
Perception of Stress and Styles of Coping with It in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU

 , and
, and
Abstract
1. Introduction
1.1. Transfer—Placing the Newborn into the KC Position (Kangaroo Care)
1.2. The Influence of KMC on the Behavior of the Newborn
1.3. The Influence of KMC on the Development and the Psychosocial Sphere
1.4. Aim
2. Materials and Methods
2.1. Design
2.2. Setting and Participants
2.3. Data Collection
2.4. Measurements
2.5. Data Analysis
2.6. Ethical Statement
3. Results
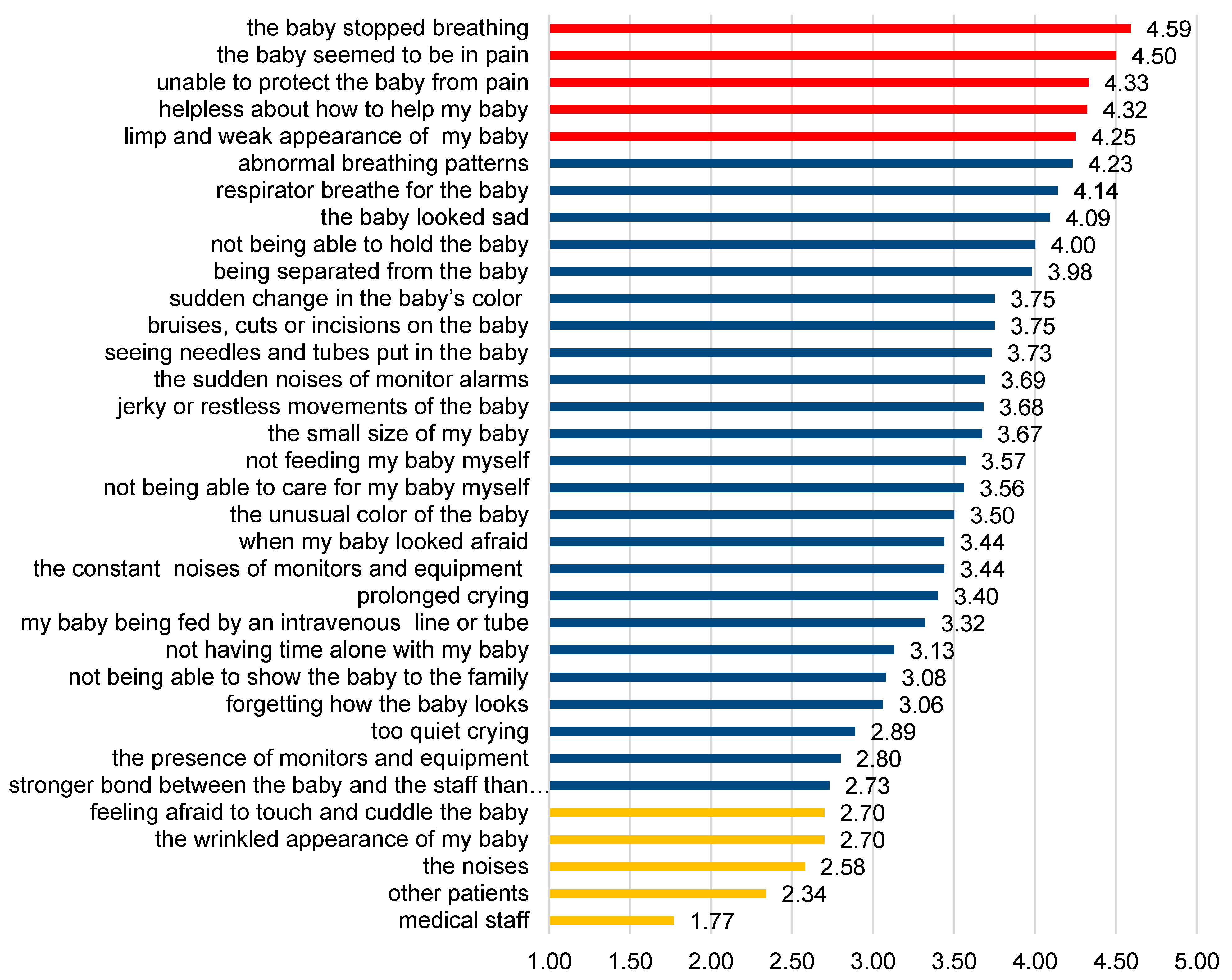
3.1. The Stress Parents Giving KMC to Their Children during Hospitalization in NICU
3.2. Coping Strategies in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parsa, P.; Karimi, S.; Basiri, B.; Roshanaei, G. The effect of kangaroo mother care on physiological parameters of premature infants in Hamadan City, Iran. Pan Afr. Med. J. 2018, 30, 89. [Google Scholar] [CrossRef] [PubMed]
- Als, H.; McAnulty, G.B. The Newborn Individualized Developmental Care and Assessment Program (NIDCAP) with Kangaroo Mother Care (KMC): Comprehensive Care for Preterm Infants. Curr. Women’s Health Rev. 2011, 7, 288–301. [Google Scholar] [CrossRef]
- Johnston, C.; Campbell-Yeo, M.; Fernandes, A.; Inglis, D.; Streiner, D.; Zee, R. Skin-to-skin care for procedural pain in neonates. Cochrane Database Syst. Rev. 2014, 1. [Google Scholar] [CrossRef]
- Anderson, G.C.; Moore, E.; Hepworth, J.; Bergman, N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst. Rev. 2003, 2. [Google Scholar] [CrossRef]
- Cong, X.; Ludington-Hoe, S.M.; McCain, G.; Fu, P. Kangaroo Care modifies preterm infant heart rate variability in response to heel stick pain: Pilot study. Early Hum. Dev. 2009, 85, 561–567. [Google Scholar] [CrossRef]
- Castral, T.C.; Warnock, F.F.; Ribeiro, L.M.; de Vasconcelos, M.G.; Leite, A.M.; Scochi, C.G. Maternal factors regulating preterm infants’ responses to pain and stress while in maternal kangaroo care. Revista Latino-Americana de Enfermagem 2012, 20, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Erlandsson, K.; Dsilna, A.; Fagerberg, I.; Christensson, K. Skin-to-skin care with the father after cesarean birth and its effect on newborn crying and prefeeding behavior. Birth 2007, 34, 105–114. [Google Scholar] [CrossRef]
- Johnston, C.C.; Filion, F.; Campbell-Yeo, M.; Goulet, C.; Bell, L.; McNaughton, K.; Byron, J.; Aita, M.; Finley, G.A.; Walker, D.-C. Kangaroo mother care diminishes pain from heel lance in very preterm neonates: A crossover trial. BMC Pediatr. 2008, 8, 13. [Google Scholar] [CrossRef]
- Boundy, E.O.; Dastjerdi, R.; Spiegelman, D.; Fawzi, W.W.; Missmer, S.A.; Lieberman, E.; Kajeepeta, S.; Wall, S.; Chan, G.J. Kangaroo mother care and neonatal outcomes: A meta-analysis. Pediatrics 2016, 137, 1–16. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Belizán, J.M.; Diaz-Rossello, J. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst. Rev. 2011, 3. [Google Scholar] [CrossRef]
- Widström, A.M.; Lilja, G.; Aaltomaa-Michalias, P.; Dahllöf, A.; Lintula, M.; Nissen, E. Newborn behaviour to locate the breast when skin-to-skin: A possible method for enabling early self-regulation. Acta Paediatr. 2011, 100, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Heidarzadeh, M.; Hosseini, M.B.; Ershadmanesh, M.; Gholamitabar, M.; Tabari, G.; Khazaee, S. The Effect of Kangaroo Mother Care (KMC) on Breast Feeding at the Time of NICU Discharge. Iran. Red Crescent Med. J. 2013, 15, 302–306. [Google Scholar] [CrossRef]
- Moore, E.R.; Bergman, N.; Anderson, G.C.; Medley, N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database Syst Rev. 2016, 11. [Google Scholar] [CrossRef]
- Holditch-Davis, D.; White-Traut, R.C.; Levy, J.A.; O’Shea, T.M.; Geraldo, V.; David, R.J. Maternally administered interventions for preterm infants in the NICU: Effects on maternal psychological distress and mother-infant relationship. Infant Behav. Dev. 2014, 37, 695–710. [Google Scholar] [CrossRef]
- Charpak, N.; Ruiz, J.G.; Zupan, J.; Cattaneo, A.; Figueroa, Z.; Tessier, R.; Cristo, M.; Anderson, G.; Ludington, S.; Mendoza, S.; et al. Kangaroo Mother Care: 25 years after. Acta Paediatr. 2005, 94, 514–522. [Google Scholar] [CrossRef]
- DiPietro, J.A.; Goldshore, M.A.; Kivlighan, K.T.; Pater, H.A.; Costigan, K.A. The ups and downs of early mothering. J. Psychosom. Obstet. Gynaecol. 2015, 36, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.S.; Carter, M.C.; Riddle, I.; Hennessey, J.; Eberly, T.W. The pediatric intensive care unit environment as a source of stress for parents. Matern. Child Nurs. J. 1989, 18, 199–206. [Google Scholar] [PubMed]
- Escartí, A.; Boronat, N.; Llopis, R.; Torres, R.; Vento, M. Pilot study on stress and resilience in families with premature newborns. Anales de Pediatría 2016, 84, 3–9. [Google Scholar] [CrossRef]
- Schappin, R.; Wijnroks, L.; Uniken Venema, M.M.; Jongmans, M.J. Rethinking stress in parents of preterm infants: A meta-analysis. PLoS ONE 2013, 8, e54992. [Google Scholar]
- Kadivar, M.; Seyedfatemi, N.; Akbari, N.; Haghani, H.; Fayaz, M. Evaluation of the effect of narrative writing on the stress sources of the parents of preterm neonates admitted to the NICU. J. Matern. Fetal Neonatal Med. 2017, 30, 1616–1620. [Google Scholar] [CrossRef]
- Aghdas, K.; Talat, K.; Sepideh, B. Effect of immediate and continuous mother-infant skin-to-skin contact on breastfeeding self-efficacy of primiparous women: A randomised control trial. Women Birth 2017, 27, 37–40. [Google Scholar] [CrossRef]
- Hake-Brooks, S.J.; Anderson, G.C. Kangaroo care and breastfeeding of mother-preterm infant dyads 0-18 months: A randomized, controlled trial. Neonatal Netw. 2008, 27, 151–159. [Google Scholar] [CrossRef]
- Mahmood, I.; Jamal, M.; Khan, N. Effect of mother-infant early skin-to-skin contact on breastfeeding status: A randomized controlled trial. J. Coll. Physicians Surg. Pak. 2011, 21, 601–605. [Google Scholar] [PubMed]
- Baylis, R.; Ewald, U.; Gradin, M.; Hedberg Nyqvist, K.; Rubertsson, C.; Thernström Blomqvist, Y. First-time events between parents and preterm infants are affected by the designs and routines of neonatal intensive care units. Acta Paediatr. 2014, 103, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Vogl, J.L.; Dunne, E.C.; Liu, C.; Bradley, A.; Rwei, A.; Lonergan, E.K.; Hopkins, B.S.; Kwak, S.S.; Simon, C.D.; Rand, C.M.; et al. Kangaroo father care: A pilot feasibility study of physiologic, biologic, and psychosocial measures to capture the effects of father-infant and mother-infant skin-to-skin contact in the Neonatal Intensive Care Unit. Dev. Psychobiol. 2021, 63, 1521–1533. [Google Scholar] [CrossRef]
- Mu, P.F.; Lee, M.Y.; Chen, Y.C.; Yang, H.C.; Yang, S.H. Experiences of parents providing kangaroo care to a premature infant: A qualitative systematic review. Nurs. Health Sci. 2020, 22, 149–161. [Google Scholar] [CrossRef]
- Kumar, D. Living with a Disabled: A Study of Cognitive Emotion Regulation of Siblings & Mothers of Disabled Children. IJSSIR 2015, 4, 80–85. [Google Scholar]
- Sharp, H.; Hill, J.; Hellier, J.; Pickles, A. Maternal antenatal anxiety, postnatal stroking and emotional problems in children: Outcomes predicted from pre- and postnatal programming hypotheses. Psychol. Med. 2015, 45, 269–283. [Google Scholar] [CrossRef]
- Mohammed, I.; Yacoub Muna, S.; Alkharabsheh Rasha, S.; Abu Zaitoun Ensherah, K.; Al-Atiat, K. The Arabic version of the Parental Stressor Scale: Psychometric properties and Jordanian parents’ stress during child admission to PICU. J. Res. Nurs. 2013, 18, 619–633. [Google Scholar]
- Rozkrut, D. (Ed.) . Demographic Yearbook of Poland; Central Statistical Office: Warsaw, Poland, 2020.
- Miles, M.S.; Funk, S.G.; Carlson, J. Parental Stressor Scale: Neonatal Intensive Care Unit. Nursing 1993, 42, 148–152. [Google Scholar] [CrossRef]
- Endler, N.S.; Parker, J.D.A. Coping Inventory for Stressful Situations (CISS): Manual; Multi-Health Systems, Inc.: Toronto, ON, Canada, 1990. [Google Scholar]
- Libera, A.; Leszczyńska-Gorzelak, B.; Oleszczuk, J. Applicability of the Polish equivalent of Neonatal Unit Parental Stress Scale [SSR: OITN] in clinical diagnosis of women after preterm delivery. Pol. Gynecol. 2013, 84, 281–285. [Google Scholar]
- Aftyka, A.; Rozalska, I.; Rybojad, B.; Samardakiewicz, M.E. Polish version of the Parental Stressor Scale: Neonatal Intensive Care Unit. Ann. Agric. Environ. Med. 2019, 26, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Endler, N.S.; Parker, J.D.A. Multidimensional assessment of coping: A critical evaluation. J. Personal. Soc. Psychol. 1990, 58, 844–854. [Google Scholar] [CrossRef]
- Strelau, J.; Jaworowska, A.; Wrześniewski, K.; Szczepania, P. Kwestionariusz Radzenia Sobie w Sytuacjach Stresowych CISS. Podręcznik; [Parental Stress Scale: Neonatal Intensive Care Unit]; Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego: Warsaw, Poland, 2013. (In Polish) [Google Scholar]
- Kumar, B.S.; Avabratha, K.S. Parental stress: A study from a pediatric intensive care unit in Mangalore. Int. J. Contemp. Ped. 2015, 2, 401–405. [Google Scholar] [CrossRef]
- Miles, M.S.; Burchinal, P.; Holditch-Davis, D.; Brunssen, S.; Wilson, S.M. Perceptions of stress, worry, and support in Black and White mothers of hospitalized, medically fragile infants. J. Pediatr. Nurs. 2002, 17, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Diffin, J.; Spence, K.; Naranian, T.; Badawi, N.; Johnston, J. Stress and distress in parents of neonates admitted to the neonatal intensive care unit for cardiac surgery. Early Hum. Dev. 2016, 103, 101–107. [Google Scholar] [CrossRef]
- Miles, M.S.; Mathes, M. Preparation of parents for the ICU experience: What are we missing? Child Health Care 1991, 20, 132–137. [Google Scholar] [CrossRef]
- Valizadeh, L.; Hosseini, M.B.; Heydarpoor Damanabad, Z.; Rahkar Farshi, M.; Asgari Jafarabadi, M.; Ranjbar Kochaksaraie, F. Effect of NICU Department Orientation Program on Mother’s Anxiety: A Randomized Clinical Trial. J. Caring Sci. 2016, 5, 205–214. [Google Scholar] [CrossRef]
- Bouet, K.M.; Claudio, N.; Ramirez, V.; García-Fragoso, L. Loss of parental role as a cause of stress in the neonatal intensive care unit. Boletin de la Asociacion Medica de Puerto Rico 2012, 104, 8–11. [Google Scholar]
- Dudek-Shriber, L. Parent stress in the neonatal intensive care unit and the influence of parent and infant characteristics. Am. J. Occup. Ther. 2004, 58, 509–520. [Google Scholar] [CrossRef]
- Turan, T.; Başbakkal, Z.; Ozbek, S. Effect of nursing interventions on stressors of parents of premature infants in neonatal intensive care unit. J. Clin. Nurs. 2008, 17, 2856–2866. [Google Scholar] [CrossRef]
- Lazarus, R.S. From Psychological Stress to the Emotions: A History of Changing Outlooks. Annu. Rev. Psychol. 1993, 44, 1–21. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1986. [Google Scholar]
- Rogers, C.E.; Kidokoro, H.; Wallendorf, M.; Inder, T.E. Identifying Mothers of Very Preterm Infants At-risk for Postpartum Depression and Anxiety Prior to Discharge. J. Perinatol. 2013, 33, 171–176. [Google Scholar] [CrossRef]
- Mariańczyk, K.; Libera, A.; Oleszczuk, J. The feeling of hopelessness and ways of coping with stress in women after preterm delivery. Pol. Gynecol. 2010, 81, 342–346. [Google Scholar]
- Bucholc, M.; Kucharczyk, G.C.; Kanadys, K.; Wiktor, K.; Wiktor, H. Selected determinants of strategies to cope with the disease among women treated for gynecological cancer. Pol. J. Public Health 2016, 126, 161–164. [Google Scholar] [CrossRef]
- Raina, P.; O’Donnell, M.; Schwellnus, H.; Rosenbaum, P.; King, G.; Brehaut, J.; Russell, D.; Swinton, M.; King, S.; Wong, M.; et al. Caregiving process and caregiver burden: Conceptual models to guide research and practice. BMC Ped. 2004, 4, 1. [Google Scholar] [CrossRef]
- Ghorbani, M.; Dolatian, M.; Shams, J.; Alavi-Majd, H.; Tavakolian, S. Factors associated with posttraumatic stress disorder and its coping styles in parents of preterm and full-term infants. Glob. J. Health Sci. 2014, 6, 65–73. [Google Scholar] [CrossRef]
- Raina, P.; O’Donnell, M.; Rosenbaum, P.; Brehaut, J.; Walter, S.D.; Russell, D.; Swinton, M.; Zhu, B.; Wood, E. The health and well-being of caregivers of children with cerebral palsy. Pediatrics 2005, 115, e626–e636. [Google Scholar] [CrossRef]
- Ospina Romero, A.M.; Muñoz de Rodríguez, L.; Ruiz de Cárdenas, C.H. Coping and adaptation process during puerperium. Colomb. Med. 2012, 43, 167–174. [Google Scholar] [CrossRef]
- Cattell, R.B. Personality structure and measurement II: The determination and utility of trait modality. Br. J. Psychol. 2009, 100, 233–248, Reprinted from Br. J. Psychol. 1946, 36, 159–174. [Google Scholar] [CrossRef]
- Carnevale, F.A.; Alexander, E.; Davis, M.; Rennick, J.; Troini, R. Daily living with distress and enrichment: The moral experience of families with ventilator-assisted children at home. Pediatrics 2006, 117, e48–e60. [Google Scholar] [CrossRef]
- Holditch-Davis, D.; White-Traut, R.; Levy, J.; Williams, K.L.; Ryan, D.; Vonderheid, S. Maternal satisfaction with administering infant interventions in the neonatal intensive care unit. J. Obstet. Gynecol. Neonat. Nurs. 2013, 42, 641–654. [Google Scholar] [CrossRef][Green Version]
- Harrison, M.S.; Goldenberg, R.L. Global burden of prematurity. Semin. Fetal Neonatal. Med. 2016, 21, 74–79. [Google Scholar] [CrossRef]


{kind=link}
| Sociodemographic Data of the Tested Parents | n, (%) | |
| Gender | Female | 261, (77.4) |
| Male | 76, (22.6) | |
| Age | ≤24 yrs | 38, (11.3) |
| 25–34 yrs | 232, (68.8) | |
| ≥35 yrs | 67, (19.9) | |
| Education | Secondary education | 147, (43.6) |
| Higher | 190, (56.4) | |
| Clinical Data of the Course of the Present Pregnancy | n, (%) | |
| Conditions coexisting with the pregnancy | Yes | 96, (28.5) |
| No | 241, (71.5) | |
| Ailments resulting from conditions coexisting with the pregnancy | Yes | 130, (38.6) |
| No | 207, (61.4) | |
| Hospitalizations in pregnancy | Yes | 227, (67.4) |
| No | 110, (32.6) | |
| Number of hospitalizations in pregnancy | One | 123, (54.2) |
| Two | 67, (29.5) | |
| Three or more | 37, (16.3) | |
| Delivery method | Vaginal birth | 59, (17.1) |
| Caesarean section | 278, (82.9) | |
| Sociodemographic and Clinical Data of the Infant | ||
| Infant’s gender | Female | 217, (54.5) |
| Male | 181, (45.5) | |
| Single vs. Multiple Pregnancy | Single Pregnancy | 279, (82.8) |
| Multiple Pregnancy: twins | 58, (17.2) | |
| Week of pregnancy completion | <29 | 107, (26.9) |
| 29–32 | 161, (40.4) | |
| 33–36 | 111, (27.9) | |
| >36 | 19, (4.8) | |
| Body weight at birth | <1000 g | 75, (18.8) |
| 1000–1499 g | 93, (23.4) | |
| 1500–2499 g | 161, (40.4) | |
| ≥2500 g | 69, (17.4) | |
| Body length n, (x ± SD) | 23–63 cm | 398, (44.00 ± 7.88 cm) |
| Apgar score n, (x ± SD) | 1st minute | 304, (5.71 ± 3.16 pts) |
| 3rd minute | 188, (5.21 ± 3.27 pts) | |
| 5th minute | 217, (6.01 ± 3.31 pts) | |
| 10th minute | 203, (6.28 ± 3.49 pts) | |
| Data on Undertaking KMC in Parents | n, (%) | |
| Undertaking KMC | Yes | 298, (88.4) |
| No | 39, (11.6) | |
| KMC Initiation | Week 1 of infant’s life | 194, (65.1) |
| Week 2–3 of infant’s life | 104, (34.9) | |
| KMC Frequency | Daily | 167, (56.0) |
| Intermittently | 131, (44.0) | |
| PSS-NICU and KMC | Parents Giving KMC | Parents Not Giving KMC | p | ||||
| Me | SD | Me | SD | ||||
|---|---|---|---|---|---|---|---|
| Subscale I | 2.85 | 2.83 | 0.86 | 2.45 | 2.42 | 0.94 | 0.006 * |
| Subscale II | 3.67 | 3.82 | 0.89 | 3.38 | 3.38 | 1.01 | 0.093 |
| Subscale III | 3.58 | 3.70 | 0.95 | 3.33 | 3.27 | 1.08 | 0.198 |
| The general level of stress in parents: | 3.35 | 3.39 | 0.77 | 3.07 | 2.97 | 0.91 | 0.056 |
| PSS-NICU and KMC Initiation | KMC from Week 1 of Infant’s Life | KMC from Week 2 of Infant’s Life | p | ||||
| Me | SD | Me | SD | ||||
| Subscale I | 2.75 | 2.80 | 0.89 | 2.98 | 3.00 | 0.74 | 0.050 |
| Subscale II | 3.59 | 3.76 | 0.95 | 3.75 | 3.88 | 0.78 | 0.254 |
| Subscale III | 3.49 | 3.44 | 1.00 | 3.72 | 3.88 | 0.82 | 0.058 |
| The general level of stress in parents: | 3.26 | 3.31 | 0.80 | 3.48 | 3.50 | 0.66 | 0.022 * |
| PSS-NICU and KMC Frequency | KMC Daily | KMC Intermittently | p | ||||
| Me | SD | Me | SD | ||||
| Subscale I | 2.84 | 2.83 | 0.86 | 2.84 | 2.83 | 0.85 | 0.975 |
| Subscale II | 3.68 | 3.82 | 0.87 | 3.64 | 3.75 | 0.90 | 0.653 |
| Subscale III | 3.57 | 3.67 | 0.94 | 3.60 | 3.73 | 0.95 | 0.781 |
| The general level of stress in parents: | 3.35 | 3.36 | 0.76 | 3.34 | 3.42 | 0.76 | 0.908 |
| Evaluation of the Stress Coping Strategy | Low 1–4 STEN | Average 5–6 STEN | High 7–10 STEN | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Task-Oriented Coping | 63 | 18.7 | 129 | 38.3 | 145 | 43.0 |
| Emotion-Oriented Coping | 103 | 30.6 | 217 | 64.4 | 17 | 5.0 |
| Avoidance-Oriented Coping | 208 | 61.7 | 89 | 26.4 | 40 | 11.9 |
| search for social contacts | 171 | 50.7 | 101 | 30.0 | 65 | 19.3 |
| engaging in substitute activities | 91 | 27.0 | 155 | 46.0 | 91 | 27.0 |
| CISS and KMC | Parents Giving KMC | Parents Not Giving KMC | p | ||||
| Me | SD | Me | SD | ||||
|---|---|---|---|---|---|---|---|
| Task-Oriented Coping | 59.78 | 60.00 | 8.77 | 60.77 | 62.00 | 9.49 | 0.340 |
| Emotion-Oriented Coping | 42.30 | 42.50 | 10.10 | 41.87 | 42.00 | 12.12 | 0.721 |
| Avoidance-Oriented Coping | 38.03 | 37.50 | 8.04 | 36.92 | 35.00 | 8.55 | 0.218 |
| search for social contacts | 16.34 | 16.00 | 5.57 | 15.36 | 14.00 | 5.71 | 0.188 |
| engaging in substitute activities | 16.64 | 16.00 | 3.46 | 16.18 | 17.00 | 3.36 | 0.496 |
| CISS and KMC Initiation | KMC from Week 1 of Baby’s Life | KMC from Week 2 of Baby’s Life | p | ||||
| Me | SD | Me | SD | ||||
| Task-Oriented Coping | 59.90 | 60.00 | 8.86 | 59.59 | 60.00 | 8.61 | 0.913 |
| Emotion-Oriented Coping | 42.18 | 42.00 | 10.75 | 41.97 | 44.00 | 9.30 | 0.985 |
| Avoidance-Oriented Coping | 38.48 | 38.00 | 8.45 | 36.78 | 36.00 | 7.40 | 0.101 |
| search for social contacts | 16.74 | 16.00 | 5.83 | 15.36 | 15.00 | 5.12 | 0.065 |
| engaging in substitute activities | 16.71 | 17.00 | 3.61 | 16.27 | 16.00 | 3.27 | 0.150 |
| CISS and KMC Frequency | KMC Every Day | KMC Intermittently | p | ||||
| Me | SD | Me | SD | ||||
| Task-Oriented Coping | 60.08 | 60.00 | 8.95 | 59.71 | 60.00 | 8.56 | 0.807 |
| Emotion-Oriented Coping | 41.99 | 42.00 | 10.54 | 42.47 | 43.00 | 9.38 | 0.545 |
| Avoidance-Oriented Coping | 37.54 | 37.00 | 7.87 | 38.75 | 38.00 | 8.44 | 0.219 |
| seeking social contacts | 15.98 | 16.00 | 5.54 | 16.83 | 16.00 | 5.69 | 0.246 |
| engaging in substitute activities | 16.57 | 16.00 | 3.57 | 16.72 | 17.00 | 3.41 | 0.677 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zych, B.; Błaż, W.; Dmoch-Gajzlerska, E.; Kanadys, K.; Lewandowska, A.; Nagórska, M. Perception of Stress and Styles of Coping with It in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU. Int. J. Environ. Res. Public Health 2021, 18, 12694. https://doi.org/10.3390/ijerph182312694
Zych B, Błaż W, Dmoch-Gajzlerska E, Kanadys K, Lewandowska A, Nagórska M. Perception of Stress and Styles of Coping with It in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU. International Journal of Environmental Research and Public Health. 2021; 18(23):12694. https://doi.org/10.3390/ijerph182312694
Chicago/Turabian StyleZych, Barbara, Witold Błaż, Ewa Dmoch-Gajzlerska, Katarzyna Kanadys, Anna Lewandowska, and Małgorzata Nagórska. 2021. "Perception of Stress and Styles of Coping with It in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU" International Journal of Environmental Research and Public Health 18, no. 23: 12694. https://doi.org/10.3390/ijerph182312694
APA StyleZych, B., Błaż, W., Dmoch-Gajzlerska, E., Kanadys, K., Lewandowska, A., & Nagórska, M. (2021). Perception of Stress and Styles of Coping with It in Parents Giving Kangaroo Mother Care to Their Children during Hospitalization in NICU. International Journal of Environmental Research and Public Health, 18(23), 12694. https://doi.org/10.3390/ijerph182312694