
Development and Validation of the Depression Inventory for Type 1 Diabetes (DID-1)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
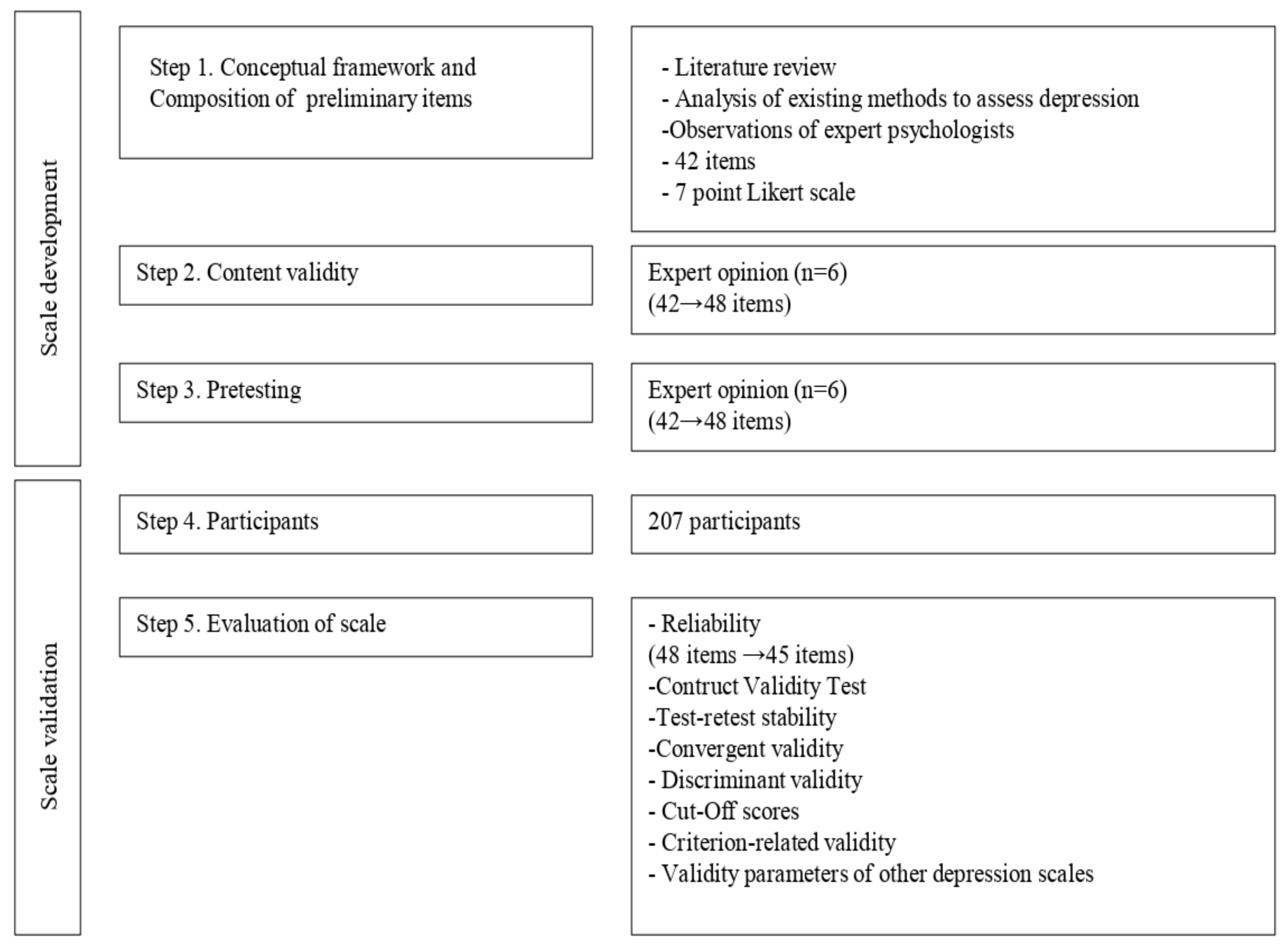
2.1. The Depression Inventory for Type 1 Diabetes (DID-1): Scale Development
2.1.1. Conceptual Framework and Composition of Preliminary Items
2.1.2. Expert Opinion
2.1.3. Pretesting
2.2. Scale Validation
2.2.1. Participants and Ethics
2.2.2. Informed Consent
2.2.3. Measures
2.2.4. Data Analyses
3. Results
3.1. Sample Characteristics
3.2. Evaluation of Scale
3.2.1. Reliability
3.2.2. Construct Validity Test
3.2.3. Test-Retest Stability
3.2.4. Convergent Validity
3.2.5. Discriminant Validity
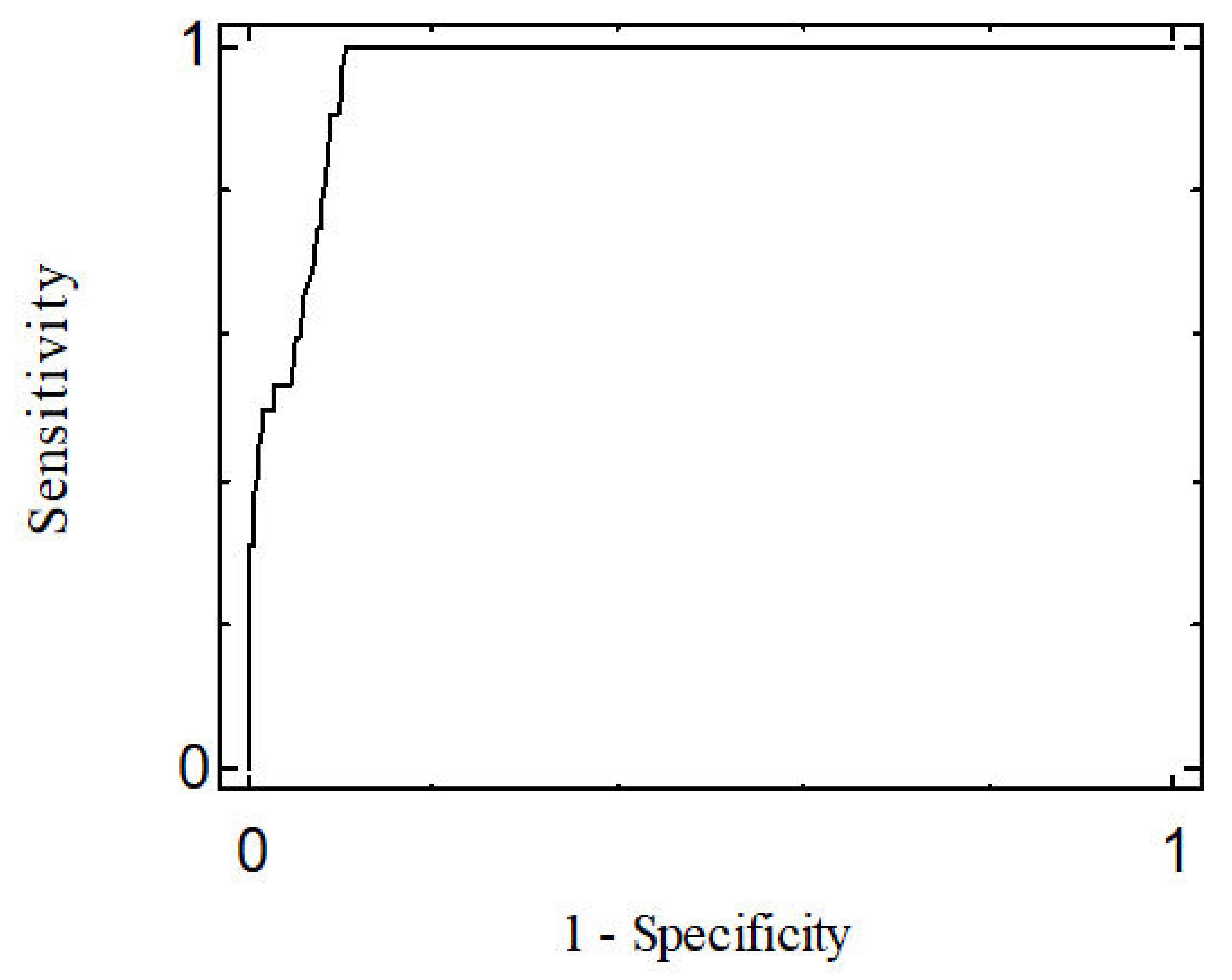
3.2.6. Cut-Off Scores
3.2.7. Criterion-Related Validity
3.2.8. Validity Parameters of Other Depression Scales
3.3. Prevalence of Depressive Symptoms
3.4. Differences in DID-1 and 7-Factor Scores as a Function of Subject Characteristics
4. Discussion
5. Conclusions
- -
- The DID-1 has excellent psychometric properties, with high internal consistency and test-retest reliability.
- -
- The DID-1 is a depression assessment instrument designed specifically for people with T1D.
- -
- The DID-1 is a good instrument for screening or initial assessment to determine the presence of depressive symptoms in patients with T1D.
- -
- The DID-1 offers advantages compared with the scales used in the general population: The scores on these scales are usually distributed according to the severity of the symptoms (mild, moderate…). With this instrument we are providing healthcare professionals with a tool to detect whether or not the patient has depressive symptoms.
- -
- The DDI-1 is also a useful tool for research in T1D, as it is specific to this population, has good psychometric properties and its use would standardize studies using the same assessment tool.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chireh, B.; Li, M.; D’Arcy, C. Diabetes increases the risk of depression: A systematic review, meta-analysis and estimates of population attributable fractions based on prospective studies. Prev. Med. Rep. 2019, 14, 100822. [Google Scholar] [CrossRef] [PubMed]
- Meurs, M.; Roest, A.M.; Wolffenbuttel, B.H.R.; Stolk, R.P.; de Jonge, P.; Rosmalen, J.G.M. Association of Depressive and Anxiety Disorders with Diagnosed Versus Undiagnosed Diabetes: An Epidemiological Study of 90,686 Participants. Psychosom. Med. 2016, 78, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deschênes, S.S.; Burns, R.J.; Pouwer, F.; Schmitz, N. Diabetes Complications and Depressive Symptoms: Prospective Results from the Montreal Diabetes Health and Well-Being Study. Psychosom. Med. 2017, 79, 603–612. [Google Scholar] [CrossRef]
- Bąk, E.; Marcisz-Dyla, E.; Młynarska, A.; Sternal, D.; Kadłubowska, M.; Marcisz, C. Prevalence of Depressive Symptoms in Patients with Type 1 and 2 Diabetes Mellitus. Patient Prefer. Adherence 2020, 14, 443–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishizawa, K.; Babazono, T.; Horiba, Y.; Nakajima, J.; Takasaki, K.; Miura, J.; Sakura, H.; Uchigata, Y. The relationship between depressive symptoms and diabetic complications in elderly patients with diabetes: Analysis using the Diabetes Study from the Center of Tokyo Women’s Medical University (DIACET). J. Diabetes Complicat. 2016, 30, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Nouwen, A.; Adriaanse, M.C.; van Dam, K.; Iversen, M.M.; Viechtbauer, W.; Peyrot, M.; Caramlau, I.; Kokoszka, A.; Kanc, K.; de Groot, M.; et al. Longitudinal associations between depression and diabetes complications: A systematic review and meta-analysis. Diabet. Med. 2019, 36, 1562–1572. [Google Scholar] [CrossRef]
- Holt, R.I.G.; de Groot, M.; Golden, S.H. Diabetes and Depression. Curr. Diab. Rep. 2014, 14, 491. [Google Scholar] [CrossRef] [Green Version]
- Browne, J.L.; Ventura, A.; Mosely, K.; Speight, J. ‘I call it the blame and shame disease’: A qualitative study about perceptions of social stigma surrounding type 2 diabetes. BMJ Open 2013, 3, e003384. [Google Scholar] [CrossRef] [Green Version]
- Browne, J.L.; Ventura, A.; Mosely, K.; Speight, J. ‘I’m not a druggie, I’m just a diabetic’: A qualitative study of stigma from the perspective of adults with type 1 diabetes. BMJ Open 2014, 4, e005625. [Google Scholar] [CrossRef] [Green Version]
- Delamater, A.M.; Jacobson, A.M.; Anderson, B.; Cox, D.; Fisher, L.; Lustman, P.; Rubin, R.; Wysocki, T. Psychosocial therapies in diabetes. Report of the psychosocial therapies working group. Diabetes Care 2001, 24, 1286–1292. [Google Scholar] [CrossRef] [Green Version]
- Roy, T.; Lloyd, C.E. Epidemiology of depression and diabetes: A systematic review. J. Affect. Disord. 2012, 142, S8–S21. [Google Scholar] [CrossRef]
- Castellano-Guerrero, A.M.; Guerrero, R.; Relimpio, F.; Losada, F.; Mangas, M.A.; Pumar, A.; Martínez-Brocca, M.A. Prevalence and predictors of depression and anxiety in adult patients with type 1 diabetes in tertiary care setting. Acta Diabetol. 2018, 55, 943–953. [Google Scholar] [CrossRef]
- Carreira, M.; Anarte, M.T.; de Adana, M.S.R.; Caballero, F.F.; Machado, A.; Domínguez-López, M.; Molero, I.G.; de Antonio, I.E.; Valdés, S.; González-Romero, S.; et al. Depresión en la diabetes mellitus tipo 1 y factores asociados. Med. Clin. 2010, 135, 151–155. [Google Scholar] [CrossRef]
- Aschner, P.; Gagliardino, J.J.; Ilkova, H.; Lavalle, F.; Ramachandran, A.; Mbanya, J.C.; Shestakova, M.; Bourhis, Y.; Chantelot, J.M.; Chan, J.C. High Prevalence of Depressive Symptoms in Patients With Type 1 and Type 2 Diabetes in Developing Countries: Results From the International Diabetes Management Practices Study. Diabetes Care 2021, 44, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 10 November 2021).
- Anarte, M.T.; Carreira, M.; Ruiz de Adana, M.S.; Caballero, F.F.; Godoy, A.; Soriguer, F.C. Precisión del diagnóstico de depresión en pacientes con diabetes mellitus tipo 1 [Accuracy of diagnosis of depression in patients with Type 1 diabetes mellitus]. Psicothema 2011, 23, 606–610. [Google Scholar]
- Poulsen, K.M.; Pachana, N.A.; McDermott, B.M. Health professionals’ detection of depression and anxiety in their patients with diabetes: The influence of patient, illness and psychological factors. J. Health Psychol. 2016, 21, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Davis, W.A.; Bruce, D.G.; Dragovic, M.; Davis, T.M.; Starkstein, S.E. The utility of the Diabetes Anxiety Depression Scale in Type 2 diabetes mellitus: The Fremantle Diabetes Study Phase II. PLoS ONE 2018, 13, e0194417. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Mohr, D.; Masharani, U.; Glasgow, R.; Laurencin, G. Clinical Depression Versus Distress Among Patients with Type 2 Diabetes: Not just a question of semantics. Diabetes Care 2007, 30, 542–548. [Google Scholar] [CrossRef] [Green Version]
- González, D.A.; Jenkins, S.R. Cross-Measure Equivalence and Communicability in the Assessment of Depression: A Focus on Factor-Based Scales. Assessment 2014, 21, 731–741. [Google Scholar] [CrossRef]
- Anderson, R.J.; Freedland, K.E.; Clouse, R.E.; Lustman, P.J. The Prevalence of Comorbid Depression in Adults with Diabetes: A meta-analysis. Diabetes Care 2001, 24, 1069–1078. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-T.; Lin, L.-Y.; Tuan, C.-W.; Yang, C.-Y.; Tang, P.-L. Analyzing the Association HbA1c control by Depression, social participation and Utilizing Self-management Questionnaire. Diabetes Res. Clin. Pract. 2019, 153, 103–110. [Google Scholar] [CrossRef]
- Rauwerda, N.L.; Tovote, K.A.; Peeters, A.C.; Sanderman, R.; Emmelkamp, P.M.; Schroevers, M.J.; Fleer, J. WHO-5 and BDI-II are acceptable screening instruments for depression in people with diabetes. Diabet. Med. 2018, 35, 1678–1685. [Google Scholar] [CrossRef]
- Roy, T.; Lloyd, C.E.; Pouwer, F.; Holt, R.I.G.; Sartorius, N. Screening tools used for measuring depression among people with Type 1 and Type 2 diabetes: A systematic review: Screening tools used for measuring depression in diabetes. Diabet. Med. 2012, 29, 164–175. [Google Scholar] [CrossRef]
- van Dijk, S.E.; Adriaanse, M.C.; van der Zwaan, L.; Bosmans, J.E.; van Marwijk, H.W.; van Tulder, M.W.; Terwee, C.B. Measurement properties of depression questionnaires in patients with diabetes: A systematic review. Qual. Life Res. 2018, 27, 1415–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, L.; Hessler, D.M.; Polonsky, W.H.; Masharani, U.; Peters, A.L.; Blumer, I.; Strycker, L.A. Prevalence of depression in Type 1 diabetes and the problem of over-diagnosis. Diabet. Med. 2016, 33, 1590–1597. [Google Scholar] [CrossRef] [PubMed]
- De Joode, J.W.; Van Dijk, S.E.; Walburg, F.S.; Bosmans, J.E.; Van Marwijk, H.W.; de Boer, M.R.; Van Tulder, M.W.; Adriaanse, M.C. Diagnostic accuracy of depression questionnaires in adult patients with diabetes: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0218512. [Google Scholar] [CrossRef] [Green Version]
- Dantzer, C.; Swendsen, J.; Maurice-Tison, S.; Salamon, R. Anxiety and depression in juvenile diabetes: A critical review. Clin. Psychol. Rev. 2003, 23, 787–800. [Google Scholar] [CrossRef]
- Petrak, F.; Röhrig, B.; Ismail, K. Depression and Diabetes. 2000. Available online: http://www.ncbi.nlm.nih.gov/books/NBK498652/ (accessed on 7 September 2021).
- Pouwer, F.; Schram, M.T.; Iversen, M.M.; Nouwen, A.; Holt, R.I.G. How 25 years of psychosocial research has contributed to a better understanding of the links between depression and diabetes. Diabet. Med. 2020, 37, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Tanenbaum, M.L.; Gonzalez, J.S. The Influence of Diabetes on a Clinician-Rated Assessment of Depression in Adults with Type 1 Diabetes. Diabetes Educ. 2012, 38, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Van Der Donk, L.J.; Fleer, J.; Sanderman, R.; Emmelkamp, P.M.; Links, T.P.; Tovote, K.A.; Schroevers, M.J. Is type of depressive symptoms associated with patient-perceived need for professional psychological care in depressed individuals with diabetes? PLoS ONE 2019, 14, e0212304. [Google Scholar] [CrossRef] [Green Version]
- Ciechanowski, P.S.; Katon, W.J.; Russo, J.E.; Hirsch, I.B. The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes. Gen. Hosp. Psychiatry 2003, 25, 246–252. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Fisher, L.; Polonsky, W.H. Depression in Diabetes: Have We Been Missing Something Important? Diabetes Care 2011, 34, 236–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snoek, F.J.; Bremmer, M.A.; Hermanns, N. Constructs of depression and distress in diabetes: Time for an appraisal. Lancet Diabetes Endocrinol. 2015, 3, 450–460. [Google Scholar] [CrossRef]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Entrevista Clínica Estructurada Para Los Trastornos Del Eje I Del DSM-IV (SCID-I) [Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I)]; Masson: Barcelona, Spain, 1999. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Zung, W.W. A SELF-RATING DEPRESSION SCALE. Arch. Gen. Psychiatry 1965, 12, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Downloading IBM SPSS Modeler 16.0.2014. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-modeler-160 (accessed on 6 September 2021).
- Thomas, J.; Jones, G.; Scarinci, I.; Brantley, P. A descriptive and comparative study of the prevalence of depressive and anxiety disorders in low-income adults with type 2 diabetes and other chronic illnesses. Diabetes Care 2003, 26, 2311–2317. [Google Scholar] [CrossRef] [Green Version]
- Fisher, L.; Gonzalez, J.S.; Polonsky, W.H. The confusing tale of depression and distress in patients with diabetes: A call for greater clarity and precision. Diabet. Med. 2014, 31, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Hermanns, N.; Caputo, S.; Dzida, G.; Khunti, K.; Meneghini, L.F.; Snoek, F. Screening, evaluation and management of depression in people with diabetes in primary care. Prim. Care Diabetes 2013, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.C.; Cavanaugh, S.V.; Gibbons, R.D. The Core Symptoms of Depression in Medical and Psychiatric Patients. J. Nerv. Ment. Dis. 1983, 171, 705–713. [Google Scholar] [CrossRef]
- Beck Depression Inventory®—FastScreen (BDI®-FastScreen). Pearson Assessment. Available online: https://www.pearsonclinical.co.uk/Psychology/AdultMentalHealth/AdultMentalHealth/BeckDepressionInventory-FastScreen(BDI-FastScreen)/BeckDepressionInventory-FastScreen(BDI-FastScreen).aspx (accessed on 10 November 2021).
- Egbuonu, I.; Trief, P.M.; Roe, C.; Weinstock, R.S. Glycemic outcomes related to depression in adults with type 1 diabetes. J Health Psychol. 2021, 26, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Sartorius, N. Depression and diabetes. Dialogues Clin. Neurosci. 2018, 20, 47–52. [Google Scholar]
- Schmitt, A.; McSharry, J.; Speight, J.; Holmes-Truscott, E.; Hendrieckx, C.; Skinner, T.; Pouwer, F.; Byrne, M. Symptoms of depression and anxiety in adults with type 1 diabetes: Associations with self-care behaviour, glycaemia and incident complications over four years–Results from diabetes MILES–Australia. J. Affect. Disord. 2021, 282, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Alvarado-Martel, D.; Ruiz Fernández, M.; Cuadrado Vigaray, M.; Carrillo, A.; Boronat, M.; Expósito Montesdeoca, A.; Wägner, A.M. Identification of Psychological Factors Associated with Adherence to Self-Care Behaviors amongst Patients with Type 1 Diabetes. J. Diabetes Res. 2019, 2019, 6271591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Tilburg, M.A.; McCaskill, C.C.; Lane, J.D.; Edwards, C.L.; Bethel, A.; Feinglos, M.N.; Surwit, R.S. Depressed Mood Is a Factor in Glycemic Control in Type 1 Diabetes. Psychosom. Med. 2001, 63, 551–555. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E.; Abramson, L.Y.; Semmel, A.; Von Baeyer, C. Depressive attributional style. J. Abnorm. Psychol. 1979, 88, 242–247. [Google Scholar] [CrossRef]
- Beran, M.; Muzambi, R.; Geraets, A.; Albertorio-Diaz, J.R.; Adriaanse, M.C.; Iversen, M.M.; Kokoszka, A.; Nefs, G.; Nouwen, A.; Pouwer, F.; et al. The Bidirectional Longitudinal Association between Depressive Symptoms and HbA1c: A Systematic Review and Meta-Analysis. 2021. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1111/dme.14671 (accessed on 10 November 2021).
- Holt, R.I.G.; van der Feltz-Cornelis, C.M. Key concepts in screening for depression in people with diabetes. J. Affect. Disord. 2012, 142, S72–S79. [Google Scholar] [CrossRef]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes. Diabetes Care 2021, 44 (Suppl. 1), S53–S72. [Google Scholar] [CrossRef]
- Anarte, M.T.; Carreira, M. Traducción al Español del Cuestionario de Áreas Problemáticas en Diabetes (Problem Areas in Diabetes-PAID); Universidad de Málaga: Málaga, Spain, 2019; Unpublished work. [Google Scholar]


{kind=link}
{kind=link}
| Depression (SCID-I) (N = 207) | Depression (DID-1) (N = 207) | |||
|---|---|---|---|---|
| Variable | Yes (n = 32) | No (n = 175) | Yes (n = 45) | No (n = 162) |
| Sex | ||||
| Men | 6 (18.8) | 93 (53.1) | 12 (26.7) | 87 (53.7) |
| Women | 26 (81.3) | 82 (46.9) | 33 (73.3) | 75 (46.3) |
| Physical illness | ||||
| Yes | 20 (62.5) | 56 (32) | 26 (57.8) | 50 (30.9) |
| No | 12 (37.5) | 119 (68) | 19 (42.2) | 112 (69.1) |
| Age of the participants * | 40.41 ± 10.84 (18–57) | 32.60 ± 10.74 (15–65) | 36.24 ± 11.68 (16–57) | 33.12 ± 10.86 (15–65) |
| Diabetes duration * | 16.82 ± 9.85 (0.07–35) | 15.08 ± 9.65 (0.04–50) | 15.57 ± 9.77 (0.07–36) | 15.28 ± 9.64 (0.04–50) |
| HbA1c (%) * | 7.8 ± 1.8 (5.70–14) | 7.6 ± 1.3 (5.10–14) | 7.76 ± 1.67 (5.10–14) | 7.57 ± 1.32 (5.20–14) |
| HbA1c (mmol/mol) * | 62 ± −3.82 (39–130) | 60 ± −9.3 (32–130) | 61 ± −5.24 (32–130) | 59 ± −9.07 (33–130) |
| Items | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | Factor 7 |
|---|---|---|---|---|---|---|---|
| FACTOR 1: Symptoms of depression | |||||||
| 2. People around me have noticed sudden changes in my mood | 0.877 | −0.114 | −0.292 | 0.124 | −0.007 | 0.072 | 0.101 |
| 3. I often have feelings of emptiness or sadness | 0.870 | −0.063 | 0.051 | −0.039 | 0.113 | −0.065 | −0.050 |
| 1. My general mood isn’t good | 0.869 | −0.095 | 0.020 | −0.051 | 0.048 | −0.085 | 0.075 |
| 4. I frequently feel like crying | 0.765 | −0.036 | 0.107 | 0.055 | 0.016 | −0.089 | 0.031 |
| 25. I feel unhappy | 0.722 | 0.085 | 0.061 | 0.172 | −0.109 | −0.060 | 0.104 |
| 24. I don’t feel as happy as before | 0.709 | −0.081 | 0.131 | −0.082 | 0.005 | 0.112 | 0.069 |
| 5. I frequently feel like screaming, hitting or breaking something | 0.708 | −0.005 | −0.224 | 0.124 | −0.001 | 0.025 | 0.170 |
| 13. I don’t take care of my appearance | 0.685 | 0.005 | −0.125 | −0.140 | 0.152 | 0.153 | −0.116 |
| 26. My current situation drives me to despair | 0.662 | 0.025 | 0.225 | 0.123 | −0.007 | −0.146 | 0.012 |
| 20. I obsess over things | 0.661 | 0.038 | −0.054 | −0.199 | 0.318 | −0.057 | −0.142 |
| 7. I often feel like being alone | 0.660 | 0.247 | 0.138 | −0.171 | −0.228 | −0.149 | 0.035 |
| 29. Time seems to pass more slowly | 0.660 | −0.072 | −0.199 | 0.111 | −0.207 | 0.303 | 0.185 |
| 27. It terrorizes me to think about my future | 0.653 | −0.057 | −0.131 | 0.063 | 0.352 | 0.076 | −0.050 |
| 22. It is hard for me to fall asleep when I go to bed | 0.621 | −0.001 | 0.021 | 0.064 | −0.057 | −0.230 | 0.357 |
| 18. I often feel useless | 0.610 | 0.040 | 0.390 | 0.112 | −0.153 | −0.032 | −0.119 |
| 21. I am restless and it is difficult for me to stay still | 0.573 | 0.039 | −0.149 | 0.044 | 0.164 | −0.099 | 0.284 |
| 6. I am more tired than usual | 0.568 | −0.023 | 0.060 | −0.108 | 0.145 | −0.249 | 0.341 |
| 28. It is difficult for me to do the things I used to do | 0.542 | 0.053 | 0.136 | −0.067 | 0.032 | 0.017 | 0.276 |
| 8. I think my life is going to be a failure | 0.507 | −0.004 | 0.400 | 0.054 | −0.074 | 0.139 | −0.029 |
| 11. I feel inferior to everyone else | 0.465 | 0.001 | 0.339 | −0.001 | 0.161 | 0.026 | −0.205 |
| 12. Things don’t satisfy me as much as they used to | 0.459 | 0.089 | 0.305 | −0.135 | 0.043 | 0.223 | 0.148 |
| 19. I feel like the people who loved me have abandoned me | 0.458 | −0.042 | 0.174 | 0.382 | −0.165 | 0.180 | −0.163 |
| 10. I don’t trust people | 0.416 | 0.177 | 0.150 | −0.220 | −0.179 | 0.189 | 0.100 |
| FACTOR 2: Diminished interest | |||||||
| 31. I don’t want to take my glucose test results to my doctor | −0.129 | 0.804 | 0.031 | 0.088 | −0.010 | −0.093 | 0.194 |
| 40. I don’t feel like going to my medical checkups | −0.024 | 0.779 | −0.061 | 0.090 | −0.060 | 0.163 | 0.142 |
| 45. I am not interested in learning anything else about diabetes | −0.136 | 0.683 | −0.193 | 0.080 | −0.042 | 0.335 | 0.048 |
| 42. I’ve stopped taking care of my diabetes | 0.157 | 0.651 | −0.275 | 0.177 | 0.155 | 0.085 | −0.294 |
| 16. I don’t take care of my health like before | 0.398 | 0.595 | −0.007 | −0.024 | 0.022 | −0.103 | −0.221 |
| FACTOR 3: Hopelessness and dissatisfaction | |||||||
| 17. I’ve thought about taking my life | −0.094 | −0.130 | 0.834 | 0.141 | 0.017 | −0.165 | 0.037 |
| 15. I think my life serves no purpose anymore | 0.180 | −0.182 | 0.662 | 0.134 | 0.032 | 0.111 | 0.102 |
| 32. I feel like I can’t cope with my diabetes | −0.093 | 0.415 | 0.467 | 0.069 | 0.271 | −0.080 | 0.088 |
| 14. Sexual relations don’t satisfy me | 0.303 | −0.031 | 0.316 | −0.254 | 0.078 | 0.166 | 0.179 |
| FACTOR 4: Guilt | |||||||
| 38. I think my diabetes is a punishment | 0.009 | 0.083 | 0.087 | 0.712 | −0.018 | 0.113 | −0.035 |
| 36. I am ashamed of my diabetes | −0.167 | 0.255 | 0.025 | 0.664 | −0.080 | 0.130 | 0.183 |
| 33. I feel guilty about my diabetes | −0.107 | 0.207 | 0.196 | 0.613 | 0.126 | −0.236 | 0.089 |
| 23. I feel like everyone would be better off if I died | 0.104 | −0.111 | 0.487 | 0.532 | −0.106 | −0.024 | −0.127 |
| 34. I feel like I can’t take care of myself and that I need help from others | 0.207 | −0.048 | −0.101 | 0.385 | 0.326 | −0.145 | 0.247 |
| FACTOR 5: Fear, frustration and irritability | |||||||
| 41. I dread thinking about the possible complications that diabetes might cause me | 0.052 | 0.032 | −0.076 | −0.025 | 0.787 | 0.078 | 0.014 |
| 30. I feel angry about my diabetes | 0.038 | −0.014 | 0.323 | −0.030 | 0.565 | 0.111 | 0.132 |
| 44. I feel like I can’t live a normal life like everyone else | 0.070 | 0.009 | 0.120 | 0.039 | 0.550 | 0.328 | 0.044 |
| FACTOR 6: Defenselessness | |||||||
| 43. I don’t believe any treatment can improve my diabetes | −0.128 | 0.104 | −0.052 | 0.042 | 0.149 | 0.815 | −0.076 |
| 37. I feel like I can’t do anything to improve my diabetes | 0.122 | 0.288 | −0.069 | 0.005 | 0.151 | 0.486 | 0.118 |
| FACTOR 7: Interference in daily life | |||||||
| 9. My sleep schedule has changed (I sleep more hours or less hours than before) | 0.575 | 0.136 | −0.129 | −0.052 | −0.131 | −0.105 | 0.577 |
| 35. It is hard for me to concentrate because of my diabetes | −0.042 | 0.071 | 0.204 | 0.147 | 0.178 | 0.113 | 0.515 |
| 39. I worry about my diabetes so much that I can’t think about anything else | 0.106 | −0.224 | 0.077 | 0.321 | 0.189 | 0.150 | 0.371 |
| Factor | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1 | 1.000 | 0.338 | 0.568 | 0.299 | 0.421 | 0.309 | 0.268 |
| 2 | 1.000 | 0.308 | 0.125 | 0.370 | 0.238 | 0.115 | |
| 3 | 1.000 | 0.182 | 0.295 | 0.258 | 0.187 | ||
| 4 | 1.000 | 0.300 | 0.166 | 0.143 | |||
| 5 | 1.000 | 0.113 | 0.242 | ||||
| 6 | 1.000 | 0.163 | |||||
| 7 | 1.000 |
| N = 207 | DID-1 Scale | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Factor 6 | Factor 7 | |
|---|---|---|---|---|---|---|---|---|---|
| Variable | N (%) | M ± SD t/p | M ± SD t/p | M ± SD t/p | M ± SD t/p | M ± SD t/p | M ± SD t/p | M ± SD t/p | M ± SD t/p |
| Sex | |||||||||
| Men | 108 (47.8) | 97.79 ± 44.51 | 59.53 ± 31.08 | 11.37 ± 6.93 | 2.50 ± 1.51 | 9.44 ± 5.74 | 8.72 ± 4.51 | 4.27 ± 2.96 | 1.93 ± 1.55 |
| Women | 99 (52.2) | 122.22 ± 51.01 −3.679/≥ 0.001 | 77.87 ± 36.62 −3.866/≥ 0.001 | 12.58 ± 6.67 −1.279/0.202 | 3.29 ± 2.46 −2.813/0.005 | 10.80 ± 5.73 −1.704/0.090 | 10.92 ± 5.34 −3.193/0.002 | 4.34 ± 2.79 −0.175/0.861 | 2.41 ± 1.82 −2.039/0.043 |
| Physical illness | |||||||||
| Yes | 76 (36.7) | 125.30 ± 54.52 | 80.14 ± 38.86 | 12.46 ± 6.26 | 3.76 ± 2.99 | 10.85 ± 6.48 | 10.92 ± 5.47 | 4.66 ± 3.03 | 2.50 ± 1.87 |
| No | 131 (63.3) | 101.97 ± 44.22 3.174/0.002 | 62.70 ± 31.33 3.336/0.001 | 11.74 ± 7.12 0.733/0.465 | 2.42 ± 1.06 3.757/≥0.001 | 9.75 ± 5.29 1.334/0.184 | 9.26 ± 4.74 2.209/0.029 | 4.10 ± 2.75 1.337/0.183 | 1.99 ± 1.58 1.986/0.049 |
| Age of the participants | |||||||||
| <30 years old ≥30 years old | 78 (37.7) 129 (62.3) | 108.55 ± 46.68 111.73 ± 51.16 −0.448/0.654 | 65.65 ± 31.19 71.18 ± 37.41 −1.146/0.253 | 12.86 ± 8.07 11.49 ± 5.89 1.304/0.195 | 2.48 ± 1.18 3.18 ± 2.45 −2.717/0.007 | 10.70±5.95 9.82 ± 5.65 1.068/0.287 | 10.24 ± 5.23 9.64 ± 4.97 0.824/0.411 | 4.51 ± 3.14 4.18 ± 2.69 0.795/0.428 | 2.09 ± 1.77 2.23 ± 1.67 −0.581/0.562 |
| Diabetes duration | |||||||||
| <15 years with diabetes ≥15 years with diabetes | 101 (48.8) 106 (51.2) | 111.81 ± 48.28 109.32 ± 50.70 0.362/0.718 | 69.93 ± 34.90 68.31 ± 35.67 0.330/0.742 | 12.17 ± 7.04 11.85 ± 6.61 0.336/0.737 | 2.86 ± 1.91 2.97 ± 2.26 −0.378/0.706 | 10.39 ± 5.81 9.92 ± 5.74 0.587/0.558 | 9.93 ± 5.16 9.81 ± 5.00 0.169/0.866 | 4.36 ± 2.98 4.25 ± 2.76 0.280/0.780 | 2.16 ± 1.65 2.19 ± 1.77 −0.167/0.868 |
| HbA1c (%) | |||||||||
| <7.0% ≥7.0% | 71 (34.6) 134 (65.4) | 104.29 ± 47.96 113.26 ± 49.70 −1.244/0.215 | 65.56 ± 34.05 70.57 ± 35.54 −0.974/0.331 | 9.80 ± 4.05 13.23 ± 7.66 −4.189/≥0.001 | 2.80 ± 1.95 2.99 ± 2.18 −0.614/0.540 | 10.09 ± 5.70 10.06 ± 5.60 0.038/0.970 | 9.66 ± 4.80 9.88 ± 5.19 −0.294/0.769 | 4.01 ± 2.78 4.45 ± 2.90 −1.050/0.295 | 2.35 ± 1.68 2.06 ± 1.68 1.185/0.237 |
| Depression (SCID-I) | |||||||||
| Yes | 32 (15.5) | 188.47 ± 33.60 | 126.78 ± 17.84 | 16.50 ± 8.17 | 5.87 ± 3.56 | 14.78 ± 8.79 | 14.75 ± 5.41 | 6.09 ± 3.56 | 3.68 ± 2.20 |
| No | 175 (84.5) | 96.29 ± 37.02 13.126/≥ 0.001 | 58.55 ± 26.23 18.309/≥ 0.001 | 11.18 ± 6.21 3.499/0.001 | 2.37 ± 1.01 5.513/≥ 0.001 | 9.31 ± 4.57 3.436/0.002 | 8.97 ± 4.47 6.483/≥ 0.001 | 3.98 ± 2.60 3.202/0.003 | 1.90 ± 1.44 4.406/≥ 0.001 |
| DID-1 | BDI-II | SDS | |
|---|---|---|---|
| Sensitivity (Se) | 0.906 | 0.969 | 0.719 |
| Specificity (Sp) | 0.909 | 0.843 | 0.937 |
| False Positives (FP) | 9.14% | 15.70% | 6.29% |
| False Negatives (FN) | 9.38% | 3.12% | 28.13% |
| Youden’s Index | 0.815 | 0.812 | 0.622 |
| Prevalence | 21.74% | 28.43% | 16.43% |
| PPV a | 0.644 | 0.534 | 0.676 |
| NPV b | 0.981 | 0.993 | 0.948 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carreira, M.; Ruiz de Adana, M.S.; Domínguez, M.; Valdés, S.; Almaraz, M.C.; Olveira, G.; Anarte, M.T. Development and Validation of the Depression Inventory for Type 1 Diabetes (DID-1). Int. J. Environ. Res. Public Health 2021, 18, 12529. https://doi.org/10.3390/ijerph182312529
Carreira M, Ruiz de Adana MS, Domínguez M, Valdés S, Almaraz MC, Olveira G, Anarte MT. Development and Validation of the Depression Inventory for Type 1 Diabetes (DID-1). International Journal of Environmental Research and Public Health. 2021; 18(23):12529. https://doi.org/10.3390/ijerph182312529
Chicago/Turabian StyleCarreira, Mónica, María Soledad Ruiz de Adana, Marta Domínguez, Sergio Valdés, Maria Cruz Almaraz, Gabriel Olveira, and María Teresa Anarte. 2021. "Development and Validation of the Depression Inventory for Type 1 Diabetes (DID-1)" International Journal of Environmental Research and Public Health 18, no. 23: 12529. https://doi.org/10.3390/ijerph182312529
APA StyleCarreira, M., Ruiz de Adana, M. S., Domínguez, M., Valdés, S., Almaraz, M. C., Olveira, G., & Anarte, M. T. (2021). Development and Validation of the Depression Inventory for Type 1 Diabetes (DID-1). International Journal of Environmental Research and Public Health, 18(23), 12529. https://doi.org/10.3390/ijerph182312529