
Dyslipidemia, Obesity, and Ethnicity in Mexican Children

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Anthropometric and Lipid Measurements
2.2. Classification of Obesity by BMI and BFP
2.3. Classification of Lipid Disorders
2.4. Data Analysis
3. Results
3.1. Population Study and Lipid Disorder Prevalence
3.2. The Ability of BMI and BFP to Discriminate Lipid Disorders
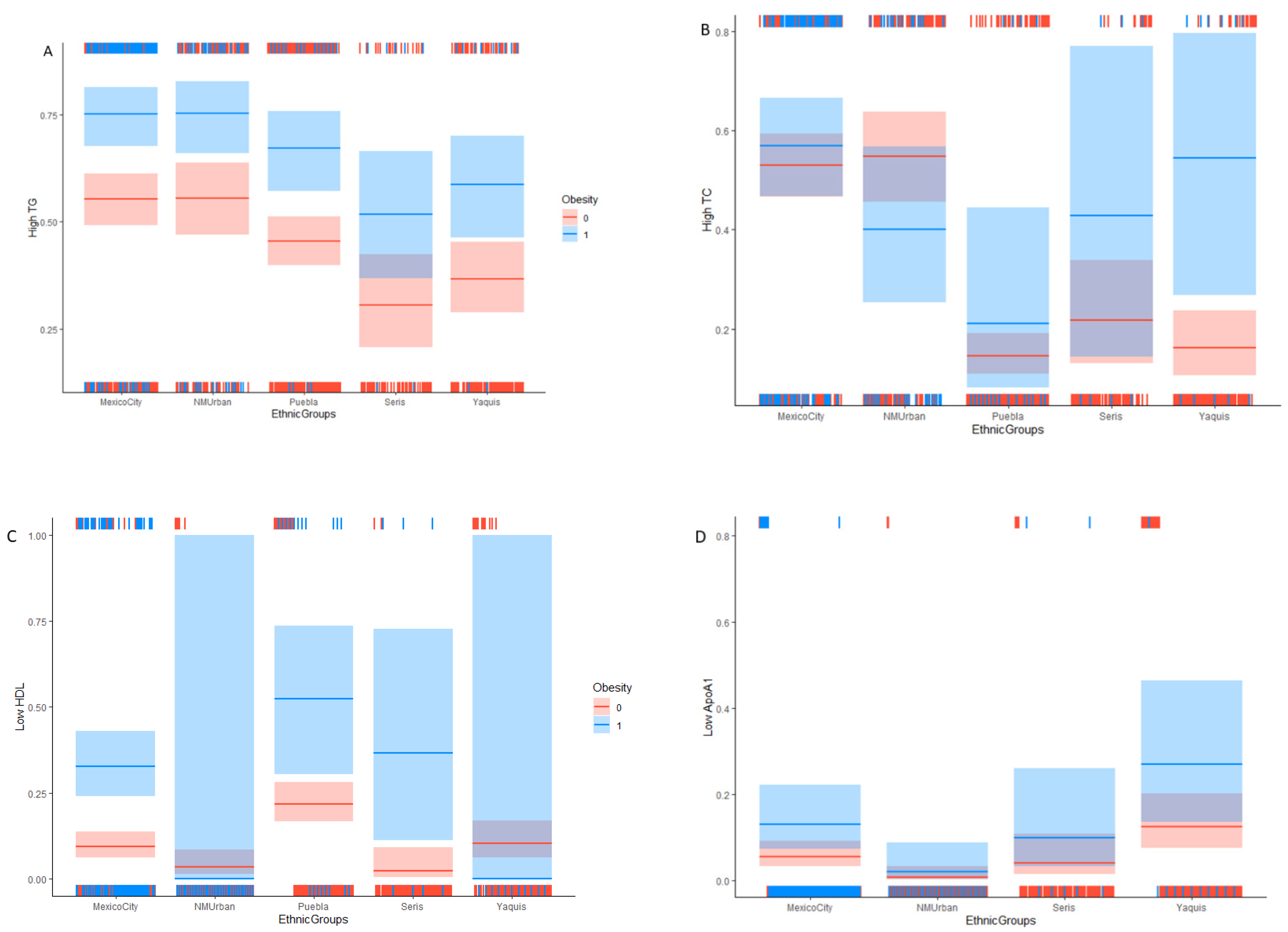
3.3. Obesity’s Association with Lipid Disorders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chung, T.S.; Onuzuruike, A.U.; Magge, S.N. Cardiometabolic risk in obese children. Ann. N. Y. Acad. Sci. 2018, 1441, 166–183. [Google Scholar] [CrossRef] [PubMed]
- Franks, P.W.; Hanson, R.L.; Knowler, W.C.; Sievers, M.L.; Looker, H.C. Childhood Obesity, Other Cardiovascular Risk Factors, and Premature Death Paul. N. Engl. J. Med. 2010, 362, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Burlutskaya, A.V.; Tril, V.E.; Polischuk, L.V.; Pokrovskii, V.M. Dyslipidemia in pediatrician’s practice. Rev. Cardiovasc. Med. 2021, 22, 817–834. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Summary report. Pediatrics 2011, 128, S213–S256, originally published online 14 November 2011. [CrossRef]
- ENSANUT. Encuesta Nacional de Salud y Nutrición de Medio Camino; Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2016. [Google Scholar] [CrossRef]
- GBD 2017 DALYs and HALE Collaborators; Yu, k.; Abate, H.H.; Abate, D.; Abay, K.H.; Abbafati, S.M.; Abbasi, C.; Abbastabar, N.; Abd-Allah, H.; Abdela, F.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Dávila-Cervantes, C.A. Cardiovascular disease in Mexico 1990–2017: Secondary data analysis from the global burden of disease study. Int. J. Public Health 2020, 65, 661–671. [Google Scholar] [CrossRef]
- Costa-Urrutia, P.; Álvarez-Fariña, R.; Abud, C.; Franco-Trecu, V.; Esparza-Romero, J.; López-Morales, C.M.; Rodríguez-Arellano, M.E.; Leal, J.V.; Colistro, V.; Granados, J. Effect of multi-component school-based program on body mass index, cardiovascular and diabetes risks in a multi-ethnic study. BMC Pediatr. 2019, 19, 401–409. [Google Scholar] [CrossRef]
- Costa-Urrutia, P.; Abud, C.; Franco-Trecu, V.; Colistro, V.; Rodríguez-Arellano, M.E.; Alvarez-Fariña, R.; Alonso, V.A.; Bertoni, B.; Granados, J. Effect of 15 BMI-associated polymorphisms, reported for Europeans, across ethnicities and degrees of amerindian ancestry in Mexican children. Int. J. Mol. Sci. 2020, 21, 374. [Google Scholar] [CrossRef]
- Moreno-Estrada, A.; Gignoux, C.R.; Fernández-López, J.C.; Zakharia, F.; Sikora, M.; Contreras, A.V.; Acuña-Alonzo, V.; Sandoval, K.; Eng, C.; Romero-Hidalgo, S.; et al. The genetics of Mexico recapitulates Native American substructure and affects biomedical traits. Science 2014, 344, 1280–1285. [Google Scholar] [CrossRef]
- Skinner, A.C.; Perrin, E.M.; Moss, L.A.; Skelton, J.A. Cardiometabolic Risks and Severity of Obesity in Children and Young Adults. N. Engl. J. Med. 2015, 373, 1307–1317. [Google Scholar] [CrossRef]
- Freedman, D.S.; Mei, Z.; Srinivasan, S.R.; Berenson, G.S.; Dietz, W.H. Cardiovascular Risk Factors and Excess Adiposity Among Overweight Children and Adolescents: The Bogalusa Heart Study. J. Pediatr. 2007, 150, 474–488. [Google Scholar] [CrossRef]
- Leyva-Flores, R.; Infante-Xibille, C.; Pablo Gutiérrez, J. Inequidad persistente en salud y acceso a los servicios para los pueblos indígenas de México, 2006–2012. Salud Publica Mex. 2013, 55, 123. [Google Scholar] [CrossRef]
- Costa-Urrutia, P.; Vizuet-Gámez, A.; Ramirez-Alcántara, M.; Guillen-González, M.Á.; Medina-Contreras, O.; Valdes-Moreno, M.; Musalem-Younes, C.; Solares-Tlapechco, J.; Granados, J.; Franco-Trecu, V.; et al. Obesity measured as percent body fat, relationship with body mass index, and percentile curves for Mexican pediatric population. PLoS ONE 2019, 14, e0212792. [Google Scholar] [CrossRef]
- Fomon, S.J.; Haschke, F.; Ziegler, E.E.; Nelson, S.E. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 812–819. [Google Scholar] [CrossRef]
- WHO; WHO Child Growth Standards; WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. Geneva: World Health Organization. Paediatr. Croat. Suppl. 2006, 52, 13–17. [Google Scholar] [CrossRef]
- Williams, D.P.; Going, S.B.; Lohman, T.G.; Harsha, D.W.; Srinivasan, S.R.; Webber, L.S.; Berenson, G.S. Body Fatness and Risk for Elevated Blood-Pressure, Total Cholesterol, and Serum-Lipoprotein Ratios in Children and Adolescents. Am. J. Public Health 1992, 82, 358–363. [Google Scholar] [CrossRef]
- Javier, F.; Díez, A.; Albillos, J.A.R.; Nieves, G.; Valero, L. Dislipemias en edad pediátrica. Asoc. Española Pediatría 2019, 1, 125–140. [Google Scholar] [CrossRef]
- Perkins, N.J.; Schisterman, E.F. The Inconsistency of “Optimal” Cut-points Using Two ROC Based Criteria. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef]
- Burnham, K.P.; Anderson, D.R. Multimodel Inference Understanding AIC and BIC in Model Selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008; p. 2673. Available online: https://www.r-project.org/ (accessed on 28 November 2021).
- Pérez, E.; Soriano, M.; Lozano, V.; Morales, M.; De-la-Luz, L.; Rugerio, M. Factores de riesgo cardiovascular en población adulta aparentemente sana de la ciudad de Puebla. Rev. Mex. Enfer. Cardiol. 2008, 16, 87–92. [Google Scholar]
- Jiménez-Cruz, A.; Bacardí-Gascón, M.; Spindler, A.A. Obesity and hunger among Mexican-Indian migrant children on the US-Mexico border. Int. J. Obes. 2003, 27, 740–747. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Meléndez, J.; Cañez, G.; Frías, H. Comportamiento alimentario y obesidad infantil en Sonora, México. Rev. Latinoam. Ciencias Soc. Niñez Juv. 2010, 8, 1131–1147. [Google Scholar]
- Castro-juarez, A.A.; Serna-gutiérrez, A.; Lozoya-villegas, J.F.; Toledo-domínguez, I.D.J.; Díaz-zavala, R.G.; Esparza-romero, J. Prevalence of previous diagnosis of hypertension and associated factors in the Yaqui indigenous of Sonora. Rev. Mex. Cardiol. 2018, 29, 90–97. [Google Scholar]
- Alberto Acosta, A.; García, A.M.; Composto, C.; Diego Pérez Roig, D.; Pineda, E.; Scheinvar, E.; Salazar, E.; Velázquez, G.; Tzul, G.; Alimonda, H.; et al. Territorios en disputa. Despojo capitalista, luchas en defensa de los bienes comunes naturales y alternativas emancipatorias para América Latina. Primera. Ciudad. Mex. Bajo Tierr. 2014. [Google Scholar]
- Rodríguez-Morán, M.; Guerrero-Romero, F.; Brito-Zurita, O.; Rascón-Pacheco, R.A.; Pérez-Fuentes, R.; Sánchez-Guillén, M.C.; González-Ortiz, M.; Martínez-Abundis, E.; Simental-Mendía, L.E.; Madero, A.; et al. Cardiovascular Risk Factors and Acculturation in Yaquis and Tepehuanos Indians from Mexico. Arch. Med. Res. 2008, 39, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Morales, I.; Colin-Ramirez, E.; Rivera-Mancía, S.; Vallejo, M.; Vázquez-Antona, C. Performance of waist-to-height ratio, waist circumference, and body mass index in discriminating cardio-metabolic risk factors in a sample of school-aged Mexican children. Nutrients 2018, 10, 1850. [Google Scholar] [CrossRef]
- Narchi, N.E.; Marlett, C.M.; Hernández-Santana, G. What Happened to Seri Sweets? Dietary Transition through Culinary Acculturation. J. Ethnobiol. 2020, 40, 348–367. [Google Scholar] [CrossRef]
- Burckhalter, D. Eelgrass: A Traditional Comcaac (Seri) Seafood and a Revolutionary Source of Grain. J. Southwest 2021, 63, 369–384. [Google Scholar] [CrossRef]
- Jayasekara, C.; Mendis, E.; Kim, S. Seafood in the Human Diet for Better Nutrition and Health. Encycl. Mar. Biotechnol. 2020, 2939–2959. [Google Scholar] [CrossRef]
- Li, Y.; Zou, Z.; Luo, J.; Ma, J.; Ma, Y.; Jing, J.; Zhang, X.; Luo, C.; Wang, H.; Zhao, H.; et al. The predictive value of anthropometric indices for cardiometabolic risk factors in Chinese children and adolescents: A national multicenter school-based study. PLoS ONE 2020, 15, e0227954. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Guzmán, I.P.; Salgado-Bernabé, A.B.; Muñoz Valle, J.F.; Vences-Velázquez, A.; Parra-Rojas, I. Prevalencia de síndrome metabólico en niños con obesidad y sin ella. Med. Clin. 2015, 144, 198–203. [Google Scholar] [CrossRef]
- Robles, M.; Gallegos, A.; Díaz, R.; Urquídez, R.; Quizán, T.; Esparza, J. Adaptación y factibilidad de un programa de prevención de diabetes en la comunidad Comcáac (Seri) de Sonora, México. Tecnociencia Chihuah. 2015, 9, 75–83. [Google Scholar]
- Robles-Ordaz, M.D.; Gallegos-Aguilar, A.C.; Urquidez-Romero, R.; Diaz-Zavala, R.G.; Lavandera-Torres, M.G.; Esparza-Romero, J. Prevalence of prediabetes and modifiable factors in an ethnic group of Mexico: The Comcáac Project. Public Health Nutr. 2018, 21, 333–338. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Boys, n = 572 | Girls, n = 405 | ||||
|---|---|---|---|---|---|
| All, n = 977 | Median | IQR | Median | IQR | p |
| Age | 9.0 | 4.0 | 9.0 | 3.0 | 0.29 |
| BMI | 17.6 | 6.7 | 17.0 | 4.6 | 0.01 |
| BMIz | −0.3 | 1.4 | −0.2 | 1.1 | 0.60 |
| TG | 87.0 | 61.9 | 85.5 | 51.0 | 0.91 |
| TC | 157.8 | 44.5 | 155.0 | 38.0 | 0.10 |
| HDL | 56.5 | 15.4 | 55.1 | 17.3 | 0.27 |
| LDL | 83.5 | 30.6 | 81.1 | 26.0 | 0.20 |
| ApoA1 | 153.0 | 52.0 | 153.0 | 58.0 | 0.23 |
| ApoB | 86.0 | 34.6 | 87.5 | 27.8 | 0.38 |
| CM-Mexico City, n = 325 | |||||
| Age | 9.0 | 4.0 | 9.0 | 4.0 | 0.42 |
| BMI | 20.4 | 8.3 | 18.5 | 5.4 | 0.02 |
| BMIz | 0.3 | 1.7 | 0.3 | 1.3 | 0.75 |
| TG | 102.0 | 75.0 | 102.0 | 52.5 | 0.71 |
| TC | 173.0 | 46.0 | 169.5 | 35.5 | 0.05 |
| HDL | 56.1 | 16.1 | 57.2 | 20.2 | 0.91 |
| LDL | 92.8 | 37.9 | 89.6 | 28.1 | 0.09 |
| ApoA1 | 152.0 | 42.0 | 142.0 | 34.3 | 0.01 |
| ApoB | 82.0 | 29.0 | 82.0 | 25.5 | 0.94 |
| CM-Puebla, n = 302 | |||||
| Age | 9.0 | 3.0 | 9.0 | 3.0 | 0.52 |
| BMI | 16.6 | 3.4 | 16.7 | 3.5 | 0.86 |
| BMIz | 0.5 | 0.8 | 0.3 | 0.8 | 0.02 |
| TG | 77.1 | 47.7 | 81.8 | 46.5 | 0.19 |
| TC | 145.3 | 31.4 | 141.5 | 32.5 | 0.82 |
| HDL | 54.8 | 15.4 | 49.7 | 14.3 | 0.01 |
| LDL | 79.8 | 19.2 | 79.5 | 27.0 | 0.21 |
| NM-Urban, n = 148 | |||||
| Age | 8.0 | 3.0 | 9.0 | 3.0 | 0.47 |
| BMI | 18.3 | 6.1 | 17.9 | 6.6 | 0.48 |
| BMIz | 01.0 | 1.3 | 01.0 | 1.4 | 0.47 |
| TG | 89.0 | 59.5 | 89.5 | 71.0 | 0.80 |
| TC | 167.0 | 48.0 | 170.5 | 37.0 | 0.61 |
| HDL | 63.6 | 16.6 | 67.4 | 16.3 | 0.38 |
| LDL | 84.0 | 33.3 | 85.4 | 25.1 | 0.97 |
| ApoA1 | 194.0 | 31.5 | 191.0 | 44.3 | 0.59 |
| ApoB | 100.3 | 21.9 | 94.0 | 21.8 | 0.15 |
| NM-Yaquis, n = 135 | |||||
| Age | 9.0 | 4.0 | 9.0 | 5.0 | 0.57 |
| BMI | 16.2 | 4.1 | 16.2 | 4.0 | 0.86 |
| BMIz | −0.6 | 0.9 | −0.4 | 0.9 | 0.50 |
| TG | 79.0 | 51.5 | 88.0 | 38.0 | 0.13 |
| TC | 145.5 | 32.0 | 151.0 | 28.0 | 0.16 |
| HDL | 55.7 | 11.9 | 52.7 | 11.1 | 0.24 |
| LDL | 72.4 | 17.5 | 77.1 | 18.1 | 0.06 |
| ApoA1 | 139.5 | 29.3 | 135.0 | 22.0 | 0.14 |
| ApoB | 68.5 | 21.4 | 74.0 | 14.0 | 0.07 |
| NM-Seris, n = 67 | |||||
| Age | 9.5 | 3.0 | 10.0 | 2.3 | 0.72 |
| BMI | 17.6 | 4.0 | 17.3 | 4.0 | 0.89 |
| BMIz | −0.5 | 0.8 | −0.4 | 1.0 | 0.75 |
| TG | 77.0 | 44.0 | 73.0 | 21.8 | 0.71 |
| TC | 152.0 | 36.3 | 148.0 | 29.3 | 0.56 |
| HDL | 54.5 | 6.3 | 54.4 | 9.0 | 0.81 |
| LDL | 68.3 | 21.7 | 72.3 | 15.6 | 0.32 |
| ApoA1 | 145.0 | 19.0 | 139.0 | 28.3 | 0.35 |
| ApoB | 65.0 | 24.6 | 67.5 | 14.8 | 0.40 |
| Prevalence | All n = 977 | CM-Mexico City n = 325 | CM-Puebla n = 302 | NM-Urban n = 148 | NM-Yaquis n = 135 | NM-Seris n = 67 |
|---|---|---|---|---|---|---|
| OB % | 17 | 28.6 | 6.3 | 23.6 | 8.14 | 20.4 |
| High TG, n (%) | 496 (50.7) | 198 (60.9) | 138 (45.7) | 86 (58.1) | 51 (37.8) | 23 (34.3) |
| % High TG with OB | 23.0 | 34.8 | 10.9 | 24.4 | 17.4 | 21.7 |
| High TC, n (%) | 339 (34.7) | 176 (54.2) | 45 (14.9) | 76 (51.4) | 26 (19.3) | 16 (23.9) |
| % High TC with OB | 23.6 | 30.1 | 8.9 | 18.4 | 23.1 | 18.8 |
| Low HDL, n (%) | 166 (17.0) | 58 (17.8) | 83 (27.5) | 5 (3.4) | 15 (11.1) | 5 (7.5) |
| % Low HDL with OB | 28.3 | 56.9 | 13.3 | 0.0 | 0 | 60.0 |
| High LDL n (%) | 132 (13.5) | 84 (25.4) | 22 (7.3) | 20 (13.5) | 4 (3.0) | 2 (3.0) |
| % High LDL with OB | 28.0 | 33.3 | 18.2 | 25.0 | 0 | 0 |
| Low ApoA1, n (%) | 58 (8.6) | 27 (8.3) | na | 2 (1.4) | 24 (17.8) | 5 (7.4) |
| % Low ApoA1 with OB | 20.7 | 33.3 | na | 0.0 | 4.1 | 40.0 |
| High ApoB, n (%) | 242 (35.8) | 118 (36.3) | na | 93 (62.8) | 22 (16.3) | 9 (13.4) |
| % High ApoB with OB | 31.0 | 37.3 | na | 24.7 | 27.3 | 22.2 |
| Dyslipidemia, n (%) | 644 (66.0) | 255 (75.5) | 175 (58.0) | 113 (76.4) | 70 (52.0) | 31 (46.3) |
| % Dyslipidemia with OB | 21.7 | 32.2 | 10.3 | 22.1 | 12.9 | 19.4 |
| AUC (95%CI), p | ||||||
|---|---|---|---|---|---|---|
| All | CM-Mexico City | CM-Puebla | NM-Urban | NM-Yaquis | NM-Seris | |
| High TG | 0.68 (0.65–0.71), <0.001 | 0.68 (0.62–0.74), <0.001 | 0.67 (0.60–0.73), <0.001 | 0.55 (0.45–0.64), 0.322 | 0.66 (0.56–0.76), 0.002 | 0.82 (0.73–0.93), <0.001 |
| High TC | 0.60 (0.56–0.66), <0.001 | 0.54 (0.48–0.61), 0.183 | 0.57 (0.47–0.66), 0.144 | 0.47 (0.37–0.56), 0.464 | 0.53 (0.39–0.67), 0.652 | 0.62 (0.46–0.79), 0.146 |
| Low HDL | 0.64 (0.59–0.69), <0.001 | 0.75 (0.69–0.82), <0.001 | 0.66 (0.60–0.73), <0.001 | 0.46 (0.28–0.65), 0.700 | 0.50 (0.26–0.60), 0.411 | 0.95 (0.90–1.00), <0.001 |
| High LDL | 0.61 (0.56–0.69), <0.001 | 0.59 (0.52–0.66), 0.010 | 0.80 (0.69–0.85), <0.001 | 0.50 (0.37–0.64), 0.964 | 0.50 (0.16–0.64), 0.412 | 0.67 (0.30–1.00), 0.352 |
| Low ApoA1 | 0.50 (0.40–0.56), 0.562 | 0.56 (0.42–0.67), 0.233 | na | 0.53 (0.32–0.73), 0.782 | 0.50 (0.33–0.58), 0.585 | 0.74 (0.47–1.00), 0.081 |
| High ApoB | 0.64 (0.60–0.68), <0.001 | 0.60 (0.53–0.62), 0.003 | na | 0.60 (0.50–0.69), 0.063 | 0.68 (0.54–0.81), 0.012 | 0.77 (0.61–0.94), 0.001 |
| Dyslipidemia | 0.68 (0.64–0.71), <0.001 | 0.68 (0.61–0.76), <0.001 | 0.64 (0.58–0.70), <0.001 | 0.53 (0.41–0.65), 0.141 | 0.57 (0.48–0.67), 0.146 | 0.76 (0.64–0.87), <0.001 |
| High TG | Estimate | SE | Z | OR (CI 95%) | p |
|---|---|---|---|---|---|
| Intercept | −0.95 | 0.32 | −2.99 | 0.39 (0.21, 0.72) | 0.003 |
| Age | 0.13 | 0.03 | 3.93 | 1.14 (1.07, 1.21) | ˂0.001 |
| OB | 0.9 | 0.19 | 4.61 | 2.45 (1.68, 3.62) | ˂0.001 |
| NM-Urban | 0.01 | 0.21 | 0.05 | 1.01 (0.67, 1.52) | 0.960 |
| CM-Puebla | −0.39 | 0.17 | −2.33 | 0.67 (0.48, 0.94) | 0.020 |
| NM-Seris | −1.04 | 0.29 | −3.6 | 0.36 (0.20, 0.62) | ˂0.001 |
| NM-Yaquis | −0.76 | 0.22 | −3.48 | 0.47 (0.32, 0.72) | ˂0.001 |
| High TC | |||||
| Intercept | 0.12 | 0.13 | 0.92 | 1.13 (0.87, 1.46) | 0.360 |
| OB | 0.16 | 0.25 | 0.65 | 1.17 (0.72, 1.91) | 0.520 |
| NM | 0.07 | 0.23 | 0.32 | 1.08 (0.69, 1.70) | 0.750 |
| CM-Puebla | −1.90 | 0.21 | −8.86 | 0.15 (0.10, 0.23) | <0.001 |
| NM-Seris | −1.41 | 0.34 | −4.14 | 0.25 (0.12, 0.46) | <0.001 |
| NM-Yaquis | −1.77 | 0.28 | −6.38 | 0.17 (0.11, 0.29) | <0.001 |
| NM*OB | −0.76 | 0.46 | −1.64 | 0.47 (0.19, 1.15) | 0.100 |
| CM-Puebla*OB | 0.29 | 0.64 | 0.46 | 1.34 (0.34, 4.36) | 0.650 |
| NM-Seris*OB | 0.84 | 0.86 | 0.97 | 2.31 (0.39, 12.64) | 0.330 |
| NM-Yaquis*OB | 1.67 | 0.70 | 2.39 | 5.31 (1.35, 21.81) | 0.021 |
| Low HDL | |||||
| Intercept | −3.08 | 0.49 | −6.31 | 0.05 (0.02, 0.12) | <0.001 |
| Age | 0.09 | 0.05 | 1.94 | 1.09 (1.00, 1.20) | 0.051 |
| OB | 1.56 | 0.31 | 5.09 | 4.74 (2.62, 8.72) | <0.001 |
| Gender (girls) | 0.47 | 0.19 | 2.49 | 1.60 (1.11, 2.31) | 0.011 |
| NM-Urban | −1.03 | 0.51 | −2.02 | 0.36 (0.12, 0.92) | 0.043 |
| CM-Puebla | 1.00 | 0.26 | 3.88 | 2.72 (1.66, 4.57) | <0.001 |
| NM-Seris | −1.46 | 0.75 | −1.94 | 0.23 (0.04, 0.82) | 0.052 |
| NM-Yaquis | 0.11 | 0.35 | 0.31 | 1.11 (0.55, 2.19) | 0.763 |
| NM-Urban*OB | −16.07 | 64.21 | −0.02 | 0.01 (0.01, 61.55) | 0.982 |
| CM-Puebla*OB | −0.18 | 0.58 | −0.32 | 0.83 (0.27, 2.64) | 0.752 |
| NM-Seris*OB | 1.63 | 1.10 | 1.48 | 5.11 (0.61, 15.37) | 0.143 |
| NM-Yaquis*OB | −17.40 | 80.06 | −0.02 | 0.02 (0.01, 6.77) | 0.999 |
| High LDL | |||||
| Intercept | −1.78 | 0.46 | −3.84 | 0.17 (0.07, 0.41) | ˂0.001 |
| Age | 0.09 | 0.05 | 1.91 | 1.10 (1.10, 1.20) | 0.062 |
| Gender (Girls) | −0.45 | 0.22 | −2.05 | 0.64 (0.41, 0.97) | 0.042 |
| NM | −0.61 | 0.28 | −2.17 | 0.54 (0.31, 0.93) | 0.033 |
| CM-Puebla | −1.37 | 0.26 | −5.31 | 0.25 (0.15, 0.41) | ˂0.001 |
| Seris | −2.33 | 0.73 | −3.18 | 0.10 (0.02, 0.32) | 0.001 |
| Yaquis | −2.35 | 0.52 | −4.48 | 0.10 (0.03, 0.24) | ˂0.001 |
| Low ApoA1 | |||||
| Intercept | −2.84 | 0.28 | −10.02 | 0.06 (0.03, 0.1) | ˂0.001 |
| OB | 0.94 | 0.42 | 2.26 | 2.57 (1.10, 5.77) | 0.022 |
| Gender (Girls) | 0.92 | 0.33 | 2.82 | 2.51 (1.33, 4.8) | ˂0.001 |
| NM | −1.98 | 0.75 | −2.64 | 0.14 (0.02, 0.48) | 0.011 |
| Seris | −0.3 | 0.53 | −0.57 | 0.74 (0.23, 1.94) | 0.572 |
| Yaquis | 0.9 | 0.33 | 2.76 | 2.47 (1.3, 4.71) | 0.012 |
| Girls*OB | −2.78 | 1.12 | −2.49 | 0.06 (0.03, 0.39) | 0.011 |
| High ApoB | |||||
| Intercept | −1.59 | 0.4 | −3.99 | 0.20 (0.09, 0.44) | ˂0.001 |
| Age | 0.09 | 0.04 | 2.21 | 1.10 (1.01, 1.19) | 0.032 |
| OB | 0.68 | 0.2 | 3.33 | 1.97 (1.32, 2.94) | ˂0.001 |
| NM | 1.22 | 0.21 | 5.72 | 3.38 (2.24, 5.15) | ˂0.001 |
| Seris | −1.23 | 0.38 | −3.23 | 0.29 (0.13, 0.59) | ˂0.001 |
| Yaquis | −0.92 | 0.27 | −3.46 | 0.40 (0.23, 0.66) | ˂0.001 |
| Dyslipidemia | |||||
| Intercept | 1.08 | 0.15 | 7.14 | 2.93 (2.20, 3.97) | ˂0.001 |
| OB | 0.93 | 0.35 | 2.63 | 2.54 (1.31, 5.34) | 0.009 |
| NM | 0.18 | 0.27 | 0.67 | 1.20 (0.71, 2.07) | 0.500 |
| CM-Puebla | −0.86 | 0.19 | −4.45 | 0.42 (0.29, 0.62) | ˂0.001 |
| Seris | −1.41 | 0.3 | −4.67 | 0.24 (0.13, 0.44) | ˂0.001 |
| Yaquis | −1.11 | 0.23 | −4.73 | 0.33 (0.21, 0.52) | ˂0.001 |
| NM-Urban*OB | −1.28 | 0.56 | −2.26 | 0.28 (0.09, 0.85) | 0.022 |
| CM-Puebla*OB | 1.74 | 1.09 | 1.59 | 5.68 (0.96, 10.05) | 0.112 |
| Seris*OB | 1.2 | 1.17 | 1.02 | 3.30 (0.45, 8.29) | 0.314 |
| Yaquis*OB | 0.6 | 0.88 | 0.69 | 1.83 (0.37, 13.59) | 0.492 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa-Urrutia, P.; Colistro, V.; Franco-Trecu, V.; Granados, J.; Álvarez Fariña, R.; Rodríguez-Arellano, M.E. Dyslipidemia, Obesity, and Ethnicity in Mexican Children. Int. J. Environ. Res. Public Health 2021, 18, 12659. https://doi.org/10.3390/ijerph182312659
Costa-Urrutia P, Colistro V, Franco-Trecu V, Granados J, Álvarez Fariña R, Rodríguez-Arellano ME. Dyslipidemia, Obesity, and Ethnicity in Mexican Children. International Journal of Environmental Research and Public Health. 2021; 18(23):12659. https://doi.org/10.3390/ijerph182312659
Chicago/Turabian StyleCosta-Urrutia, Paula, Valentina Colistro, Valentina Franco-Trecu, Julio Granados, Rafael Álvarez Fariña, and Martha Eunice Rodríguez-Arellano. 2021. "Dyslipidemia, Obesity, and Ethnicity in Mexican Children" International Journal of Environmental Research and Public Health 18, no. 23: 12659. https://doi.org/10.3390/ijerph182312659
APA StyleCosta-Urrutia, P., Colistro, V., Franco-Trecu, V., Granados, J., Álvarez Fariña, R., & Rodríguez-Arellano, M. E. (2021). Dyslipidemia, Obesity, and Ethnicity in Mexican Children. International Journal of Environmental Research and Public Health, 18(23), 12659. https://doi.org/10.3390/ijerph182312659