
Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility and Recruitment
2.3. Randomization
2.4. Intervention
2.5. Questionnaires
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Music Therapy Sessions
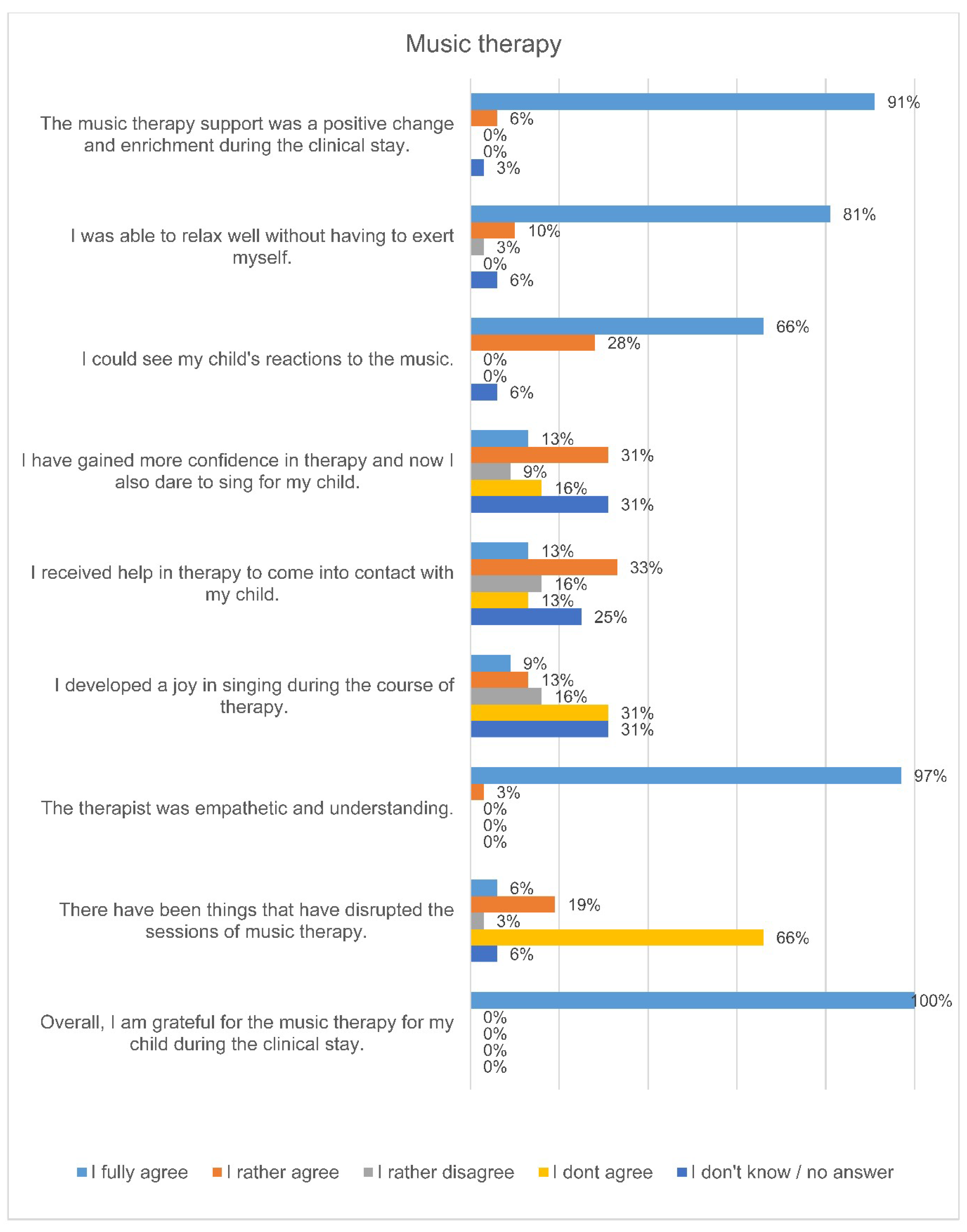
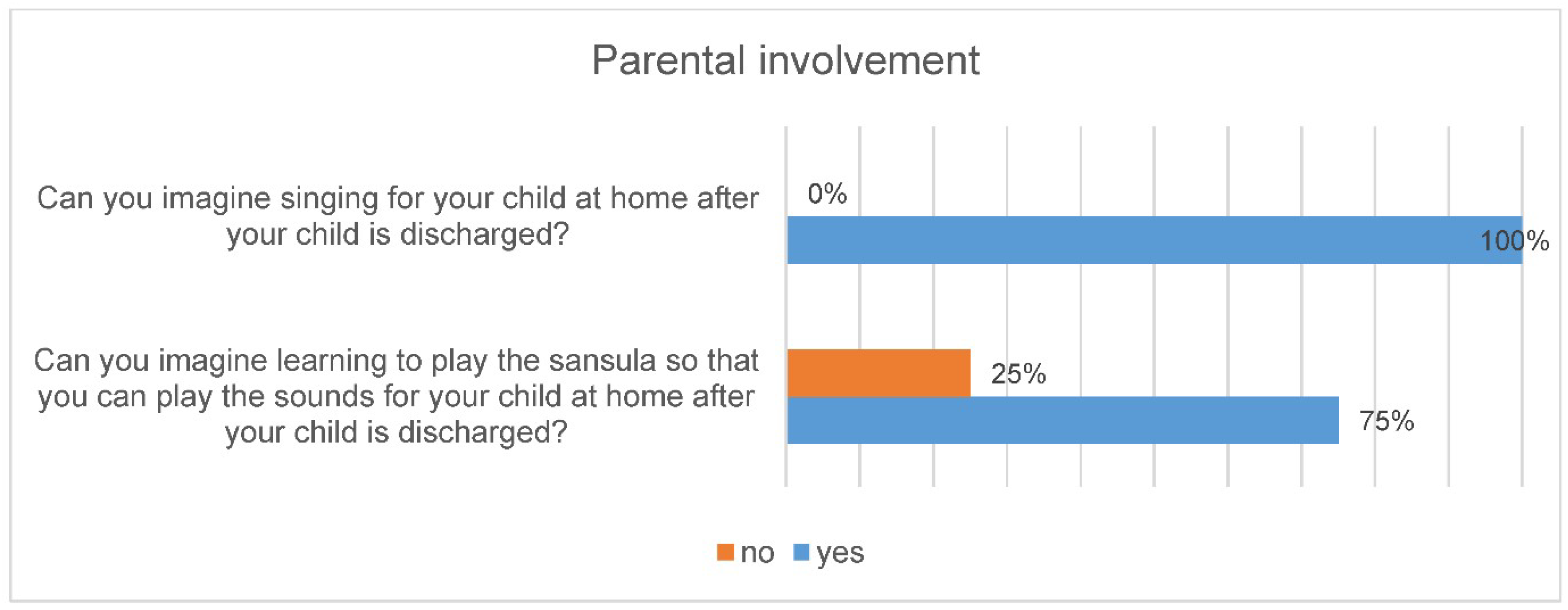
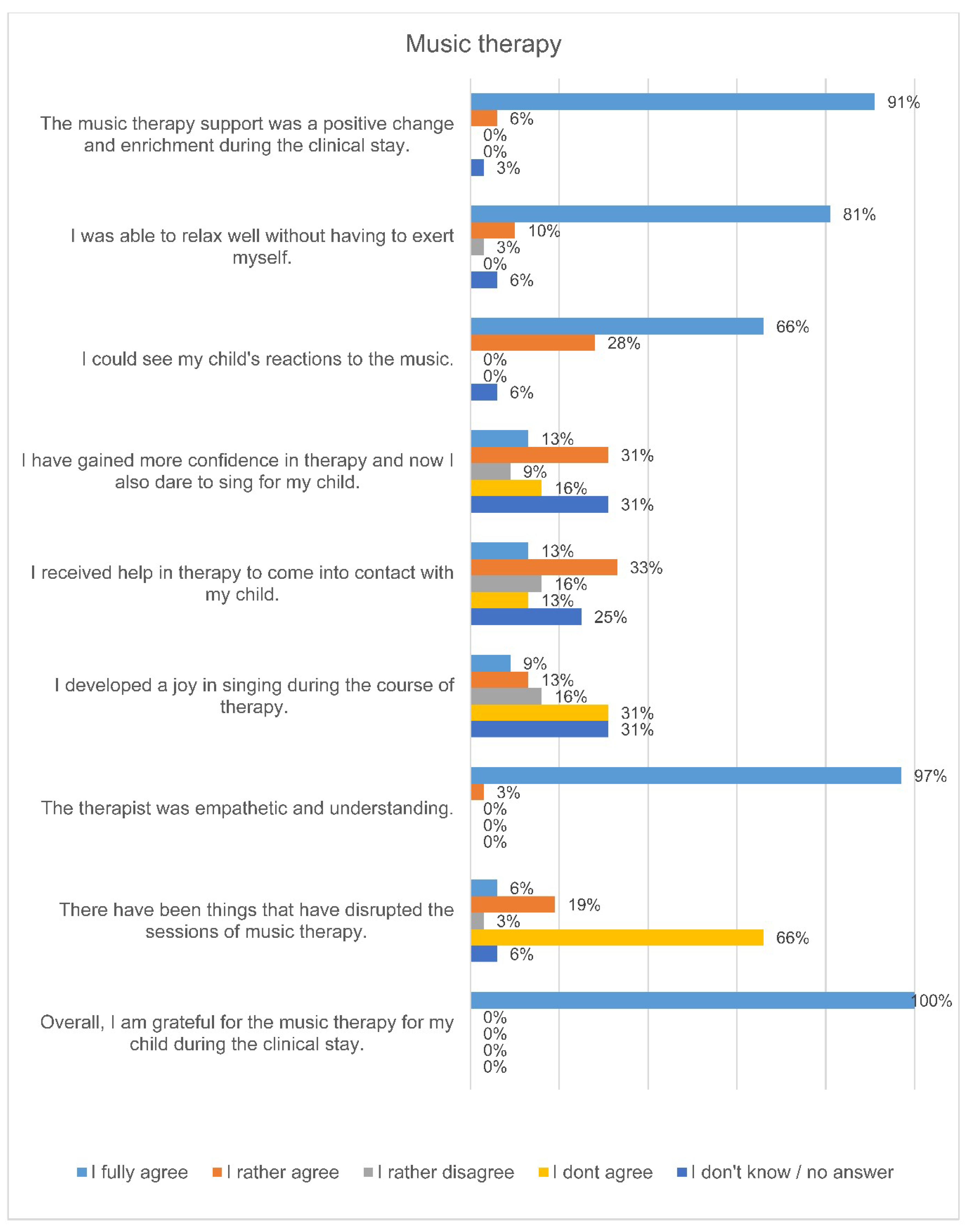
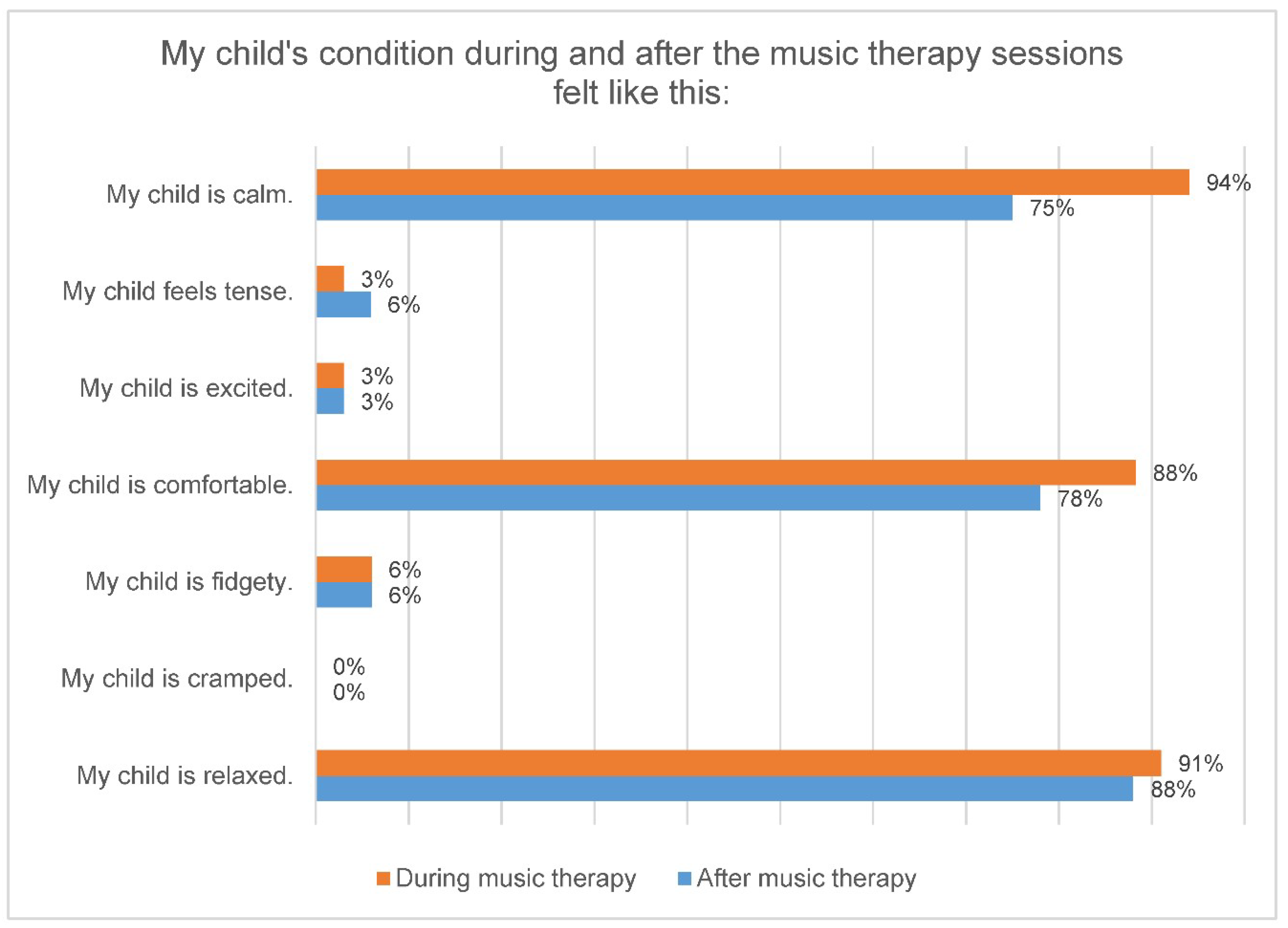
3.3. Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Liu, G.; Feng, Z.; Tan, X.; Yang, C.; Ye, X.; Dai, Y.; Liang, W.; Ye, X.; Mo, J.; et al. Short-term outcomes of extremely preterm infants at discharge: A multicenter study from Guangdong province during 2008–2017. BMC Pediatr. 2019, 19, 405. [Google Scholar] [CrossRef]
- Huening, B.M.; Reimann, M.; Sahlmen, S.; Leibold, S.; Nabring, J.C.; Felderhoff-Müser, U. Konzeptanalyse einer stationären und ambulanten psychosozialen familienzentrierten Betreuung in der Neonatologie in Zeiten des G-BA-Beschlusses. Klin. Padiatr. 2016, 228, 195–201. [Google Scholar] [CrossRef]
- Kobus, S. Musikalische Begleitung für Frühgeborene und ihre Familien. Reihe Zeitpunkt Musik; Dr. Ludwig Reichert Verlag: Wiesbaden, Germany, 2018. [Google Scholar]
- Haslbeck, F. Fortbildung Musik als Therapie auf der Frühgeborenenstation.“ Einführung und Orientierung”; Einführung und Orientierung: München, Germany, 2013. [Google Scholar]
- Bieleninik, L.; Ghetti, C.; Gold, C. Music Therapy for Preterm Infants and Their Parents: A Meta-analysis. Pediatrics 2016, 138, e20160971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haslbeck, F.B. Music therapy for premature infants and their parents: An integrative review. Nord. J. Music. Ther. 2012, 21, 203–226. [Google Scholar] [CrossRef]
- Standley, J.M. Music therapy research in the NICU: An updated meta-analysis. Neonatal Netw. 2012, 31, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Hartling, L.; Shaik, M.S.; Tjosvold, L.; Leicht, R.; Liang, Y.; Kumar, M. Music for medical indications in the neonatal period: A systematic review of randomised controlled trials. Arch. Dis. Child. Fetal Neonatal Ed. 2009, 94, F349–F354. [Google Scholar] [CrossRef]
- Loewy, J.; Stewart, K.; Dassler, A.-M.; Telsey, A.; Homel, P. The effects of music therapy on vital signs, feeding, and sleep in premature infants. Pediatrics 2013, 131, 902–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobus, S.; Diezel, M.; Dewan, M.V.; Huening, B.; Dathe, A.-K.; Felderhoff-Mueser, U.; Bruns, N. Music Therapy Is Effective during Sleep in Preterm Infants. Int. J. Environ. Res. Public Health 2021, 18, 8245. [Google Scholar] [CrossRef]
- Haslbeck, F.B.; Jakab, A.; Held, U.; Bassler, D.; Buchera, H.-U.; Hagmann, C. Creative music therapy to promote brain function and brain structure in preterm infants: A randomized controlled pilot study. NeuroImage Clin. 2020, 25, 102171. [Google Scholar] [CrossRef] [PubMed]
- Dudek-Shriber, L. Parent stress in the neonatal intensive care unit and the influence of parent and infant characteristics. Am. J. Occup. Ther. 2004, 58, 509–520. [Google Scholar] [CrossRef] [Green Version]
- Howe, T.-H.; Sheu, C.-F.; Wang, T.-N.; Hsu, Y.-W. Parenting stress in families with very low birth weight preterm infants in early infancy. Res. Dev. Disabil. 2014, 35, 1748–1756. [Google Scholar] [CrossRef] [PubMed]
- Baley, J. Skin-to-Skin Care for Term and Preterm Infants in the Neonatal ICU. Pediatr. Sept. 2015, 136, 596–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lüdin, C. Leidenschaft Vaterschaft. In Über die Bedeutung von Bindungsfördernden Elementen der Emotionalen Ersten Hilfe (EEH) für Väter, als Basis der Eltern-Kind-Bindung; Abschlussarbeit der Ausbildung zum Fachberater Emotionelle Erste Hilfe (EEH): Basel, Switzerland, 2014. [Google Scholar]
- Sarimski, K.; Porz, F. Frühgeborene nach der Entlassung. In Informationsbroschüre des Bundesverbandes “Das Frühgeborene Kind” e.V. Available online: http://www.fruehgeborene.de (accessed on 12 October 2021).
- Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Very preterm birth influences parental mental health and family outcomes seven years after birth. J. Pediatr. 2014, 164, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaari, M.; Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Preterm Birth and Maternal Mental Health: Longitudinal Trajectories and Predictors. J. Pediatr. Psychol. 2019, 44, 736–747. [Google Scholar] [CrossRef]
- Janus, L. Wie Die Seele Entsteht—Unser Psychisches Leben vor, Während und Nach der Geburt; Mattes Verlag: Heidelberg, Germany, 2011. [Google Scholar]
- Rose, S.A.; Feldman, J.F.; Jankowski, J.J.; Van Rossem, R. Pathways from prematurity and infant abilities to later cognition. Child Dev. 2005, 76, 1172–1184. [Google Scholar] [CrossRef]
- Papoušek, M. Vorwort. In Hören—Brücke ins Leben. Musiktherapie mit früh-und Neugeborenen Kindern. 7–11; Nöcker-Ribaupierre, M., Ed.; Vandenhoek & Ruprecht Verlag: Göttingen, Germany, 2012. [Google Scholar]
- Nöcker-Ribaupierre, M. Internationale musiktherapeutische Ansätze für frühgeborene Kinder. In Musiktherapeutische Umschau. Forschung und Praxis der Musiktherapie. Bd. 36,2; Vandenhoeck & Ruprecht GmbH & Co. KG.: Göttingen, Germany, 2015. [Google Scholar]
- Arnon, S.; Diamant, C.; Bauer, S.; Regev, R.; Sirota, G.; Litmanovitz, I. Maternal singing during kangaroo care led to autonomic stability in preterm infants and reduced maternal anxiety. Acta Paediatr. 2014, 103, 1039–1044. [Google Scholar] [CrossRef]
- Ribeiro, M.K.A.; Alcântara-Silva, T.R.M.; Oliveira, J.C.M.; Paula, T.C.; Dutra, J.B.R.; Pedrino, G.R.; Simões, K.; Sousa, R.B.; Rebelo, A.C.S. Music therapy intervention in cardiac autonomic modulation, anxiety, and depression in mothers of preterms: Randomized controlled trial. BMC Psychol. 2018, 6, 57. [Google Scholar] [CrossRef]
- Palazzi, A.; Meschini, R.; Piccinini, C.A. NICU music therapy effects on maternal mental health and preterm infant’s emotional arousal. Infant Ment. Health J. 2021, 42, 672–689. [Google Scholar] [CrossRef]
- Schlez, A.; Litmanovitz, I.; Bauer, S.; Dolfin, T.; Regev, R.; Arnon, S. Combining kangaroo care and live harp music therapy in the neonatal intensive care unit setting. Isr. Med. Assoc. J. 2011, 13, 354–358. [Google Scholar]
- Vianna, M.N.S.; Barbosa, A.P.; Carvalhaes, A.S.; Cunha, A.J.L.A. Music therapy may increase breastfeeding rates among mothers of premature newborns: A randomized controlled trial. J. Pediatr. (Rio J.) 2011, 87, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehl, S.M.; La Marca-Ghaemmaghami, P.; Haller, M.; Pichler-Stachl, E.; Bucher, H.U.; Bassler, D.; Haslbeck, F.B. Creative Music Therapy with Premature Infants and Their Parents: A Mixed-Method Pilot Study on Parents’ Anxiety, Stress and Depressive Symptoms and Parent-Infant Attachment. Int. J. Environ. Res. Public Health 2020, 18, 265. [Google Scholar] [CrossRef] [PubMed]
- Roa, E.; Ettenberger, M. Music Therapy Self-Care Group for Parents of Preterm Infants in the Neonatal Intensive Care Unit: A Clinical Pilot Intervention. Medicines 2018, 5, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Therapy Group (n = 40) | Control Group (n = 40) | |
|---|---|---|
| Male, n (%) | 22 (55%) | 18 (45%) |
| Gestational age (weeks), mean ± SD (range) | 28.6 ± 2.6 (23 + 6–31 + 5) | 28.8 ± 2.5 (22 + 6–31 + 6) |
| Birth weight (g), mean ± SD (range) | 1136 ± 404 (340–1790) | 1147 ± 396 (360–2120) |
| Twins, n (%) | 6 (15%) | 2 (5%) |
| Died, n (%) | 3 (8%) | 2 (5%) |
| n (%) | |
|---|---|
| Parent | |
| Father | 6 (19) |
| Mother | 24 (75) |
| Father and mother together | 2 (6) |
| Age (years) | |
| <25 | 3 (9) |
| 26 to 30 | 4 (13) |
| 31 to 40 | 24 (75) |
| >40 | 1 (3) |
| Education | |
| High school degree (13 years of education completed) | 21 (66) |
| Degree “Realschule” (9 years of education completed) | 5 (16) |
| Degree “Hauptschule” (8 years of education completed) | 3 (9) |
| Other degree | 1 (3) |
| No degree | 2 (6) |
| Current professional situation (multiple answers possible) | |
| Parental time | 25 (78) |
| Studying University/College | 4 (13) |
| Professional working | 7 (22) |
| Housewife/Houseman | 3 (9) |
| Native language | |
| German | 22 (69) |
| Other languages | 10 (31) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobus, S.; Diezel, M.; Huening, B.; Dewan, M.V.; Felderhoff-Mueser, U.; Bruns, N. Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants. Int. J. Environ. Res. Public Health 2021, 18, 12813. https://doi.org/10.3390/ijerph182312813
Kobus S, Diezel M, Huening B, Dewan MV, Felderhoff-Mueser U, Bruns N. Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants. International Journal of Environmental Research and Public Health. 2021; 18(23):12813. https://doi.org/10.3390/ijerph182312813
Chicago/Turabian StyleKobus, Susann, Marlis Diezel, Britta Huening, Monia Vanessa Dewan, Ursula Felderhoff-Mueser, and Nora Bruns. 2021. "Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants" International Journal of Environmental Research and Public Health 18, no. 23: 12813. https://doi.org/10.3390/ijerph182312813
APA StyleKobus, S., Diezel, M., Huening, B., Dewan, M. V., Felderhoff-Mueser, U., & Bruns, N. (2021). Parents’ Perception of Family-Centered Music Therapy with Stable Preterm Infants. International Journal of Environmental Research and Public Health, 18(23), 12813. https://doi.org/10.3390/ijerph182312813