
The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
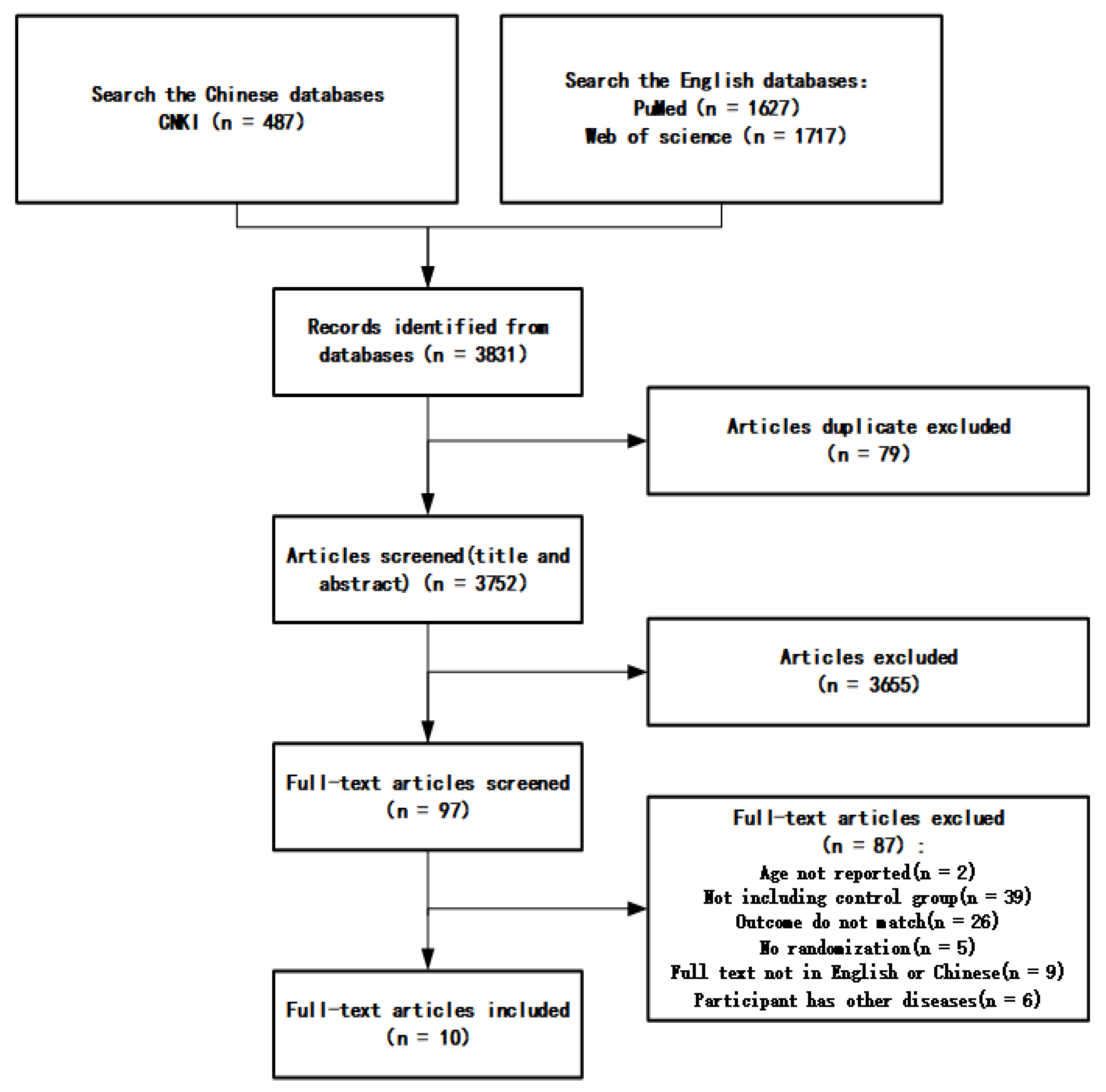
2.1. Search Strategy
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Quality Assessment
2.4. Data Analysis
3. Results
3.1. Basic Information of the Included Studies
3.1.1. Characteristics of the Included Studies
3.1.2. Characteristics of the Interventions in Included Studies and Outcome Indicators
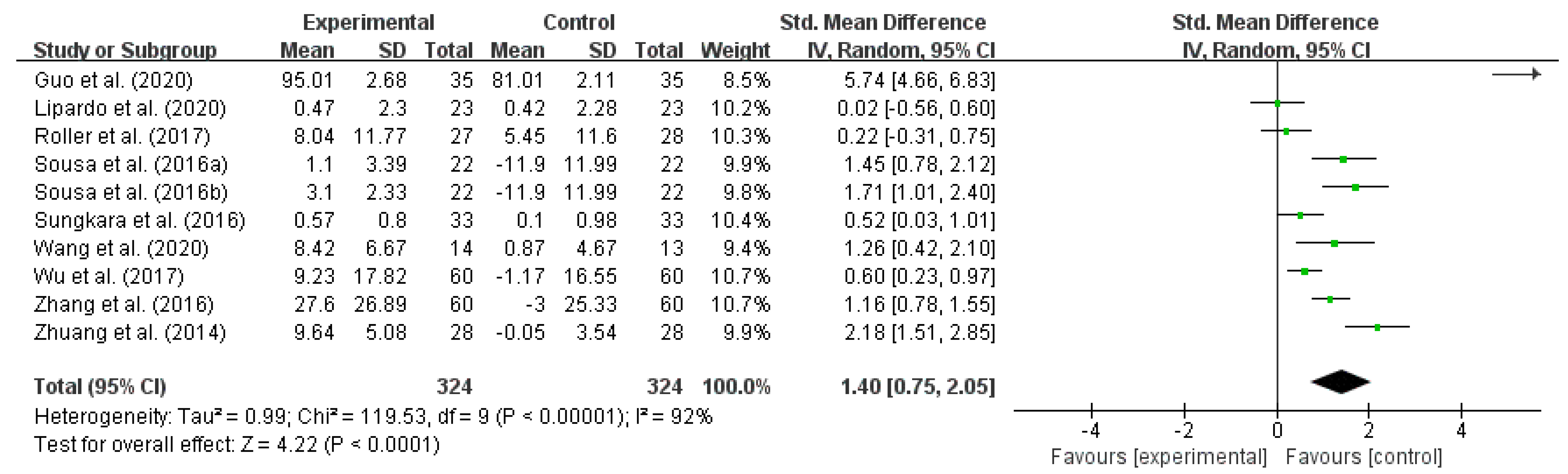
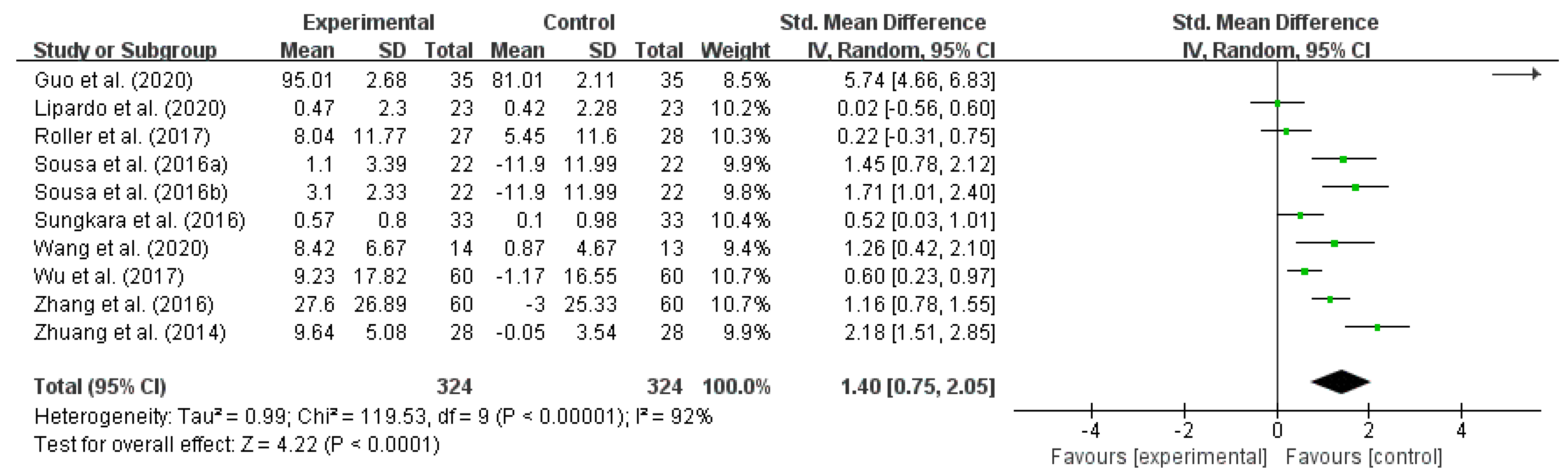
3.2. The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults
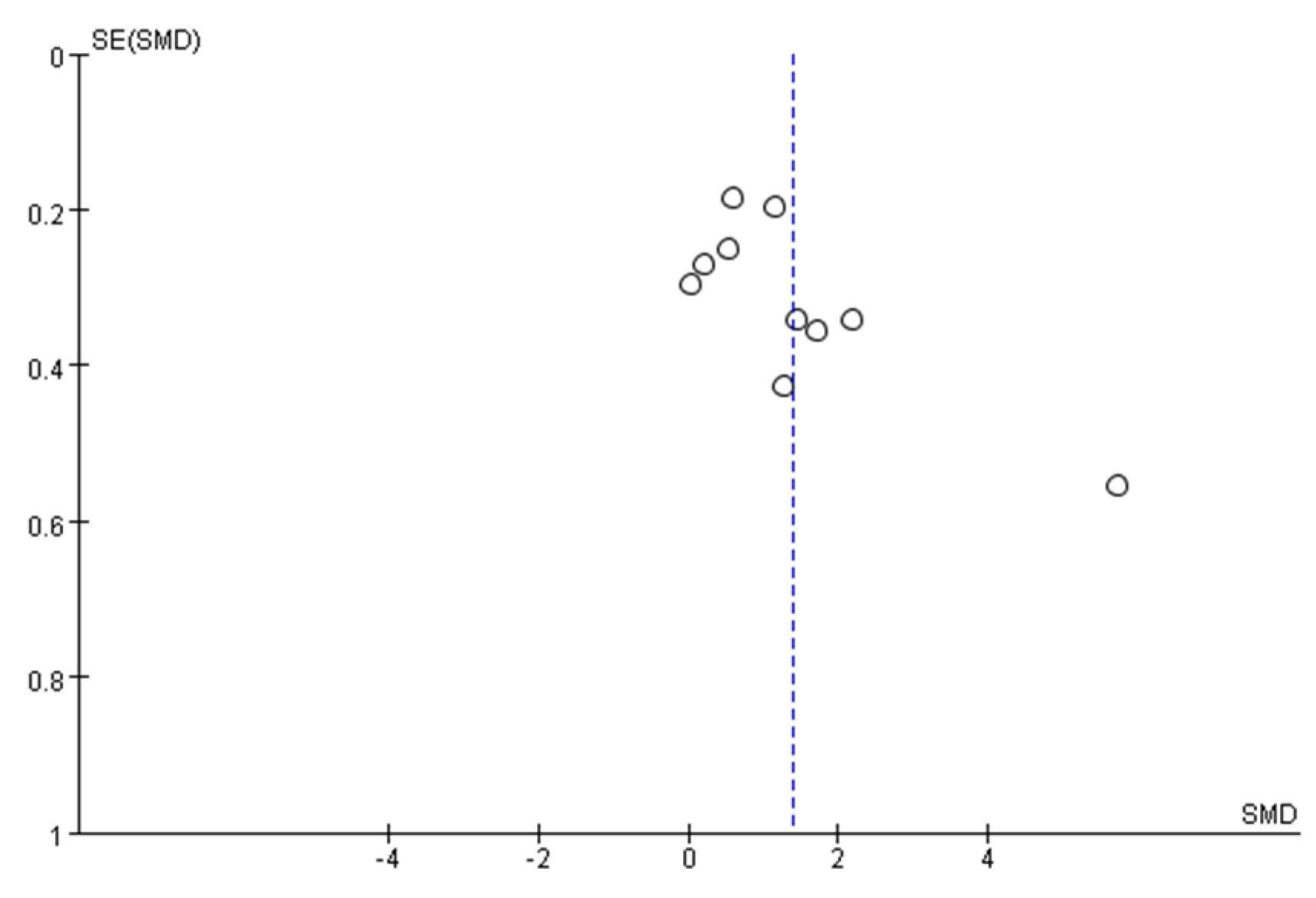
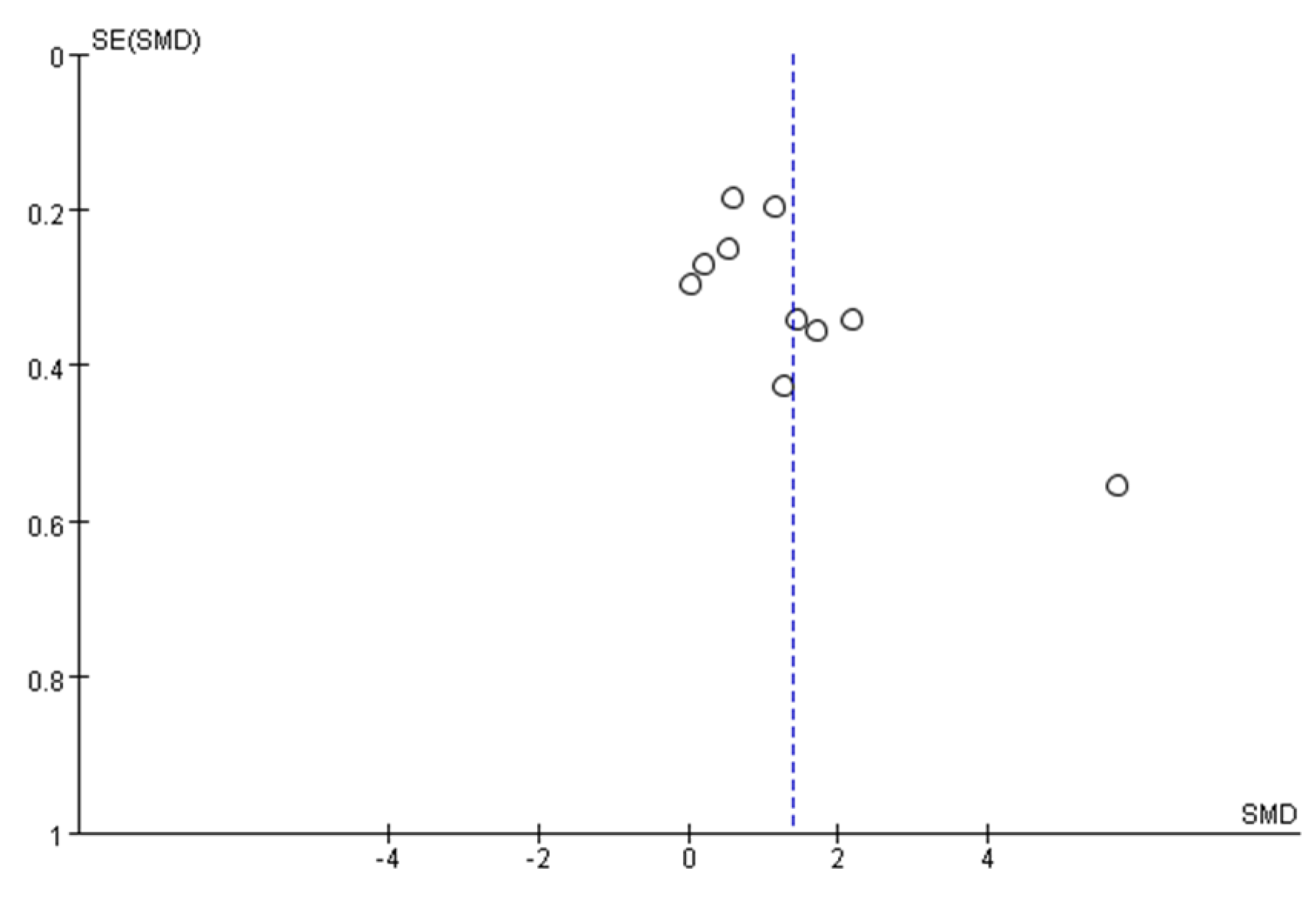
3.3. Publication Bias Assessment
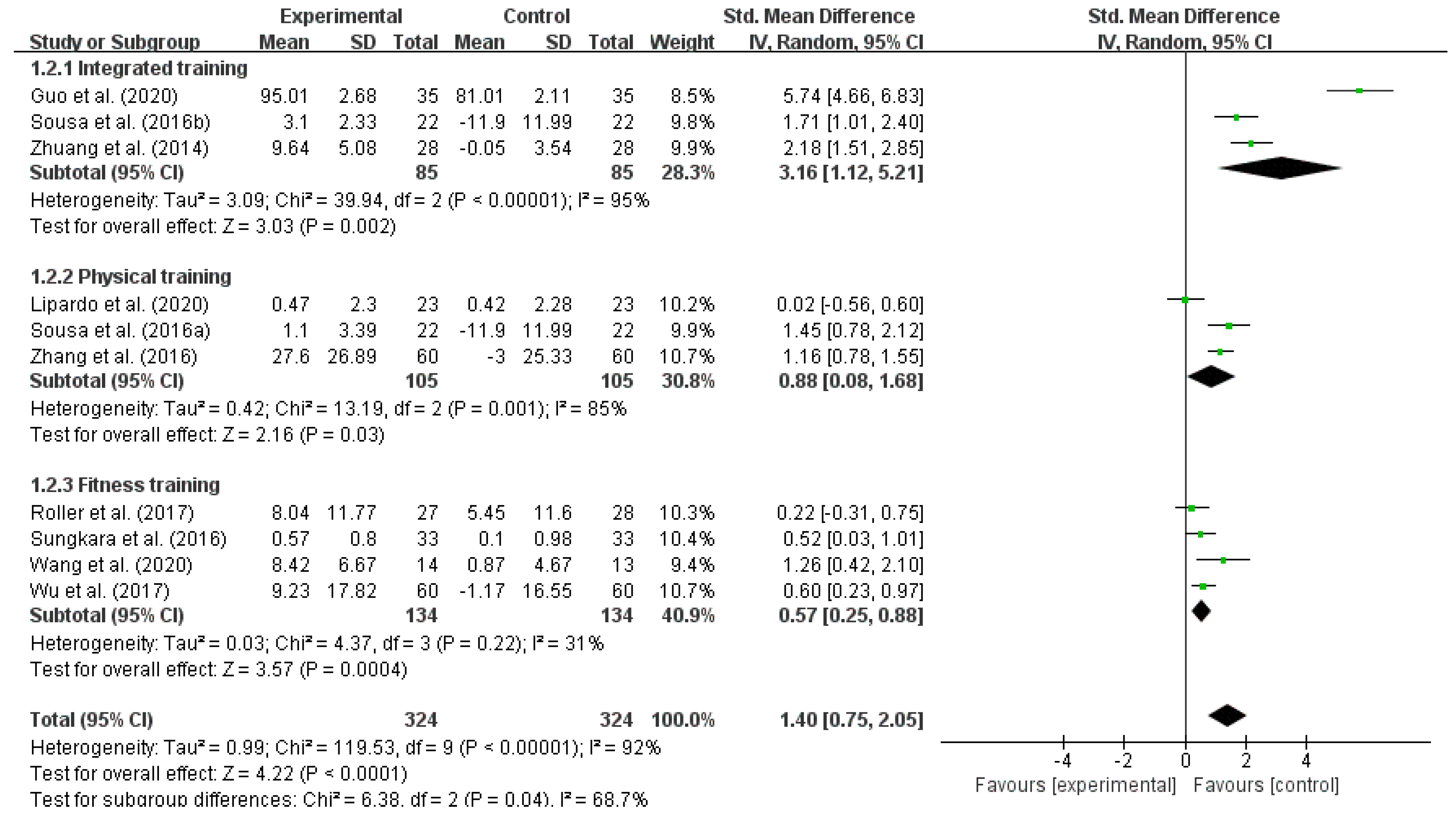
3.4. Results of Subgroup Analysis of Effect Sizes
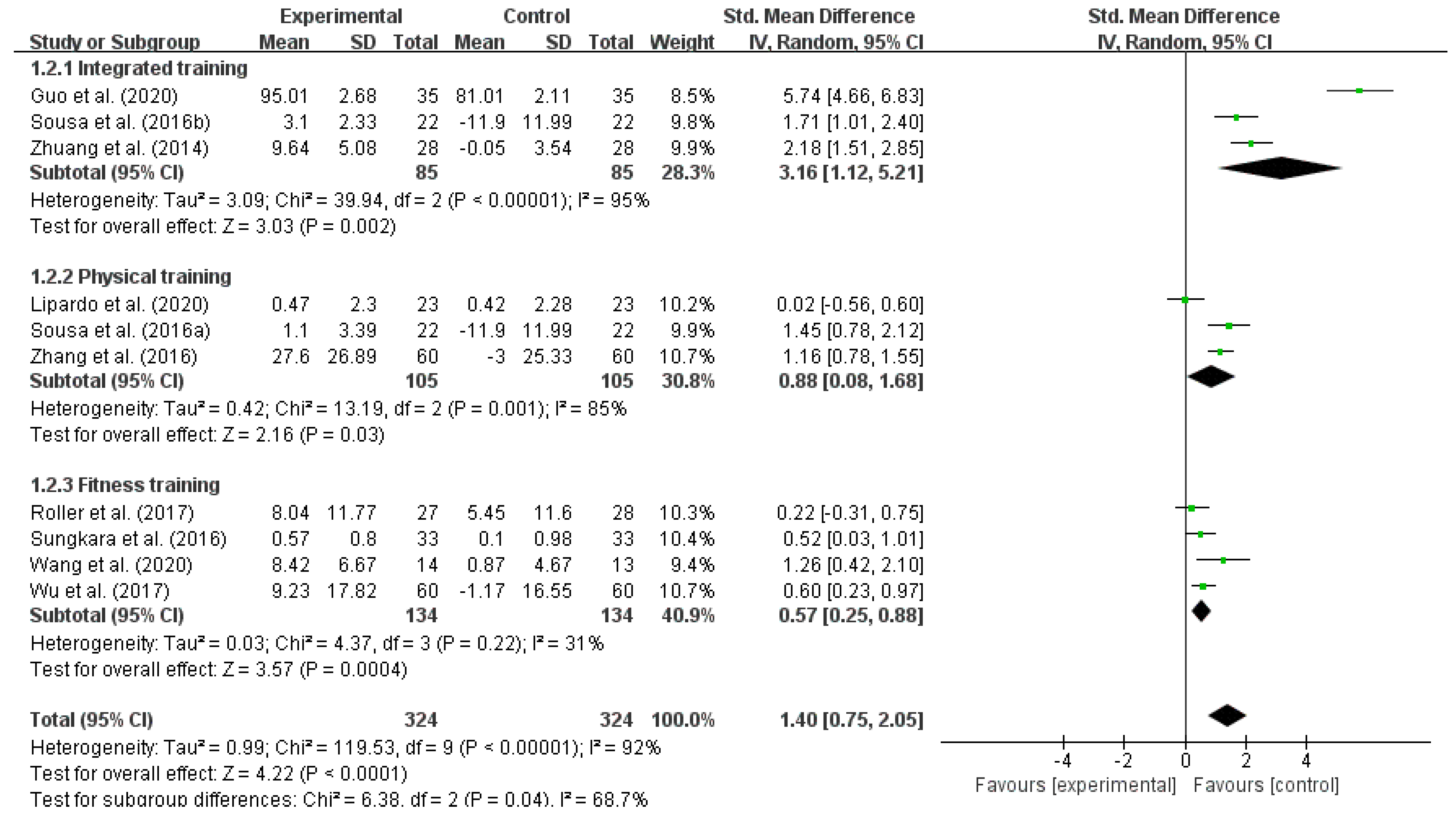
3.4.1. The Effect of Different Types of Exercise Interventions on Reducing the Fall Risk in Older Adults
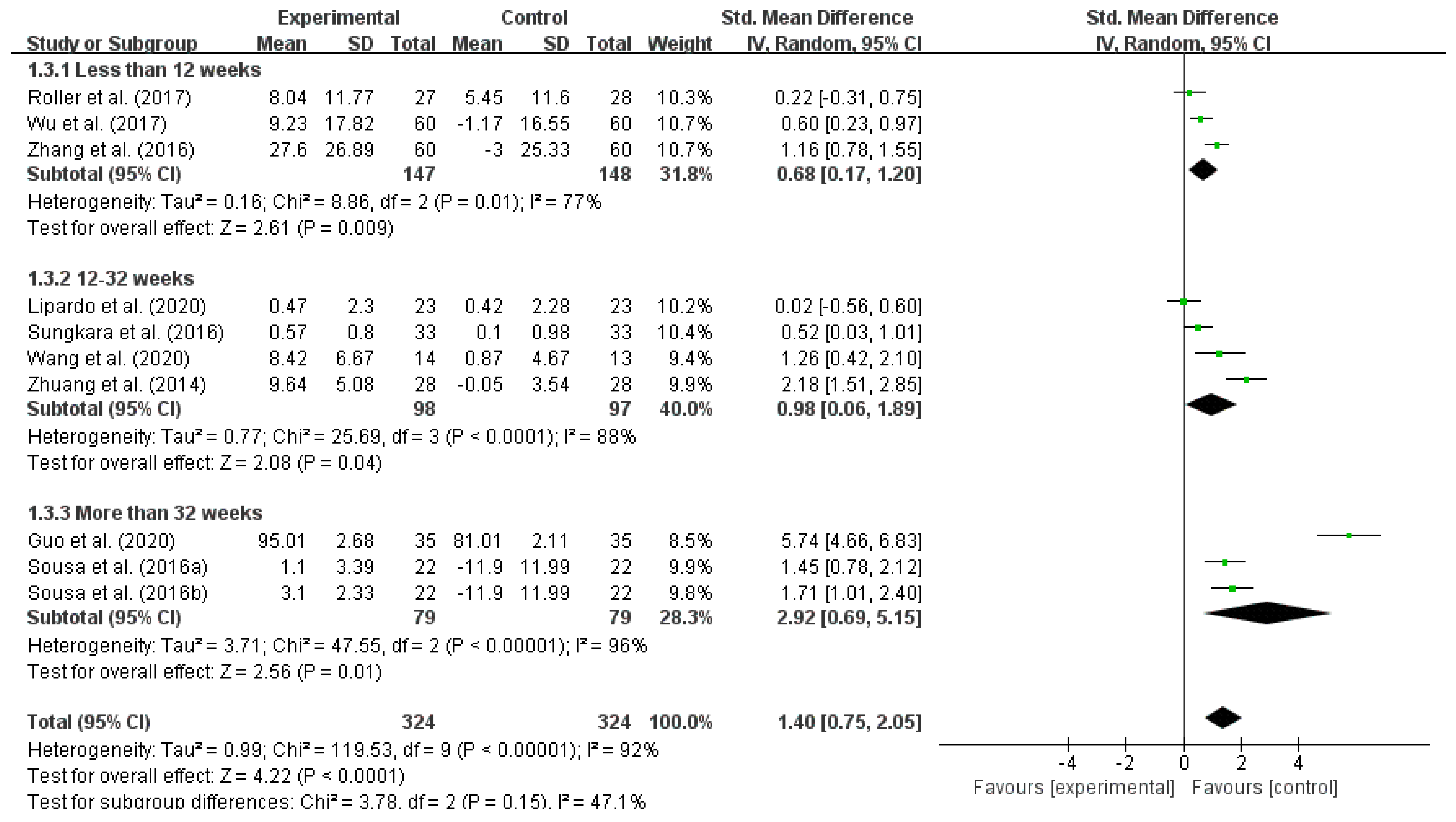
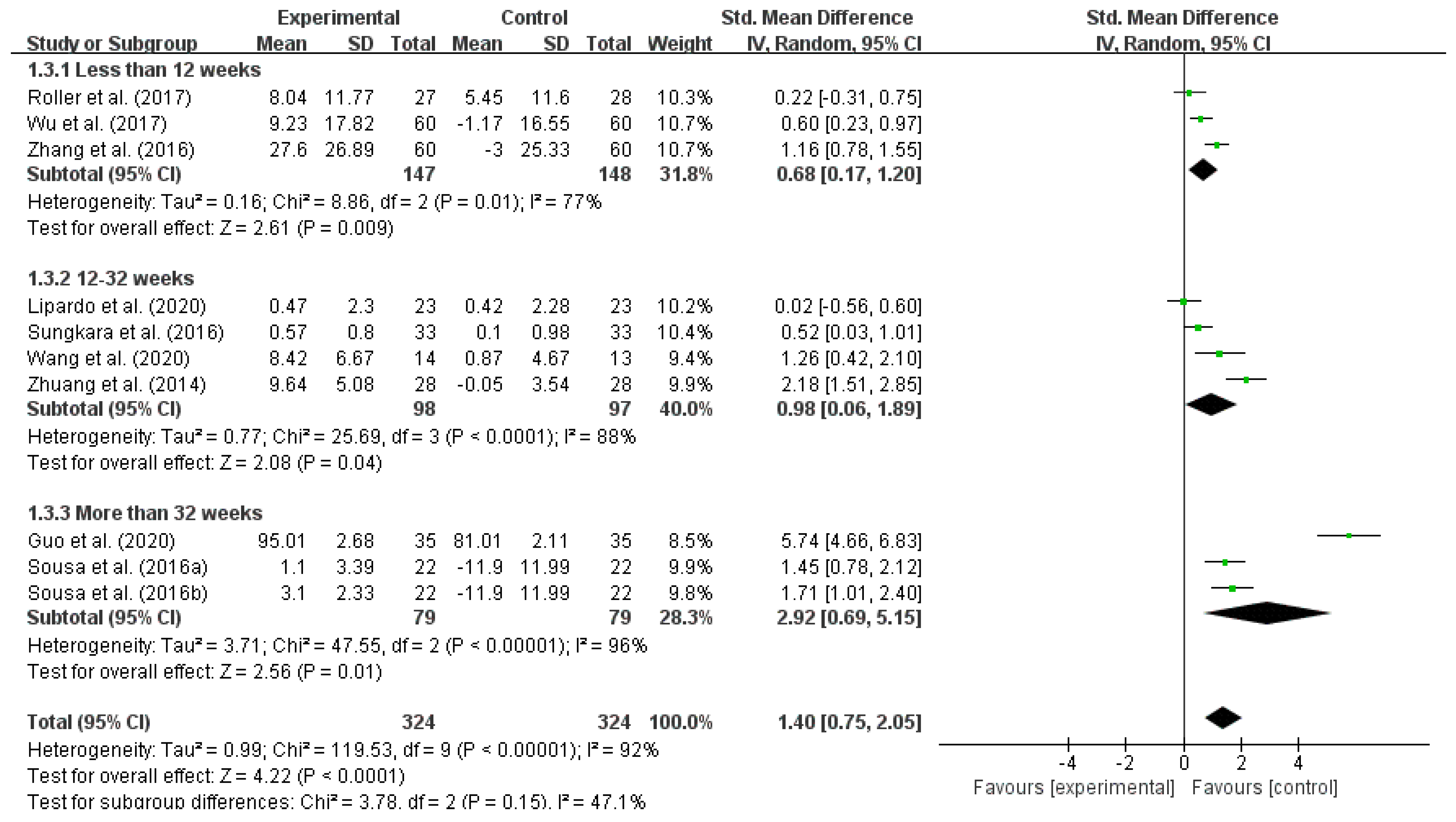
3.4.2. Effect of Different Intervention Durations on Reducing the Fall Risk in Older Adults
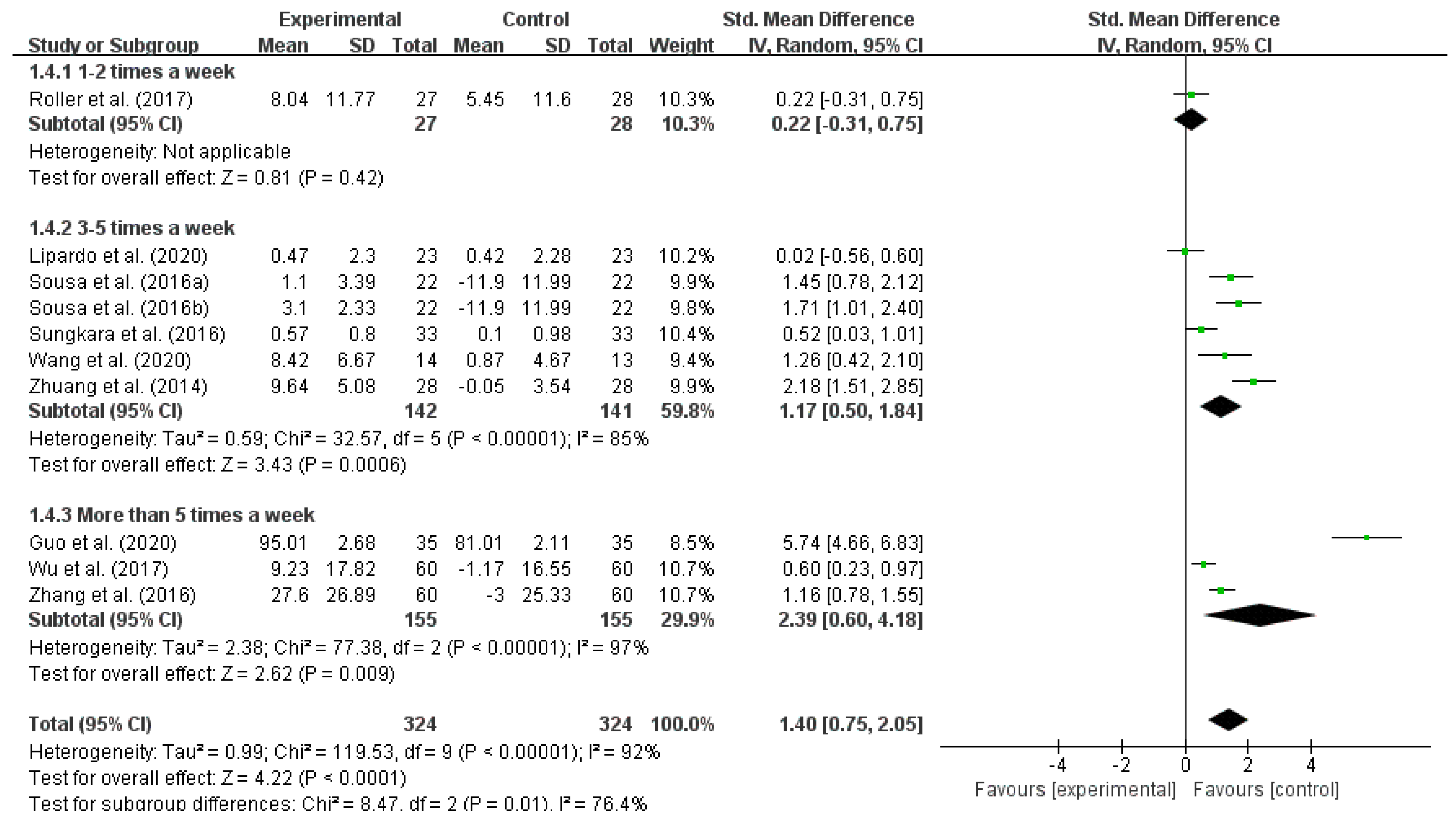
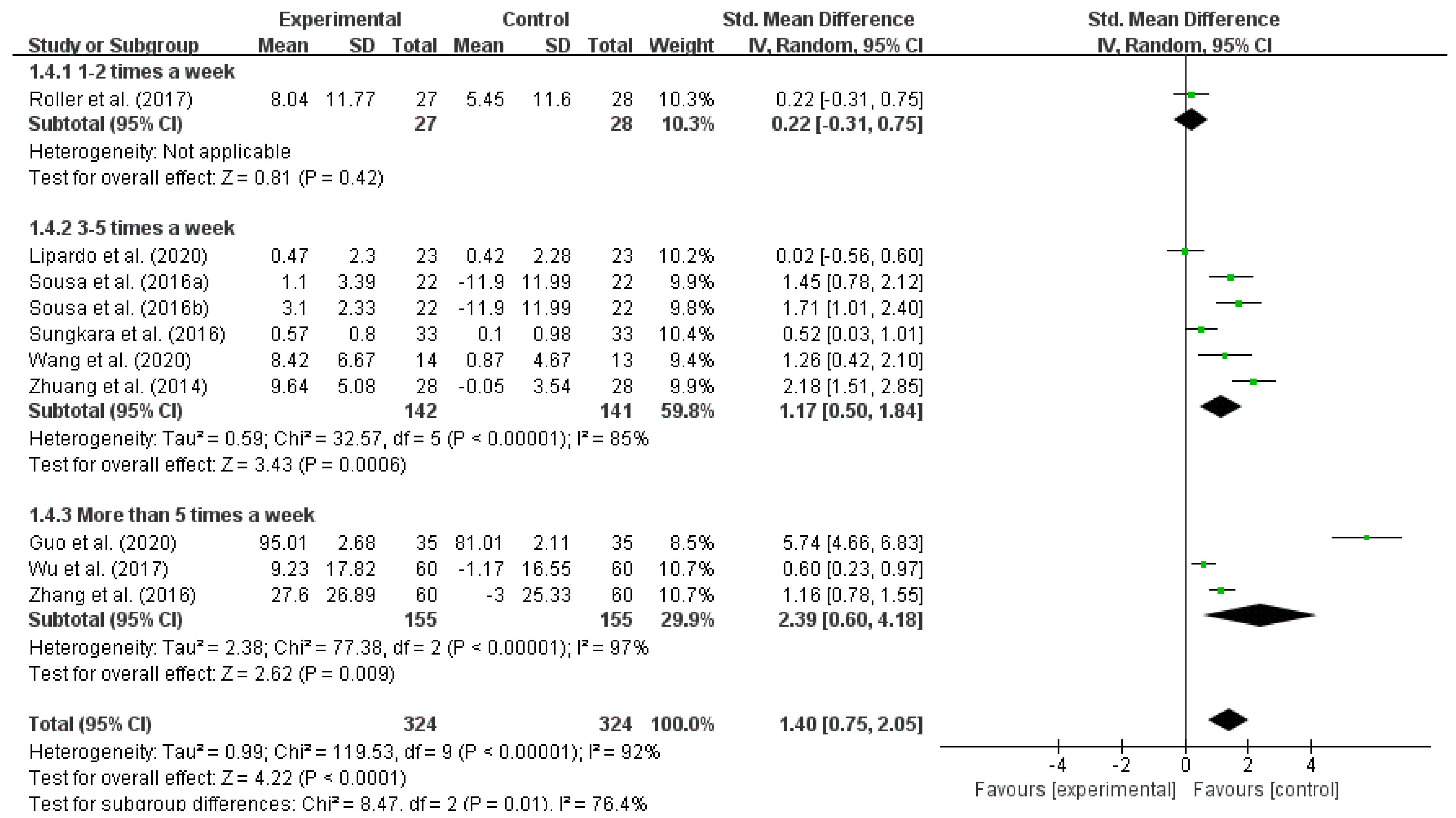
3.4.3. Effect of Different Intervention Frequencies on Reducing the Fall Risk in Older Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Park, S.-H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥65 Years—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Akers, L.; Chou, L.-S.; Pidgeon, D.; Voit, J.; Winters-Stone, K. Tai Ji Quan vs. a Multimodal Exercise Intervention for Preventing Falls in High-Risk Older Adult. JAMA Intern. Med. 2018, 178, 1301–1310. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-Y.; Huang, C.-S. Aging in Taiwan: Building a Society for Active Aging and Aging in Place. Gerontologist 2015, 56, 176–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolding, D.J.; Corman, E. Falls in the Geriatric Patient. Clin. Geriatr. Med. 2019, 35, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, G.A.R.; Haastregt, J.C.M.V.; Eijk, J.T.M.V.; Rossum, E.V.; Stalenhoef, P.A.; Kempen, G.I.J.M. Prevalence and correlates of fear of falling, and associated avoidance of activity in the general population of community-living older people. Age Ageing 2007, 36, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Hoof, J.V.; Kazak, J.K.; Perek-Białas, J.M.; Peek, S.T.M. The Challenges of Urban Ageing: Making Cities Age-Friendly in Europe. Int. J. Environ. Res. Public Health 2018, 15, 2473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoof, J.V.; Marston, H.R. Age-Friendly Cities and Communities: State of the Art and Future Perspectives. Int. J. Environ. Res. Public Health 2021, 18, 1644. [Google Scholar] [CrossRef]
- Elsawahli, H.; Ali, A.S.; Ahmad, F.; Al-Obaidi, K.M. Evaluating Potential Environmental Variables and Active Aging in Older Adults for Age-Friendly Neighborhoods in Malaysia. J. Hous. Elder. 2017, 31, 74–92. [Google Scholar] [CrossRef]
- Clarkea, P.; Nieuwenhuijsen, E.R. Environments for healthy ageing: A critical review. Maturitas 2009, 64, 14–19. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Global Report on Falls Prevention in Older Age. Available online: http://www.who.int/mediacentre/factsheets/fs344/en/ (accessed on 24 September 2021).
- Karlsson, M.K.; Vonschewelov, T.; Karlsson, C.; Cöster, M.; Rosengen, B.E. Prevention of falls in the elderly: A review. Scand J. Public Health 2013, 41, 442–454. [Google Scholar] [CrossRef] [PubMed]
- Reinoso, H.; McCaffrey, R.G.; Taylor, D.W.M. Mitigating fall risk: A community fall reduction program. Geriatr. Nurs. 2018, 39, 199–203. [Google Scholar] [CrossRef]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. Does a home-based strength and balance programme in people aged >80 years provide the best value for money to prevent falls? A systematic review of economic evaluations of falls prevention interventions. Br. J. Sports Med. 2010, 44, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S. Exercise for preventing falls in older people living in the community: An abridged Cochrane systematic Review. Br. J. Sports Med. 2020, 54, 885–891. [Google Scholar] [CrossRef]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C.T. Effective Exercise for the Prevention of Falls: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Noopud, P.; Suputtitada, A.; Khongprasert, S.; Kanungsukkasem, V. Effects of Thai traditional dance on balance performance in daily life among older women. Aging Clin. Exp. Res. 2019, 31, 961–967. [Google Scholar] [CrossRef]
- Jung, D.-I.; Ko, D.-S.; Jeong, M.-A. Kinematic effect of Nintendo WiiTM sports program exercise on obstacle gait in elderly women with falling risk. J. Phys. Ther. Sci. 2015, 27, 1397–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, M.Y.; Jeong, H.; Petrofsky, J.; Lee, H.; Yim, J. Effects of a randomized controlled recurrent fall prevention program on risk factors for falls in frail elderly living at home in rural communities. Med. Sci. Monit. 2014, 20, 2283–2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, T.; Kondo, K.; Suzuki, K.; Yamada, M.; Matsumoto, D. Factors Associated with Falls in Community-Dwelling Older People with Focus on Participation in Sport Organizations: The Japan Gerontological Evaluation Study Project. Biomed. Res. Int. 2014, 537614. [Google Scholar] [CrossRef]
- Sibley, K.M.; Thomas, S.M.; Veroniki, A.A.; Rodrigues, M.; Hamid, J.S.; Lachance, C.C.; Cogo, E.; Khan, P.A.; Riva, J.J.; Thavorn, K.; et al. Comparative effectiveness of exercise interventions for preventing falls in older adults: A secondary analysis of a systematic review with network meta-analysis. Exp. Gerontol. 2021, 143, 111151. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Ng, C.A.C.M.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 144. [Google Scholar] [CrossRef]
- Lee, S.H.; Yu, S. Effectiveness of multifactorial interventions in preventing falls among older adults in the community: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2020, 106, 103564. [Google Scholar] [CrossRef] [PubMed]
- Gulka, H.J.; Patel, V.; Arora, T.; McArthur, C.; Iaboni, A. Efficacy and Generalizability of Falls Prevention Interventions in Nursing Homes: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 1024–1035. [Google Scholar] [CrossRef]
- Papalia, G.F.; Papalia, R.; Balzani, L.A.D.; Torre, G.; Zampogna, B.; Vasta, S.; Fossati, C.; Alifano, A.M.; Denaro, V. The Effects of Physical Exercise on Balance and Prevention of Falls in Older People: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2595. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.B.; DeShon, R.P. Combining Effect Size Estimates in Meta-Analysis With Repeated Measures and Independent-Groups Designs. Psychol. Methods 2002, 7, 105. [Google Scholar] [CrossRef]
- Guo, L. Evaluation of the Effect of Exercise Therapy combined with Drug Intervention on the Fall Risk of Patients with Osteoporosis in Senile Care Hospital. Guide China Med. 2020, 18, 256–257. [Google Scholar] [CrossRef]
- Lipardo, D.S.; Tsang, W.W. Effects of combined physical and cognitive training on fall prevention and risk reduction in older persons with mild cognitive impairment: A randomized controlled study. Clin. Rehabil. 2020, 34, 773–782. [Google Scholar] [CrossRef]
- Roller, M.; Kachingwe, A.; Beling, J.; Ickes, D.-M.; Cabot, A.; Shrier, G. Pilates Reformer exercises for fall risk reduction in older adults: A randomized controlled trial. J. Bodyw. Mov. Ther. 2018, 22, 983–998. [Google Scholar] [CrossRef]
- Sousa, N.; Mendes, R.; Silva, A.; Oliveira, J. Combined exercise is more effective than aerobic exercise in the improvement of fall risk factors: A randomized controlled trial in community-dwelling older men. Clin. Rehabil. 2017, 31, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Sungkarat, S.; Boripuntakul, S.; Chattipakorn, N.; Watcharasaksilp, K.; Lord, S.R. Effects of Tai Chi on Cognition and Fall Risk in Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Am. Geriatr. Soc. 2017, 65, 721–727. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Li, W.; Zuo, J.; Wang, C.; He, Y. Effects of Diabolo Diabolo on the Balance Ability, Lower Limb Muscle Strength and Fall Risk of Rural Elderly Women. Chin. J. Gerontol. 2020, 40, 4784–4787. [Google Scholar] [CrossRef]
- Wu, X.; Xue, W.G.; Fang, J.; Wang, J.X.; Fan, X.L.; Ma, H.X. Baduanjin of Movements on the Risk of Falls in Community Elderly People for 60 Cases. Chin. Med. Mod. Distance Educ. China 2017, 15, 106–109. [Google Scholar] [CrossRef]
- Zhang, J.; Lin, C. Balance Traning for the Elderly Fall Risk Intervention Observation. Chin. J. Coal Ind. Med. 2016, 19, 518–521. [Google Scholar] [CrossRef]
- Zhuang, J.; Huang, L.; Wu, Y.; Zhang, Y. The effectiveness of a combined exercise intervention on physical fitness factors related to falls in community-dwelling older adults. Clin. Interv. Aging 2014, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Kyrdalen, I.L.; Thingstad, P.; Sandvik, L.; Ormstad, H. Associations between gait speed and well-known fall risk factors among community-dwelling older adults. Physiother. Res. Int. 2018, 24, e1743. [Google Scholar] [CrossRef] [Green Version]
- Galloza, J.; Castillo, B.; Micheo, W. Benefits of Exercise in the Older Population. Phys. Med. Rehabil. Clin. 2017, 28, 659–669. [Google Scholar] [CrossRef]
- Segev-Jacubovski, O.; Herman, T.; Yogev-Seligmann, G.; Mirelman, A.; Giladi, N.; Hausdorff, J.M. The interplay between gait, falls and cognition: Can cognitive therapy reduce fall risk? Expert Rev. Neurother. 2011, 11, 1057–1075. [Google Scholar] [CrossRef] [Green Version]
- Kruschke, C.; Butcher, H.K. Evidence-Based Practice Guideline: Fall Prevention for Older Adults. J. Gerontol. Nurs. 2017, 43, 15–21. [Google Scholar] [CrossRef]
- Cho, E.H.; Woo, Y.J.; Han, A.; Chung, Y.C.; Kim, Y.H.; Park, H.-A. Comparison of the Predictive Validity of Three Fall Risk Assessment Tools and Analysis of Fall Risk Factors at a Tertiary Teaching Hospital. J. Clin. Nurs. 2020, 29, 3482–3493. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, N.A.; Kuwae, Y.; Tamura, T.; Minato, K.; Kanaya, S. Quantitative analysis of fall risk using TUG test. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Ohtsu, H.; Yoshida, S.; Minamisawa, T.; Katagiri, N.; Yamaguchi, T.; Takahashi, T.; Yomogida, S.-I.; Kanzaki, H. Does the balance strategy during walking in elderly persons show an association with fall risk assessment? J. Biomech. 2020, 103, 109657. [Google Scholar] [CrossRef] [PubMed]
- Rivolta, M.W.; Aktaruzzaman, M.; Rizzo, G.; Lafortuna, C.L.; Ferrarin, M.; Bovi, G.; Bonardi, D.R.; Caspani, A.; Sassi, R. Evaluation of the Tinetti score and fall risk assessment via accelerometry-based movement analysis. Artif. Intell. Med. 2019, 95, 38–47. [Google Scholar] [CrossRef]
- Thiamwong, L. A hybrid concept analysis of fall risk appraisal: Integration of older adults’ perspectives with an integrative literature review. Nurs. Forum 2020, 55, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Low, S.; Ang, L.W.; Goh, K.S.; Chew, S.K. A systematic review of the effectiveness of Tai Chi on fall reduction among the elderly. Arch. Gerontol. Geriatr. 2009, 48, 325–331. [Google Scholar] [CrossRef]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Kim, S.H. Risk factors for severe injury following indoor and outdoor falls in geriatric patients. Arch. Gerontol. Geriatr. 2015, 62, 75–82. [Google Scholar] [CrossRef]
- Khow, K.S.F.; Visvanathan, R. Falls in the Aging Population. Clin. Geriatr. Med. 2017, 33, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Close, J.C.T. New horizons in falls prevention. Age Ageing 2018, 47, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-C.; Chang, K.-C.; Tsauo, J.-Y.; Hung, J.-W.; Huang, Y.-C.; Lin, S.-I. Effects of a multifactorial fall prevention program on fall incidence and physical function in community-dwelling older adults with risk of falls. Arch. Phys. Med. Rehabil. 2013, 94, 606–615. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | Type | Definition |
|---|---|---|
| Inclusion Criteria | Study type | Randomized controlled trial (RCT) studies in Chinese and English. |
| Study subject | Middle-aged and older adults (over 50 years old) without disabilities and other diseases that make them unsuitable for exercise interventions. | |
| Intervention requirement | Physical activity at baseline levels is the same in both groups, and the duration of the intervention is greater than or equal to 4 weeks. | |
| Outcome indicators | Fall risk index, fall risk score. | |
| Exclusion Criteria | Indicators without clear comparability. | |
| Baseline level data not available. | ||
| Missing full text or incomplete data on outcome indicators. |
| Code | Publish Time | Country | intervention Programs | Exercise Intervention Type | Participant Type | Age | Gender | Test Group Size | Control Group Size | PEDro Score | Literature Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Guo et al. (2020) [29] | 2020 | China | Exercise includes weight-bearing exercise, balance training and muscle training. Weight-bearing exercises are carried out 3 times a day, 20 min each time. Balance exercise can improve balance ability, which is carried out 3 times a day, 20 min each time. | Integrated training (weight training, balance training, and muscle training) | Older adults with osteoporosis | 62–80 | Mixed | 35 | 35 | 5 | Medium |
| Lipardo et al. (2020) [30] | 2020 | Philippines | 12 consecutive weeks, 3 sessions per week, 60 to 90 min of physical training | Physical training | Older adults in the community with mild cognitive impairment | 60–83 | Mixed | 23 | 23 | 5 | Medium |
| Roller et al. (2017) [31] | 2018 | United States | Subjects in the Pilates group attended 8 × 10³sessions of a 45-min Pilates exercise program using a Reformer once a week over a 10-week period | Pilates | Older adults over 65 years old with a history of falls in the past year | 65–95 | Mixed | 27 | 28 | 7 | High |
| Sousa et al. (2016a) [32] | 2016 | Portugal | The aerobic exercise group trained twice per week in a land environment (Mondays and Wednesdays) and once per week in an aquatic environment (Fridays). All aerobic training sessions consisted of: (i) a 10-min warm-up period, which included walking and flexibility exercises; (ii)a 30-min cardiorespiratory period, including walking and/or brisk walking; (iii) a 10-min muscular endurance, which included three exercises (three sets of 15–20 repetitions) using only bodyweight and gravity for strengthening the lower and upper limbs in a land environment, and water resistance in an aquatic environment; and (iv) a 5-min cool-down period, which included breathing and stretching exercises. | Aerobic exercise | Older men in the community | 65–74 | Male | 22 | 22 | 6 | Medium |
| Sousa et al. (2016b) [32] | 2016 | Portugal | the aerobic training session on Mondays were replaced by a resistance exercise session. The intensity of the resistance training sessions was defined by the pyramidal method set to 65% of 1-RM in the first eight weeks; 75% of 1-RM for Weeks 8–24; 70% of 1-RM for Weeks 24–28; and 65% of 1-RM for Weeks 28–32 (three sets of 10–12 repetitions in all sessions). Each session always began with a 10-min warm-up and ended with a cool-down period. The main part of the sessions consisted of a circuit of seven exercises: bench press, leg press, lateral pull-down, leg extension, military press, leg curl and arm curl, in this order, and carried out with conventional variable resistance devices (PANATTA, Fitline 2000 series, Italy). The 1-RM values were taken at the first workout of Week 1, Week 8, Week 16 and Week 24, and at the last workout of Week 32, allowing periodic adjustment of the resistance training intensity for the combined exercise group. | Integrated training (weight training, balance training, and muscle training) | Older men in the community | 65–74 | Male | 22 | 22 | 6 | Medium |
| Sungkarat et al. (2016) [33] | 2017 | Thailand | Participants in the Tai Chi group attended Tai Chi classes led by a certified Tai Chi instructor for 3 weeks (9 sessions) to learn Tai Chi principles and the 10-form Tai Chi. The Tai Chi classes were held with six or seven persons per class in the exercise room at the Department of Physical Therapy. Participants then practiced Tai Chi at home three times per week for 12 weeks. | Tai chi | Older adults with mild cognitive impairment | 61–75 | Mixed | 33 | 33 | 6 | Medium |
| Wang et al. (2020) [34] | 2020 | China | Exercise 5 times a week, time is 7:00–8:30 in the morning, each exercise time is 90 min, including 15 min of warm-up activities, 60 min of formal exercises, and 15 min of relaxation. | Diabolo training | Older adults in rural area | 60–72 | Female | 14 | 13 | 5 | Medium |
| Wu et al. (2017) [35] | 2017 | China | Baduanjin exercises are performed 2 times a day, 3 times each time, and the treatment cycle is 30 days. The patient chooses appropriate actions for practice under the guidance of doctors according to their own conditions and individual differences | Ba Duan Jin | Older adults in the community | 65–80 | Mixed | 60 | 60 | 6 | Medium |
| Zhang et al. (2016) [36] | 2016 | China | Training time is 45 min, training 5 days per week, and the intervention time is 8 weeks | Balance training | Older adults in the community | 63–78 | Mixed | 60 | 60 | 6 | Medium |
| Zhuang et al. (2014) [37] | 2014 | China | The intervention group received 60 min exercise classes three times per week for 12 weeks in the community center. The intensity of the exercise was increased gradually over time to help participants achieve success. Each class started with a 5-min warm-up, followed by 15 min of balance exercises, 15 min of muscle-strength training, 15 min of 8-form Yang style Tai Chi Chuan, and ending with 10 min of flexibility/stretching and cool-down. | Integrated training (muscle training, balance raining, and Tai Chi) | Older adults in the community | 60–80 | Mixed | 28 | 28 | 6 | Medium |
| Code | Main Indicator | Outcome Indicator | Intervention Duration | Intervention Frequency | Result |
|---|---|---|---|---|---|
| Guo et al. (2020) [29] | Comparison of disease efficacy, disease awareness, fall prevention awareness, psychological anxiety level, body immunity status, bone density before and after care, and incidence of falls between the two groups of older adults with osteoporosis. | Fall prevention awareness score | 1 year | Daily | Medication and exercise interventions have a better preventive effect on older adults. |
| Lipardo et al. (2020) [30] | Assessment of fall incidence, overall fall risk, dynamic balance, walking speed, and lower-extremity strength. | PPA (Physiological Profile Assessment) test | 12 weeks | 3 times a week | No significant differences in fall rates and fall risk were found between the groups after the intervention. Physical training and cognitive training and the combination of them can improve dynamic balance. Further studies with larger sample sizes are needed to determine if the interventions are effective. |
| Roller et al. (2017) [31] | SOT score of the NeuroCom® system, Timed Up and Go (TUG), and Activity Specific Balance Confidence (ABC) Scale. | SOT score | 10 weeks | Once a week | Pilates modified exercises once a week for 10 weeks can reduce the fall risk in adults aged 65 and older who are at risk of falls. This exercise significantly improved static and dynamic balance, functional mobility, balance self-efficacy, and lower-extremity AROM. In contrast, the control group showed no significant improvement in any of the indicators. Pilates modified exercises were more effective than no exercise intervention in improving AROM in the hip and ankle joints. |
| Sousa et al. (2016a) [32] | Timed up test, functional reach (FR) test, CS-30 test, and 6-min walk test. | CS-30 test | 32 weeks | 3 times a week | The addition of resistance exercise to aerobic exercise may improve factors associated with increased fall risk. Both combined exercise and aerobic exercise are more effective than no exercise in reducing the fall risk. |
| Sousa et al. (2016b) [32] | Timed up test, FR test, CS-30 test, and 6-min walk test. | CS-30 test | 32 weeks | 3 times a week | The addition of resistance exercise to aerobic exercise may improve factors associated with increased fall risk. Both combined exercise and aerobic exercise are more effective than no exercise in reducing the fall risk. |
| Sungkarat et al. (2016) [33] | Fall risk index with physiological profile assessment (PPA). | PPA test | 12 weeks | 3 times a week | In older adults with multi-domain amnestic mild cognitive impairment, the combination of core training and Tai Chi three times a week for 15 weeks significantly improved cognitive function and modestly reduced the fall risk. In particular, Tai Chi may have quite great effects on reducing the fall risk. |
| Wang et al. (2020) [34] | Static and dynamic balance ability test (Good Balance balance tester), CS-30 test, Tetrax fall risk test. | Tetrax fall risk index | 14 weeks | 5 times a week | The 14-week diabolo exercise strengthened the lower-extremity muscles of older adults, reducing the possibility of the fall risk and improving balance. Eight weeks of physical education and health lectures motivated older adults to take action, increasing their exercise frequencies. |
| Wu et al. (2017) [35] | MFS, Berg balance scale score, “get-up-and-walk” timing test, self-rating anxiety scale, Riker SAS score, and the SF-36 health survey. | MFS | 30 days | Daily | Ba Duan Jin could effectively reduce the fall risk among older adults in the community to a certain extent. |
| Zhang et al. (2016) [36] | Fall risk score | Fall risk score | 8 weeks | Daily | Balance training could reduce the fall risk in older adults. |
| Zhuang et al. (2014) [37] | CS-30 test, TUG test, FR test, and star offset balance test (SEBT). | CS-30 test | 12 weeks | 3 times a week | This study provided an effective, evidence-based fall prevention program that can be implemented to improve the physical health of older adults in the community and reduce the fall risk. In the assessment of fall risk in older adults, the SEBT might be a sensitive measure of physical performance. |
| Model | Sample Size | Heterogeneity Test | Total Effect Size Test | SMD | 95% CI | ||
|---|---|---|---|---|---|---|---|
| I2 | p | Z | p | ||||
| Random-Effect Model | 10 | 92% | <0.00001 | 4.22 | <0.0001 | 1.4 | 0.75–2.05 |
| Type | No. of Studies | Test Group Size | Control Group Size | I2 | SMD | 95% CI | p |
|---|---|---|---|---|---|---|---|
| Integrated training | 3 | 85 | 85 | 95% | 3.16 | 1.12–5.21 | 0.002 |
| Physical training | 3 | 105 | 105 | 85% | 0.88 | 0.08–1.68 | 0.03 |
| Fitness training | 4 | 134 | 134 | 31% | 0.57 | 0.25–0.88 | 0.004 |
| Total | 10 | 324 | 324 | 92% | 1.4 | 0.75–2.05 | <0.0001 |
| Duration | No. of Studies | Test Group Size | Control Group Size | I2 | SMD | 95% CI | p |
|---|---|---|---|---|---|---|---|
| Less than 12 weeks | 3 | 147 | 148 | 77% | 0.68 | 0.17–1.20 | 0.009 |
| 12–32 weeks | 4 | 98 | 97 | 88% | 0.98 | 0.06–1.89 | 0.04 |
| More than 32 weeks | 4 | 79 | 79 | 96% | 2.92 | 0.69–5.15 | 0.01 |
| Total | 10 | 324 | 324 | 92% | 1.4 | 0.75–2.05 | <0.0001 |
| Frequency | No. of Studies | Test Group Size | Control Group Size | I2 | SMD | 95% CI | p |
|---|---|---|---|---|---|---|---|
| 1–2 times a week | 1 | 27 | 27 | - | 0.22 | −0.31–0.75 | 0.42 |
| 3–5 times a week | 6 | 142 | 141 | 85% | 1.75 | 0.50–1.84 | 0.0006 |
| More than 5 times a week | 3 | 155 | 155 | 97% | 2.39 | 0.60–4.18 | 0.009 |
| Total | 10 | 324 | 324 | 92% | 1.4 | 0.75–2.05 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, M.; Min, L.; Xu, N.; Huang, L.; Li, X. The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 12562. https://doi.org/10.3390/ijerph182312562
Sun M, Min L, Xu N, Huang L, Li X. The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health. 2021; 18(23):12562. https://doi.org/10.3390/ijerph182312562
Chicago/Turabian StyleSun, Mingyu, Leizi Min, Na Xu, Lei Huang, and Xuemei Li. 2021. "The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials" International Journal of Environmental Research and Public Health 18, no. 23: 12562. https://doi.org/10.3390/ijerph182312562
APA StyleSun, M., Min, L., Xu, N., Huang, L., & Li, X. (2021). The Effect of Exercise Intervention on Reducing the Fall Risk in Older Adults: A Meta-Analysis of Randomized Controlled Trials. International Journal of Environmental Research and Public Health, 18(23), 12562. https://doi.org/10.3390/ijerph182312562