
Acute Effects of Air Pollution on Ischemic Heart Disease Hospitalizations: A Population-Based Time-Series Study in Wuhan, China, 2017–2018

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Hospitalization Data
2.3. Air Pollution and Meteorological Data
2.4. Statistical Analysis
3. Results
3.1. Descriptive Analysis
3.2. Statistical Model Analysis
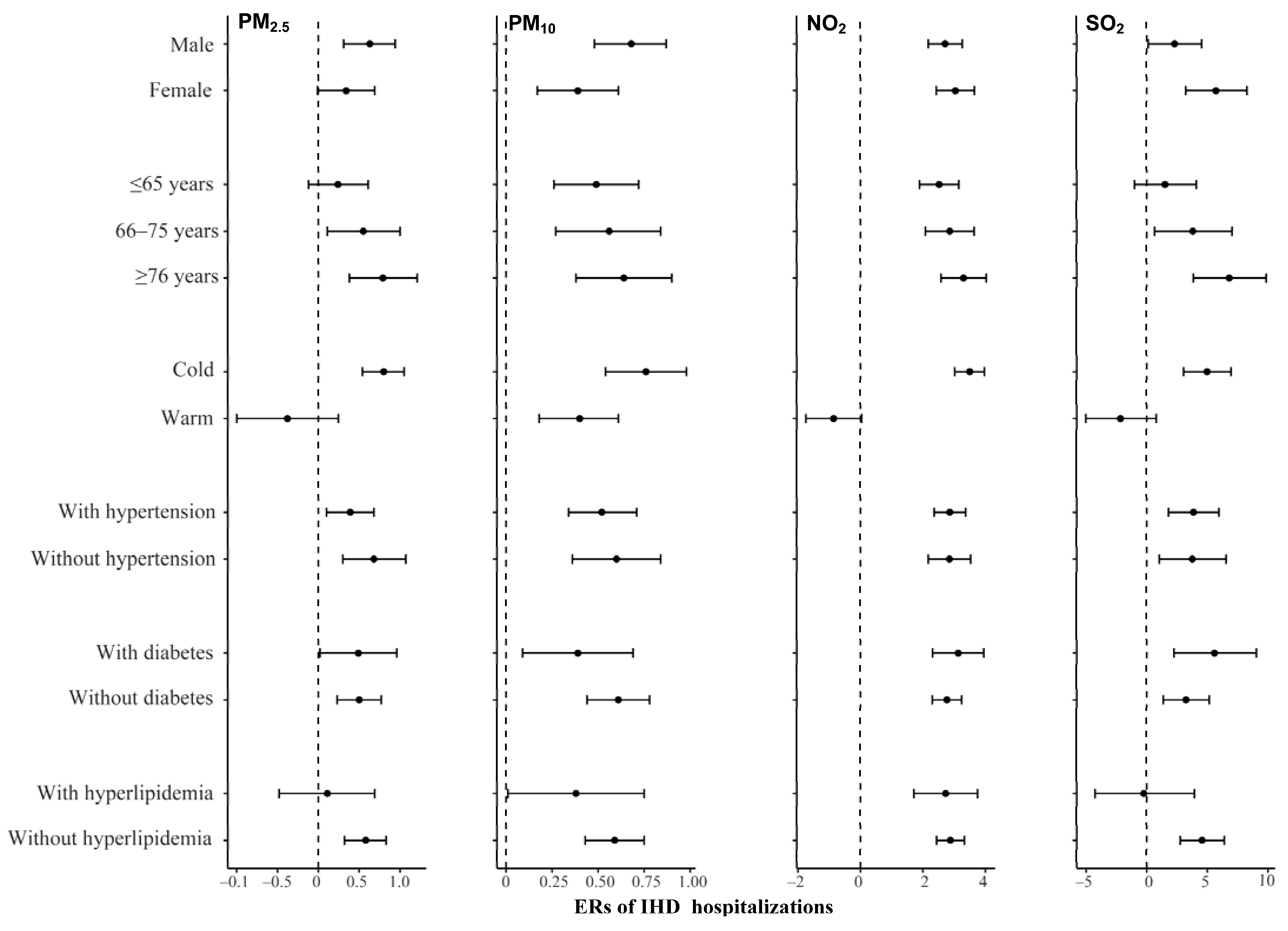
3.3. Stratified Analysis
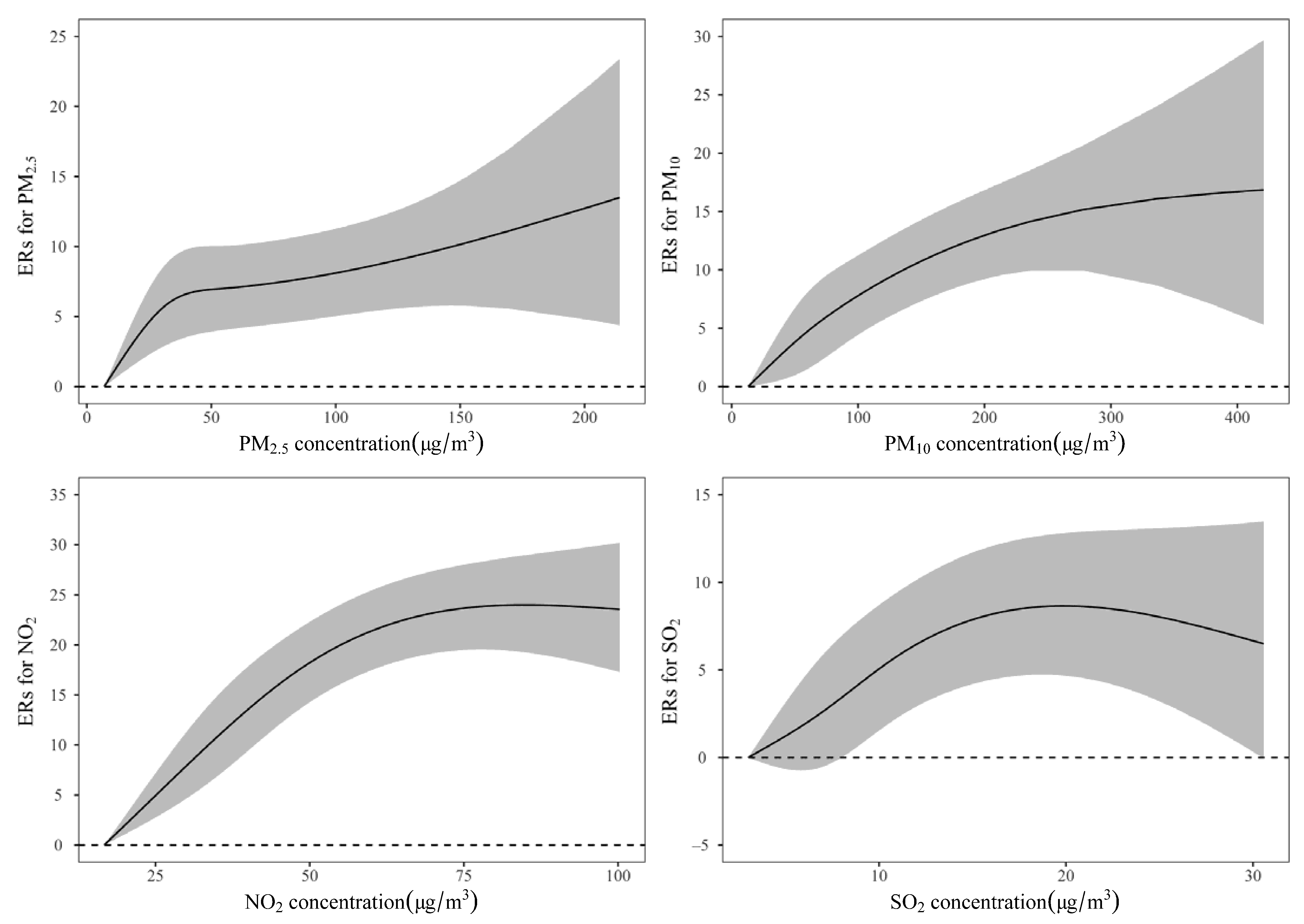
3.4. Exposure-Response Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Air Pollutants | China AQS Grade I Criteria | China AQS Grade II Criteria | ||
|---|---|---|---|---|
| 24-h Concentration (μg/m3) | Days Exceeded Criteria (%) | 24-h Concentration (μg/m3) | Days Exceeded Criteria (%) | |
| PM2.5 | 35 | 442 (61) | 75 | 115 (16) |
| PM10 | 50 | 539 (74) | 150 | 44 (6) |
| NO2 | 80 | 31 (4) | 80 | 31 (4) |
| SO2 | 50 | 0 (0) | 150 | 0 (0) |

References
- Pun, V.C.; Yu, I.T.; Ho, K.; Qiu, H.; Sun, Z.; Tian, L. Differential Effects of Source-Specific Particulate Matter on Emergency Hospitalizations for Ischemic Heart Disease in Hong Kong. Environ. Health Perspect. 2014, 122, 391–396. [Google Scholar] [CrossRef] [PubMed]
- The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 4 October 2021).
- Wang, C.R.; Meng, X.F.; Wang, C.P.; Liu, S.W. Trends of burden on ischemic heart disease and epidemiological transition of related risk factors in China, 1990–2017. Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi 2020, 41, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- The Writing Committee of the Report on Cardiovascular Health and Diseases in China Report on Cardiovascular Health and Diseases Burden in China: An Updated Summary of 2020. Chin. Circ. J. 2021, 36, 521–545. [CrossRef]
- Ren, Z.; Liu, X.; Liu, T.; Chen, D.; Jiao, K.; Wang, X.; Suo, J.; Yang, H.; Liao, J.; Ma, L. Effect of Ambient Fine Particulates (PM2.5) on Hospital Admissions for Respiratory and Cardiovascular Diseases in Wuhan, China. Respir. Res. 2021, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Loxham, M.; Davies, D.E.; Holgate, S.T. The Health Effects of Fine Particulate Air Pollution. BMJ 2019, l6609. [Google Scholar] [CrossRef] [PubMed]
- Xu, A.; Mu, Z.; Jiang, B.; Wang, W.; Yu, H.; Zhang, L.; Li, J. Acute Effects of Particulate Air Pollution on Ischemic Heart Disease Hospitalizations in Shanghai, China. Int. J. Environ. Res. Public. Health 2017, 14, 168. [Google Scholar] [CrossRef]
- Hu, J.; Tang, M.; Zhang, X.; Ma, Y.; Li, Y.; Chen, R.; Kan, H.; Cui, Z.; Ge, J. Size-Fractionated Particulate Air Pollution and Myocardial Infarction Emergency Hospitalization in Shanghai, China. Sci. Total Environ. 2020, 737, 140100. [Google Scholar] [CrossRef]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of Gaseous and Solid Constituents of Air Pollution on Endothelial Function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehbi, H.-M.; Blangiardo, M.; Gulliver, J.; Fecht, D.; de Hoogh, K.; Al-Kanaani, Z.; Tillin, T.; Hardy, R.; Chaturvedi, N.; Hansell, A.L. Air Pollution and Cardiovascular Mortality with over 25years Follow-up: A Combined Analysis of Two British Cohorts. Environ. Int. 2017, 99, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Yu, Y.; Yu, C.; Shi, F.; Zhang, Y. Associations between Acute Exposure to Ambient Air Pollution and Length of Stay for Inpatients with Ischemic Heart Disease: A Multi-City Analysis in Central China. Environ. Sci. Pollut. Res. 2020, 27, 43743–43754. [Google Scholar] [CrossRef]
- Qiu, H.; Yu, I.T.-S.; Wang, X.; Tian, L.; Tse, L.A.; Wong, T.W. Cool and Dry Weather Enhances the Effects of Air Pollution on Emergency IHD Hospital Admissions. Int. J. Cardiol. 2013, 168, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine Particulate Air Pollution and Hospital Admission for Cardiovascular and Respiratory Diseases. JAMA 2006, 295, 1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, L.P.; Millet, D.B.; Marshall, J.D. National Patterns in Environmental Injustice and Inequality: Outdoor NO2 Air Pollution in the United States. PLoS ONE 2014, 9, e94431. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.W. Associations between Daily Mortalities from Respiratory and Cardiovascular Diseases and Air Pollution in Hong Kong, China. Occup. Environ. Med. 2002, 59, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Xu, M.M.; Jia, Y.P.; Li, G.X.; Liu, L.Q.; Mo, Y.Z.; Jin, X.B.; Pan, X.C. Relationship between Ambient Fine Particles and Ventricular Repolarization Changes and Heart Rate Variability of Elderly People with Heart Disease in Beijing, China. Biomed. Environ. Sci. BES 2013, 26, 629–637. [Google Scholar] [CrossRef]
- Zhang, C.; Ding, R.; Xiao, C.; Xu, Y.; Cheng, H.; Zhu, F.; Lei, R.; Di, D.; Zhao, Q.; Cao, J. Association between Air Pollution and Cardiovascular Mortality in Hefei, China: A Time-Series Analysis. Environ. Pollut. 2017, 229, 790–797. [Google Scholar] [CrossRef]
- Zhao, D.; Xin, J.; Wang, W.; Jia, D.; Wang, Z.; Xiao, H.; Liu, C.; Zhou, J.; Tong, L.; Ma, Y.; et al. Effects of the Sea-Land Breeze on Coastal Ozone Pollution in the Yangtze River Delta, China. Sci. Total Environ. 2022, 807, 150306. [Google Scholar] [CrossRef]
- Wang, X.; Wang, W.; Jiao, S.; Yuan, J.; Hu, C.; Wang, L. The Effects of Air Pollution on Daily Cardiovascular Diseases Hospital Admissions in Wuhan from 2013 to 2015. Atmos. Environ. 2018, 182, 307–312. [Google Scholar] [CrossRef]
- Xu, Z.; Xiong, L.; Jin, D.; Tan, J. Association between Short-Term Exposure to Sulfur Dioxide and Carbon Monoxide and Ischemic Heart Disease and Non-Accidental Death in Changsha City, China. PLoS ONE 2021, 16, e0251108. [Google Scholar] [CrossRef]
- Gao, M.; Lv, J.; Yu, C.; Guo, Y.; Bian, Z.; Yang, R.; Du, H.; Yang, L.; Chen, Y.; Li, Z.; et al. Metabolically Healthy Obesity, Transition to Unhealthy Metabolic Status, and Vascular Disease in Chinese Adults: A Cohort Study. PLoS Med. 2020, 17, e1003351. [Google Scholar] [CrossRef]
- de FC Lichtenfels, A.J.; van der Plaat, D.A.; de Jong, K.; van Diemen, C.C.; Postma, D.S.; Nedeljkovic, I.; van Duijn, C.M.; Amin, N.; la Bastide-van Gemert, S.; de Vries, M.; et al. Long-Term Air Pollution Exposure, Genome-Wide DNA Methylation and Lung Function in the LifeLines Cohort Study. Environ. Health Perspect. 2018, 126, 027004. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, X.; Lv, C.; Li, W.; Ma, D.; Zhang, Q.; Dong, L. The Effect of Air Pollution on Hospitalization of Individuals with Respiratory and Cardiovascular Diseases in Jinan, China. Medicine 2019, 98, e15634. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Wu, M.; Qian, S.; Li, D.; Jin, M.; Wang, J.; Shui, L.; Lin, H.; Tang, M.; Chen, K. Association between Short-Term Exposure to Ambient Air Pollution and Hospital Visits for Depression in China. Sci. Total Environ. 2020, 724, 138207. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Luo, Y.; Tan, P.; Xu, Q.; Tao, L.; Guo, J.; Zhang, F.; Xie, X.; Guo, X. Gaseous Air Pollution and the Risk for Stroke Admissions: A Case-Crossover Study in Beijing, China. Int. J. Environ. Res. Public. Health 2017, 14, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Effects of Air Pollution on the Incidence of Myocardial Infarction. Heart Br. Card. Soc. 2009, 95, 1746–1759. [Google Scholar] [CrossRef] [Green Version]
- Stieb, D.M.; Szyszkowicz, M.; Rowe, B.H.; Leech, J.A. Air Pollution and Emergency Department Visits for Cardiac and Respiratory Conditions: A Multi-City Time-Series Analysis. Environ. Health 2009, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Routledge, H.C. Effect of Inhaled Sulphur Dioxide and Carbon Particles on Heart Rate Variability and Markers of Inflammation and Coagulation in Human Subjects. Heart 2006, 92, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.A.; Muhlestein, J.B.; May, H.T.; Renlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic Heart Disease Events Triggered by Short-Term Exposure to Fine Particulate Air Pollution. Circulation 2006, 114, 2443–2448. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wang, T.; Liu, S.; Brook, R.D.; Feng, B.; Zhao, Q.; Song, X.; Yi, T.; Chen, J.; Zhang, Y.; et al. Extreme Levels of Air Pollution Associated With Changes in Biomarkers of Atherosclerotic Plaque Vulnerability and Thrombogenicity in Healthy Adults: The Beijing AIRCHD Study. Circ. Res. 2019, 124, e30–e43. [Google Scholar] [CrossRef]
- Chen, R.; Chu, C.; Tan, J.; Cao, J.; Song, W.; Xu, X.; Jiang, C.; Ma, W.; Yang, C.; Chen, B.; et al. Ambient Air Pollution and Hospital Admission in Shanghai, China. J. Hazard. Mater. 2010, 181, 234–240. [Google Scholar] [CrossRef]
- Huang, J.; Li, G.; Qian, X.; Xu, G.; Zhao, Y.; Huang, J.; Liu, Q.; He, T.; Guo, X. The Burden of Ischemic Heart Disease Related to Ambient Air Pollution Exposure in a Coastal City in South China. Environ. Res. 2018, 164, 255–261. [Google Scholar] [CrossRef]
- Miller, M.R. Oxidative Stress and the Cardiovascular Effects of Air Pollution. Free Radic. Biol. Med. 2020, 151, 69–87. [Google Scholar] [CrossRef] [PubMed]
- Bourdrel, T.; Bind, M.-A.; Béjot, Y.; Morel, O.; Argacha, J.-F. Cardiovascular Effects of Air Pollution. Arch. Cardiovasc. Dis. 2017, 110, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.G.; Williams, G.M.; Schwartz, J.; Best, T.L.; Neller, A.H.; Petroeschevsky, A.L.; Simpson, R.W. The Effects of Air Pollution on Hospitalizations for Cardiovascular Diseasein Elderly People in Australian and New Zealand Cities. Environ. Health Perspect. 2006, 114, 1018–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, J.D.; Adar, S.D.; Barr, R.G.; Budoff, M.; Burke, G.L.; Curl, C.L.; Daviglus, M.L.; Roux, A.V.D.; Gassett, A.J.; Jacobs, D.R.; et al. Association between Air Pollution and Coronary Artery Calcification within Six Metropolitan Areas in the USA (the Multi-Ethnic Study of Atherosclerosis and Air Pollution): A Longitudinal Cohort Study. Lancet 2016, 388, 696–704. [Google Scholar] [CrossRef] [Green Version]
- Goldberg, M.S.; Burnett, R.T.; Stieb, D.M.; Brophy, J.M.; Daskalopoulou, S.S.; Valois, M.-F.; Brook, J.R. Associations between Ambient Air Pollution and Daily Mortality among Elderly Persons in Montreal, Quebec. Sci. Total Environ. 2013, 463–464, 931–942. [Google Scholar] [CrossRef]
- Zhang, R.; Jiang, Y.; Zhang, G.; Yu, M.; Wang, Y.; Liu, G. Association between Short-Term Exposure to Ambient Air Pollution and Hospital Admissions for Transient Ischemic Attacks in Beijing, China. Environ. Sci. Pollut. Res. 2021, 28, 6877–6885. [Google Scholar] [CrossRef]
- Bai, L.; Weichenthal, S.; Kwong, J.C.; Burnett, R.T.; Hatzopoulou, M.; Jerrett, M.; van Donkelaar, A.; Martin, R.V.; Van Ryswyk, K.; Lu, H.; et al. Associations of Long-Term Exposure to Ultrafine Particles and Nitrogen Dioxide with Increased Incidence of Congestive Heart Failure and Acute Myocardial Infarction. Am. J. Epidemiol. 2019, 188, 151–159. [Google Scholar] [CrossRef]
- Zhang, S.; Li, G.; Tian, L.; Guo, Q.; Pan, X. Short-Term Exposure to Air Pollution and Morbidity of COPD and Asthma in East Asian Area: A Systematic Review and Meta-Analysis. Environ. Res. 2016, 148, 15–23. [Google Scholar] [CrossRef]
- Henneberger, A.; Zareba, W.; Ibald-Mulli, A.; Rückerl, R.; Cyrys, J.; Couderc, J.-P.; Mykins, B.; Woelke, G.; Wichmann, H.-E.; Peters, A. Repolarization Changes Induced by Air Pollution in Ischemic Heart Disease Patients. Environ. Health Perspect. 2005, 113, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Patsouras, M.D.; Vlachoyiannopoulos, P.G. Evidence of Epigenetic Alterations in Thrombosis and Coagulation: A Systematic Review. J. Autoimmun. 2019, 104, 102347. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Maquiling, A.; Thomson, E.M.; Park, I.-W.; Stieb, D.M.; Dehghani, P. Sex-Difference in Air Pollution-Related Acute Circulatory and Respiratory Mortality and Hospitalization. Sci. Total Environ. 2022, 806, 150515. [Google Scholar] [CrossRef] [PubMed]
- Clougherty, J.E. A Growing Role for Gender Analysis in Air Pollution Epidemiology. Environ. Health Perspect. 2010, 118, 167–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Regitz-Zagrosek, V. (Ed.) Sex and Gender Differences in Pharmacology. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2012; Volume 214, ISBN 978-3-642-30725-6. [Google Scholar]
- Chen, Y.-C.; Weng, Y.-H.; Chiu, Y.-W.; Yang, C.-Y. Short-Term Effects of Coarse Particulate Matter on Hospital Admissions for Cardiovascular Diseases: A Case-Crossover Study in a Tropical City. J. Toxicol. Environ. Health A 2015, 78, 1241–1253. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Gao, J.; Cao, G.; Ouyang, F. Chemical Composition and Source Identification of PM2.5 in the Suburb of Shenzhen, China. Atmosp. Res. 2013, 122, 391–400. [Google Scholar] [CrossRef]
- Hoffmann, B.; Luttmann-Gibson, H.; Cohen, A.; Zanobetti, A.; de Souza, C.; Foley, C.; Suh, H.H.; Coull, B.A.; Schwartz, J.; Mittleman, M.; et al. Opposing Effects of Particle Pollution, Ozone, and Ambient Temperature on Arterial Blood Pressure. Environ. Health Perspect. 2012, 120, 241–246. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J. Air Pollution and Emergency Admissions in Boston, MA. J. Epidemiol. Community Health 2006, 60, 890–895. [Google Scholar] [CrossRef] [Green Version]
- Pereira Filho, M.A.; Pereira, L.A.A.; Arbex, F.F.; Arbex, M.; Conceição, G.M.; Santos, U.P.; Lopes, A.C.; Saldiva, P.H.N.; Braga, A.L.F.; Cendon, S. Effect of Air Pollution on Diabetes and Cardiovascular Diseases in São Paulo, Brazil. Braz. J. Med. Biol. Res. 2008, 41, 526–532. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.K.; Tager, I.B.; Lurmann, F.; Segal, M.; Quesenberry, C.P.; Lugg, M.M.; Shan, J.; Van Den Eeden, S.K. Air Pollution and Hospital Admissions for Ischemic Heart Disease in Persons with Congestive Heart Failure or Arrhythmia. Environ. Health Perspect. 2002, 110, 1247–1252. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Liu, X.; Wang, X.; Qu, W.; Li, W.; Dong, L. Effect of Air Pollution on Hospitalization for Acute Exacerbation of Chronic Obstructive Pulmonary Disease, Stroke, and Myocardial Infarction. Environ. Sci. Pollut. Res. 2020, 27, 3384–3400. [Google Scholar] [CrossRef]
- Doiron, D.; de Hoogh, K.; Probst-Hensch, N.; Fortier, I.; Cai, Y.; De Matteis, S.; Hansell, A.L. Air Pollution, Lung Function and COPD: Results from the Population-Based UK Biobank Study. Eur. Respir. J. 2019, 54, 1802140. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.D.; Spalt, E.W.; Curl, C.L.; Hajat, A.; Jones, M.R.; Kim, S.-Y.; Vedal, S.; Szpiro, A.A.; Gassett, A.; Sheppard, L.; et al. Advances in Understanding Air Pollution and CVD. Glob. Heart 2016, 11, 343. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Tuzcu, E.M.; Libby, P.; Thompson, P.D.; Ghali, M.; Garza, D.; Berman, L.; Shi, H.; Buebendorf, E.; Topol, E.J. Effect of Antihypertensive Agents on Cardiovascular Events in Patients with Coronary Disease and Normal Blood Pressure: The CAMELOT study: A randomized controlled trial. JAMA 2004, 292, 2217–2225. [Google Scholar] [CrossRef] [Green Version]
- Leru, P.M.; Eftimie, A.-M.; Anton, V.F.; Thibaudon, M. Five-Year Data on Pollen Monitoring, Distribution and Health Impact of Allergenic Plants in Bucharest and the Southeastern Region of Romania. Medicina 2019, 55, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otrisal, P.; Bungau, C.; Obsel, V.; Melicharik, Z.; Tont, G. Selected Respiratory Protective Devices: Respirators and Significance of Some Markings. Sustainability 2021, 13, 4988. [Google Scholar] [CrossRef]
- Apostol, L.; Berca, L.; Mosoiu, C.; Badea, M.; Bungau, S.; Oprea, O.B.; Cioca, G. Partially Defatted Pumpkin (Cucurbita Maxima) Seeds—A Rich Source of Nutrients for Use in Food Products. Rev. Chim. 2018, 69, 1398–1402. [Google Scholar] [CrossRef]
- Behl, T.; Bungau, S.; Kumar, K.; Zengin, G.; Khan, F.; Kumar, A.; Kaur, R.; Venkatachalam, T.; Tit, D.M.; Vesa, C.M.; et al. Pleotropic Effects of Polyphenols in Cardiovascular System. Biomed. Pharmacother. 2020, 130, 110714. [Google Scholar] [CrossRef]
- Kumar, S.; Behl, T.; Sachdeva, M.; Sehgal, A.; Kumari, S.; Kumar, A.; Kaur, G.; Yadav, H.N.; Bungau, S. Implicating the Effect of Ketogenic Diet as a Preventive Measure to Obesity and Diabetes Mellitus. Life Sci. 2021, 264, 118661. [Google Scholar] [CrossRef]
- Host, S.; Honoré, C.; Joly, F.; Saunal, A.; Le Tertre, A.; Medina, S. Implementation of Various Hypothetical Low Emission Zone Scenarios in Greater Paris: Assessment of Fine-Scale Reduction in Exposure and Expected Health Benefits. Environ. Res. 2020, 185, 109405. [Google Scholar] [CrossRef]
- Cosselman, K.E.; Navas-Acien, A.; Kaufman, J.D. Environmental Factors in Cardiovascular Disease. Nat. Rev. Cardiol. 2015, 12, 627–642. [Google Scholar] [CrossRef]



| Population Characteristics | IHD Hospitalizations (n = 139,616) |
|---|---|
| Age, mean ± SD | 68.56 ± 12.4 |
| Age group, n (%) | |
| ≤65 | 58,197 (41.7) |
| 66–75 | 37,351 (26.8) |
| ≥76 | 44,068 (31.6) |
| Gender, n (%) | |
| Male | 77,724 (55.7) |
| Female | 61,892 (44.3) |
| Season at admission, n (%) | |
| Cold | 71,832 (51.4) |
| Warm | 67,784 (48.6) |
| With Hypertension, n (%) | 88,425 (63.3) |
| With Diabetes, n (%) | 34,560 (24.8) |
| With Hyperlipidemia, n (%) | 24,891 (17.8) |
| Variables | Mean ± SD | Min | P25 | Median | P75 | Max |
|---|---|---|---|---|---|---|
| Air pollutants (μg/m3) | ||||||
| PM2.5 | 48.43 ± 29.47 | 6.97 | 26.79 | 41.51 | 61.79 | 214.10 |
| PM10 | 82.07 ± 47.89 | 9.86 | 49.15 | 73.52 | 10.54 | 559.35 |
| NO2 | 42.22 ± 16.11 | 16.67 | 32.04 | 41.21 | 52.16 | 100.27 |
| SO2 | 9.78 ± 4.80 | 3.00 | 6.19 | 8.57 | 12.05 | 30.57 |
| Weather conditions | ||||||
| Temperature (°C) | 17.52 ± 9.32 | −3.80 | 9.50 | 18.10 | 25.80 | 33.90 |
| Humidity (%) | 79.39 ± 10.26 | 47.00 | 72.00 | 80.00 | 87.00 | 100.00 |
| Daily IHD case | 192.60 ± 69.50 | 47.00 | 135.00 | 189.00 | 238.00 | 456.00 |
| Air Pollution | Single Lag | Moving-Average Lag | ||
|---|---|---|---|---|
| Lag Day | ERs (95% CI) | Lag Day | ERs (95% CI) | |
| PM2.5 | 0 | 0.50 (0.27–0.73) | 01 | 0.31 (0.18–0.44) |
| 1 | 0.49 (0.25–0.73) | 02 | 0.20 (0.05–0.34) | |
| 2 | 0.03 (−0.19–0.26) | 03 | 0.24 (0.09–0.39) | |
| 3 | 0.03 (−0.19–0.26) | |||
| PM10 | 0 | 0.50 (0.36–0.64) | 01 | 0.55 (0.41–0.70) |
| 1 | 0.39 (0.27–0.52) | 02 | 0.48 (0.32–0.63) | |
| 2 | 0.09 (−0.02–0.21) | 03 | 0.38 (0.21–0.54) | |
| 3 | −0.10 (−0.22–0.02) | |||
| NO2 | 0 | 2.86 (2.45–3.26) | 01 | 2.76 (2.31–3.20) |
| 1 | 1.78 (1.38–2.18) | 02 | 2.43 (1.95–2.91) | |
| 2 | 0.60 (0.21–0.99) | 03 | 2.06 (1.55–2.56) | |
| 3 | −0.2 (−0.59–0.19) | |||
| SO2 | 0 | 3.82 (2.17–5.49) | 01 | 2.17 (0.45–3.93) |
| 1 | −0.03 (−1.46–1.42) | 02 | 2.20 (0.41–4.02) | |
| 2 | 1.37 (0.01–2.75) | 03 | 1.49 (−0.36–3.37) | |
| 3 | −0.77 (−2.1–0.58) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, W.; Liu, X.; Huang, Z.; Du, Y.; Zhang, B.; Wang, Q.; Xiang, J.; Zou, Y.; Ma, L. Acute Effects of Air Pollution on Ischemic Heart Disease Hospitalizations: A Population-Based Time-Series Study in Wuhan, China, 2017–2018. Int. J. Environ. Res. Public Health 2021, 18, 12527. https://doi.org/10.3390/ijerph182312527
Xu W, Liu X, Huang Z, Du Y, Zhang B, Wang Q, Xiang J, Zou Y, Ma L. Acute Effects of Air Pollution on Ischemic Heart Disease Hospitalizations: A Population-Based Time-Series Study in Wuhan, China, 2017–2018. International Journal of Environmental Research and Public Health. 2021; 18(23):12527. https://doi.org/10.3390/ijerph182312527
Chicago/Turabian StyleXu, Wanglin, Xingyuan Liu, Zenghui Huang, Yating Du, Biao Zhang, Qiaomai Wang, Jing Xiang, Yuliang Zou, and Lu Ma. 2021. "Acute Effects of Air Pollution on Ischemic Heart Disease Hospitalizations: A Population-Based Time-Series Study in Wuhan, China, 2017–2018" International Journal of Environmental Research and Public Health 18, no. 23: 12527. https://doi.org/10.3390/ijerph182312527
APA StyleXu, W., Liu, X., Huang, Z., Du, Y., Zhang, B., Wang, Q., Xiang, J., Zou, Y., & Ma, L. (2021). Acute Effects of Air Pollution on Ischemic Heart Disease Hospitalizations: A Population-Based Time-Series Study in Wuhan, China, 2017–2018. International Journal of Environmental Research and Public Health, 18(23), 12527. https://doi.org/10.3390/ijerph182312527