Effect of Standardized Yelling on Subjective Perception and Autonomic Nervous System Activity in Motion Sickness

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Motion Sickness Induced by Coriolis Stimulation
2.3. Quantification of Motion Sickness Severity
2.4. Assessment of Individual Attention and Concentration Performance
2.5. Evaluation of Autonomic Nervous System Activity
2.6. Introduction of the Standardized Yelling Maneuver and the Time of Intervention
2.7. Experimental Procedure
2.8. Statistical Analysis
3. Results
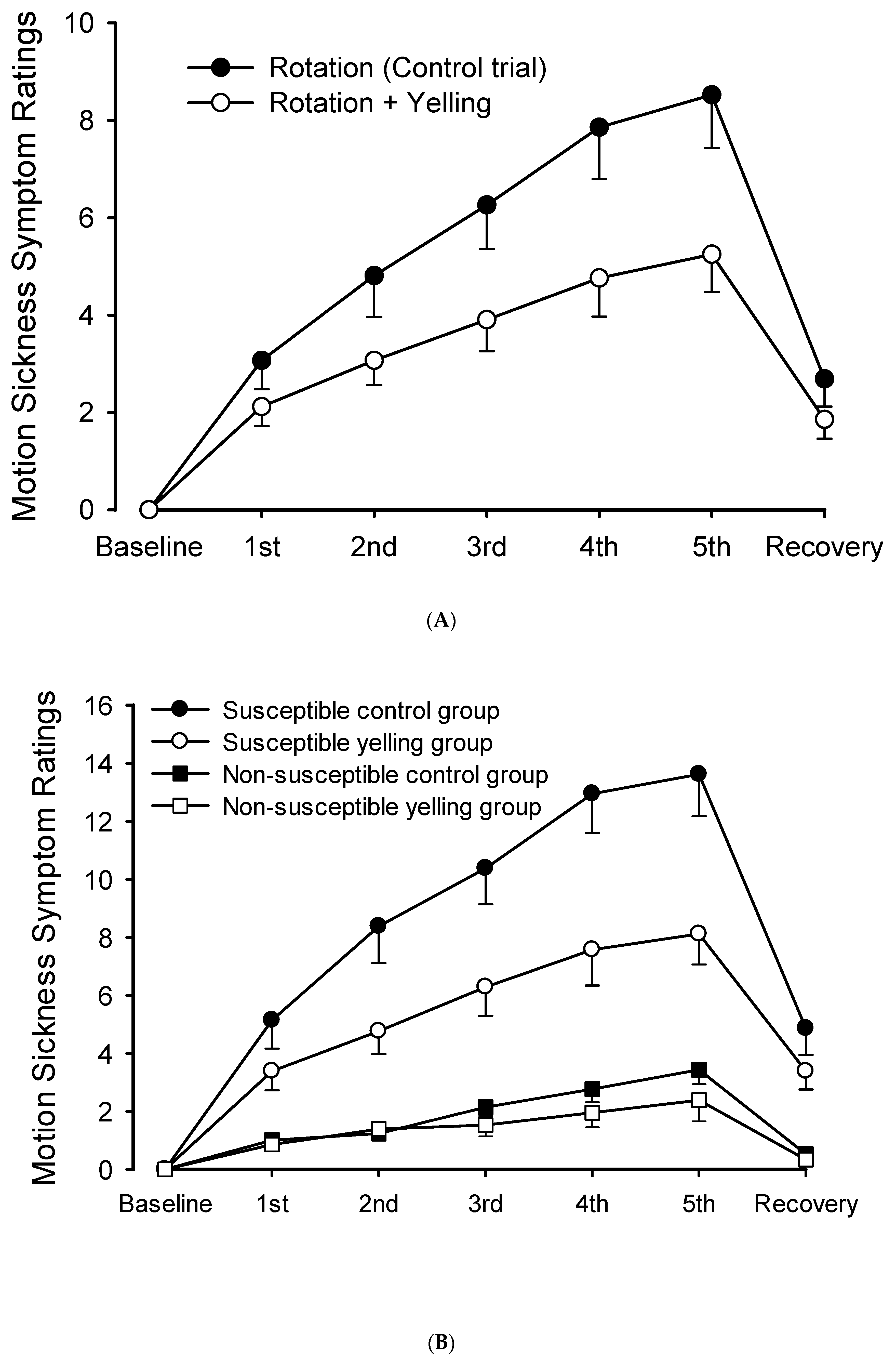
3.1. Effect of the Yelling Intervention on the Severity of Motion Sickness Symptoms
3.2. Effects of the Yelling Intervention on Cognition and Attention after Inducing Motion Sickness
3.3. Effects of Simple Yelling on Cardiovascular and HRV at Rest
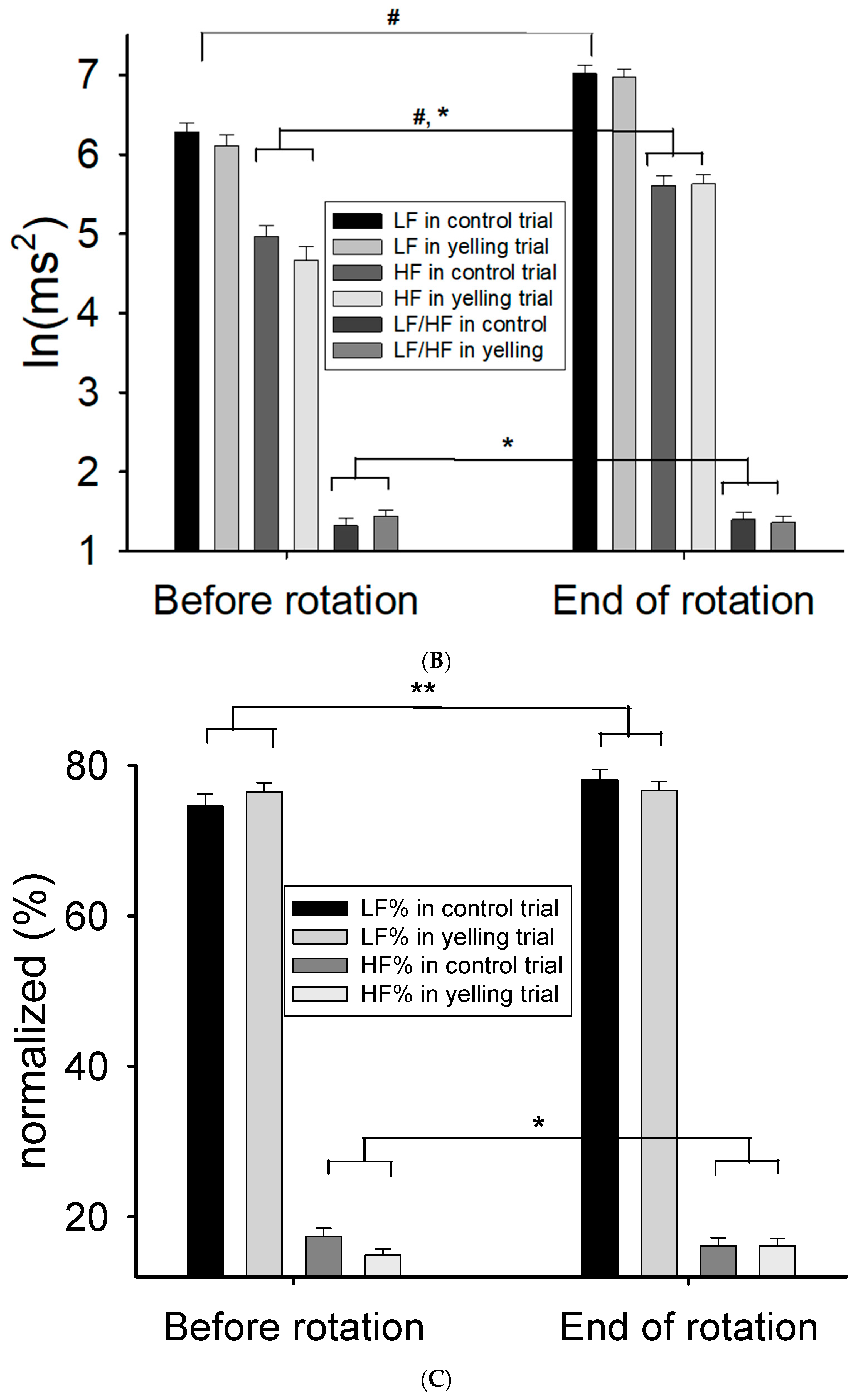
3.4. Effects of the Yelling Intervention on Cardiovascular and Heart Rate Variability during Rotation Stimulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Claremont, C. The psychology of seasickness. Psyche 1931, 11, 86–90. [Google Scholar]
- Golding, J.F. Motion sickness. Handb. Clin. Neurol. 2016, 137, 371–390. [Google Scholar]
- Golding, J.F. Motion sickness susceptibility. Auton. Neurosci. 2006, 129, 67–76. [Google Scholar] [CrossRef]
- Shupak, A.; Gordon, C.R. Motion sickness: Advances in pathogenesis, prediction, prevention, and treatment. Aviat. Space Environ. Med. 2006, 77, 1213–1223. [Google Scholar] [PubMed]
- Mullen, T.J.; Berger, R.D.; Oman, C.M.; Cohen, R.J. Human heart rate variability relation is unchanged during motion sickness. J. Vestib. Res. 1998, 8, 95–105. [Google Scholar] [CrossRef]
- Yokota, Y.; Aoki, M.; Mizuta, K.; Ito, Y.; Isu, N. Motion sickness susceptibility associated with visually induced postural instability and cardiac autonomic responses in healthy subjects. Acta Oto-Laryngol. 2005, 125, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Park, S.J.J.I.A. Big-Ecg. Cardiographic Predictive Cyber-Physical System for Stroke Management. IEEE Access 2021, 9, 123146–123164. [Google Scholar] [CrossRef]
- Buckey, J.C.; Alvarenga, D.; Cole, B.; Rigas, J.R. Chlorpheniramine for motion sickness. J. Vestib. Res. Equilib. Orientat. 2004, 14, 53–61. [Google Scholar] [CrossRef]
- Spinks, A.; Wasiak, J. Scopolamine (hyoscine) for preventing and treating motion sickness. Cochrane Database Syst. Rev. 2011, 2011, Cd002851. [Google Scholar] [CrossRef]
- Kuo, B.-J.; Chen, C.-L.; Chen, H.-Y.; Wen, T.-S. EEG Analysis during Spatial Disorientation with and without Yelling Maneuver. J. Aviat. Med. Sci. ROC 2004, 18, 91–99, (Full Text in Chinese). [Google Scholar]
- Chen, C.-L.; Hong, C.-T.; Kuo, B.-J.; Lin, Y.-T.; Long, F.-W.; Sun, C.-M.; Wen, T.-S. The Influence of APRL Maneuver on the Residual Effect of Coriolis Illusion. J. Aviat. Med. Sci. ROC 2007, 21, 95–104, (Full Text in Chinese). [Google Scholar]
- Chen, C.L.; Yu, N.Y.; Tang, J.S.; Chang, S.H.; Yang, Y.R.; Wang, L. Effect of yelling on maximal aerobic power during an incremental test of cycling performance. J. Sport Health Sci. 2016, 5, 456–461. [Google Scholar] [CrossRef]
- Hussain, I.; Young, S.; Kim, C.H.; Benjamin, H.C.M.; Park, S.J.J.S. Quantifying Physiological Biomarkers of a Microwave Brain Stimulation Device. Sensors 2021, 21, 1896. [Google Scholar] [CrossRef]
- Tang, J.-S.; Yu, N.-Y.; Lee, F.-H.; Lung, C.-W.; Lee, L.-C.; Liau, B.-Y.; Chen, C.-L. Influence of Location and Frequency Variations of Binaural Electrostimulation on Heart Rate Variability. In International Conference on Applied Human Factors and Ergonomics: 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 70–79. [Google Scholar]
- Kotani, K.; Tachibana, M.; Takamasu, K. Investigation of the influence of swallowing, coughing and vocalization on heart rate variability with respiratory-phase domain analysis. Methods Inf. Med. 2007, 46, 179–185. [Google Scholar]
- Tian, D.; Mo, F.; Cai, X.; Miao, Z.; Xiao, F.; Chang, Y.; Wu, L.; Tang, Y.; Wang, X.; Ye, C.; et al. Acupuncture relieves motion sickness via the IRβ-ERK1/2-dependent insulin receptor signalling pathway. Acupunct. Med. J. Br. Med. Acupunct. Soc. 2018, 36, 153–161. [Google Scholar] [CrossRef]
- Davis, J.R.; Johnson, R.; Stepanek, J. Spatial Orientation in Flight. In Fundamentals of Aerospace Medicine, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 174–176. [Google Scholar]
- Sanderson, J.; Oman, C.M.; Harris, L.R. Measurement of oscillopsia induced by vestibular Coriolis stimulation. J. Vestib. Res. Equilib. Orientat. 2007, 17, 289–299. [Google Scholar] [CrossRef]
- Klosterhalfen, S.; Kellermann, S.; Pan, F.; STOcKHORST, U.; Hall, G.; ENcK, P. Effects of ethnicity and gender on motion sickness susceptibility. Aviat. Space Environ. Med. 2005, 76, 1051–1057. [Google Scholar]
- Bates, M.E.; Lemay, E.P. The d2 Test of attention: Construct validity and extensions in scoring techniques. J. Int. Neuropsychol. Soc. 2004, 10, 392–400. [Google Scholar] [CrossRef]
- Kuo, T.B.; Lin, T.; Yang, C.C.; Li, C.-L.; Chen, C.-F.; Chou, P. Effect of aging on gender differences in neural control of heart rate. Am. J. Physiol.-Heart Circ. Physiol. 1999, 277, H2233–H2239. [Google Scholar] [CrossRef]
- Kuo, T.; Chan, S. Continuous, on-line, real-time spectral analysis of systemic arterial pressure signals. Am. J. Physiol.-Heart Circ. Physiol. 1993, 264, H2208–H2213. [Google Scholar] [CrossRef]
- Berger, R.D.; Saul, J.P.; Cohen, R.J. Transfer function analysis of autonomic regulation. I. Canine atrial rate response. Am. J. Physiol.-Heart Circ. Physiol. 1989, 256, H142–H152. [Google Scholar] [CrossRef]
- Malik, M. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use: Task force of the European Society of Cardiology and the North American Society for Pacing and Electrophysiology. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar] [CrossRef]
- Doweck, I.; Gordon, C.R.; Shlitner, A.; Spitzer, O.; Gonen, A.; Binah, O.; Melamed, Y.; Shupak, A. Alterations in R–R variability associated with experimental motion sickness. J. Auton. Nerv. Syst. 1997, 67, 31–37. [Google Scholar] [CrossRef]
- Ohyama, S.; Nishiike, S.; Watanabe, H.; Matsuoka, K.; Akizuki, H.; Takeda, N.; Harada, T. Autonomic responses during motion sickness induced by virtual reality. Auris Nasus Larynx 2007, 34, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.; Li, M.-H.; Ye, N.-Y.; Chiou, W.-Y. Effects of cranial electrostimulation on motion sickness induced by Coriolis stimulation. J. Med. Sci. 2012, 32, 69–74. [Google Scholar]
- Chu, H.; Li, M.-H.; Huang, Y.-C.; Lee, S.-Y. Simultaneous transcutaneous electrical nerve stimulation mitigates simulator sickness symptoms in healthy adults: A crossover study. BMC Complement. Altern. Med. 2013, 13, 84. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J.J.I.A. HealthSOS: Real-Time Health Monitoring System for Stroke Prognostics. IEEE Access 2020, 8, 213574–213586. [Google Scholar] [CrossRef]
- Hussain, I.; Park, S.J. Quantitative evaluation of task-induced neurological outcome after stroke. Brain Sci. 2021, 11, 900. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trials (C vs. Y) | Before Rotation | After Rotation | p Value (Trial) | p Value (Time) | p Value (Trial × Time) | |
|---|---|---|---|---|---|---|
| Susceptible group (n = 21) | ||||||
| TN | Control | 243.0 ± 15.7 | 259.4 ± 10.9 | 0.834 | <0.001 | 0.227 |
| Yelling | 240.6 ± 16.4 | 265.5 ± 14.4 | ||||
| E% | Control | 33.10 ± 6.04 | 22.18 ± 4.93 | 0.714 | <0.001 | 0.621 |
| Yelling | 36.09 ± 7.07 | 22.78 ± 5.62 | ||||
| TN-E | Control | 176.9 ± 24.8 | 209.6 ± 17.7 | 0.848 | <0.001 | 0.205 |
| Yelling | 171.4 ± 26.5 | 221.9 ± 22.9 | ||||
| CP | Control | 242.6 ± 15.8 | 259.0 ± 10.9 | 0.848 | 0.001 | 0.205 |
| Yelling | 239.9 ± 16.6 | 265.1 ± 14.5 | ||||
| Non-susceptible group (n = 21) | ||||||
| TN | Control | 257.8 ± 11.4 | 284.0 ± 8.8 | 0.633 | <0.001 | 0.481 |
| Yelling | 250.5 ± 14.9 | 282.0 ± 11.7 | ||||
| E% | Control | 23.36 ± 4.80 | 9.78 ± 2.38 | 0.538 | <0.001 | 0.405 |
| Yelling | 28.40 ± 5.25 | 10.79 ± 2.39 | ||||
| TN-E | Control | 205.2 ± 17.8 | 257.8 ± 11.3 | 0.661 | <0.001 | 0.462 |
| Yelling | 191.0 ± 23.1 | 254.8 ± 15.7 | ||||
| CP | Control | 256.8 ± 11.5 | 283.1 ± 8.5 | 0.662 | <0.001 | 0.460 |
| Yelling | 249.7 ± 14.9 | 281.6 ± 11.7 | ||||
| Parameters | Before Yelling | During Yelling | p Value |
|---|---|---|---|
| HR (bpm) | 71.8 ± 3.2 | 70.3 ± 3.3 | 0.450 |
| SBP (mmHg) | 117.1 ± 4.3 | 121.0 ± 4.4 | 0.047 |
| DBP (mmHg) | 74.5 ± 2.9 | 79.5 ± 3.3 | 0.006 |
| TP [ln(ms2)] | 7.88 ± 0.16 | 8.02 ± 0.17 | 0.169 |
| LF [ln(ms2)] | 7.27 ± 0.15 | 7.35 ± 0.15 | 0.377 |
| HF [ln(ms2)] | 5.95 ± 0.19 | 6.04 ± 0.24 | 0.747 |
| LF/HF (ln ratio) | 1.32 ± 0.08 | 1.36 ± 0.16 | 0.747 |
| LF (%) | 77.13 ± 1.60 | 76.74 ± 2.49 | 0.852 |
| HF (%) | 17.15 ± 1.05 | 16.98 ± 2.02 | 0.934 |
| Parameters | Trials | Before Rotation | End of Rotation | p Value (Trial) | p Value (Time) | p Value (Trial × Time) |
|---|---|---|---|---|---|---|
| HR (bpm) | Control | 74.8 ± 1.6 | 71.7 ± 1.4 | 0.858 | <0.001 | 0.236 |
| Yelling | 75.6 ± 1.7 | 71.3 ± 1.7 | ||||
| SBP (mmHg) | Control | 123.0 ± 1.7 | 125.6 ± 1.8 | 0.724 | 0.019 | 0.423 |
| Yelling | 124.0 ± 1.7 | 125.5 ± 1.7 | ||||
| DBP (mmHg) | Control | 74.9 ± 1.2 | 78.7 ± 1.5 | 0.351 | <0.001 | 0.947 |
| Yelling | 75.7 ± 1.5 | 79.6 ± 1.3 | ||||
| TP [ln(ms2)] | Control | 6.94 ± 0.11 | 7.67 ± 0.09 | 0.848 | <0.001 | 0.202 |
| Yelling | 6.84 ± 0.12 | 7.73 ± 0.09 | ||||
| LF [ln(ms2)] | Control | 6.29 ± 0.11 | 7.02 ± 0.10 | 0.315 | <0.001 | 0.372 |
| Yelling | 6.11 ± 0.14 | 6.98 ± 0.09 | ||||
| HF [ln(ms2)] | Control | 4.97 ± 0.14 | 5.61 ± 0.12 | 0.228 | <0.001 | 0.069 |
| Yelling | 4.67 ± 0.17 | 5.63 ± 0.11 | ||||
| LF/HF (ln ratio) | Control | 1.32 ± 0.09 | 1.40 ± 0.09 | 0.607 | 0.979 | 0.069 |
| Yelling | 1.44 ± 0.07 | 1.36 ± 0.08 | ||||
| LF (%) | Control | 74.6 ± 1.6 | 78.1 ± 1.4 | 0.826 | 0.098 | 0.036 |
| Yelling | 76.5 ± 1.2 | 76.7 ± 1.2 | ||||
| HF (%) | Control | 17.4 ± 1.1 | 16.1 ± 1.1 | 0.131 | 0.947 | 0.077 |
| Yelling | 14.9 ± 0.8 | 16.1 ± 1.0 |
| Parameters | Trials | Before Rotation | End of Rotation | p Value (Trial) | p Value (Time) | p Value (Trial × Time) |
|---|---|---|---|---|---|---|
| Susceptive group (n = 21) | ||||||
| TP [ln(ms2)] | Control | 6.97 ± 0.17 | 7.67 ± 0.14 | 0.588 | <0.001 | 0.691 |
| Yelling | 7.02 ± 0.15 | 7.76 ± 0.15 | ||||
| LF [ln(ms2)] | Control | 6.32 ± 0.17 | 6.96 ± 0.17 | 0.906 | <0.001 | 0.917 |
| Yelling | 6.33 ± 0.15 | 6.99 ± 0.15 | ||||
| HF [ln(ms2)] | Control | 4.99 ± 0.22 | 5.55 ± 0.18 | 0.942 | <0.001 | 0.508 |
| Yelling | 4.94 ± 0.18 | 5.58 ± 0.18 | ||||
| LF/HF (ln ratio) | Control | 1.33 ± 0.10 | 1.42 ± 0.12 | 0.788 | 0.583 | 0.538 |
| Yelling | 1.40 ± 0.09 | 1.41 ± 0.12 | ||||
| LF (%) | Control | 74.9 ± 1.8 | 78.1 ± 1.7 | 0.998 | 0.164 | 0.567 |
| Yelling | 75.6 ± 1.8 | 77.4 ± 1.8 | ||||
| HF (%) | Control | 16.9 ± 1.5 | 15.3 ± 1.4 | 0.249 | 0.333 | 0.590 |
| Yelling | 15.2 ± 1.1 | 14.6 ± 1.4 | ||||
| Non-susceptible group (n = 21) | ||||||
| TP [ln(ms2)] | Control | 6.90 ± 0.14 | 7.67 ± 0.11 | 0.412 | <0.001 | 0.229 |
| Yelling | 6.65 ± 0.19 | 7.71 ± 0.11 | ||||
| LF [ln(ms2)] | Control | 6.25 ± 0.14 | 7.07 ± 0.11 | 0.122 | <0.001 | 0.360 |
| Yelling | 5.89 ± 0.23 | 6.98 ± 0.12 | ||||
| HF [ln(ms2)] | Control | 4.94 ± 0.16 | 5.68 ± 0.15 | 0.103 | <0.001 | 0.093 |
| Yelling | 4.41 ± 0.27 | 5.67 ± 0.14 | ||||
| LF/HF (ln ratio) | Control | 1.31 ± 0.14 | 1.39 ± 0.13 | 0.650 | 0.535 | 0.061 |
| Yelling | 1.48 ± 0.09 | 1.30 ± 0.11 | ||||
| LF (%) | Control | 74.2 ± 2.6 | 78.2 ± 2.4 | 0.772 | 0.381 | 0.017 |
| Yelling | 77.5 ± 1.5 | 76.0 ± 1.6 | ||||
| HF (%) | Control | 17.9 ± 1.7 | 16.8 ± 1.7 | 0.327 | 0.389 | 0.074 |
| Yelling | 14.6 ± 1.2 | 17.6 ± 1.4 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tu, M.-Y.; Chu, H.; Lai, C.-Y.; Chiang, K.-T.; Huang, C.-C.; Chin, H.-C.; Wen, Y.-H.; Chen, C.-L. Effect of Standardized Yelling on Subjective Perception and Autonomic Nervous System Activity in Motion Sickness. Int. J. Environ. Res. Public Health 2021, 18, 12854. https://doi.org/10.3390/ijerph182312854
Tu M-Y, Chu H, Lai C-Y, Chiang K-T, Huang C-C, Chin H-C, Wen Y-H, Chen C-L. Effect of Standardized Yelling on Subjective Perception and Autonomic Nervous System Activity in Motion Sickness. International Journal of Environmental Research and Public Health. 2021; 18(23):12854. https://doi.org/10.3390/ijerph182312854
Chicago/Turabian StyleTu, Min-Yu, Hsin Chu, Chung-Yu Lai, Kwo-Tsao Chiang, Chi-Chan Huang, Hsien-Chuan Chin, Yu-Hsin Wen, and Chien-Liang Chen. 2021. "Effect of Standardized Yelling on Subjective Perception and Autonomic Nervous System Activity in Motion Sickness" International Journal of Environmental Research and Public Health 18, no. 23: 12854. https://doi.org/10.3390/ijerph182312854
APA StyleTu, M.-Y., Chu, H., Lai, C.-Y., Chiang, K.-T., Huang, C.-C., Chin, H.-C., Wen, Y.-H., & Chen, C.-L. (2021). Effect of Standardized Yelling on Subjective Perception and Autonomic Nervous System Activity in Motion Sickness. International Journal of Environmental Research and Public Health, 18(23), 12854. https://doi.org/10.3390/ijerph182312854