
Economic Evaluation of Community Tuberculosis Active Case-Finding Approaches in Cambodia: A Quasi-Experimental Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
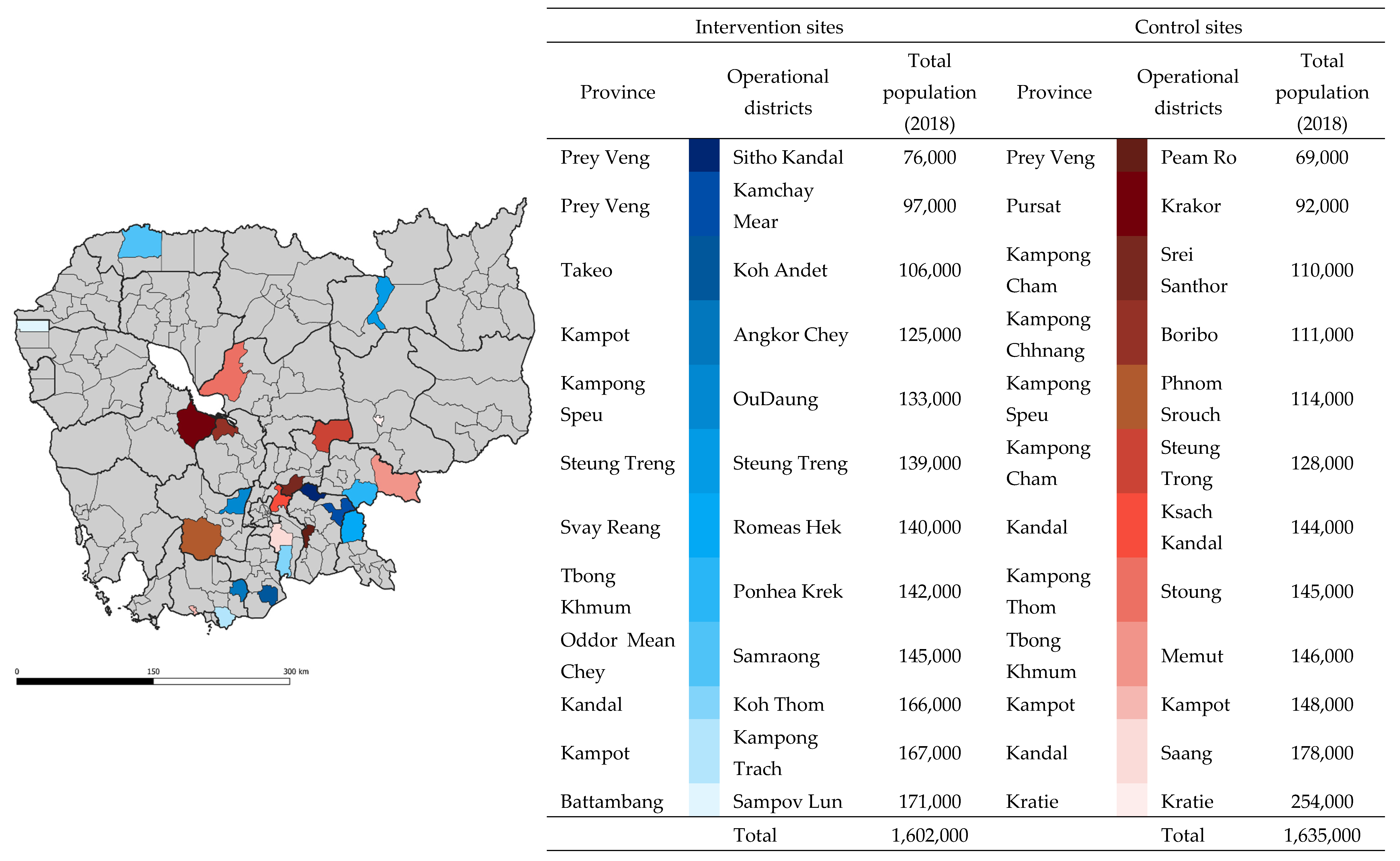
2.1. Study Setting and Population
2.2. Description of the ACF Models
2.3. ACF SAR Model
2.4. One-Off ACF
2.5. Description of the PCF Model
2.6. Program and Health System Costs
2.6.1. Costs of ACF Interventions
2.6.2. Cost of PCF
2.7. Study Outcomes
2.8. Cost-Effectiveness Model Descriptions and Assumptions
2.9. Years Lost due to Disability (YLD)
2.10. Years of Life Lost (YLL)
2.11. Data Analyses
2.11.1. Primary Analyses
2.11.2. Sensitivity Analyses
3. Results
3.1. Comparison of Intervention and Control Sites
3.2. TB Case Detection, the Number People with Presumptive TB Needed to Be Screened and Tested to Find One Person with TB
3.3. Costs of Interventions and Control
3.4. Cost per TB Diagnosis, DALYs, and ICER
3.5. Sensitivity Analyses: Costs of PCF, Diagnostics and Medical Procedures, and Treatment/C-DOTS
3.6. Sensitivity Analyses: Variation of YLL, Undetected Cases in the Control Sites, and Disability Weights
3.7. Probabilistic Sensitivity Analyses: Costs of PCF, Diagnostics and Medical Procedures, and C-DOTS, Variation of YLL, Undetected Cases in the Control Sites, and Disability Weights
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240037021 (accessed on 25 September 2021).
- World Health Organization. TB Country Profile: Cambodia; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Stop TB Partnership, United Nations Office for Project Services (UNOPS). 90-90-90. In The Tuberculosis Report for Heads of State and Governments; Stop TB Partnership and UNOPS: Geneva, Switzerland, 2017.
- Department of Planning and Health Information. Health Information System Master Plan 2016–2020; Ministry of Planning: Phnom Penh, Cambodia, 2017; Available online: http://hismohcambodia.org/public/fileupload/carousel/HIS-MasterPlan-Nov2017.pdf (accessed on 25 September 2021).
- World Health Organization. WHO Releases New Global Lists of High-Burden Countries for TB, HIV-Associated TB and Drug-Resistant TB. 2021. Available online: https://www.who.int/news/item/17-06-2021-who-releases-new-global-lists-of-high-burden-countries-for-tb-hiv-associated-tb-and-drug-resistant-tb (accessed on 14 November 2021).
- Teo, A.K.J.; Ork, C.; Eng, S.; Sok, N.; Tuot, S.; Hsu, L.Y.; Yi, S. Determinants of delayed diagnosis and treatment of tuberculosis in Cambodia: A mixed-methods study. Infect. Dis. Poverty 2020, 9, 49. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Fox, G.J.; Marais, B.J. Passive Case Finding for Tuberculosis is not Enough. Int. J. Mycobact. 2016, 5, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Teo, A.K.J.; Prem, K.; Tuot, S.; Ork, C.; Eng, S.; Pande, T.; Chry, M.; Hsu, L.Y.; Yi, S. Mobilising Community Networks for Early Identification of Tuberculosis and Treatment Initiation in Cambodia: An Evaluation of a Seed-and-Recruit Model. ERJ Open Research. ERJ Open Res. 2020, 6, 00368–2019. Available online: https://openres.ersjournals.com/content/6/2/00368-2019 (accessed on 4 May 2020). [CrossRef]
- Tuot, S.; Teo, A.K.J.; Cazabon, D.; Sok, S.; Ung, M.; Ly, S.; Choub, S.C.; Yi, S. Acceptability of active case finding with a seed-and-recruit model to improve tuberculosis case detection and linkage to treatment in Cambodia: A qualitative study. PLoS ONE 2019, 14, e0210919. [Google Scholar] [CrossRef] [PubMed]
- Camelique, O.; Scholtissen, S.; Dousset, J.-P.; Bonnet, M.; Bastard, M.; Hewison, C. Mobile community-based active case-finding for tuberculosis among older populations in rural Cambodia. Int. J. Tuberc. Lung Dis. 2019, 23, 1107–1114. [Google Scholar] [CrossRef]
- James, R.; Khim, K.; Boudarene, L.; Yoong, J.; Phalla, C.; Saint, S.; Koeut, P.; Mao, T.E.; Coker, R.; Khan, M.S. Tuberculosis Active case finding in Cambodia: A Pragmatic, Cost-Effectiveness Comparison of Three Implementation Models. BMC Infect. Dis. 2017, 17, 1–7. Available online: http://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-017-2670-8 (accessed on 15 January 2018). [CrossRef]
- Yadav, R.P.; Nishikiori, N.; Satha, P.; Eang, M.T.; Lubell, Y. Cost-effectiveness of a tuberculosis active case finding program targeting household and neighborhood contacts in Cambodia. Am. J. Trop. Med. Hyg. 2014, 90, 866–872. [Google Scholar] [CrossRef]
- Jo, Y.; Mirzoeva, F.; Chry, M.; Qin, Z.Z.; Codlin, A.; Bobokhojaev, O.; Creswell, J.; Sohn, H. Standardized framework for evaluating costs of active case-finding programs: An analysis of two programs in Cambodia and Tajikistan. PLoS ONE 2020, 15, e0228216. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0228216 (accessed on 19 July 2020). [CrossRef]
- Eang, M.T.; Satha, P.; Yadav, R.P.; Morishita, F.; Nishikiori, N.; Van-Maaren, P.; Weezenbeek, C.L.-V. Early Detection of Tuberculosis through Community-Based Active Case Finding in Cambodia. BMC Public Health 2012, 12, 469. Available online: http://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-12-469 (accessed on 17 July 2018). [CrossRef]
- Teo, A.K.J.; Prem, K.; Evdokimov, K.; Ork, C.; Eng, S.; Tuot, S.; Chry, M.; Mao, T.E.; Hsu, L.Y.; Yi, S. Effect of Community Active Case-Finding Strategies for Detection of Tuberculosis in Cambodia: Study Protocol for a Pragmatic Cluster Randomized Controlled Trial. Trials 2020, 21, 1–15. Available online: https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-020-4138-1 (accessed on 25 February 2020). [CrossRef] [PubMed]
- National Center for Tuberculosis and Leprosy Control (CENAT). Technical Guidelines on Tuberculosis Control, 2nd ed.; Ministry of Health: Phnom Penh, Cambodian, 2016. [Google Scholar]
- Yi, S.; Teo, A.K.J.; Sok, S.; Tuot, S.; Tieng, S.; Khun, K.E.; Choub, S.C.; Pheng, S.H.; Mao, T.E. Barriers in Access to Services and Information Gaps by Genders and Key Populations in the National Tuberculosis Programme in Cambodia. Glob. Public Health 2021, 1–14. Available online: https://www.tandfonline.com/doi/full/:10.1080/17441692.2021.1954226 (accessed on 25 September 2021).
- Pallas, S.; Courey, M.; Hy, C.; Killam, W.P.; Warren, D.; Moore, B. Cost Analysis of Tuberculosis Diagnosis in Cambodia with and without Xpert® MTB/RIF for People Living with HIV/AIDS and People with Presumptive Multidrug-resistant Tuberculosis. Appl. Health Econ. Health Policy 2018, 16, 537–548. [Google Scholar] [CrossRef]
- World Bank. Cambodia Consumer Price Index. 2020. Available online: https://data.worldbank.org/indicator/FP.CPI.TOTL?locations=KH (accessed on 19 July 2020).
- World Health Organization. TB Country Profile: Cambodia; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- York Health Economics Consortium. Incremental Cost-Effectiveness Ratio (ICER). YHEC—York Health Economics Consortium. 2016. Available online: https://yhec.co.uk/glossary/incremental-cost-effectiveness-ratio-icer/ (accessed on 26 July 2020).
- World Health Organization. Metrics: Disability-Adjusted Life Year (DALY). WHO World Health Organization. 2014. Available online: https://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/ (accessed on 24 July 2020).
- Salomon, J.A.; Haagsma, J.A.; Davis, A.; de Noordhout, C.M.; Polinder, S.; Havelaar, A.H.; Cassini, A.; Devleesschauwer, B.; Kretzschmar, M.; Speybroeck, N.; et al. Disability weights for the Global Burden of Disease 2013 study. Lancet Glob. Health 2015, 3, e712–e723. Available online: https://www.thelancet.com/journals/langlo/article/PIIs2214-109x(15)00069-8/abstract (accessed on 26 July 2020). [CrossRef]
- Prem, K.; Pheng, S.H.; Teo, A.K.J.; Evdokimov, K.; Nang, E.E.K.; Hsu, L.Y.; Saphonn, V.; Tieng, S.; Mao, T.E.; Cook, A. Spatial and Temporal Projections of the Prevalence of Active Tuberculosis in Cambodia. BMJ Glob. Health 2019, 4, e001083. Available online: https://gh.bmj.com/content/4/gh-201/e8-001083 (accessed on 18 April 2019). [CrossRef]
- World Health Organization. Life Tables by Country: Cambodia. WHO World Health Organization.. 2016. Available online: https://apps.who.int/gho/data/view.main.60270 (accessed on 25 July 2020).
- Hoa, N.B.; Sokun, C.; Wei, C.; Lauritsen, J.; Rieder, H.L. Time to unsuccessful tuberculosis treatment outcome, Cambodia, China, and Viet Nam. Public Health Action 2012, 2, 15–20. Available online: https://www.ncbi.nlm.nih.gov5588/pmc/harticles/PMC.11.0024536555/ (accessed on 25 July 2020). [CrossRef][Green Version]
- World Bank. Life Expectancy at Birth, Total (years): Cambodia. 2019. Available online: https://data.worldbank.org/indicator/SP.DYN.LE00.IN?locations=KH (accessed on 25 July 2020).
- World Health Organization. Macroeconomics and Health: Investing in Health for Economic Development: Report of the Commission on Macroeconomics and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.-P. Cost–effectiveness Thresholds: Pros and Cons. Bull. World Health Organ. 2016, 94, 925–930. Available online: http://www.who.int/entity/bulletin/volumes/94/12/15-164418.pdf (accessed on 27 July 2020). [CrossRef]
- World Bank. GDP Per Capita (Current US$): Cambodia. 2020. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD?locations=KH (accessed on 26 July 2020).
- United States Department of Labor, Bureau of Labor Statistics. CPI Inflation Calculator. 2020. Available online: https://www.bls.gov/data/inflation_calculator.htm (accessed on 22 January 2021).
- Ochalek, J.; Lomas, J.; Claxton, K. Estimating Health Opportunity Costs in Low-Income and Middle-Income Countries: A Novel Approach and Evidence from Cross-Country Data. BMJ Glob. Health 2018, 3, e000964. Available online: https://gh.bmj.com/content/3/6/egh-2018-000964 (accessed on 26 July 2020). [CrossRef]
- Pichenda, K.; Nakamura, K.; Morita, A.; Kizuki, M.; Seino, K.; Takano, T. Non-Hospital DOT and Early Diagnosis of Tuberculosis Reduce Costs while Achieving Treatment Success. Int. J. Tuberc. Lung Dis. 2012, 16, 828–834. Available online: http://www.ingentaconnect.com/content/10.5588/ijtld.11.0688 (accessed on 11 August 2020). [CrossRef]
- Dobler, C.C. Screening Strategies for Active Tuberculosis: Focus on Cost-Effectiveness. Clin. Outcomes Res. 2016, 8, 335–347. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC493224456/ (accessed on 29 July 2020). [CrossRef] [PubMed]
- Lung, T.; Marks, G.; Nhung, N.V.; Anh, N.T.; Hoa, N.L.P.; Anh, L.T.N.; Hoa, N.B.; Britton, W.J.; Bestrashniy, J.; Jan, S.; et al. Household Contact Investigation for the Detection of Tuberculosis in Vietnam: Economic Evaluation of a Cluster-Randomised Trial. Lancet Glob. Health 2019, 7, e376–e384. Available online: https://www.thelancet.com/journals/langlo/article/PIIs2214-109x(18)30520-5/abstract (accessed on 30 July 2020). [CrossRef]
- Shapiro, A.E.; Chakravorty, R.; Akande, T.; Lonnroth, K.; Golub, J.E. A Systematic Review of the Number Needed to Screen to Detect a Case of Active Tuberculosis in Different Risk Groups; World Health Organization: Geneva, Switzerland, 2013; p. 86. [Google Scholar]
- Choun, K.; DeCroo, T.; Mao, T.E.; Lorent, N.; Gerstel, L.; Creswell, J.; Codlin, A.J.; Lynen, L.; Thai, S. Performance of algorithms for tuberculosis active case finding in underserved high-prevalence settings in Cambodia: A cross-sectional study. Glob. Health Action 2019, 12, 1646024. [Google Scholar] [CrossRef] [PubMed]
- Lorent, N.; Choun, K.; Thai, S.; Rigouts, L.; Lynen, L. Active tuberculosis screening of close contacts among the urban poor: A Cambodian experience. Int. J. Tuberc. Lung Dis. 2014, 18, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- Graves, N.; Walker, D.; Raine, R.; Hutchings, A.; Roberts, J.A. Cost Data for Individual Patients Included in Clinical Studies: No Amount of Statistical Analysis can Compensate for Inadequate Costing Methods. Health Econ. 2002, 11, 735–739. Available online: http://onlinelibrary.wiley.com/doi/abs/:10.1002/hec.683 (accessed on 22 January 2021). [CrossRef] [PubMed]
- Kolappan, C.; Subramani, R.; Kumaraswami, V.; Santha, T.; Narayanan, P.R. Excess mortality and risk factors for mortality among a cohort of TB patients from rural south India. Int. J. Tuberc. Lung Dis. 2008, 12, 81–86. [Google Scholar]
- Global TB Report. 2020. Available online: https://www.who.int/publications/i/item/9789240013131 (accessed on 19 April 2021).




{kind=link}
{kind=link}
{kind=link}
| Parameters | Best Estimate | Upper Bound | Lower Bound | Comments | References |
|---|---|---|---|---|---|
| Epidemiology and DALY determinants | |||||
| Incident cases identified by ACF SAR | 1577 | Primary data | |||
| Incident cases identified by one-off ACF | 2303 | Primary data | |||
| Incident cases identified by PCF (intervention sites) | 2191 | Primary data | |||
| Incident cases identified by PCF (control sites) | 2875 | Primary data | |||
| Other undetected cases in the control sites | 4615 | Difference between the total number of TB cases (estimated) and cases notified by PCF † | |||
| Number of people living with HIV | 6 | Primary data | |||
| Disability weights (HIV positive) | 0.41 | 0.27 | 0.55 | [23] | |
| Disability weights (HIV negative) | 0.33 | 0.22 | 0.45 | [23] | |
| Number of TB deaths | |||||
| ACF SAR | 7 | Primary data | |||
| One-off ACF | 13 | Primary data | |||
| PCF (intervention sites) | 4 | Primary data | |||
| PCF (control sites) | 32 | Primary data | |||
| Among other undetected cases (estimated) | 51 | Estimated from the proportion of TB deaths reported by PCF in the control sites †† | |||
| Premature years of life lost | Expectation of life at age x | x = age of people with TB who died (primary data). Premature years of life lost based on WHO life tables for Cambodia 2019 | [25] | ||
| Mean age of people with TB who died | 46.3 | [26] | |||
| Standard life expectancy | 69.57 | Standard life expectancy at birth in 2018 | [27] | ||
| Cost estimates | |||||
| Program cost (human resources, case-finding activities, diagnostics, and medical procedures) | |||||
| ACF SAR (USD) * | 487,631 | Primary data | |||
| One-off ACF (USD) | 440,756 | Primary data | |||
| Health system costs | |||||
| GeneXpert (USD) | 39.0 | 40.8 | 37.3 | Published data | [18] |
| Clinical exam (USD) | 1.7 | 2.0 | 1.3 | Published data | [18] |
| Chest X-rays (USD) | 2.3 | 2.4 | 2.2 | Published data | [18] |
| Fluorescent smear microscopy (USD) | 1.9 | 2.1 | 1.7 | Published data | [18] |
| Ziehl–Neelsen smear microscopy (USD) | 1.4 | 1.4 | NA | Published data | [18] |
| Liquid culture (USD) | 19.0 | 25.1 | 12.8 | Published data | [18] |
| Follow-up work on positive culture results and identification of MTB complex (USD) | 14.4 | 16.2 | 12.6 | Published data | [18] |
| Drug susceptibility testing for MDRTB (USD) | 48.7 | 48.7 | NA | Published data | [18] |
| Specimen transport (USD) | 3.6 | 5.7 | 1.5 | Published data | [18] |
| C-DOTS/TB treatment (USD) | 65.0 | 74.0 | 56.7 | Published data | [18] |
| C-DOTS/TB treatment (USD) | 250 | 300 | 200 | Published data. Included in sensitivity analysis. | [12] |
| PCF cost (USD) | 75.5 | 111.0 | 50.4 | Published data. Upper and lower bounds estimated from a log-normal distribution. Standard deviation 20% of the means assumed. Included in sensitivity analysis. | [12] |
| PCF cost (USD) | 49.6 | 71.8 | 33.1 | [33] |
| ACF Using A Seed-and-Recruit Model | One-Off Roving ACF | |
|---|---|---|
| The number of individuals screened for symptoms suggestive of TB or eligibility for referral and TB tests | 21,539 | 189,865 |
| The number of individuals referred and tested for TB | 12,074 | 51,636 |
| The number of TB (all-forms) cases detected | 1577 | 2303 |
| The number of bacteriologically confirmed TB cases detected | 443 | 657 |
| The number of people with TB (all-forms) who initiated treatment | 1560 | 2251 |
| The number of TB deaths reported | 7 | 13 |
| The number needed to screen to find 1 TB (all-forms) case | 13.7 | 82.4 |
| The number needed to screen to find 1 bacteriologically confirmed TB case | 48.6 | 289.0 |
| The number needed to test to find 1 TB (all-forms) case | 7.7 | 22.4 |
| The number needed to test to find 1 bacteriologically confirmed TB case | 27.4 | 78.6 |
| ACF Using a Seed-and-Recruit Model | One-Off Roving ACF | |
|---|---|---|
| ACF Program | USD | USD |
| Human resources | 89,680 | 76,751 |
| Case-finding activities—intervention implementation and field workforce, project-related travels, logistics and setup, facilitation of referrals, meetings and workshops, and information, education, and communication materials | 347,267 | 211,516 |
| Diagnostics and medical procedures | 12,955 * | 97,519 |
| Administrative | 37,729 | 54,970 |
| Total (program) | 487,631 | 440,755 |
| Health system | USD | USD |
| GeneXpert MTB/RIF | 205,488 | 0 |
| Consultation and clinical examination | 20,313 | 0 |
| Smear microscopy (fluorescent or Ziehl–Neelsen) | 8821 | 0 |
| Liquid culture and other follow-up work on positive culture results and identification of Mycobacterium tuberculosis complex | 67 | 0 |
| Drug susceptibility testing for individuals suspected of drug-resistant TB | 243 | 97 |
| Treatment/C-DOTS | 101,941 | 147,096 |
| Total (health system) | 336,873 | 147,193 |
| Total (program and health system) | 824,503 | 587,948 |
| Total Costs (USD) | Total TB Cases | Total TB Deaths | YLL | YLD | DALY | Cost (USD) per DALY Averted | |
|---|---|---|---|---|---|---|---|
| Intervention sites | |||||||
| ACF SAR | 722,562 | 1577 | 7 | 92.6 | 525.4 | 620.5 | 257 |
| One-off ACF | 440,853 | 2303 | 13 | 238.5 | 766.9 | 1001.7 | 204 |
| PCF | 188,158 | 2191 | 4 | 93.1 | 729.6 | 822.7 | |
| Control sites | |||||||
| Undetected TB cases | 4615 | 51 | 1186.8 | 1536.7 | 2723.5 | Reference group | |
| PCF | 246,898 | 2875 | 32 | 744.6 | 957.4 | 1702.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teo, A.K.J.; Prem, K.; Wang, Y.; Pande, T.; Smelyanskaya, M.; Gerstel, L.; Chry, M.; Tuot, S.; Yi, S. Economic Evaluation of Community Tuberculosis Active Case-Finding Approaches in Cambodia: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2021, 18, 12690. https://doi.org/10.3390/ijerph182312690
Teo AKJ, Prem K, Wang Y, Pande T, Smelyanskaya M, Gerstel L, Chry M, Tuot S, Yi S. Economic Evaluation of Community Tuberculosis Active Case-Finding Approaches in Cambodia: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12690. https://doi.org/10.3390/ijerph182312690
Chicago/Turabian StyleTeo, Alvin Kuo Jing, Kiesha Prem, Yi Wang, Tripti Pande, Marina Smelyanskaya, Lisanne Gerstel, Monyrath Chry, Sovannary Tuot, and Siyan Yi. 2021. "Economic Evaluation of Community Tuberculosis Active Case-Finding Approaches in Cambodia: A Quasi-Experimental Study" International Journal of Environmental Research and Public Health 18, no. 23: 12690. https://doi.org/10.3390/ijerph182312690
APA StyleTeo, A. K. J., Prem, K., Wang, Y., Pande, T., Smelyanskaya, M., Gerstel, L., Chry, M., Tuot, S., & Yi, S. (2021). Economic Evaluation of Community Tuberculosis Active Case-Finding Approaches in Cambodia: A Quasi-Experimental Study. International Journal of Environmental Research and Public Health, 18(23), 12690. https://doi.org/10.3390/ijerph182312690