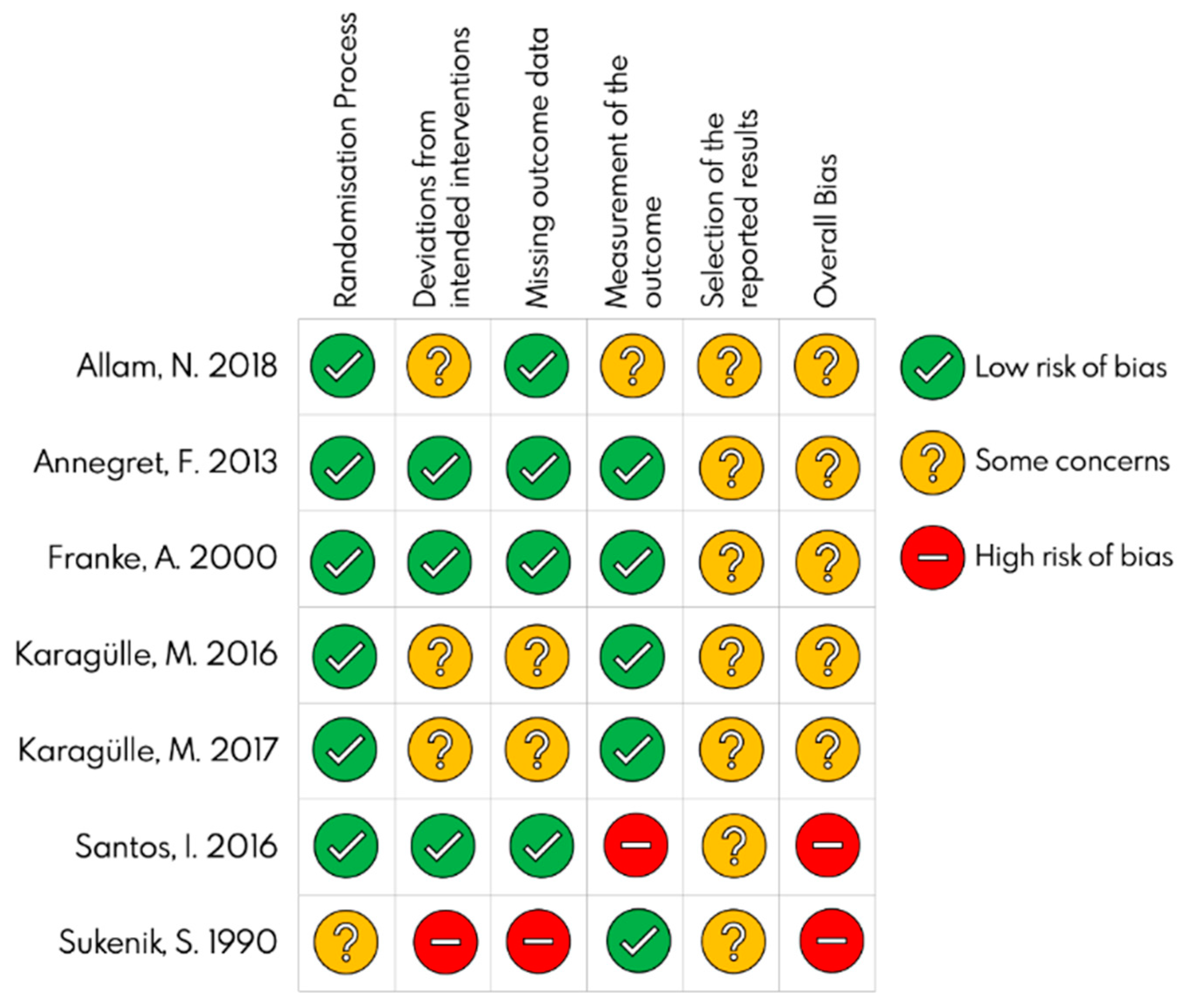
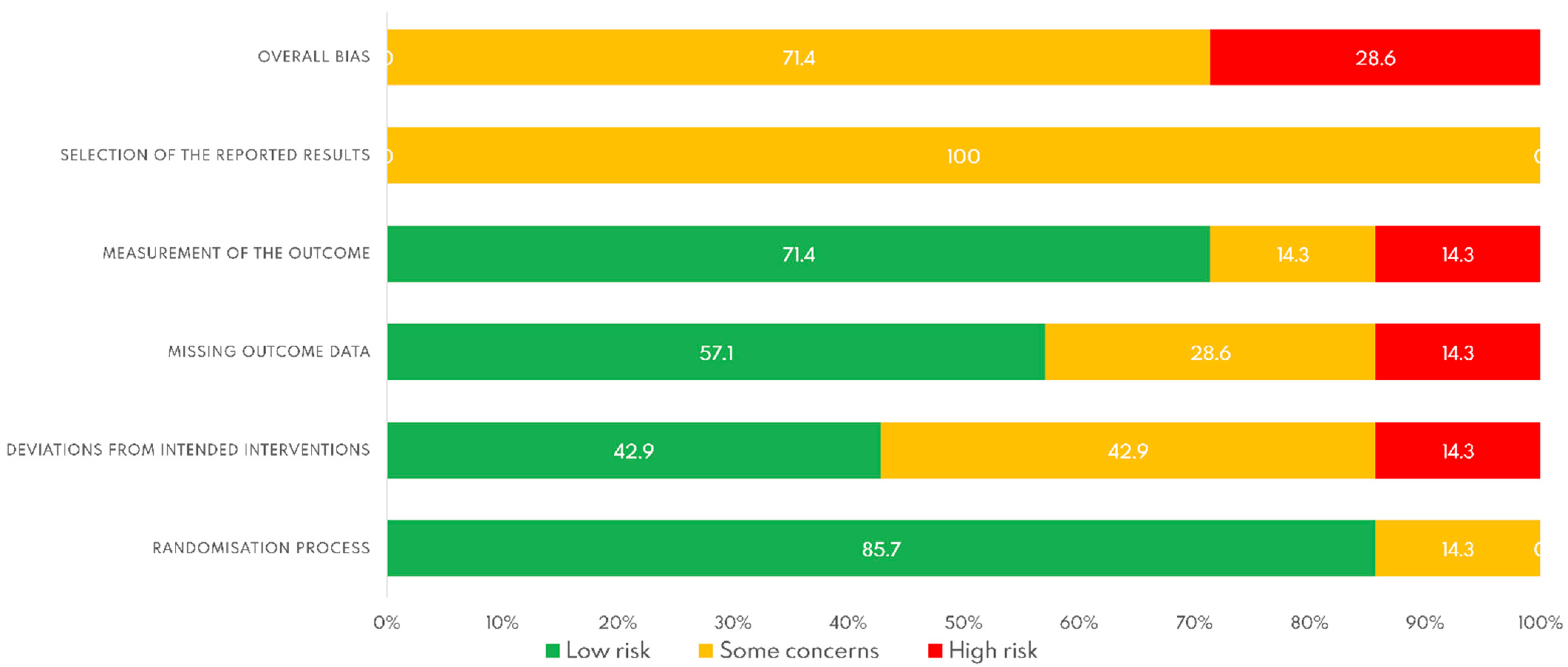
2.6. Risk of Bias
3. Results
3.1. Descriptive Study
3.2. Interventions
3.3. Outcome
3.4. Risk of Bias
4. Discussion
4.1. Limitations and Strenghts
4.2. Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Search Strategy
Appendix A.1. Pubmed
Appendix A.2. Scopus
Appendix A.3. Web of Sciencie
Appendix A.4. Cochrane Library
References
- Almutairi, K.; Nossent, J.; Preen, D.; Keen, H.; Inderjeeth, C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatol. Int. 2021, 41, 863–877. [Google Scholar] [CrossRef] [PubMed]
- Safiri, S.; Kolahi, A.-A.; Cross, M.; Hill, C.; Smith, E.; Carson-Chahhoud, K.; Mansournia, M.A.; Almasi-Hashiani, A.; Ashrafi-Asgarabad, A.; Kaufman, J.; et al. Prevalence, Deaths, and Disability-Adjusted Life Years Due to Musculoskeletal Disorders for 195 Countries and Territories 1990–2017. Arthritis Rheumatol. 2021, 73, 702–714. [Google Scholar] [CrossRef] [PubMed]
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. ERD Work. Pap. Ser. 2002, 81, 646–656. [Google Scholar]
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Conforti, A.; Di Cola, I.; Pavlych, V.; Ruscitti, P.; Berardicurti, O.; Ursini, F.; Giacomelli, R.; Cipriani, P. Beyond the joints, the extra-articular manifestations in rheumatoid arthritis. Autoimmun. Rev. 2021, 20, 102735. [Google Scholar] [CrossRef]
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Prim. 2018, 4, 1800. [Google Scholar] [CrossRef]
- Bullock, J.; Rizvi, S.A.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid arthritis: A brief overview of the treatment. Med. Princ. Pract. 2019, 27, 501–507. [Google Scholar] [CrossRef]
- Stanmore, E.K.; Oldham, J.; Skelton, D.A.; O’Neill, T.; Pilling, M.; Campbell, A.J.; Todd, C. Fall incidence and outcomes of falls in a prospective study of adults with rheumatoid arthritis. Arthritis Care Res. 2013, 65, 737–744. [Google Scholar] [CrossRef]
- Rosa-Gonçalves, D.; Bernardes, M.; Costa, L. Quality of life and functional capacity in patients with rheumatoid arthritis—Cross-sectional study. Reumatol. Clin. 2018, 14, 360–366. [Google Scholar] [CrossRef]
- Morer, C.; Roques, C.-F.; Françon, A.; Forestier, R.; Maraver, F. The role of mineral elements and other chemical compounds used in balneology: Data from double-blind randomized clinical trials. Int. J. Biometeorol. 2017, 61, 2159–2173. [Google Scholar] [CrossRef]
- Király, M.; Kővári, E.; Hodosi, K.; Bálint, P.V.; Bender, T. The effects of Tiszasüly and Kolop mud pack therapy on knee osteoarthritis: A double-blind, randomised, non-inferiority controlled study. Int. J. Biometeorol. 2020, 64, 943–950. [Google Scholar] [CrossRef]
- Brosseau, L.; Robinson, V.; Léonard, G.; Casimiro, L.; Pelland, L.; Wells, G.; Tugwell, P. Efficacy of Balneotherapy for Rheumatoid Arthritis: A Meta-analysis. Phys. Ther. Rev. 2002, 7, 67–87. [Google Scholar] [CrossRef]
- Fioravanti, A.; Manica, P.; Bortolotti, R.; Cevenini, G.; Tenti, S.; Paolazzi, G. Is balneotherapy effective for fibromyalgia? Results from a 6-month double-blind randomized clinical trial. Clin. Rheumatol. 2018, 37, 2203–2212. [Google Scholar] [CrossRef]
- Gutenbrunner, C.; Bender, T.; Cantista, P.; Karagülle, Z. A proposal for a worldwide definition of health resort medicine, balneology, medical hydrology and climatology. Int. J. Biometeorol. 2010, 54, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Verhagen, A.P.; Bierma-Zeinstra, S.M.; Boers, M.; Cardoso, J.R.; Lambeck, J.; de Bie, R.; de Vet, H.C. Balneotherapy (or spa therapy) for rheumatoid arthritis. Cochrane Database Syst. Rev. 2015, 2015, CD00051. [Google Scholar] [CrossRef]
- Fioravanti, A.; Cantarini, L.; Guidelli, G.M.; Galeazzi, M. Mechanisms of action of spa therapies in rheumatic diseases: What scientific evidence is there? Rheumatol. Int. 2011, 31, 1–8. [Google Scholar] [CrossRef]
- Falagas, M.E.; Zarkadoulia, E.; Rafailidis, P.I. The therapeutic effect of balneotherapy: Evaluation of the evidence from randomised controlled trials. Int. J. Clin. Pract. 2009, 63, 1068–1084. [Google Scholar] [CrossRef]
- Verhagen, A.P.; Bierma-Zeinstra, S.; Lambeck, J.; Cardoso, J.R.; De Bie, R.; Boers, M.; De Vet, H.C.W. Balneotherapy for osteoarthritis. A cochrane review. J. Rheumatol. 2008, 35, 1118–1123. [Google Scholar] [PubMed]
- Santos, I.; Cantista, P.; Vasconcelos, C. Balneotherapy in rheumatoid arthritis-a systematic review. Int. J. Biometeorol. 2016, 60, 1287–1301. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Estarli, M.; Barrera, E.S.A.; et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev. Esp. Nutr. Humana y Diet. 2016, 20, 148–160. [Google Scholar] [CrossRef]
- Bruce, B.; Fries, J.F. The Stanford Health Assessment Questionnaire: Dimensions and practical applications. Health Qual. Life Outcomes 2003, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.; Bird, H.A.; Lawton, C.W.; Wright, V. The arthritis impact measurement scales: An anglicized version to assess the outcome of British patients with rheumatoid arthritis. Rheumatology 1990, 29, 193–196. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Allam, N.M.; Koura, G.M.R.; Alrawaili, S.M.; Hamada, H.A.; Khater, H.A.; Balbaa, A.A. The effect of siwan therapy in management of patients with rheumatoid arthritis: A single blind randomized controlled trial. Biomed. Res. 2018, 29, 1400–1406. [Google Scholar] [CrossRef]
- Annegret, F.; Thomas, F. Long-term benefits of radon spa therapy in rheumatic diseases: Results of the randomised, multi-centre IMuRa trial. Rheumatol. Int. 2013, 33, 2839–2850. [Google Scholar] [CrossRef] [PubMed]
- Franke, A.; Reiner, L.; Pratzel, H.G.; Franke, T.; Resch, K.L. Long-term efficacy of radon spa therapy in rheumatoid arthrirtis—A randomized, sham-controlled study and follow-up. Rheumatology 2000, 39, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Karagülle, M.; Kardeş, S.; Karagülle, O.; Dişçi, R.; Avcı, A.; Durak, İ.; Karagülle, M.Z. Effect of spa therapy with saline balneotherapy on oxidant/antioxidant status in patients with rheumatoid arthritis: A single-blind randomized controlled trial. Int. J. Biometeorol. 2017, 61, 169–180. [Google Scholar] [CrossRef]
- Karagülle, M.; Kardeş, S.; Dişçi, R.; Karagülle, M.Z. Spa therapy adjunct to pharmacotherapy is beneficial in rheumatoid arthritis: A crossover randomized controlled trial. Int. J. Biometeorol. 2018, 62, 195–205. [Google Scholar] [CrossRef]
- Santos, I.; Cantista, P.; Vasconcelos, C.; Amado, J. Balneotherapy and rheumatoid arthritis: A randomized control trial. Isr. Med. Assoc. J. 2016, 18, 474–478. [Google Scholar]
- Sukenik, S.; Buskila, D.; Neumann, L.; Kleiner-Baumgarten, A.; Zimlichman, S.; Horowitz, J. Sulphur bath and mud pack treatment for rheumatoid arthritis at the Dead Sea area. Ann. Rheum. Dis. 1990, 49, 99–102. [Google Scholar] [CrossRef]
- Kamioka, H.; Tsutani, K.; Okuizumi, H.; Mutoh, Y.; Ohta, M.; Handa, S.; Okada, S.; Kitayuguchi, J.; Kamada, M.; Shiozawa, N.; et al. Effectiveness of aquatic exercise and balneotherapy: A summary of systematic reviews based on randomized controlled trials of water immersion therapies. J. Epidemiol. 2010, 20, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, A.; Cheleschi, S.; Tent, S. Mechanisms of Action of Balneotherapy in Rheumatic Diseases: The Scientific Evidence. Cad. Naturologia e Ter. Complement. 2014, 3, 63. [Google Scholar] [CrossRef][Green Version]
- Ortega, E.; Gálvez, I.; Hinchado, M.D.; Guerrero, J.; Martín-Cordero, L.; Torres-Piles, S. Anti-inflammatory effect as a mechanism of effectiveness underlying the clinical benefits of pelotherapy in osteoarthritis patients: Regulation of the altered inflammatory and stress feedback response. Int. J. Biometeorol. 2017, 61, 1777–1785. [Google Scholar] [CrossRef] [PubMed]
- Kuciel-Lewandowska, J.; Kasperczak, M.; Paprocka-Borowicz, M. Assessment of Changes in the Hemoglobin Level under the Influence of Comprehensive Spa Therapy Using Therapeutic Radon-Sulfur Waters and Its Correlation with Free Radical Reactions. Evid. Based. Complement. Alternat. Med. 2020, 2020, 4637129. [Google Scholar] [CrossRef] [PubMed]
- Cucu, A.; Shreder, K.; Kraft, D.; Rühle, P.F.; Klein, G.; Thiel, G.; Frey, B.; Gaipl, U.S.; Fournier, C. Decrease of Markers Related to Bone Erosion in Serum of Patients with Musculoskeletal Disorders after Serial Low-Dose Radon Spa Therapy. Front. Immunol. 2017, 8, 882. [Google Scholar] [CrossRef]
- Suter, G.W. Review papers are important and worth writing. Environ. Toxicol. Chem. 2013, 32, 1929–1930. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Desing | Participant | Intervention | Scales | Secondary Outcomes | Results |
|---|---|---|---|---|---|---|
| Allam, N.M., et al. [24] 2018 | RCT | N = 30 IG; n = 15 CG; n = 15 | IG: Siwan therapy 7 days of hot sand baths for 20 min and massage with olive oil CG: standard physiotherapy treatment | HAQ | Pain (VAS) | The scale score were decreased significantly compared with baseline in spa group but not in control group |
| Annegret, F., et al. [25] 2013 | RCT | N = 98 IG; n = 48 CG; n = 50 | 3–4 weeks of intervetion IG: 12 total radon baths every 2 or 3 days in spedificil locations for 20 min a day CG: 12 tap water baths with artificial CO2 for 20 min | HAQ | Pain (VAS) SF-12 | There is a significant improvement in the HAQ scores of the intervetion group versus the control group |
| Annegret, F., et al. [26] 2000 | RCT | N = 60 IG; n = 30 CG; n = 30 | 4 weeks of intervetion IG: 15 total radon baths for 20 min a day CG: 15 baths in tap water baths with artificial CO2 for 20 min | AIMS | Pain (VAS) Keitel funcional test (KFI) | Significant differences were found in terms of the improvement in the result of the AIMS scale in the intervention group at 3 and 6 months of follow-up. |
| Karagülle, M., et al. [27] 2017 | RCT | N = 37 IG; n = 15 CG; n = 22 | 2 weeks of intervetion IG: 12 balneotherapy sessions in mineral water for 20 min a day CG: standard drug treatment | HAQ | Pain (VAS) Disease Activity Score (DAS28) Patient global assessment (VAS) Biochemical analysis | HAQ scores were significantly reduced compared to baseline results in the intervention group, but not in the control group |
| Karagülle, M., et al. [28] 2018 | CRCT | N first period = 15 N second period = 22 | 2 weeks of intervetion IG: 12 balneotherapy sessions in mineral water for 20 min a day CG: standard drug treatment | HAQ | Pain (VAS) Disease Activity Score (DAS28) Patient global assessment (VAS) | A significant difference was found in the intervention group at 3 months; however, there were no significant differences at 6 months |
| Santos, I., et al. [29] 2016 | RCT | N = 44 IG; n = 22 CG; n = 22 | 21 days of intervention IG: two treatments on alternate days. Treatment 1 consisted of sulphur baths of 30 min and underwater exercises. Treatment 2 consisted of sulphur baths of 20 min and underwater jets for 10 min in painful joints CG: standard drug treatment | HAQ | Global health assessment (VAS) Pain (VAS) Quality of life (VAS) Fatigue (VAS) Disease Activity Score (DAS28) | HAQ improved significantly in the intervention group compared to the control group |
| Sukenik, S., et al. [30] 1990 | RCT | N = 40 4 groups of 10 patiens each one | 2 weeks fo intervetion Group 1: daily mud packs in full body for 20 min a day Group 2: daily sulphur baths for 20 min a day Group 3: combination of daily mud packs and daily sulphur baths Group 4: control, without treatment | Patient assessment of disease severity | Morning stiffness Fifteen metre walk time Circunference of proximal interphalangeal joints Activities of daily living | Significant improvements were found in terms of the patient’s perception of the disease in the three treatment groups |
| Author, year | Scales | Baseline Evaluation | Post-Treatment Evaluation | Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Control Group | Intervention Group | Control Group | Intervetion Group | Intragroup | Intergroup | Control Group | Intervention Group | Intragroup | Intergroup | ||
| Allam, N.M., et al. [24] 2018 | HAQ | 1.82 ± 0.52 | 1.75 ± 0.58 | 1.58 ± 0.67 | 0.82 ± 0.50 | p < 0.05 in intervention group | p < 0.05 in favor to intervention group | - | - | - | - |
| Annegret, F., et al. [25] 2013 a | HAQ | 0.95 (0.62) | 0.93 (0.52) | 0.10 (0.29) | 0.08 (0.39) | p < 0.05 in intervention group | p > 0.05 | 3 months = 0.08(0.31) 6 months = 0.07(0.43) 9 months = 0.07(0.34) | 3 months = 0.10 (0.42) 6 months = 0.17(0.37) 9 months = 0.09 (0.45) | p > 0.05 | p < 0.05 |
| Annegret, F., et al. [26] 2000 a | AIMS | 6.60 (1.10) | 6.27 (1.33) | - | - | p > 0.05 | p < 0.05 in favor to intervention group | 3 months = −0.06 (−0.34, 0.23) 6 months = −0.18 (−0.36, 0.20) | 3 months = 0.41 (0.06, 0.75) 6 months = 0.41 (0.06, 0.74) | ||
| Karagülle, M., et al. [27] 2017 | HAQ | 1.43 ± 0.76 | 1.33 ± 0.68 | 2 weeks post tto. 1.23 ± 0.75 | 2 weeks post tto. 0.79 ± 0.64 | p < 0.05 in intervention group | p < 0.05 in favor to intervention group | - | - | ||
| Karagülle, M., et al. [28] 2018 a | HAQ | 0.96 (0.66, 1.99) | 1.40 (0.73, 1.83) | 2 weeks post tto. 1.10 (1.51, 1.76) | 2 weeks post tto. 0.08 (0.33, 1.13) | p < 0.05 in intervention group | p < 0.05 in favor to intervention group | 3 months = 1.00 (0.51, 1.76) 6 months = 1.10 (0.41, 1.55) | 3 months = 0.60 (0.40, 0.98) 6 months = 0.65 (0.38, 1.43) | ||
| Santos, I., et al. [29] 2016 a | HAQ | 1.34 (0.97, 1.7) | 1.50 (1.24, 1.76) | Difference between groups 0.37 (0.09, 0.64) | - | p < 0.05 | Difference between groups at 3 months 0.44 (0.15, 0.72) | p < 0.05 | |||
| Sukenik, S., et al. [30] 1990 b | Patient’s self assessment of the disease | 5.5 | Mud packs 4.1 | Mud packs 6.5 | 6.1 | p < 0.05 in the three treatment groups | 3 months Mud packs 5.7 | 3 months 5.7 | |||
| Sulphur baths 5.0 | Sulphur baths 6.4 | 3 months Sulphur baths 6.3 | |||||||||
| Combination 4.8 | Combination 7.0 | 3 months Combination 5.7 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandez-Gonzalez, M.; Fernandez-Lao, C.; Martin-Martin, L.; Gonzalez-Santos, A.; Lopez-Garzon, M.; Ortiz-Comino, L.; Lozano-Lozano, M. Therapeutic Benefits of Balneotherapy on Quality of Life of Patients with Rheumatoid Arthritis: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 13216. https://doi.org/10.3390/ijerph182413216
Fernandez-Gonzalez M, Fernandez-Lao C, Martin-Martin L, Gonzalez-Santos A, Lopez-Garzon M, Ortiz-Comino L, Lozano-Lozano M. Therapeutic Benefits of Balneotherapy on Quality of Life of Patients with Rheumatoid Arthritis: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(24):13216. https://doi.org/10.3390/ijerph182413216
Chicago/Turabian StyleFernandez-Gonzalez, Maria, Carolina Fernandez-Lao, Lydia Martin-Martin, Angela Gonzalez-Santos, Maria Lopez-Garzon, Lucia Ortiz-Comino, and Mario Lozano-Lozano. 2021. "Therapeutic Benefits of Balneotherapy on Quality of Life of Patients with Rheumatoid Arthritis: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 24: 13216. https://doi.org/10.3390/ijerph182413216
APA StyleFernandez-Gonzalez, M., Fernandez-Lao, C., Martin-Martin, L., Gonzalez-Santos, A., Lopez-Garzon, M., Ortiz-Comino, L., & Lozano-Lozano, M. (2021). Therapeutic Benefits of Balneotherapy on Quality of Life of Patients with Rheumatoid Arthritis: A Systematic Review. International Journal of Environmental Research and Public Health, 18(24), 13216. https://doi.org/10.3390/ijerph182413216