
Dynamics of Mask Use as a Prevention Strategy against SARS-CoV-2 in Panama

 , ,
, , 
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Processing and Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reid, M.; Abdool-Karim, Q.; Geng, E.; Goosby, E. How will COVID-19 transform global health post-pandemic? Defining research and investment opportunities and priorities. PLoS Med. 2021, 18, e1003564. [Google Scholar] [CrossRef]
- Gostin, L.O.; Moon, S.; Meier, B.M. Reimagining global health governance in the age of COVID-19. Am. J. Public Health 2020, 110, 1615–1619. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report-71. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200331-sitrep-71-covid-19.pdf?sfvrsn=4360e92b_8 (accessed on 31 March 2020).
- Liu, Y.; Ning, Z.; Chen, Y.; Guo, M.; Liu, Y.; Gali, N.K.; Sun, L.; Duan, Y.; Cai, J.; Westerdahl, D.; et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature 2020, 582, 557–560. [Google Scholar] [CrossRef]
- Zhang, X.; Ji, Z.; Yue, Y.; Liu, H.; Wang, J. Infection risk assessment of COVID-19 through aerosol transmission: A case study of South China seafood market. Environ. Sci. Technol. 2021, 55, 4123–4133. [Google Scholar] [CrossRef]
- Feng, S.; Shen, C.; Xia, N.; Song, W.; Fan, M.; Cowling, B.J. Rational use of face masks in the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 434–436. [Google Scholar] [CrossRef]
- National Health Service (UK). Are Face Masks Useful for Preventing Coronavirus? 2020. Available online: https://www.nhs.uk/conditions/coronavirus-covid-19/common-questions/ (accessed on 9 April 2020).
- Greenhalgh, T.; Schmid, M.B.; Czypionka, T.; Bassler, D.; Gruer, L. Face masks for the public during the covid-19 crisis. BMJ 2020, 369, m1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, D.; Akl, E.; Duda, S.; Solo, K.; Yaacoub, S.; Schunemann, H. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.H.; et al. An evidence review of face masks against COVID-19. Proc. Nat. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, N.; Witt, C.; Rapp, S.; Wild, P.S.; Andreae, M.O.; Pöschl, U.; Su, H. Face masks effectively limit the probability of SARS-CoV-2 transmission. Science 2021, 372, 1439–1443. [Google Scholar] [CrossRef]
- Tay, B.K.; Roby, C.A.; Wu, J.W.; Tam, D.Y. Dynamical analysis of universal masking on the pandemic. Int. J. Environ. Res. Public Health 2021, 18, 9027. [Google Scholar] [CrossRef] [PubMed]
- Lyu, W.; Wehby, G.L. Community use of face masks and COVID-19: Evidence from a natural experiment of state mandates in the US. Health Aff. 2020, 39, 1419–1425. [Google Scholar] [CrossRef]
- Worby, C.J.; Chang, H.H. Face mask use in the general population and optimal resource allocation during the COVID-19 pandemic. Nat. Commun. 2020, 11, 4049. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.L.; Huang, J.; Zhang, C.J.P.; He, Z.; Ming, W.K. Facemask shortage and the novel coronavirus disease (COVID-19) outbreak: Reflections on public health measures. EClin. Med. 2020, 21, 100329. [Google Scholar]
- Dallas, M.P.; Horner, R.; Li, L. The mutual constraints of states and global value chains during COVID-19: The case of personal protective equipment. World Dev. 2021, 139, 105324. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.U.; Crimbly, F.; Khan, S.; Choudry, E.; Mehwish, S. Strategies for rational use of personal protective equipment (PPE) among healthcare providers during the COVID-19 crisis. Cureus 2020, 12, e8248. [Google Scholar] [CrossRef] [PubMed]
- Borkan, G.A.; Bachman, S.S.; Norris, A.H. Comparison of visually estimated age with physiologically predicted age as indicators of rates of aging. Soc. Sci. Med. 1982, 16, 197–204. [Google Scholar] [CrossRef]
- Olde Rikkert, M.G. Visual estimation of biological age of elderly subjects: Good interrater agreement. Gerontology 1999, 45, 165–167. [Google Scholar] [CrossRef]
- Bolker, B.M.; Brooks, M.E.; Clark, C.J.; Geange, S.W.; Poulsen, J.R.; Stevens, M.H.H.; White, J.-S.S. Generalized linear mixed models: A practical guide for ecology and evolution. Trends Ecol. Evol. 2009, 24, 127–135. [Google Scholar] [CrossRef]
- Zuur, A.F.; Ieno, E.N.; Elphick, C.S. A protocol for data exploration to avoid common statistical problems. Methods Ecol. Evol. 2010, 1, 3–14. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Brooks, M.E.; Kristensen, K.; van Benthem, K.J.; Magnusson, A.; Berg, C.W.; Nielsen, A.; Skaug, H.J.; Mächler, M.; Bolker, B.M. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. R J. 2017, 9, 378–400. [Google Scholar] [CrossRef] [Green Version]
- Bolker, B. Maximum Likelihood Estimation and Analysis with the Bbmle Package. 2014. Available online: https://cran.r-project.org/web/packages/bbmle/vignettes/mle2.pdf (accessed on 20 August 2021).
- Hartig, F. DHARMa: Residual Diagnostics for Hierarchical (Multi-Level/Mixed) Regression Models. R Package Version 0.1.5. 2017. Available online: http://cran.nexr.com/web/packages/DHARMa/vignettes/DHARMa.html (accessed on 14 May 2021).
- Fox, J.; Weisberg, S. An R Companion to Applied Regression; Sage publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S; Springer: New York, NY, USA, 2002. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- The World Bank. Data, Panama. 2021. Available online: https://data.worldbank.org/country/PA (accessed on 1 August 2021).
- Logistics in Panama. Available online: https://www.rvo.nl/sites/default/files/2018/08/Logistics%20report%20Panama%202018.pdf (accessed on 1 September 2021).
- Franco, D.; Gonzalez, C.; Abrego, L.E.; Carrera, J.P.; Diaz, Y.; Caicedo, Y.; Moreno, A.; Chavarria, O.; Gondola, J.; Castillo, M.; et al. Gorgas COVID19 team and Panama COVID19 Laboratory Network. Early transmission dynamics, spread, and genomic characterization of SARS-CoV-2 in Panama. Emerg. Infect. Dis. 2021, 27, 612–615. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Lorusso, F. Facial skin temperature and discomfort when wearing protective face masks: Thermal infrared imaging evaluation and hands moving the mask. Int. J. Environ. Res. Public Health 2020, 17, 4624. [Google Scholar] [CrossRef] [PubMed]
- Umberson, D. Gender, marital status and the social control of health behavior. Soc. Sci. Med. 1992, 34, 907–917. [Google Scholar] [CrossRef]
- Olcaysoy Okten, I.; Gollwitzer, A.; Oettingen, G. Gender differences in preventing the spread of coronavirus. Behav. Sci. Policy 2020, 6, 109–122. [Google Scholar] [CrossRef]
- Hutchins, H.J.; Wolff, B.; Leeb, R.; Ko, J.Y.; Odom, E.; Willey, J.; Friedman, A.; Bitsko, R.H. COVID-19 Mitigation behaviors by age group—United States, April–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1584–1590. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Response | Predictors | Odds Ratio | 95% C.I. | Wald−Test | p−Value |
|---|---|---|---|---|---|
| Cloth vs. valve | |||||
| Women | 3.54 | 2.96–4.25 | 13.69 | 0.001 | |
| Time period | 0.98 | 0.96–0.99 | −3.39 | 0.001 | |
| Market | 1.04 | 0.84–1.28 | 0.35 | 0.723 | |
| neighborhood | 1.98 | 1.10–3.58 | 2.27 | 0.023 | |
| Terminal | 1.1 | 0.93–1.31 | 1.14 | 0.253 | |
| Early adulthood | 1.24 | 0.85–1.82 | 1.12 | 0.263 | |
| Late middle adulthood | 1.01 | 0.86–1.18 | 0.09 | 0.931 | |
| Late adulthood | 1.53 | 1.17–2.01 | 3.06 | 0.002 | |
| KN95 vs. valve | |||||
| Women | 3.61 | 2.94–4.44 | 12.25 | 0.001 | |
| Time period | 1.02 | 1.00–1.03 | 1.9 | 0.057 | |
| Market | 1.07 | 0.84–1.37 | 0.56 | 0.578 | |
| neighborhood | 1.17 | 0.57–2.37 | 0.42 | 0.672 | |
| Terminal | 0.9 | 0.74–1.10 | −1.01 | 0.312 | |
| Early adulthood | 0.46 | 0.27–0.79 | −2.82 | 0.005 | |
| Late middle adulthood | 1.12 | 0.93–1.36 | 1.17 | 0.242 | |
| Late adulthood | 2.17 | 1.60–2.94 | 4.96 | 0.001 | |
| Surgical vs. valve | |||||
| Women | 3.71 | 3.10–4.44 | 14.3 | 0.001 | |
| Time period | 1.02 | 1.01–1.04 | 3.15 | 0.002 | |
| Market | 0.96 | 0.78–1.18 | −0.4 | 0.69 | |
| neighborhood | 1.83 | 1.02–3.29 | 2.02 | 0.043 | |
| Terminal | 1.02 | 0.86–1.21 | 0.24 | 0.813 | |
| Early adulthood | 0.95 | 0.65–1.38 | −0.29 | 0.773 | |
| Late middle adulthood | 0.8 | 0.69–0.94 | −2.71 | 0.007 | |
| Late adulthood | 1.19 | 0.91–1.56 | 1.27 | 0.204 |
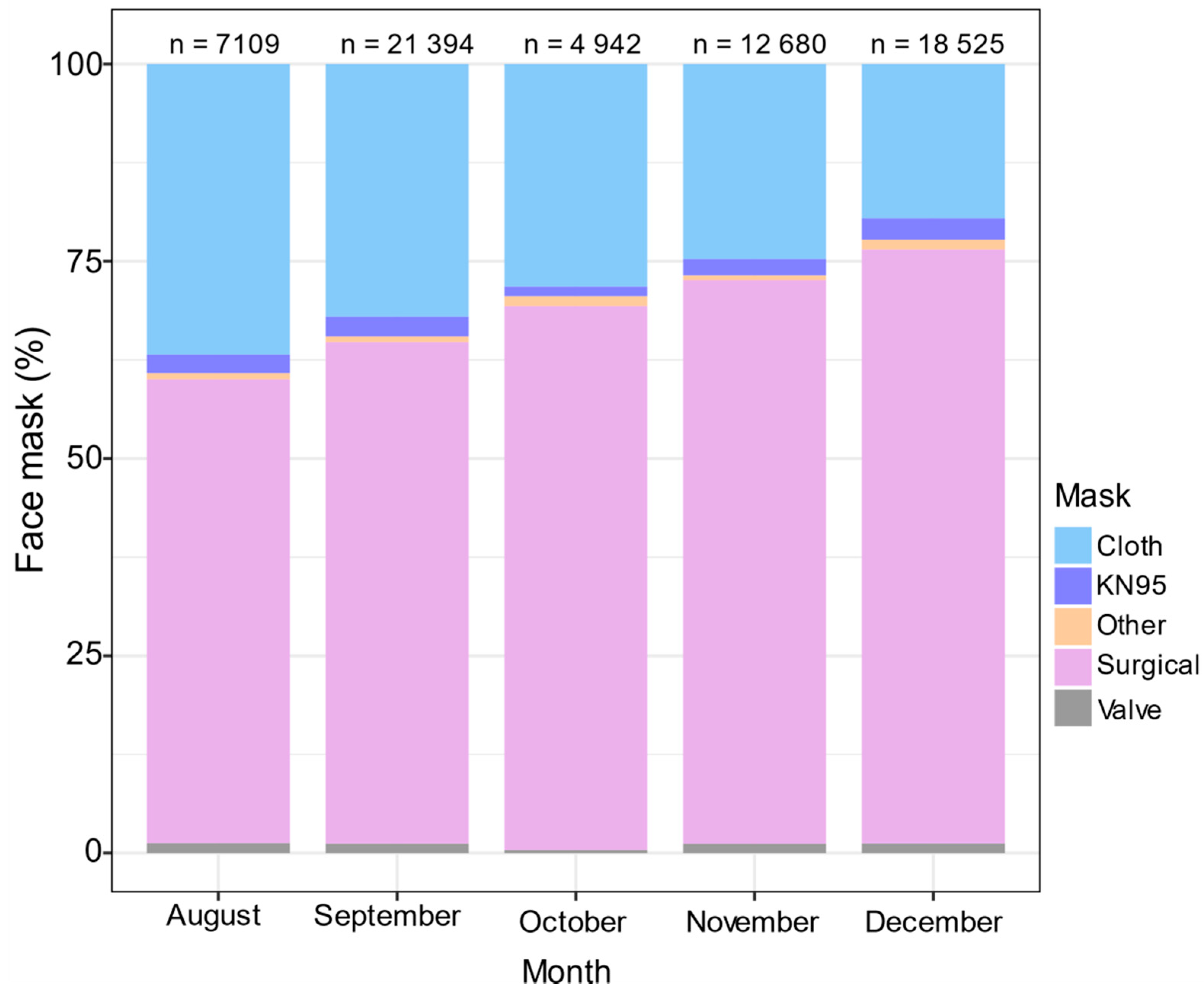
| Month (2020) | Prices per Unit of Surgical Masks Mean ± SD | Prices Range per Unit of Cloth Masks | Prices per Unit of KN 95 Masks Mean ± SD |
|---|---|---|---|
| August | 0.19 ± 0.08 | 1.50–3.50 | 1.86 ± 0.95 |
| September | 0.08 ± 0.04 | 1.50–3.50 | 1.65 ± 0.97 |
| October | 0.09 ± 0.04 | 1.50–3.50 | 1.82 ± 0.91 |
| November | 0.07 ± 0.05 | 1.50–3.50 | 1.12 ± 0.28 |
| December | 0.07 ± 0.03 | 1.00–3.50 | 1.05 ± 0.88 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Marín, H.; Bruner-Montero, G.; Portugal-Loayza, A.; Miranda, V.; Villarreal Dominguez, A.E.; Ortega-Barría, E.; Núñez-Samudio, V.; Landires, I.; Mejía, L.C.; López-Vergès, S.; et al. Dynamics of Mask Use as a Prevention Strategy against SARS-CoV-2 in Panama. Int. J. Environ. Res. Public Health 2021, 18, 12982. https://doi.org/10.3390/ijerph182412982
Fernández-Marín H, Bruner-Montero G, Portugal-Loayza A, Miranda V, Villarreal Dominguez AE, Ortega-Barría E, Núñez-Samudio V, Landires I, Mejía LC, López-Vergès S, et al. Dynamics of Mask Use as a Prevention Strategy against SARS-CoV-2 in Panama. International Journal of Environmental Research and Public Health. 2021; 18(24):12982. https://doi.org/10.3390/ijerph182412982
Chicago/Turabian StyleFernández-Marín, Hermógenes, Gaspar Bruner-Montero, Ana Portugal-Loayza, Virginia Miranda, Alcibiades Elias Villarreal Dominguez, Eduardo Ortega-Barría, Virginia Núñez-Samudio, Iván Landires, Luis C. Mejía, Sandra López-Vergès, and et al. 2021. "Dynamics of Mask Use as a Prevention Strategy against SARS-CoV-2 in Panama" International Journal of Environmental Research and Public Health 18, no. 24: 12982. https://doi.org/10.3390/ijerph182412982
APA StyleFernández-Marín, H., Bruner-Montero, G., Portugal-Loayza, A., Miranda, V., Villarreal Dominguez, A. E., Ortega-Barría, E., Núñez-Samudio, V., Landires, I., Mejía, L. C., López-Vergès, S., Wcislo, W. T., & Kosagisharaf, J. R. (2021). Dynamics of Mask Use as a Prevention Strategy against SARS-CoV-2 in Panama. International Journal of Environmental Research and Public Health, 18(24), 12982. https://doi.org/10.3390/ijerph182412982