
Ethnic Inequalities in Healthcare Use and Care Quality among People with Multiple Long-Term Health Conditions Living in the United Kingdom: A Systematic Review and Narrative Synthesis


Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Outcomes
2.5. Data Analysis
3. Results
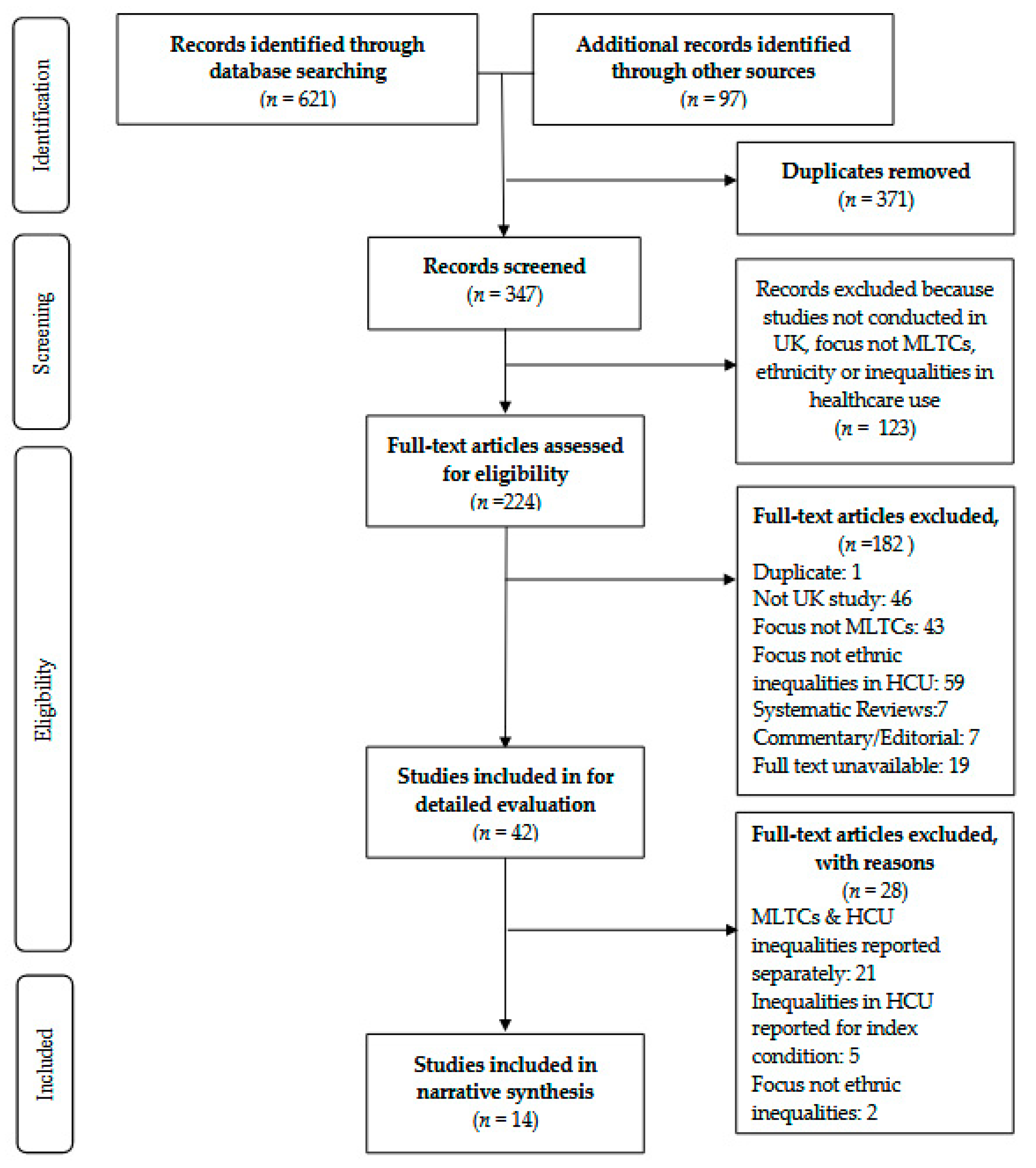
3.1. Overview of Included Studies
3.2. Participant Characteristics
3.2.1. Ethnic Group Identification
3.2.2. Ethnic Group Categorisation
3.2.3. Missing Ethnicity Data
3.2.4. Gender and Age
3.3. Domains of Healthcare Use and Care Quality Assessed in Included Studies
3.4. Studies Reporting on Ethnic Differences in Patterns of Healthcare Use and Care Quality among People with Multiple Long-Term Conditions Living in the UK
3.5. Evidence of Ethnic Inequalities in Healthcare Use among People with Multiple Long-Term Conditions
3.5.1. Ethnic Inequalities in Disease Management among People with Multiple Long-Term Conditions
3.5.2. Ethnic Inequalities in Emergency Admission among People with Multiple Long-Term Conditions
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Reviews
4.3. Mechanisms
4.4. Strengths and Limitations
4.5. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| 10 | MLTCs + Ethnicity + inequality + quality care + country | (((MAINSUBJECT.EXACT.EXPLODE (“Mixed ethnicity”) OR MAINSUBJECT.EXACT. EXPLODE (“Ethnicity”) OR ab,ti,if (“Ethnic Group?” OR “african continental ancestry group” OR Arab OR Africa? OR Afro? OR Asian OR “Asian Continental Ancestry Group” OR “Asylum seeker” OR Bangladesh? OR Black OR “BME” OR “BAME” OR Caribbean OR China OR Chinese OR Cultur? OR Divers? OR Ethnic? OR Gypsy OR India? OR Irish OR Migrant OR Minorit? OR Mixed OR “Mixed ethnic?” OR “Multiple ethnic?” OR Multi rac? OR ‘Other White’ OR Pakistan? OR Roma OR “White Other” OR Refugee? OR race OR racial? OR “South Asian” OR “European Continental Ancestry Group”)) AND (MAINSUBJECT.EXACT (“England and Wales”) OR MAINSUBJECT.EXACT (“Channel Islands”) OR MAINSUBJECT.EXACT (“UK”) OR MAINSUBJECT.EXACT (“Scotland”) OR MAINSUBJECT.EXACT (“England”) OR MAINSUBJECT.EXACT (“Northern Ireland”) OR MAINSUBJECT.EXACT (“Wales”) OR ti, ab, if (“United Kingdom” OR “UK” OR England OR Wales OR Scotland OR “Northern Ireland” OR Britain OR “Great Britain”)) AND (ti, ab, if (“Multiple Chronic Conditions” OR Co morbid? OR Multi morbidity OR Multi patholog? OR “multiple condition?” OR “Multiple health condition?” OR “Multiple health problems” OR “Multiple medical conditions” OR “Multiple medical problems” OR “Pluri$patholog?” OR Polymorbid? OR “multiple illness?” OR “Multiple Chronic Health Conditions” OR “Multiple Chronic Medical Conditions” OR “multiple chronic illness?”) OR MAINSUBJECT.EXACT.EXPLODE (“Comorbidity”))) NOT (MAINSUBJECT.EXACT. EXPLODE (“USA”) OR MAINSUBJECT.EXACT.EXPLODE (“North America”) OR MAINSUBJECT.EXACT.EXPLODE (“Canada”) OR MAINSUBJECT.EXACT.EXPLODE (“Australia”) OR MAINSUBJECT.EXACT.EXPLODE (“New Zealand”) OR MAINSUBJECT.EXACT. EXPLODE (“South America”) OR MAINSUBJECT.EXACT.EXPLODE (“Central America”) OR ti, ab, if (“Americas” OR “USA” OR America OR “North America” OR Canada OR Australia OR “New Zealand”))) AND (ti, ab, if (“Health Equity” OR “Healthcare disparit?” OR Inequalit? OR disparit? OR “Healthcare Disparit?” OR “Health care Disparit?” OR “Health-care Disparit?” OR “Health Care Inequalit?” “Healthcare Inequalit?” OR “Health-care Inequalit?” OR “inequalit? in healthcare” OR “inequalit? in health care” OR “inequality in health-care” OR “disparit? in healthcare” OR “disparit? in health care” OR “disparit? in health-care” OR “inequit?” OR “health inequit?”) OR MAINSUBJECT.EXACT (“Health inequalities”)) AND (ti, ab, if (“Quality of Health Care” OR “Patient Acceptance of Health Care” OR “Patient Satisfaction” OR “Health Care Quality, Access, and Evaluation” OR “Care Quality” OR “Quality of care” OR “Quality of health care” OR “quality of health-care” OR “Quality of healthcare” “healthcare quality” OR “health-care quality” OR “health care quality” OR “quality health service” OR “health service quality” OR satisfaction OR dissatisfaction OR satisfied OR dissatisfied OR “effectiveness” OR safety OR responsiveness OR acceptab? OR appropriate? OR timeliness) OR MAINSUBJECT.EXACT. EXPLODE (“Quality of care”)) |
| 9 | MLTCs + Ethnicity + Healthcare use + inequality + country | (((MAINSUBJECT.EXACT.EXPLODE (“Mixed ethnicity”) OR MAINSUBJECT.EXACT. EXPLODE (“Ethnicity”) OR ab,ti,if (“Ethnic Group?” OR “african continental ancestry group” OR Arab OR Africa? OR Afro? OR Asian OR “Asian Continental Ancestry Group” OR “Asylum seeker” OR Bangladesh? OR Black OR “BME” OR “BAME” OR Caribbean OR China OR Chinese OR Cultur? OR Divers? OR Ethnic? OR Gypsy OR India? OR Irish OR Migrant OR Minorit? OR Mixed OR “Mixed ethnic?” OR “Multiple ethnic?” OR Multi rac? OR ‘Other White’ OR Pakistan? OR Roma OR “White Other” OR Refugee? OR race OR racial? OR “South Asian” OR “European Continental Ancestry Group”)) AND (MAINSUBJECT.EXACT (“England and Wales”) OR MAINSUBJECT.EXACT (“Channel Islands”) OR MAINSUBJECT.EXACT (“UK”) OR MAINSUBJECT.EXACT (“Scotland”) OR MAINSUBJECT.EXACT (“England”) OR MAINSUBJECT.EXACT (“Northern Ireland”) OR MAINSUBJECT.EXACT (“Wales”) OR ti, ab, if (“United Kingdom” OR “UK” OR England OR Wales OR Scotland OR “Northern Ireland” OR Britain OR “Great Britain”)) AND (ti, ab, if (“Multiple Chronic Conditions” OR Co morbid? OR Multi morbidity OR Multi patholog? OR “multiple condition?” OR “Multiple health condition?” OR “Multiple health problems” OR “Multiple medical conditions” OR “Multiple medical problems” OR “Pluri$patholog?” OR Polymorbid? OR “multiple illness?” OR “Multiple Chronic Health Conditions” OR “Multiple Chronic Medical Conditions” OR “multiple chronic illness?”) OR MAINSUBJECT.EXACT.EXPLODE (“Comorbidity”))) NOT (MAINSUBJECT.EXACT. EXPLODE (“USA”) OR MAINSUBJECT.EXACT.EXPLODE (“North America”) OR MAINSUBJECT.EXACT.EXPLODE (“Canada”) OR MAINSUBJECT.EXACT.EXPLODE (“Australia”) OR MAINSUBJECT.EXACT.EXPLODE (“New Zealand”) OR MAINSUBJECT.EXACT. EXPLODE (“South America”) OR MAINSUBJECT.EXACT.EXPLODE (“Central America”) OR ti, ab, if (“Americas” OR “USA” OR America OR “North America” OR Canada OR Australia OR “New Zealand”))) AND (ti, ab, if (“Health Equity” OR “Healthcare disparit?” OR Inequalit? OR disparit? OR “Healthcare Disparit?” OR “Health care Disparit?” OR “Health-care Disparit?” OR “Health Care Inequalit?” “Healthcare Inequalit?” OR “Health-care Inequalit?” OR “inequalit? in healthcare” OR “inequalit? in health care” OR “inequality in health-care” OR “disparit? in healthcare” OR “disparit? in health care” OR “disparit? in health-care” OR “inequit?” OR “health inequit?”) OR MAINSUBJECT.EXACT (“Health inequalities”)) AND (ti, ab, if (“Delivery of Health Care” OR “Tertiary Healthcare” OR “Primary Health Care” OR “Health Care Quality, Access, and Evaluation” [Mesh] OR “Community Health Services” OR Healthcare OR health-care OR “health care” OR “health service” OR “health centre” OR “Health centre” OR “medical care” OR “National Health Service” OR “NHS” OR A E OR “Accident and emergency” OR “Acute healthcare” OR “Acute health care” OR “Acute health-care” OR “Acute hospital care” OR “urgent care” OR “emergency care” OR “primary care” OR “general practitioner” OR “GP” OR “General pract? visit” OR “GP visit?” OR “GP consult?” OR “General pract? consult?” OR “medical consult?” “GP services” OR “General practitioner services” OR “physician visit” OR “Family Physician” OR Dental OR Dentist OR dentistry OR “Eye care” OR Optician OR “Oral health” OR Pharmacy OR pharmacies OR “pharmacy service” OR “Secondary care” OR Hospital OR “Hospital visit” OR “hospital admission” OR “Day patient” OR in-patient OR “inpatient” OR outpatient OR out-patient OR referral OR therap? OR “Preventative healthcare” OR “preventative health care” OR “preventative health-care” OR “preventative service” OR “preventative medicine” OR “health outreach” OR screen? OR vaccinat? OR “Palliative care” OR “Case manag?” OR “Community care” OR “Community nurse” OR “Community services?” OR “Tertiary care” OR “tertiary health care” OR “tertiary healthcare” OR “tertiary health-care” OR specialist OR “specialist health service” OR “Mental health service” OR “sexual health service”) OR MAINSUBJECT.EXACT.EXPLODE (“Health care”)) |
| 8 | quality care | ti, ab, if (“Quality of Health Care” OR “Patient Acceptance of Health Care” OR “Patient Satisfaction” OR “Health Care Quality, Access, and Evaluation” OR “Care Quality” OR “Quality of care” OR “Quality of health care” OR “quality of health-care” OR “Quality of healthcare” “healthcare quality” OR “health-care quality” OR “health care quality” OR “quality health service” OR “health service quality” OR satisfaction OR dissatisfaction OR satisfied Or dissatisfied OR “effectiveness” OR safety OR responsiveness OR acceptab? OR appropriate? OR timeliness) OR MAINSUBJECT.EXACT.EXPLODE (“Quality of care”) |
| 7 | healthcare utilisation | ti, ab, if (“Delivery of Health Care” OR “Tertiary Healthcare” OR “Primary Health Care” OR “Health Care Quality, Access, and Evaluation” [Mesh] OR “Community Health Services” OR Healthcare OR health-care OR “health care” OR “health service” OR “health centre” OR “Health centre” OR “medical care” OR “National Health Service” OR “NHS” OR A&E OR “Accident and emergency” OR “Acute healthcare” OR “Acute health care” OR “Acute health-care” OR “Acute hospital care” OR “urgent care” OR “emergency care” OR “primary care” OR “general practitioner” OR “GP” OR “General pract? visit” OR “GP visit?” OR “GP consult?” OR “General pract? consult?” OR “medical consult?” “GP services” OR “General practitioner services” OR “physician visit” OR “Family Physician” OR Dental OR Dentist OR dentistry OR “Eye care” OR Optician OR “Oral health” OR Pharmacy OR pharmacies OR “pharmacy service” OR “Secondary care” OR Hospital OR “Hospital visit” OR “hospital admission” OR “Day patient” OR in-patient OR “inpatient” OR outpatient OR out-patient OR referral OR therap? OR “Preventative healthcare” OR “preventative health care” OR “preventative health-care“ OR “preventative service” OR “preventative medicine” OR “health outreach” OR screen? OR vaccinat? OR “Palliative care” OR “Case manag?” OR “Community care” OR “Community nurse” OR “Community services?” OR “Tertiary care” OR “tertiary health care” OR “tertiary healthcare” OR “tertiary health-care” OR specialist OR “specialist health service” OR “Mental health service” OR “sexual health service”) OR MAINSUBJECT.EXACT.EXPLODE (“Health care”) |
| 6 | Health inequality | ti, ab, if (“Health Equity” OR “Healthcare disparit?”OR Inequalit? OR disparit? OR “Healthcare Disparit?” OR “Health care Disparit?” OR “Health-care Disparit?” OR “Health Care Inequalit?” “Healthcare Inequalit?” OR “Health-care Inequalit?” OR “inequalit? in healthcare” OR “inequalit? in health care” OR “inequality in health-care” OR “disparit? in healthcare” OR “disparit? in health care” OR “disparit? in health-care” OR “inequit?” OR “health inequit?”) OR MAINSUBJECT.EXACT (“Health inequalities”) |
| 5 | MLTCs + Ethnicity + Country | (#1 AND #2 AND #3) NOT #4 ((MAINSUBJECT.EXACT.EXPLODE (“Mixed ethnicity”) OR MAINSUBJECT.EXACT.EXPLODE (“Ethnicity”) OR ab,ti,if (“Ethnic Group?” OR “african continental ancestry group” OR Arab OR Africa? OR Afro? OR Asian OR “Asian Continental Ancestry Group” OR “Asylum seeker” OR Bangladesh? OR Black OR “BME” OR “BAME” OR Caribbean OR China OR Chinese OR Cultur? OR Divers? OR Ethnic? OR Gypsy OR India? OR Irish OR Migrant OR Minorit? OR Mixed OR “Mixed ethnic?” OR “Multiple ethnic?” OR Multi$rac? OR ‘Other White’ OR Pakistan? OR Roma OR “White Other” OR Refugee? OR race OR racial? OR “South Asian” OR “European Continental Ancestry Group”)) AND (MAINSUBJECT. EXACT (“England and Wales”) OR MAINSUBJECT.EXACT (“Channel Islands”) OR MAINSUBJECT.EXACT (“UK”) OR MAINSUBJECT.EXACT (“Scotland”) OR MAINSUBJECT. EXACT (“England”) OR MAINSUBJECT.EXACT (“Northern Ireland”) OR MAINSUBJECT. EXACT (“Wales”) OR ti, ab, if (“United Kingdom” OR “UK” OR England OR Wales OR Scotland OR “Northern Ireland” OR Britain OR “Great Britain”)) AND (ti, ab, if (“Multiple Chronic Conditions” OR Co$morbid? OR Multi$morbidity OR Multi$patholog? OR “multiple condition?” OR “Multiple health condition?” OR “Multiple health problems” OR “Multiple medical conditions” OR “Multiple medical problems” OR “Pluri$patholog?” OR Polymorbid? OR “multiple illness?” OR “Multiple Chronic Health Conditions” or “Multiple Chronic Medical Conditions” OR “multiple chronic illness?”) OR MAINSUBJECT.EXACT.EXPLODE (“Comorbidity”))) NOT (MAINSUBJECT.EXACT.EXPLODE (“USA”) OR MAINSUBJECT.EXACT.EXPLODE (“North America”) OR MAINSUBJECT.EXACT.EXPLODE (“Canada”) OR MAINSUBJECT.EXACT. EXPLODE (“Australia”) OR MAINSUBJECT.EXACT.EXPLODE (“New Zealand”) OR MAINSUBJECT.EXACT.EXPLODE (“South America”) OR MAINSUBJECT.EXACT. EXPLODE (“Central America”) OR ti, ab, if (“Americas” OR “USA” OR America OR “North America” OR Canada OR Australia OR “New Zealand”)) |
| 4 | excluded countries | MAINSUBJECT.EXACT.EXPLODE (“USA”) OR MAINSUBJECT.EXACT.EXPLODE (“North America”) OR MAINSUBJECT.EXACT.EXPLODE (“Canada”) OR MAINSUBJECT.EXACT. EXPLODE (“Australia”) OR MAINSUBJECT.EXACT.EXPLODE (“New Zealand”) OR MAINSUBJECT.EXACT.EXPLODE (“South America”) OR MAINSUBJECT.EXACT. EXPLODE (“Central America”) OR ti, ab, if (“Americas” OR “USA” OR America OR “North America” OR Canada OR Australia OR “New Zealand”) |
| 3 | Country | (MAINSUBJECT.EXACT (“England and Wales”) OR MAINSUBJECT.EXACT (“Channel Islands”) OR MAINSUBJECT.EXACT (“UK”) OR MAINSUBJECT.EXACT (“Scotland”) OR MAINSUBJECT.EXACT (“England”) OR MAINSUBJECT.EXACT (“Northern Ireland”) OR MAINSUBJECT.EXACT (“Wales”)) OR ti, ab, if (“United Kingdom” OR “UK” OR England OR Wales OR Scotland OR “Northern Ireland” OR Britain OR “Great Britain”) |
| 2 | Ethnicity | (MAINSUBJECT.EXACT.EXPLODE (“Mixed ethnicity”) OR MAINSUBJECT.EXACT. EXPLODE (“Ethnicity”)) OR ab,ti,if (“Ethnic Group?” OR “african continental ancestry group” OR Arab OR Africa? OR Afro? OR Asian OR “Asian Continental Ancestry Group” OR “Asylum seeker” OR Bangladesh? OR Black OR “BME” OR “BAME” OR Caribbean OR China OR Chinese OR Cultur? OR Divers? OR Ethnic? OR Gypsy OR India? OR Irish OR Migrant OR Minorit? OR Mixed OR “Mixed ethnic?” OR “Multiple ethnic?” OR Multi$rac? OR ‘Other White’ OR Pakistan? OR Roma OR “White Other” OR Refugee? OR race OR racial? OR “South Asian” OR “European Continental Ancestry Group”) |
| 1 | Multiple long-term conditions (MLTCs) | ti, ab, if (“Multiple Chronic Conditions” OR Co$morbid? OR Multi$morbidity OR Multi$patholog? OR “multiple condition?” OR “Multiple health condition?” OR “Multiple health problems” OR “Multiple medical conditions” OR “Multiple medical problems” OR “Pluri$patholog?” OR Polymorbid? OR “multiple illness?” OR “Multiple Chronic Health Conditions” or “Multiple Chronic Medical Conditions” OR “multiple chronic illness?”) OR MAINSUBJECT.EXACT.EXPLODE (“Comorbidity”) |
References
- Moriarty, J. Long Term Conditions; Briefing Paper; Race Equality Foundation: London, UK, 2021. [Google Scholar]
- Stafford, M.; Steventon, A.; Thorlby, R.; Fisher, R.; Turton, C.; Deeny, S. Briefing: Understanding the Health Care Needs of People with Multiple Health Conditions [Online]. 2018. Available online: https://www.health.org.uk/sites/default/files/upload/publications/2018/Understanding%20the%20health%20care%20needs%20of%20people%20with%20multiple%20health%20conditions.pdf (accessed on 2 June 2021).
- National Institute for Health and Care Excellence. Multimorbidity [Online]. 2018. Available online: https://cks.nice.org.uk/topics/multimorbidity/ (accessed on 2 June 2021).
- Kingston, A.; Robinson, L.; Booth, H.; Knapp, M.; Jagger, C. Projections of multi-morbidity in the older population in England to 2035: Estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing 2018, 47, 374–380. [Google Scholar] [CrossRef]
- Whitty, C.J.M.; MacEwen, C.; Goddard, A.; Alderson, D.; Marshall, M.; Calderwood, C.; Atherton, F.; McBride, M.; Atherton, J.; Stokes-Lampard, H.; et al. Rising to the challenge of multimorbidity. BMJ 2020, 368, l6964. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multi- morbidity and implications for health care, research and medical education: A cross-sectional study. Lancet Online 2012, 380, 37–43. [Google Scholar] [CrossRef]
- The Academy of Medical Sciences. Multimorbidity: A Priority for Global Health Research. 2018. Available online: https://acmedsci.ac.uk/file-download/82222577 (accessed on 27 July 2021).
- Soley-Bori, M.; Ashworth, M.; Bisquera, A.; Dodhia, H.; Lynch, R.; Wang, Y.; Fox-Rushby, J. Impact of multimorbidity on healthcare costs and utilisation: A systematic review of the UK literature. Br. J. Gen. Pract. 2021, 71, e39–e46. [Google Scholar] [CrossRef] [PubMed]
- Sinnott, C.; Mc Hugh, S.; Browne, J.; Bradley, C. GPs’ perspectives on the management of patients with multimorbidity: Systematic review and synthesis of qualitative research. BMJ Open 2013, 3, e003610. [Google Scholar] [CrossRef] [PubMed]
- Gill, A.; Kuluski, K.; Jaakkimainen, L.; Naganathan, G.; Upshur, R.; Wodchis, W.P. “Where do we go from here?” Health system frustrations expressed by patients with multimorbidity, their caregivers and family physicians. Healthc. Policy 2014, 9, 73–89. [Google Scholar] [CrossRef]
- Hays, R.; Daker-White, G.; Esmail, A.; Barlow, W.; Minor, B.; Brown, B.; Blakeman, T.; Sanders, C.; Bower, P. Threats to patient safety in primary care reported by older people with multimorbidity: Baseline findings from a longitudinal qualitative study and implications for intervention. BMC Health Serv. Res. 2017, 17, 754. [Google Scholar] [CrossRef]
- Saltus, R.; Pithara, C. “Care from the heart”: Older minoritised women’s perceptions of dignity in care. IJMHSC 2015, 11, 57–70. [Google Scholar] [CrossRef]
- Solomon, D.; Tariq, S.; Alldis, J.; Burns, F.; Gilson, R.; Sabin, C.; Sherr, L.; Pettit, F.; Dhairyawan, R. Ethnic inequalities in mental health and socioeconomic status among older women living with HIV: Results from the PRIME Study. STI 2021, in press. [Google Scholar] [CrossRef]
- Saeed, A.; Rae, E.; Neil, R.; Connell-Hall, V.; Munro, F. To BAME or not to BAME: The Problem with Racial Terminology in the Civil Service. 2019. Available online: https://www.civilserviceworld.com/news/article/to-bame-or-not-to-bame-the-problem-with-racial-terminology-in-the-civil-service (accessed on 1 November 2021).
- Bunglawala, Z. Civil Service Blog: Please, don’t Call Me BAME or BME! 2019. Available online: https://civilservice.blog.gov.uk/2019/07/08/please-dont-call-me-bame-or-bme/ (accessed on 1 November 2021).
- Brah, A. Cartographies of Diaspora: Contesting Identities; Routledge: London, UK, 1996. [Google Scholar]
- Dawson, E. Equity, Exclusion and Everyday Science Learning: The Experiences of Minoritised Groups; Routledge: Abingdon, UK, 2019. [Google Scholar]
- Verest, W.; Galenkamp, H.; Spek, B.; Snijder, M.B.; Stronks, K.; van Valkengoed, I.G.M. Do ethnic inequalities in multimorbidity reflect ethnic differences in socioeconomic status? The HELIUS study. Eur. J. Public Health 2019, 29, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Guy’s and St Thomas’ Charity. From One to Many. Exploring People’s Progression to Multiple Long-Term Conditions in an Urban Environment. 2018. Available online: https://www.gsttcharity.org.uk/sites/default/files/GSTTC_MLTC_Report_2018.pdf (accessed on 16 May 2021).
- Hayanga, B.; Bécares, L.; Stafford, M. A Systematic Review and Narrative Synthesis of Ethnic Inequalities in Multiple Long-Term Health Conditions in the United Kingdom; School of Education and Social Work, University of Sussex: Brighton, UK, [Manuscript submitted for publication].
- Impact on Urban Health. Easing Pressures, How Work, Money and Homes Can Make Our Cities Healthier and Fairer. 2021. Available online: https://urbanhealth.org.uk/insights/reports/easing-pressures-how-work-money-and-homes-can-make-our-cities-healthier-and-fairer (accessed on 5 August 2021).
- Nazroo, J.Y. The structuring of ethnic inequalities in health: Economic position, racial discrimination, and racism. Am. J. Public Health 2003, 93, 277–284. [Google Scholar] [CrossRef] [PubMed]
- The Richmond Group of Charities, Impact on Urban Health. You only Had to Ask. What People with Multiple Conditions Say about Health Equity. A Report from the Taskforce on Multiple Conditions. July 2021. Available online: https://richmondgroupofcharities.org.uk/sites/default/files/youonlyhadtoask_fullreport_july2021_final.pdf (accessed on 29 July 2021).
- Livingston, G.; Leavey, G.; Kitchen, G.; Manela, M.; Sembhi, S.; Katona, C. Accessibility of health and social services to immigrant elders: The Islington Study. Br. J. Psychiatry 2002, 180, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Raleigh, V.; Holmes, J. The Health of People from Ethnic Minority Groups in England [Online]. 2021. Available online: https://www.kingsfund.org.uk/publications/health-people-ethnic-minority-groups-england#Diabetes (accessed on 25 May 2021).
- Race Disparity Unit. Patient Experience of Primary Care: GP Services. 2019. Available online: https://www.ethnicity-facts-figures.service.gov.uk/health/patient-experience/patient-experience-of-primary-care-gp-services/latest#by-ethnicity (accessed on 29 July 2021).
- Essink-Bot, M.-L.; Lamkaddem, M.; Jellema, P.; Nielsen, S.S.; Stronks, K. Interpreting ethnic inequalities in healthcare consumption: A conceptual framework for research. Eur. J. Public Health 2012, 23, 922–926. [Google Scholar] [CrossRef] [PubMed]
- Rees, P.; Wohland, P.; Norman, P.; Boden, P. Ethnic population projections for the UK, 2001–2051. J. Pop Res. 2012, 29, 45–89. [Google Scholar] [CrossRef]
- Dixon-Woods, M.; Kirk, D.; Agarwal, S.; Annandale, E.; Arthur, T.; Harvey, J.; Hsu, R.; Katbamna, S.; Olsen, R.; Smith, L.; et al. Vulnerable Groups and Access to Health Care: A Critical Interpretive Review. 2005. Available online: https://www.menshealthforum.org.uk/sites/default/files/pdf/sdovulnerablegroups2005.pdf (accessed on 23 July 2021).
- Norredam, M.; Nielsen, S.S.; Krasnik, A. Migrants’ utilization of somatic healthcare services in Europe—A systematic review. Eur. J. Public Health 2009, 20, 555–563. [Google Scholar] [CrossRef]
- Beach, M.C.; Gary, T.L.; Price, E.G.; Robinson, K.; Gozu, A.; Palacio, A.; Smarth, C.; Jenckes, M.; Feuerstein, C.; Bass, E.B.; et al. Improving health care quality for racial/ethnic minorities: A systematic review of the best evidence regarding provider and organization interventions. BMC Public Health 2006, 6, 104. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRIMSA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Fortin, M.; Stewart, M.; Poitras, M.E.; Almirall, J.; Maddocks, H. A systematic review of prevalence studies on multimorbidity: Toward a more uniform methodology. Ann. Fam. Med. 2012, 10, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Robertson, R. How Does the NHS Compare Internationally? Big Election Questions. 2017. Available online: https://www.kingsfund.org.uk/publications/articles/big-election-questions-nhs-international-comparisons (accessed on 28 May 2021).
- Coleman, D. Projections of the Ethnic Minority Populations of the United Kingdom 2006–2056. Pop Dev. Rev. 2010, 36, 441–486. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health Research. Multiple Long-Term Conditions (Multimorbidity): Making Sense of the Evidence [Online]. 2021. Available online: https://evidence.nihr.ac.uk/collection/making-sense-of-the-evidence-multiple-long-term-conditions-multimorbidity/ (accessed on 2 June 2021).
- Feinstein, A.R. The pre-therapeutic classification of co-morbidity in chronic disease. J. Chronic Dis. 1970, 23, 455–468. [Google Scholar] [CrossRef]
- Department of Health. Comorbidities. A Framework of Principles for System-Wide Action. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/307143/Comorbidities_framework.pdf (accessed on 25 October 2021).
- Cassell, A.; Edwards, D.; Harshfield, A.; Rhodes, K.; Brimicombe, J.; Payne, R.; Griffin, S. The epidemiology of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2018, 68, e245–e251. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.; Britt, H.; Miller, G.; Henderson, J. Examining different measures of multimorbidity, using a large prospective cross-sectional study in Australian general practice. BMJ Open 2014, 4, e004694. [Google Scholar] [CrossRef] [PubMed]
- Carrasquillo, O. Health Care Utilization. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 909–910. [Google Scholar]
- Arueira Chaves, L.; de Souza Serio dos Santos, D.M.; Rodrigues Campos, M.; Luiza, V.L. Use of health outcome and health service utilization indicators as an outcome of access to medicines in Brazil: Perspectives from a literature review. Public Health Rev. 2019, 40, 5. [Google Scholar] [CrossRef] [PubMed]
- Camenzind, P.A. Explaining regional variations in health care utilization between Swiss cantons using panel econometric models. BMC Health Serv. Res. 2012, 12, 62. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. Understanding Quality Measurement. 2021. Available online: https://www.ahrq.gov/patient-safety/quality-resources/tools/chtoolbx/understand/index.html#:~:text=The%20Institute%20of%20Medicine%20defines%20health%20care%20quality,as%20having%20the%20following%20properties%20or%20domains%3A%20Effectiveness (accessed on 27 October 2021).
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Hanefeld, J.; Powell-Jackson, T.; Balabanova, D. Understanding and measuring care quality: Dealing with complexity. Bull. World Health Organ. 2017, 95, 368–374. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Barron, E.; Bakhai, C.; Kar, P.; Weaver, A.; Bradley, D.; Ismail, H.; Knighton, P.; Holman, N.; Khunti, K.; Sattar, N.; et al. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: A whole-population study. Lancet Diabetes Endocrinol. 2020, 8, 813–822. [Google Scholar] [CrossRef]
- Wijlaars, L.P.M.M.; Hardelid, P.; Guttmann, A.; Gilbert, R. Emergency admissions and long-term conditions during transition from paediatric to adult care: A cross-sectional study using Hospital Episode Statistics data. BMJ Open 2018, 8, e021015. [Google Scholar] [CrossRef]
- Barry, E.; Laverty, A.A.; Majeed, A.; Millett, C. Ethnic group variations in alcohol-related hospital admissions in England: Does place matter? Ethn. Health 2015, 20, 557–563. [Google Scholar] [CrossRef]
- Graham, H.L.; Maslin, J.; Copello, A.; Birchwood, M.; Mueser, K.; McGovern, D.; Georgiou, G. Drug and alcohol problems amongst individuals with severe mental health problems in an inner city area of the UK. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Davies, M.J.; Ali, S.; Taub, N.A.; Stone, M.A.; Baker, R.; McNally, P.G.; Lawrence, I.G.; Khunti, K. Association of cardiac and non-cardiac chronic disease comorbidity on glycaemic control in a multi-ethnic population with type 1 and type 2 diabetes. Postgrad. Med. J. 2011, 87, 763–768. [Google Scholar] [CrossRef]
- Afuwape, S.A.; Johnson, S.; Craig, T.J.K.; Miles, H.; Leese, M.; Mohan, R.; Thornicroft, G. Ethnic differences among a community cohort of individuals with dual diagnosis in South London. J. Ment. Health 2006, 15, 551–567. [Google Scholar] [CrossRef]
- Alshamsan, R.; Majeed, A.; Vamos, E.P.; Khunti, K.; Curcin, V.; Rawaf, S.; Millett, C. Ethnic differences in diabetes management in patients with and without comorbid medical conditions: A cross-sectional study. Diabetes Care 2011, 34, 655–657. [Google Scholar] [CrossRef] [PubMed]
- Earle, K.; Porter, K.; Ostberg, J.; Yudkin, J. Variation in the progression of diabetic nephropathy according to racial origin. Nephrol. Dial. Transplant. 2001, 16, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Mathur, R.; Dreyer, G.; Yaqoob, M.M.; Hull, S.A. Ethnic differences in the progression of chronic kidney disease and risk of death in a UK diabetic population: An observational cohort study. BMJ Open 2018, 8, e020145. [Google Scholar] [CrossRef]
- Mathur, R.; Hull, S.A.; Badrick, E.; Robson, J. Cardiovascular multimorbidity: The effect of ethnicity on prevalence and risk factor management. Br. J. Gen. Pract. 2011, 61, e262–e270. [Google Scholar] [CrossRef]
- Pinto, R.; Ashworth, M.; Seed, P.; Rowlands, G.; Schofield, P.; Jones, R. Differences in the primary care management of patients with psychosis from two ethnic groups: A population-based cross-sectional study. Fam. Pract. 2010, 27, 439–446. [Google Scholar] [CrossRef]
- Schofield, P.; Baawuah, F.; Seed, P.T.; Ashworth, M. Managing hypertension in general practice: A cross-sectional study of treatment and ethnicity. Br. J. Gen. Pract. 2012, 62, e703–e709. [Google Scholar] [CrossRef][Green Version]
- Das-Munshi, J.; Schofield, P.; Ashworth, M.; Gaughran, F.; Hull, S.; Ismail, K.; Robson, J.; Stewart, R.; Mathur, R. Inequalities in glycaemic management in people living with type 2 diabetes mellitus and severe mental illnesses: Cohort study from the UK over ten year. BMJ Open Diabetes Res. Care 2021, 9, e002118. [Google Scholar] [CrossRef]
- Prady, S.L.; Pickett, K.E.; Gilbody, S.; Petherick, E.S.; Mason, D.; Sheldon, T.A.; Wright, J. Variation and ethnic inequalities in treatment of common mental disorders before, during and after pregnancy: Combined analysis of routine and research data in the Born in Bradford cohort. BMC Psychiatry 2016, 16, 99. [Google Scholar] [CrossRef]
- Kwon, I.; Shin, O.; Park, S.; Kwon, G. Multi-Morbid Health Profiles and Specialty Healthcare Service Use: A Moderating Role of Poverty. IJERPH 2019, 16, 1956. [Google Scholar] [CrossRef]
- Collins, P.; Bilge, S. Intersectionality; Polity Press: Cambridge, UK, 2016. [Google Scholar]
- Rivenbark, J.G.; Ichou, M. Discrimination in healthcare as a barrier to care: Experiences of socially disadvantaged populations in France from a nationally representative survey. BMC Public Health 2020, 20, 31. [Google Scholar] [CrossRef]
- Adegbembo, A.O.; Tomar, S.L.; Logan, H.L. Perception of racism explains the difference between Blacks’ and Whites’ level of healthcare trust. Ethn. Dis. 2006, 16, 792–798. [Google Scholar]
- Sabbah, W.; Gireesh, A.; Chari, M.; Delgado-Angulo, E.K.; Bernabé, E. Racial Discrimination and Uptake of Dental Services among American Adults. Int. J. Environ. Res. Public Health 2019, 16, 1558. [Google Scholar] [CrossRef] [PubMed]
- Ben, J.; Cormack, D.; Harris, R.; Paradies, Y.C. Racism and health service utilisation: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189900. [Google Scholar] [CrossRef] [PubMed]
- Stoll, C.R.T.; Izadi, S.; Fowler, S.; Green, P.; Suls, J.; Colditz, G.A. The value of a second reviewer for study selection in systematic reviews. Res. Synth. Methods 2019, 10, 539–545. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Multimorbidity: Clinical Assessment and Management. NICE Guideline [NG56]. 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 16 August 2021).
- Salisbury, C.; Man, M.S.; Bower, P.; Guthrie, B.; Chaplin, K.; Gaunt, D.M.; Brookes, S.; Fitzpatrick, B.; Gardner, C.; Hollinghurst, S.; et al. Management of multimorbidity using a patient-centred care model: A pragmatic cluster-randomised trial of the 3D approach. Lancet 2018, 392, 41–50. [Google Scholar] [CrossRef]
- Mann, C.; Shaw, A.; Wye, L.; Salisbury, C.; Guthrie, B. A computer template to enhance patient-centredness in multimorbidity reviews: A qualitative evaluation in primary care. Br. J. Gen. Pract. 2018, 68, e495. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, M.J.; van den Broeke, J.R.; Stronks, K.; Plochg, T. Patients with multimorbidity and their experiences with the healthcare process: A scoping review. J. Comorb. 2017, 7, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Mathur, R.; Bhaskaran, K.; Chaturvedi, N.; Leon, D.A.; vanStaa, T.; Grundy, E.; Smeeth, L. Completeness and usability of ethnicity data in UK-based primary care and hospital databases. J. Public Health 2014, 36, 684–692. [Google Scholar] [CrossRef]
- Saunders, C.L.; Abel, G.A.; El Turabi, A.; Ahmed, F.; Lyratzopoulos, G. Accuracy of routinely recorded ethnic group information compared with self-reported ethnicity: Evidence from the English Cancer Patient Experience survey. BMJ Open 2013, 3, e002882. [Google Scholar] [CrossRef]
- Scobie, S.; Spencer, J.; Raleig, V. Ethnicity coding in English health service datasets. 2021. Available online: https://www.nuffieldtrust.org.uk/files/2021-06/1622731816_nuffield-trust-ethnicity-coding-web.pdf (accessed on 28 November 2021).
- Steventon, A.; Bardsley, M. Use of secondary care in England by international immigrants. J. Health Serv. Res. Policy 2011, 16, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.L.; Steventon, A.; Janta, B.; Stafford, M.; Sinnott, C.; Allen, L.; Deeny, S.R. Healthcare utilization among migrants to the UK: Cross-sectional analysis of two national surveys. J. Health Serv. Res. Policy 2021, 26, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Jayaweera, H.; Quigley, M.A. Health status, health behaviour and healthcare use among migrants in the UK: Evidence from mothers in the Millennium Cohort Study. Soc. Sci. Med. 2010, 71, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Parry, G.; Van Cleemput, P.; Peters, J.; Walters, S.; Thomas, K.; Cooper, C. Health status of Gypsies and Travellers in England. J. Epidemiol. Community Health 2007, 61, 198–204. [Google Scholar] [CrossRef]
- Bécares, L. Which ethnic groups have the poorest health? In Ethnic Identity and Inequalities in Britain; Jivraj, S., Simpson, L., Eds.; Policy Press: Bristol, UK, 2015. [Google Scholar]

| Domains of Healthcare Use/Care Quality | Number of Studies | Sub-Domains of Healthcare Use and Care Quality |
|---|---|---|
| Disease management/monitoring | 6 | |
| Prescriptions | 3 | |
| Use of hospital services | 3 | |
| Mortality/Risk of Mortality | 2 | |
| Disease progression | 2 |
|
| Treatment quality | 2 | |
| Tertiary service utilisation | 1 |
|
| Study ID | Study Design | Geographical Location | Data Source | Sample Size | Participant Characteristics | Ethnic Group Categories | Number of Conditions | Index Condition | Sub-Domain of Healthcare | Covariates |
|---|---|---|---|---|---|---|---|---|---|---|
| Afuwape, 2006 [53] | Retrospective cohort | Local | Comorbidity Dual Diagnosis Study | 213 | %Female: 16; Mean Age: 37 years | White, Black Caribbean, Black African, Black British | 2 | Psychotic illness | Hospital admission, length of stay in hospital, service satisfaction | - |
| Barron, 2020 [48] | Cross-sectional | National | General practice records | 61,414,470 | %Female: 50.1; Mean Age (SD): 40.9 (23.2) | Asian, Black, Mixed, Other, White, Unknown | 2 | Diabetes, | In-hospital mortality | - |
| Barry, 2015 [50] | Cross-sectional | National | Hospital Episode Statistics | 264,870 | %Female: NR; Age: 10+ years | White British, White Irish, Black Caribbean, Black African, SA—Pakistani and Bangladeshi, SA—Indian | 2 | Alcohol-related health conditions | Hospital admissions | - |
| Das-Munshi, 2021 [60] | Longitudinal study | Local | Primary care records | 56,770 | %Female: 46; Mean Age (SD): 63 (14) | White British, Irish, Black African, Black Caribbean, Bangladeshi, Indian, Pakistani, Chinese | 2 | Diabetes | Glycaemic management | age, gender, deprivation |
| Earle, 2001 [55] | Retrospective case note review | Local | Diabetes Outpatient Clinic | 45 | %Female: 36; Mean Age (SD): 66 (8.5) | Indo-Asian, African-Caribbean, Caucasian | 2 | Diabetes | Systolic and diastolic blood pressure, glycaemic control, and usage of ACE inhibitors, β-blockers, calcium channel blockers, α-blockers, diuretics, rate of renal decline, antihypertensive regimen | - |
| Graham, 2001 [51] | Cross-sectional | Local | Community-based Mental Health andSubstance Misuse services | 498 | %Female: 22.2; Age: 18+ years | White UK, African-Caribbean, Asian, European, Irish, Mixed race, Black other, Other | 2 | Severe mental illness | Use of Mental Health and Substance Misuse services | - |
| Mathur, 2018 [56] | Observational community-based cohort study with nested case–control | Local | General practice records | 99,648 | %Female: 56; Age: 25+ years | White, South Asian, Black | 2 | Diabetes | Rate of decline, and risk of death | age, sex and baseline measures of HbA1c, eGFR, CVD, ACE/ARB and diabetes duration |
| Prady, 2016 [61] | Cross-sectional | Local | Primary care records | 2234 | %Female: 100; Mean Age (SD): 26.8 (5.9) | White British, Pakistani, Mixed, Indian, White non-British, Black, Bangladeshi, Other | 2 | Common mental disorders | Drug prescription for common mental disorders | - |
| Schofield, 2012 [59] | Cross-sectional | Local | Lambeth DataNet | 28,320 | %Female: 50.9; Age: 18+ years | White, Mixed, Asian or Asian British, Black or Black British, Chinese or Other | 2 | Hypertension | NICE recommended treatment | - |
| Alshamsan, 2011 [54] | Cross-sectional | Local | Electronic medical records | 6690 | %Female: 49.1; Age: 18 years | White, Black, South Asian | 10 | Diabetes | Diabetes management (HbA1c, total cholesterol, and blood pressure levels) | age, sex, diabetes duration, BMI, socioeconomic status, and practice level clustering |
| Mathur, 2011 [57] | Cross-sectional | Local | Primary care records | 6274 | %Female: NR; Age: 18+ years | White, South Asian, Black, Other | 5 | - | Cardiovascular multimorbidity risk management, cholesterol, blood pressure, blood glucose levels HbA1c levels, statin prescriptions | age and sex, clustered by general practice |
| Mehta, 2011 [52] | Cross-sectional study | Local | Outpatient diabetes clinic | 5664 | %Female: 45.6; Mean Age (SD): 33 (13) | South Asian, White European | 12 | Diabetes | Diabetes management (glycaemic control) | - |
| Pinto, 2010 [58] | Cross-sectional study | Local | Lambeth DataNet | 1090 | %Female: 39.9; Age: 16+ years | White, Black | 5 | Psychosis | Health screening and chronic disease monitoring measures (record of cervical smears, mammograms, cholesterol testing, blood pressure readings and smoking status); BMI recorded | age and IMD-2004 score |
| Wijlaars, 2018 [49] | Cross-sectional study | National | Hospital Episode Statistics | 763,199 | %Female: NR; Age range: 10–24 years | White, Black, Asian, Mixed, Unknown | 9 | - | Emergency admission | age, sex, IMD, transition |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayanga, B.; Stafford, M.; Bécares, L. Ethnic Inequalities in Healthcare Use and Care Quality among People with Multiple Long-Term Health Conditions Living in the United Kingdom: A Systematic Review and Narrative Synthesis. Int. J. Environ. Res. Public Health 2021, 18, 12599. https://doi.org/10.3390/ijerph182312599
Hayanga B, Stafford M, Bécares L. Ethnic Inequalities in Healthcare Use and Care Quality among People with Multiple Long-Term Health Conditions Living in the United Kingdom: A Systematic Review and Narrative Synthesis. International Journal of Environmental Research and Public Health. 2021; 18(23):12599. https://doi.org/10.3390/ijerph182312599
Chicago/Turabian StyleHayanga, Brenda, Mai Stafford, and Laia Bécares. 2021. "Ethnic Inequalities in Healthcare Use and Care Quality among People with Multiple Long-Term Health Conditions Living in the United Kingdom: A Systematic Review and Narrative Synthesis" International Journal of Environmental Research and Public Health 18, no. 23: 12599. https://doi.org/10.3390/ijerph182312599
APA StyleHayanga, B., Stafford, M., & Bécares, L. (2021). Ethnic Inequalities in Healthcare Use and Care Quality among People with Multiple Long-Term Health Conditions Living in the United Kingdom: A Systematic Review and Narrative Synthesis. International Journal of Environmental Research and Public Health, 18(23), 12599. https://doi.org/10.3390/ijerph182312599