
Balance of Autonomic Nervous Activity, Exercise, and Sleep Status in Older Adults: A Review of the Literature

 , ,
, ,  and
and
Abstract
1. Introduction
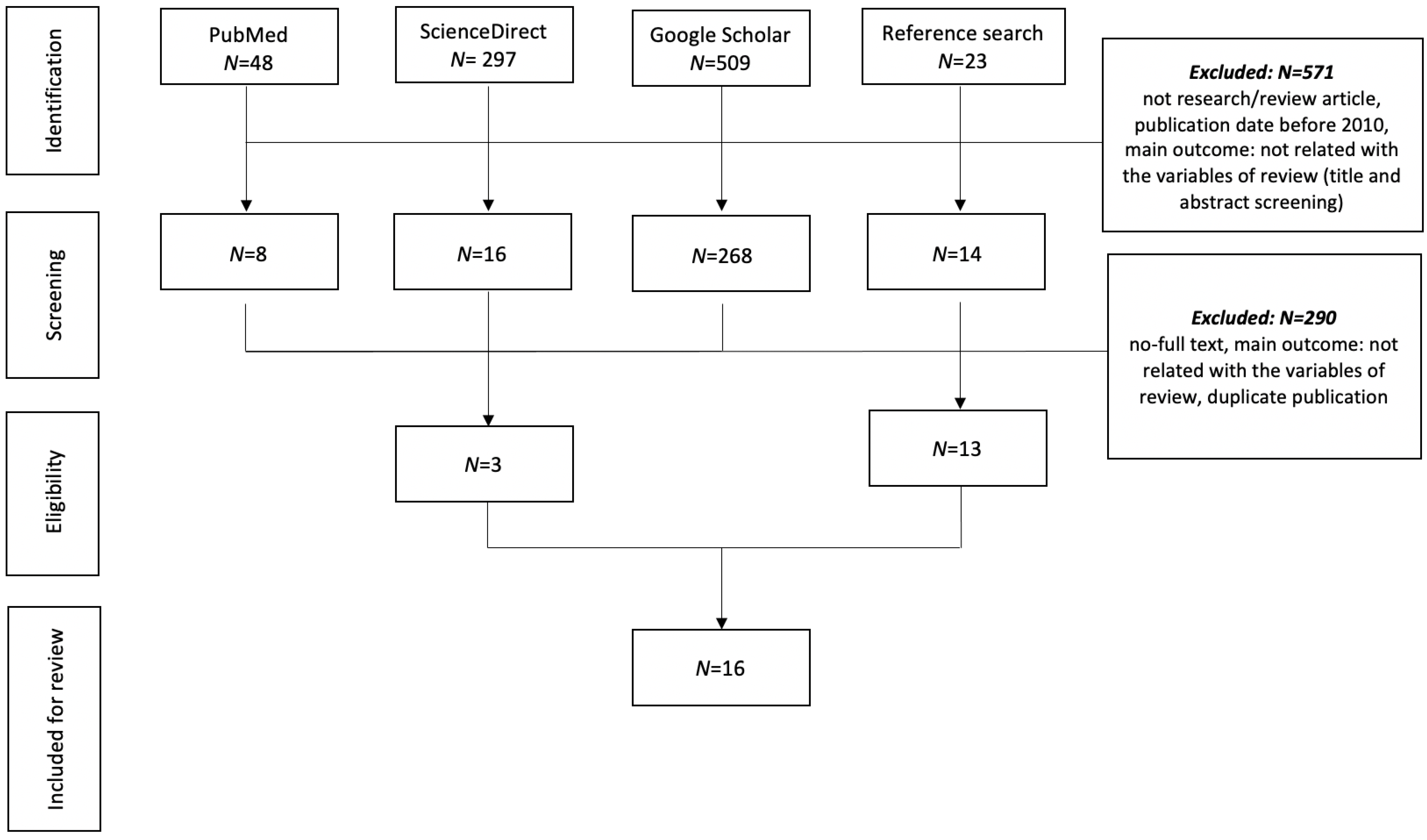
2. Materials and Methods
2.1. Design
2.2. Search Strategies
2.3. Inclusion and Exclusion Criteria
2.4. Article Synthesis and Analysis
3. Results
3.1. HRV Condition and Changes in Older Adults
3.2. Role of HRV for Healthy Aging
3.3. Factors Contributing to Healthy Aging
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute of Population and Social Security Research. Population projections for Japan (2017): 2016 to 2065. Available online: https://fpcj.jp/wp/wp-content/uploads/2017/04/1db9de3ea4ade06c3023d3ba54dd980f.pdf (accessed on 15 July 2021).
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 3 August 2021).
- Avidan, A.Y. Normal Sleep in Humans. In Atlas of Clinical Sleep Medicine, 2nd ed.; Kryger, M.H., Avidan, A.Y., Berry, R.B., Eds.; Saunders: Philadelphia, PA, USA, 2014. [Google Scholar]
- Azri, M.A.; Dahlan, A.; Masuri, M.G.; Isa, K.A.M. Sleep quality among older persons in institutions. Procedia-Soc. Behav. Sci. 2016, 234, 74–82. [Google Scholar] [CrossRef]
- Smagula, S.F.; Stone, K.L.; Fabio, A.; Cauley, J.A. Risk factors for sleep disturbances in older adults: Evidence from prospective studies. Sleep Med. Rev. 2016, 25, 21–30. [Google Scholar] [CrossRef]
- van Leeuwen, K.M.; van Loon, M.S.; van Nes, F.A.; Bosmans, J.E.; de Vet, H.; Ket, J.; Widdershoven, G.; Ostelo, R. What does quality of life mean to older adults? A thematic synthesis. PLoS ONE 2019, 14, e0213263. [Google Scholar] [CrossRef]
- Tan, J.P.H.; Beilharz, J.E.; Vollmer-Conna, U.V.; Cvejic, E. Heart rate variability as a marker of healthy ageing. Int. J. Cardiol. 2019, 275, 101–103. [Google Scholar] [CrossRef]
- Castro-Diehl, C.; Diez Roux, A.V.; Redline, S.; Seeman, T.; McKinley, P.; Sloan, R.; Shea, S. Sleep Duration and Quality in Relation to Autonomic Nervous System Measures: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2016, 39, 1927–1940. [Google Scholar] [CrossRef]
- Carnwell, R.; Daly, W. Strategies for the construction of a critical review of the literature. Nurse Educ. Pract. 2001, 1, 57–63. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Ageing and Disability. Available online: https://www.un.org/development/desa/disabilities/disability-and-ageing.html (accessed on 24 September 2021).
- Kudo, Y.; Sasaki, M. Effect of a hand massage with a warm hand bath on sleep and relaxation in elderly women with disturbance of sleep: A crossover trial. Jpn. J. Nurs. Sci. 2020, 17, e12327. [Google Scholar] [CrossRef]
- Chen, P.C.; Sattari, N.; Whitehurst, L.N.; Mednick, S.C. Age-related losses in cardiac autonomic activity during a daytime nap. Psychophysiology 2021, 58, e13701. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.Y.; Fan, Y.; Lu, Q.; Tan, L.H.; Tang, R.; Kaplan, R.M.; Pinho, M.C.; Thomas, B.P.; Chen, K.; Friston, K.J.; et al. Long-term physical exercise and mindfulness practice in an aging population. Front. Psychol. 2020, 11, 358. [Google Scholar] [CrossRef]
- Hernández-Vicente, A.; Hernando, D.; Santos-Lozano, A.; Rodríguez-Romo, G.; Vicente-Rodríguez, G.; Pueyo, E.; Bailón, R.; Garatachea, N. Heart rate variability and exceptional longevity. Front. Psychol. 2020, 11, 566399. [Google Scholar] [CrossRef]
- Queiroz, A.C.C.; Kanegusuku, H.; Chehuen, M.R.; Costa, L.A.R.; Wallerstein, L.F.; da Silva, V.J.D.; Mello, M.T.; Ugrinowitsch, C.; Forjaz, C.L.M. Cardiac work remains high after strength exercise in elderly. Int. J. Sports Med. 2013, 34, 391–397. [Google Scholar] [CrossRef]
- Albinet, C.T.; Boucard, G.; Bouquet, C.A.; Audiffren, M. Increased heart rate variability and executive performance after aerobic training in the elderly. Eur. J. Appl. Physiol. 2010, 109, 617–624. [Google Scholar] [CrossRef]
- Salmoirago-Blotcher, E.; Hovey, K.M.; Andrews, C.A.; Allison, M.; Brunner, R.L.; Denburg, N.L.; Eaton, C.; Garcia, L.; Sealy-Jefferson, S.M.; Zaslavsky, O.; et al. Psychological traits, heart rate variability, and risk of coronary heart disease in healthy aging women—The Women’s Health Initiative. Psychosom. Med. 2019, 81, 256–264. [Google Scholar] [CrossRef]
- Ogliari, G.; Mahinrad, S.; Stott, D.J.; Jukema, J.W.; Mooijaart, S.P.; Macfarlane, P.W.; Clark, E.N.; Kearney, P.M.; Westendorp, R.G.J.; de Craen, A.J.M.; et al. Resting heart rate, heart rate variability and functional decline in old age. CMAJ 2015, 187, E442–E449. [Google Scholar] [CrossRef]
- Kingsley, J.D.; Figueroa, A. Acute and training effects of resistance exercise on heart rate variability. Clin. Physiol. Funct. Imaging 2016, 36, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wu, H.; Zhang, X.; Wei, X.; Hou, F.; Ma, Y. Sleep heart rate variability assists the automatic prediction of long-term cardiovascular outcomes. Sleep Med. 2020, 67, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.; Gerhardsson, A.; van Leeuwen, W.; Lekander, M.; Ericson, M.; Fischer, H.; Kecklund, G.; Åkerstedt, T. Does sleep deprivation increase the vulnerability to acute psychosocial stress in young and older adults? Psychoneuroendocrinology 2018, 96, 155–165. [Google Scholar] [CrossRef]
- Stranges, S.; Tigbe, W.; Gómez-Olivé, F.X.; Thorogood, M.; Kandala, N.B. Sleep Problems: An Emerging Global Epidemic? Findings from the INDEPTH WHO-SAGE Study Among More Than 40,000 Older Adults From 8 Countries Across Africa and Asia. Sleep 2012, 35, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.C.; Hsu, N.W.; Chou, P. The Association Between Extreme Sleep Duration and Cardiac Autonomic Control in Community-Dwelling Older Adults: The Yilan Study, Taiwan. J. Gerontol. A Biol. Med. Sci. 2017, 72, 929–936. [Google Scholar] [CrossRef]
- Carter, J.R.; Fonkoue, I.T.; Greenlund, I.M.; Schwartz, C.E.; Mokhlesi, B.; Smoot, C.A. Sympathetic neural responsiveness to sleep deprivation in older adults: Sex differences. Am. J. Physiol. Heart Circ. Physiol. 2019, 317, H315–H322. [Google Scholar] [CrossRef] [PubMed]
- Viola, A.U.; Tobaldini, E.; Chellappa, S.L.; Casali, K.R.; Porta, A.; Montano, N. Short-Term Complexity of Cardiac Autonomic Control during Sleep: REM as a Potential Risk Factor for Cardiovascular System in Aging. PLoS ONE 2011, 6, e19002. [Google Scholar] [CrossRef] [PubMed]
- Piovezan, R.D.; Abucham, J.; Dos Santos, R.V.; Mello, M.T.; Tufik, S.; Poyares, D. The impact of sleep on age-related sarcopenia: Possible connections and clinical implications. Ageing Res. Rev. 2015, 23, 210–220. [Google Scholar] [CrossRef]
- Rocher, S.D.; Bessot, N.; Sesboüé, B.; Bulla, J.; Davenne, D. Circadian Characteristics of Older Adults and Aerobic Capacity. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 817–822. [Google Scholar] [CrossRef]
- Mizuno, K.; Kunii, M.; Seita, T.; Ono, S.; Komada, Y.; Shirakawa, S. Effects of habitual exercise on sleep habits and sleep health in middle-aged and older Japanese woman. J. Phys. Fit. Sports Med. 2004, 53, 527–536. [Google Scholar] [CrossRef][Green Version]
- Hotta, H.; Uchida, S. Aging of the autonomic nervous system and possible improvements in autonomic activity using somatic afferent stimulation. Geriatr. Gerontol. Int. 2010, 10 (Suppl. S1), S127–S136. [Google Scholar] [CrossRef]
- Liu, F.; Zhang, H.; Liu, Y.; Sun, X.; Yin, Z.; Li, H.; Deng, K.; Zhao, Y.; Wang, B.; Ren, Y.; et al. Sleep Duration Interacts With Lifestyle Risk Factors and Health Status to Alter Risk of All-Cause Mortality: The Rural Chinese Cohort Study. J. Clin. Sleep Med. 2018, 14, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Joyner, C. Meeting Sleep Guidelines Is Associated With Better Health-Related Quality of Life and Reduced Premature All-Cause Mortality Risk. Am. J. Health Promot. 2018, 32, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Kitano, N.; Tsunoda, K.; Tsuji, T.; Muraki, T.; Hotta, K.; Sanada, I.; Tanaka, K.; Okura, T. Relationship between physical activity and sleep in community-dwelling older adults. Jpn. J. Phys. Fitness Sports Med. 2013, 62, 105–112. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- Singh, D.; Vinod, K.; Saxena, S.C.; Deepak, K.K. Spectral evaluation of aging effects on blood pressure and heart rate variations in healthy subjects. J. Med. Eng. Technol. 2006, 30, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Hoevenaar-Blom, M.P.; Spijkerman, A.M.; Kromhout, D.; Verschuren, W.M. Sufficient sleep duration contributes to lower cardiovascular disease risk in addition to four traditional lifestyle factors: The MORGEN study. Eur. J. Prev. Cardiol. 2014, 21, 1367–1375. [Google Scholar] [CrossRef]
- Lee, T.; Lee, M.; Youm, C.; Noh, B.; Park, H. Association between Gait Variability and Gait-Ability Decline in Elderly Women with Subthreshold Insomnia Stage. Int. J. Environ. Res. Public Health 2020, 17, 5181. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.C.; Dzierzewski, J.M.; Alessi, C.A. Sleep problems in the elderly. Med. Clin. N. Am. 2015, 99, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Blackwell, T.L.; Redline, S.; Ancoli-Israel, S.; Paudel, M.L.; Cawthon, P.M.; Dam, T.L.; Barrett-Connor, E.; Leung, P.C.; Stone, K.L. Sleep disturbances and frailty status in older community-dwelling men. J. Am. Geriatr. Soc. 2009, 57, 2085–2093. [Google Scholar] [CrossRef]
- Ulsa, M.C.; Zheng, X.; Li, P.; Hu, K.; Gao, L. 547 Earlier-life sleep patterns and risk for delirium in elderly hospitalized patients from a 14-year longitudinal cohort. Sleep 2021, 44, A215–A216. [Google Scholar] [CrossRef]
- Zhang, J.; Lam, S.P.; Li, S.X.; Tang, N.L.; Yu, M.W.M.; Wing, Y.K. Insomnia, sleep quality, pain, and somatic symptoms: Sex differences and shared genetic components. Pain 2012, 153, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Ravan, A.R.; Bengtsson, C.; Lissner, L.; Lapidus, L.; Björkelund, C. Thirty-six-year secular trends in sleep duration and sleep satisfaction, and associations with mental stress and socioeconomic factors—Results of the Population Study of Women in Gothenburg, Sweden. J. Sleep Res. 2010, 19, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Tranah, G.J.; Parimi, N.; Blackwell, T.; Ancoli-Israel, S.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Lane, N.; Paudel, M.L.; Hilier, T.A.; et al. Postmenopausal hormones and sleep quality in the elderly: A population based study. BMC Womens Health 2010, 10, 15. [Google Scholar] [CrossRef]
- Kline, C.E.; Hillman, C.H.; Sheppard, B.B.; Tennant, B.; Conroy, D.E.; Macko, R.F.; Marquez, D.X.; Petruzzello, S.J.; Powell, K.E.; Erickson, K.I. Physical activity and sleep: An updated umbrella review of the 2018 Physical Activity Guidelines Advisory Committee report. Sleep Med. Rev. 2021, 58, 101489. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Vitiello, M.V.; Gooneratne, N.S. Sleep in Normal Aging. Sleep Med. Clin. 2018, 13, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar] [CrossRef] [PubMed]
- Yoon, I.Y.; Kripke, D.F.; Youngstedt, S.D.; Elliott, J.A. Actigraphy suggests age-related differences in napping and nocturnal sleep. J. Sleep Res. 2003, 12, 87–93. [Google Scholar] [CrossRef]
- Chaput, J.P. Sleep patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 86–91. [Google Scholar] [CrossRef]
- Salthouse, T.A. Are individual differences in rates of aging greater at older ages? Neurobiol. Aging 2012, 33, 2373–2381. [Google Scholar] [CrossRef] [PubMed]
- Stephens, R. How Does Age Impact Your Ability to Make Decisions? Available online: https://www.ucf.edu/news/how-your-age-can-impact-your-ability-to-make-decisions/ (accessed on 2 October 2021).
- Howieson, D.B. Cognitive Skills and the Aging Brain: What to Expect. Cerebrum 2015, 2015, cer-14-15. [Google Scholar]
- Okura, T.; Saghazadeh, M.; Soma, Y.; Tsunoda, K. Physical fitness, physical activity, exercise training and cognitive function in older adults. J. Phys. Fitness Sports Med. 2013, 2, 275–286. [Google Scholar] [CrossRef][Green Version]
- Guralnik, J.M.; Balfour, J.L.; Volpato, S. The ratio of older women to men: Historical perspectives and cross-national comparisons. Aging Clin. Exp. Res. 2000, 12, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Zarulli, V.; Jones, J.A.B.; Oksuzyan, A.; Lindahl-Jacobsen, R.; Christensen, K.; Vaupel, J.W. Women live longer than men even during crises. Proc. Natl. Acad. Sci. USA 2018, 115, E832–E840. [Google Scholar] [CrossRef]
- Baum, F.; Musolino, C.; Gesesew, H.A.; Popay, J. New Perspective on Why Women Live Longer Than Men: An Exploration of Power, Gender, Social Determinants, and Capitals. Int. J. Environ. Res. Public Health 2021, 18, 661. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference Number | Research Subjects | Main Findings | Limitation of the Studies |
|---|---|---|---|
| [7] |
|
| The nature of the study (cross sectional study) makes it difficult to determine the directionality of age, HRV and health associations. |
| [11] |
| A hand massage with a warm hand bath improved subjective sleep quality and provided relaxation among older women with disturbance of sleep. | Self-selection bias, in which those who wished to participate were those who were experiencing sleeping problems. |
| [12] |
|
| No standardized diagnostic assessment of psychiatric disorder or chronic medical disease was performed to confirm the self-reported screening surveys. |
| [13] |
|
| A relatively small sample of subjects with more females. |
| [14] |
|
| Gender heterogeneity in the centenarian group, with 76.5% of the centenarians’ group was women. |
| [15] |
|
| The acute effects of a strength training session in sedentary subjects who might respond differently were not evaluated. |
| [16] |
|
| Small sample size, lack of control for other potential confounders such as diet habits and vitamins or Omega 3 supplements, as well as genetic profiles. |
| [17] |
|
| Findings are not generalizable to males, younger age groups, and non-white minorities. |
| [18] |
|
| Using a 10-s ECG; so that no significant association of resting heart rate and heart rate variability with functional status could not be shown. |
| [19] | Articles including older people aged 68 years and older. |
| Timeline (from which year articles were included) was not mentioned. |
| [20] |
|
| Only conventional HRV metrics were considered in this study. |
| [21] |
| Older adults had higher autonomic activation at baseline, but their response to sleep deprivation did not significantly differ from the younger adults. | Participants in the non-sleep deprivation condition were not monitored in the lab until the test session but slept at home and arrived in time for the test session at the laboratory. |
| [22] |
|
| Data on chronic comorbidities and lifestyle behaviors were not collected, preventing any analysis adjusting for these variables. Information about sleep problems was self-reported, which could produce misclassification of true sleep patterns. |
| [23] |
|
| The timeframe of recalling sleep duration was 4 weeks, and whether this sleep duration is capable of representing the stable status over a long period remains unknown. |
| [24] |
|
| The limitation is total sleep deprivation experimental approach, because it is more common for humans to be exposed to repeated nights of short sleep (i.e., partial sleep restriction). |
| [25] |
|
| No information if there were participants excluded during the experiment. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sato, M.; Betriana, F.; Tanioka, R.; Osaka, K.; Tanioka, T.; Schoenhofer, S. Balance of Autonomic Nervous Activity, Exercise, and Sleep Status in Older Adults: A Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 12896. https://doi.org/10.3390/ijerph182412896
Sato M, Betriana F, Tanioka R, Osaka K, Tanioka T, Schoenhofer S. Balance of Autonomic Nervous Activity, Exercise, and Sleep Status in Older Adults: A Review of the Literature. International Journal of Environmental Research and Public Health. 2021; 18(24):12896. https://doi.org/10.3390/ijerph182412896
Chicago/Turabian StyleSato, Miki, Feni Betriana, Ryuichi Tanioka, Kyoko Osaka, Tetsuya Tanioka, and Savina Schoenhofer. 2021. "Balance of Autonomic Nervous Activity, Exercise, and Sleep Status in Older Adults: A Review of the Literature" International Journal of Environmental Research and Public Health 18, no. 24: 12896. https://doi.org/10.3390/ijerph182412896
APA StyleSato, M., Betriana, F., Tanioka, R., Osaka, K., Tanioka, T., & Schoenhofer, S. (2021). Balance of Autonomic Nervous Activity, Exercise, and Sleep Status in Older Adults: A Review of the Literature. International Journal of Environmental Research and Public Health, 18(24), 12896. https://doi.org/10.3390/ijerph182412896