
Acute-Stage Mental Health Symptoms by Natural Disaster Type: Consultations of Disaster Psychiatric Assistance Teams (DPATs) in Japan

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
3.1. Patient Selection
3.2. Overview of Four Types of Disasters
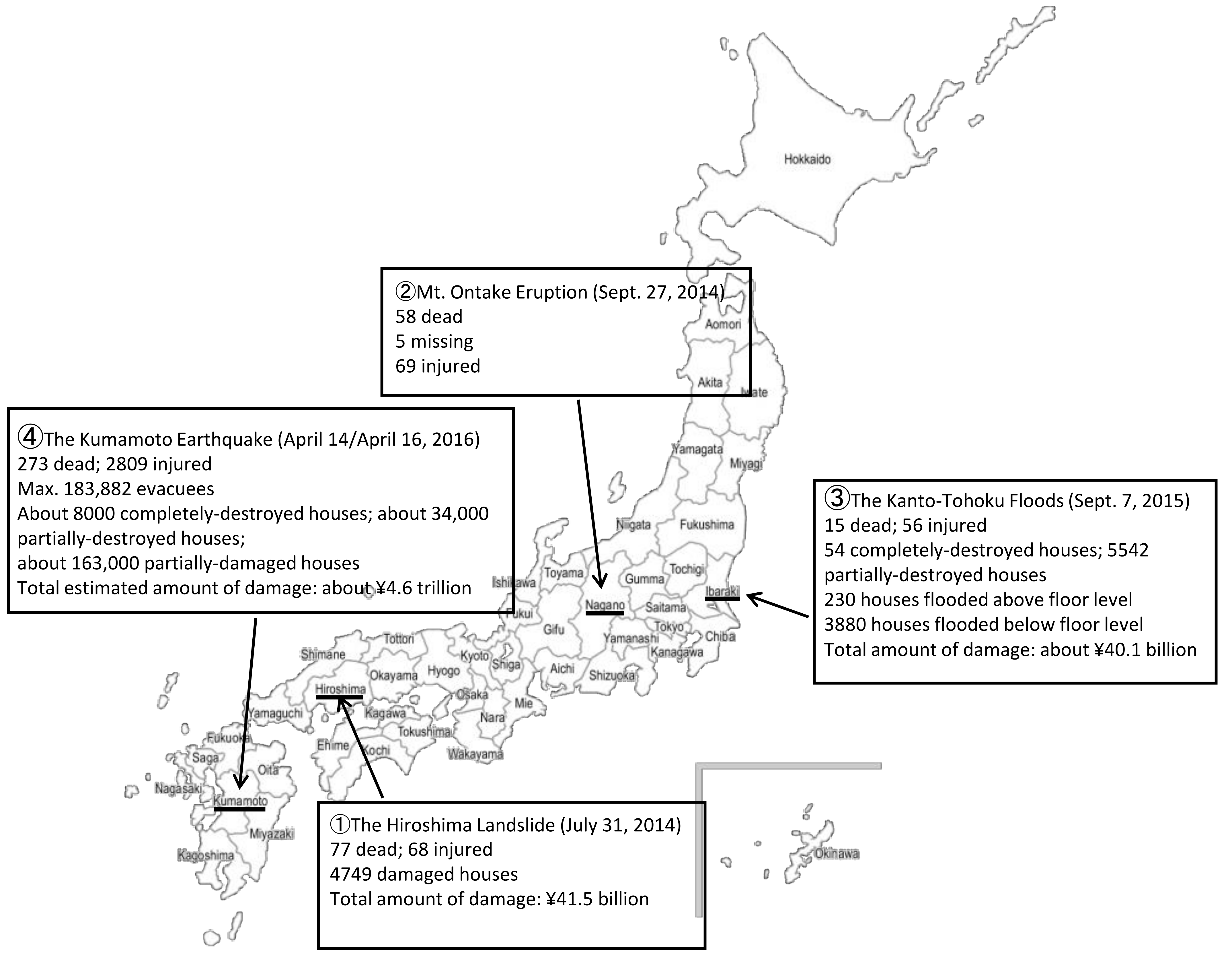
3.2.1. Hiroshima Landslide
3.2.2. The Mt. Ontake Volcanic Eruption
3.2.3. Kanto-Tohoku Floods
3.2.4. Kumamoto Earthquake
3.3. Comparison of Basic Attributes, Diagnoses, and Symptoms of the Target Population by Disaster
3.4. Diagnosis and Symptoms of Four Disasters, and Comparison with the Subjects’ Basic Attributes
3.5. Diagnosis of Four Disasters and Symptoms, and Comparison with Disaster Statuses
4. Discussion
4.1. Major Diseases and Symptoms: Acute Stage of Disasters
4.2. Risk Factors of Individuals Requiring Mental Health Support: Acute Stage of Disasters
4.3. Factors That Influence Acute-Stage Mental Health: Type of Disaster
4.4. Limitations of this Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MIMMS Japan Committee. MIMMS’ Practical Approaches Taken in on-Site Medical Activities during Major Accidents, 3rd ed.; Nagai Shoten: Yamagata, Japan, 2013. (In Japanese) [Google Scholar]
- Norris, F.H.; Elrod, C.L. Psychosocial consequences of disaster: A review of past research. In Methods for Disaster Mental Health Research; Norris, F.H., Galea, S., Friedman, M.J., Watson, P.J., Eds.; Guilford Press: New York, NY, USA, 2006; pp. 20–42. [Google Scholar]
- Ommeren, M.V.; Saxena, S.; Saraceno, B. Aid after disasters Needs a long term public mental health perspective. BMJ Open 2005, 330, 1160–1161. [Google Scholar]
- Otsuka, K.; Kato, H.; Kim, Y.; Matsumoto, K. (Eds.) Mental Health during Disasters; Igaku Shoin: Tokyo, Japan, 2016; pp. 21–24. (In Japanese) [Google Scholar]
- Storch, E.A.; Shah, A.; Salloum, A.; Valles, N.; Banu, S.; Schneider, S.C.; Kaplow, J.; Goodman, W.K. Psychiatric diagnoses and medications for Hurricane Harvey sheltered evacuees. Int. J. Environ. Res. Public Health 2019, 18, 1099–1102. [Google Scholar] [CrossRef] [PubMed]
- Neria, Y.; Nandi, A.; Galea, S. Post-traumatic stress disorder following disasters: A systematic review. Psychol. Med. 2008, 38, 467–480. [Google Scholar] [CrossRef] [PubMed]
- Makwana, N. Disaster and its impact on mental health: A narrative review. J. Fam. Med. Prim. Care 2019, 8, 3090–3095. [Google Scholar] [CrossRef] [PubMed]
- Lowe, S.R.; Bonumwezi, J.L.; Valdespino-Hayden, Z.; Galea, S. Posttraumatic stress and depression in the aftermath of envi-ronmental disasters: A review of quantitative studies published in 2018. Curr. Environ. Health Rep. 2019, 6, 344–360. [Google Scholar] [CrossRef] [PubMed]
- Paxson, C.; Fussell, E.; Rhodes, J.; Waters, M. Five years later: Recovery from post-traumatic stress and psychological distress among low-income mothers affected by Hurricane Katrina. Soc. Sci. Med. 2012, 74, 150–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raker, E.; Lowe, S.; Arcaya, M.; Johnson, S.T.; Rhodes, J.; Waters, M.C. Twelve years later: The long-term mental health consequences of Hurricane Katrina. Soc. Sci. Med. 2019, 242, 112610. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Lu, L.; Bai, Z.; Su, M.; Qi, Z.Q.; Zhang, S.Y.; Chen, Y.; Ao, B.Y.; Cui, F.Z.; Lagarde, E.; et al. Post-traumatic stress and school adaptation in adolescent survivors five years after the 2010 Yushu Earthquake in China. Int. J. Environ. Res. Public Health 2019, 16, 4167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hugelius, K.; Gifford, M.; Örtenwall, P.; Adolfsson, A. Health among disaster survivors and health professionals after the Haiyan Typhoon: A self-selected Internet-based web survey. Int. J. Emerg. Med. 2017, 10, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, E.; Tennichi, H.; Kameoka, S.; Kato, H. Long-term psychological recovery process and its associated factors among survivors of the Great Hanshin-Awaji Earthquake in Japan: A qualitative study. BMJ Open 2019, 9, e030250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwao, S.; Kouchi, Y.; Yamaguchi, N. A study of inpatients during the 3-month period after the earthquake. Jpn. J. Psychiatr. Treat. 1996, 11, 341–348. (In Japanese) [Google Scholar]
- Ritchie, E.C.; Watson, P.J.; Friedman, M.J. Psychiatric Interventions in Massive Disasters: Professional Preparations for Natural Disasters, Accidents, Wars, Terrorism Acts, etc.; Guildford Press: New York, NY, USA, 2007. (In Japanese) [Google Scholar]
- Fukuo, Y.; Tachikawa, H.; Takahashi, S.; Takagi, Y.; Yoshida, W.; Komi, M.; Arai, T.; Watari, M. An activity report of Disaster Psychiatric Assistant Team (DPAT) in the 2016 Kumamoto earthquake: Special reference to the statistical data from Disaster Mental Health Information Support System (DMHISS). J. Jpn. Emerg. Psychiatry 2018, 21, 86–94. [Google Scholar]
- Takahashi, S.; Takagi, Y.; Fukuo, Y.; Arai, T.; Watari, M.; Tachikawa, H. Acute mental health needs duration during major disasters: A phenomenological experience of disaster psychiatric assistance teams (DPATs) in Japan. Int. J. Environ. Res. Public Health. 2020, 17, 1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. Commissioned Project DPAT Office: DPAT Activity Manual Ver.2.1. Available online: https://www.dpat.jp/images/dpat_documents/3.pdf (accessed on 22 March 2021).
- Disaster Psychiatric Assistance Team (DPAT). An MHLW-Commissioned Project: Disaster Mental Health Information System: Operational Manual. Available online: https://www.dpat.jp/images/dmhiss/system_manual.pdf (accessed on 20 May 2021). (In Japanese).
- Atsushi, M.; Osamu, T. Reporting effectiveness in research papers: Basic concepts and important points. Engl. Educ. Stud. 2008, 31, 57–66. [Google Scholar]
- Jorge, I. The Influence of the E-Tutor on the Development of Collaborative Critical Thinking in a Student’s E-Forum: Association Levels with Cramer’s V. Available online: http://hdl.handle.net/10451/7097 (accessed on 20 May 2021).
- Cabinet Office. Collection of Documents on Disaster Response, Torrential Rain Disaster from 19 August 2014, Onward. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwj9gcCAktjwAhWRK5QKHRFDAz4QFjABegQIAxAD&url=http%3A%2F%2Fwww.bousai.go.jp%2Fkaigirep%2Fhoukokusho%2Fhukkousesaku%2Fsaigaitaiou%2Foutput_html_1%2Fpdf%2F201402.pdf&usg=AOvVaw3Hkf-PpUrOM_n2IlmrCoAg (accessed on 20 May 2021).
- Hiroshima City Health and Welfare Bureau, Public Health Department. Public Health and Medical Treatment Division Public Health Activities Due to Torrential Rain Disaster on 20 August 2014: On Physical and Psychological Care for Victims. Available online: http://www.bousai.go.jp/kaigirep/houkokusho/hukkousesaku/saigaitaiou/output_html_1/jirei_menu.html (accessed on 20 May 2021).
- Cabinet Office. Collection of Documents on Disaster Response Damage Due to 2014 Eruption of Mt. Ontake. Available online: http://www.bousai.go.jp/kaigirep/houkokusho/hukkousesaku/saigaitaiou/output_html_1/jirei_menu.html (accessed on 20 May 2021).
- Nagano Prefecture Mental Health and Welfare Center. Psychological Care for Disasters 2015 Care Providers’ Manual, 3rd ed. Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwjAnJqRlNjwAhUJwZQKHcJDBVQQFjAAegQIBBAD&url=https%3A%2F%2Fwww.pref.nagano.lg.jp%2Fseishin%2Ftosho%2Fdocuments%2Fdcare2015_allpage.pdf&usg=AOvVaw0c81k3BtTWlFQ5ndDCPOZ8 (accessed on 20 May 2021).
- Fire and Disaster Management Agency, Ministry of Internal Affairs and Communications. Status of Disaster by Heavy Rainfall, etc. in Typhoon No. 18 of 2015 (Report No. 40). Available online: https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&cad=rja&uact=8&ved=2ahUKEwiC3oTxlNjwAhWkzYsBHWIKBQEQFjAAegQIBBAD&url=https%3A%2F%2Fwww.fdma.go.jp%2Fdisaster%2Finfo%2Fassets%2Fpost793.pdf&usg=AOvVaw15v01CW-k3hw_xAK7gJeTZ (accessed on 20 May 2021). (In Japanese)
- FY2016 Statistical Documentation of Joso City. Available online: http://www.city.joso.lg.jp/gyosei/shokai/profile/tokei/1490083862926.html#a2 (accessed on 20 May 2021). (In Japanese).
- Cabinet Office. Collection of Documents on Disaster Response, Kumamoto Earthquake. Available online: http://www.bousai.go.jp/kaigirep/houkokusho/hukkousesaku/saigaitaiou/output_html_1/jirei_menu.html (accessed on 20 May 2021).
- Kumamoto Prefecture Population and Number of Households. Annual Report. 2015. Available online: https://www.pref.kumamoto.jp/soshiki/20/1119.html (accessed on 20 May 2021).
- Hitomi, M.; Kouhei, N.; Hyuntae, K.; Fumio, U.; Association for the Development of Earthquake Prevention. Fact-Finding Survey Report on the Operation of Evacuation Sites in the 2016 Kumamoto Earthquake. Tono Research Institute of Earthquake Science Report Seq. No. 39. Report of Committee to Research Basic Matters Concerning Standards for Regional Earthquake Preparation. Available online: http://www.tries.jp/research/2018031409513924.html (accessed on 22 November 2021). (In Japanese).
- Stoddard, F.J., Jr.; Pandya, A.; Katz, C.L.; Tomita, H.; Takahashi, Y.; Niwa, S. Disaster Psychiatry Readiness, Evaluation, and Treatment; Group for the Advancement of Psychiatry: New York, NY, USA; American Psychiatric Association: Arlington, VA, USA; London, UK, 2011. (In Japanese) [Google Scholar]
- Martin, U. Health after disaster: A perspective of psychological/health reactions to disaster. Cogent. Psychol. 2015, 2, 1053741. [Google Scholar] [CrossRef]
- Inter-Agency Standing Committee. IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings. Available online: https://www.who.int/mental_health/emergencies/guidelines_iasc_mental_health_psychosocial_june_2007.pdf (accessed on 20 May 2021).
- Briere, J.; Elliott, D. Prevalence, characteristics, and long-term sequelae of natural disaster exposure in the general population. J. Trauma. Stress 2000, 13, 661–679. [Google Scholar] [CrossRef] [PubMed]
- FY2018 Research Report on Reinforcing the Functions of the Disaster Psychiatric Assistance Team (DPAT). Available online: https://mhlw-grants.niph.go.jp/project/27286 (accessed on 22 November 2021). (In Japanese).
- Cabinet Office. Working Group to Investigate Large-Scale/Wide Area Evacuation in Floods/Storm Surge Flooding: Reference Document 3: Survey of Residents Regarding Joso Flood Damage (2015 Kanto/Tohoku Heavy Rain Disaster). Available online: http://www.bousai.go.jp/fusuigai/kozuiworking/pdf/dai3kai/sankosiryo3.pdf (accessed on 20 May 2021).
- Cabinet Office. Working Group to Investigate Disaster Response Based on Observation/Evaluation of Earthquakes along the Nankai Trough, Reference Document 1: Reasons for Evacuation and Evacuation Period of Residents in the Kumamoto Earthquake Based on the Results of an Analysis of a Questionnaire for Victims of the Kumamoto Earthquake. Available online: http://www.bousai.go.jp/jishin/nankai/taio_wg/pdf/h290703sanko01.pdf (accessed on 20 May 2021).
- Watari, M. Future disaster support—The practice of DPAT and future activities. Jap. Bull. Soc. Psychol. 2018, 27, 293–300. (In Japanese) [Google Scholar]

{kind=link}
| Total (N = 1806) | Volcanic Eruption (N = 12) | Landslide (N = 86) | Flood (N = 139) | Earthquake (N = 1569) | χ2 | Cramer’s V | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | |||||
| Gender | Man | 607 | 34.5 | 5 | 41.7 | 30 | 34.9 | 61 * | 43.9 | 511 | 33.6 | 6.27 | 0.06 | 0.00 |
| Woman | 1152 | 65.5 | 7 | 58.3 | 56 | 65.1 | 78 | 56.1 | 1011 * | 66.4 | ||||
| Age | Age under 20 | 149 | 9.5 | 0 | 0.0 | 29 | 34.5 | 4 | 3.1 | 116 | 8.6 | 78.19 | 0.16 | <0.0001 |
| Ages 20–64 | 730 | 46.7 | 6 | 75.0 | 33 * | 39.3 | 52 | 40.0 | 639 | 47.6 | ||||
| 65 and older | 685 | 43.8 | 2 | 25.0 | 22 | 26.2 | 74 * | 56.9 | 587 | 43.7 | ||||
| History of mental disease | Yes | 799 | 44.2 | 1 | 8.3 | 33 | 38.4 | 100 * | 71.9 | 665 | 42.4 | 74.24 | 0.14 | <0.0001 |
| No | 1010 | 55.8 | ||||||||||||
| DIAGNOSIS | Dementia | 96 | 9.2 | 0 | 0.0 | 1 | 2.0 | 20 * | 18.5 | 75 | 8.5 | 15.62 | 0.12 | 0.00 |
| Alcoholism | 30 | 2.9 | 0 | 0.0 | 0 | 0.0 | 2 | 1.9 | 28 | 3.2 | 2.43 | 0.05 | 0.49 | |
| Schizophrenia | 219 | 21.0 | 0 | 0.0 | 3 | 5.9 | 37 * | 34.3 | 179 | 20.4 | 20.58 | 0.14 | <0.0001 | |
| Depression | 87 | 8.3 | 0 | 0.0 | 2 | 3.9 | 8 | 7.4 | 77 | 8.8 | 2.27 | 0.05 | 0.52 | |
| Manic depression | 31 | 3.0 | 0 | 0.0 | 1 | 2.0 | 2 | 1.9 | 28 | 3.2 | 1.01 | 0.03 | 0.80 | |
| Acute stress disorders | 114 | 10.9 | 5 * | 71.4 | 11 * | 21.6 | 4 | 3.7 | 94 | 10.7 | 38.15 | 0.19 | <0.0001 | |
| PTSD | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.1 | 0.19 | 0.01 | 0.98 | |
| Natural disaster phobia | 13 | 1.2 | 0 | 0.0 | 1 | 2.0 | 0 | 0.0 | 12 | 1.4 | 1.77 | 0.04 | 0.62 | |
| Adjustment disorder | 112 | 10.7 | 1 | 14.3 | 12 * | 23.5 | 22 * | 20.4 | 77 | 8.8 | 22.88 | 0.15 | <0.0001 | |
| Other severe stress reactions | 141 | 13.5 | 0 | 0.0 | 3 | 5.9 | 0 | 0.0 | 138 * | 15.7 | 24.14 | 0.15 | <0.0001 | |
| Other anxiety disorders | 26 | 2.5 | 0 | 0.0 | 2 | 3.9 | 1 | 0.9 | 23 | 2.6 | 1.76 | 0.04 | 0.62 | |
| Somatoform disorder | 9 | 0.9 | 0 | 0.0 | 0 | 0.0 | 2 | 1.9 | 7 | 0.8 | 1.79 | 0.04 | 0.62 | |
| Sleep disorders | 76 | 7.3 | 0 | 0.0 | 7 | 13.7 | 6 | 5.6 | 63 | 7.2 | 4.19 | 0.06 | 0.24 | |
| Intellectual disability | 27 | 2.6 | 0 | 0.0 | 1 | 2.0 | 1 | 0.9 | 25 | 2.8 | 1.68 | 0.04 | 0.64 | |
| Autistic spectrum disorders | 43 | 4.1 | 0 | 0.0 | 5 * | 9.8 | 3 | 2.8 | 35 | 4.0 | 5.01 | 0.07 | 0.17 | |
| Other childhood mental disorders | 14 | 1.3 | 1 * | 14.3 | 1 | 2.0 | 0 | 0.0 | 12 | 1.4 | 10.50 | 0.10 | 0.02 | |
| Epilepsy | 6 | 0.6 | 0 | 0.0 | 1 | 2.0 | 0 | 0.0 | 5 | 0.6 | 2.38 | 0.05 | 0.50 | |
| SYMPTOM | Physical symptoms | 488 | 19.3 | 1 | 10.0 | 20 | 24.1 | 65 * | 47.8 | 402 | 27.8 | 26.88 | 0.13 | <0.0001 |
| Sleep problems | 596 | 23.5 | 1 | 10.0 | 45 * | 54.2 | 59 * | 43.4 | 491 | 34.0 | 20.60 | 0.11 | <0.0001 | |
| Anxiety symptoms | 667 | 26.3 | 8 * | 80.0 | 23 | 27.7 | 53 | 39.0 | 583 | 40.4 | 12.04 | 0.09 | 0.01 | |
| Symptoms related to mood and affect | 419 | 16.5 | 3 | 30.0 | 32 * | 38.6 | 29 | 21.3 | 355 | 24.6 | 9.37 | 0.08 | 0.03 | |
| Dissociation and conversion symptoms | 19 | 0.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 19 | 1.3 | 3.05 | 0.04 | 0.38 | |
| Oppressive symptoms | 17 | 0.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 17 | 1.2 | 2.72 | 0.04 | 0.44 | |
| Hallucinations and delusions | 103 | 4.1 | 0 | 0.0 | 3 | 3.6 | 13 | 9.6 | 87 | 6.0 | 4.35 | 0.05 | 0.23 | |
| Behavioral problems | 161 | 6.4 | 0 | 0.0 | 3 | 3.6 | 21 * | 15.4 | 137 | 9.5 | 9.83 | 0.08 | 0.02 | |
| Epileptic and convulsive seizures | 8 | 0.3 | 0 | 0.0 | 0 | 0.0 | 1 | 0.7 | 7 | 0.5 | 0.64 | 0.02 | 0.89 | |
| Drinking problems | 26 | 1.0 | 0 | 0.0 | 0 | 0.0 | 5 * | 3.7 | 21 | 1.5 | 5.57 | 0.06 | 0.14 | |
| Disturbance of consciousness | 3 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 3 | 0.2 | 0.48 | 0.02 | 0.92 | |
| Symptoms unique to children | 28 | 1.1 | 0 | 0.0 | 5 * | 6.0 | 2 | 1.5 | 21 | 1.5 | 10.17 | 0.08 | 0.02 | |
| Man | Woman | χ2 | φ | p | <20 | Age 20–64 | >65 | χ2 | Cramer’s V | p | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n | n | n | n | ||||||||
| DIAGNOSIS | Dementia | 35 | 60 | 0.03 | 0.01 | 0.87 | 0 | 3 | 85 * | 123.20 | 0.36 | <0.0001 |
| Alcoholism | 25 * | 5 | 27.55 | 0.16 | <0.0001 | 0 | 15 | 13 | 2.77 | 0.05 | 0.25 | |
| Schizophrenia | 104 * | 114 | 12.04 | 0.11 | 0.00 | 4 | 158 * | 43 | 76.66 | 0.28 | <0.0001 | |
| Depression | 25 | 61 | 2.91 | 0.05 | 0.09 | 1 | 43 | 33 | 5.86 | 0.08 | 0.05 | |
| Manic depression | 11 | 20 | 0.06 | 0.01 | 0.81 | 0 | 16 | 11 | 2.87 | 0.06 | 0.24 | |
| Acute stress disorders | 24 | 87 * | 13.53 | 0.11 | <0.0001 | 27 * | 40 | 37 | 44.02 | 0.21 | <0.0001 | |
| PTSD | 0 | 1 | 0.60 | 0.02 | 0.62 a | – | – | – | – | – | – | |
| Natural disaster phobia | 5 | 8 | 0.00 | 0.00 | 0.95 | 4 * | 4 | 4 | 9.35 | 0.10 | 0.01 | |
| Adjustment disorder | 43 | 69 | 0.03 | 0.01 | 0.85 | 10 | 48 | 52 | 2.24 | 0.05 | 0.33 | |
| Other severe stress reactions | 37 | 99 * | 7.21 | 0.08 | 0.01 | 17 | 63 | 50 | 3.66 | 0.06 | 0.18 | |
| Other anxiety disorders | 9 | 17 | 0.10 | 0.01 | 0.75 | 0 | 14 | 11 | 2.46 | 0.05 | 0.29 | |
| Somatoform disorder | 1 | 8 | 2.72 | 0.05 | 0.09 a | 0 | 6 | 3 | 1.41 | 0.04 | 0.49 | |
| Sleep disorders | 16 | 60 * | 9.57 | 0.10 | 0.00 | 2 | 21 | 48 * | 22.64 | 0.15 | <0.0001 | |
| Intellectual disability | 14 | 13 | 2.40 | 0.05 | 0.12 | 1 | 20 * | 3 | 10.86 | 0.11 | 0.00 | |
| Autistic spectrum disorders | 35 * | 7 | 39.04 | 0.19 | <0.0001 | 11 * | 28 * | 2 | 32.65 | 0.18 | <0.0001 | |
| Other childhood mental disorders | 2 | 11 | 2.77 | 0.05 | 0.08 a | 6 * | 4 | 2 | 26.29 | 0.17 | <0.0001 | |
| Epilepsy | 2 | 4 | 0.05 | 0.01 | 0.59 | 1 | 2 | 0 | 3.50 | 0.06 | 0.17 | |
| SYMPTOM | Physical symptoms | 154 | 322 | 0.68 | 0.02 | 0.41 | 26 | 184 | 219 * | 18.26 | 0.11 | <0.0001 |
| Sleep problems | 170 | 412 * | 8.72 | 0.07 | 0.00 | 42 | 264 | 241 | 4.20 | 0.05 | 0.12 | |
| Anxiety symptoms | 161 | 493 * | 41.53 | 0.16 | 0.00 | 61 | 290 | 238 | 3.86 | 0.05 | 0.15 | |
| Symptoms related to mood and affect | 136 | 274 | 0.12 | 0.01 | 0.73 | 28 | 192 | 155 | 5.27 | 0.06 | 0.07 | |
| Dissociation and conversion symptoms | 1 | 18 * | 7.02 | 0.07 | 0.00 a | 4 | 10 | 5 | 4.00 | 0.05 | 0.14 | |
| Oppressive symptoms | 9 | 8 | 2.79 | 0.04 | 0.10 | 1 | 11 | 5 | 2.23 | 0.04 | 0.33 | |
| Hallucinations and delusions | 42 | 61 | 2.35 | 0.04 | 0.13 | 3 | 71 * | 25 | 27.12 | 0.14 | <0.0001 | |
| Behavioral problems | 91 * | 67 | 43.98 | 0.16 | <0.0001 | 16 | 78 | 57 | 2.27 | 0.04 | 0.32 | |
| Epileptic and convulsive seizures | 3 | 5 | 0.05 | 0.01 | 0.55 a | 0 | 4 | 0 | 4.56 | 0.06 | 0.10 | |
| Drinking problems | 21 * | 5 | 25.96 | 0.13 | <0.0001 | 0 | 14 | 8 | 3.79 | 0.05 | 0.15 | |
| Disturbance of consciousness | 0 | 3 | 1.54 | 0.03 | 0.30 a | 0 | 0 | 2 | 2.60 | 0.04 | 0.27 | |
| Symptoms unique to children | 15 * | 13 | 4.94 | 0.06 | 0.03 | 25 * | 2 | 0 | 215.63 | 0.38 | <0.0001 | |
| History of Mental Illness | χ2 | φ | p | SCZ | χ2 | φ | p | BD | χ2 | φ | p | MDD | χ2 | φ | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | n | n | n | |||||||||||||
| SYMPTOM | ||||||||||||||||
| Physical symptoms | 199 | 2.61 | 0.05 | 0.11 | 25 * | 20.38 | 0.17 | <0.0001 | 11 * | 5.11 | 0.09 | 0.02 | 28 | 2.81 | 0.06 | 0.09 |
| Sleep problems | 296 | 2.61 | 0.05 | 0.11 | 56 * | 13.47 | 0.14 | <0.0001 | 13 | 1.56 | 0.05 | 0.21 | 51 * | 13.90 | 0.14 | <0.0001 |
| Anxiety symptoms | 311 | 2.53 | 0.04 | 0.11 | 59 * | 16.37 | 0.15 | <0.0001 | 14 | 1.83 | 0.05 | 0.18 | 36 | 0.09 | 0.01 | 0.76 |
| Symptoms related to mood and affect | 216 | 3.63 | 0.05 | 0.06 | 27 * | 29.85 | 0.21 | <0.0001 | 16 * | 15.16 | 0.15 | <0.0001 | 45 * | 24.08 | 0.19 | <0.0001 |
| Dissociation and conversion symptoms | 10 | 0.14 | 0.01 | 0.71 | 1 | 1.75 | 0.05 | 0.17 a | 0 | – | – | – | 2 | 0.45 | 0.03 | 0.38 a |
| Oppressive symptoms | 10 | 3.21 | 0.05 | 0.07 | 3 | 0.01 | 0.00 | 0.59 a | 0 | – | – | – | – | – | – | – |
| Hallucinations and delusions | 91 * | 53.05 | 0.20 | <0.0001 | 77 * | 169.30 | 0.49 | <0.0001 | 0 | – | – | – | – | – | – | – |
| Behavioral problems | 110 * | 35.78 | 0.17 | <0.0001 | 43 * | 6.77 | 0.07 | 0.01 | 2 | 1.30 | 0.04 | 0.20 a | 5 * | 8.19 | 0.11 | 0.00 |
| Epileptic and convulsive seizures | 7 * | 5.11 | 0.06 | 0.02 a | 2 | 0.00 | 0.00 | 0.68 | 0 | – | – | – | 1 | 0.01 | 0.00 | 0.62 a |
| Drinking problems | 15 | 3.50 | 0.05 | 0.06 | 3 | 0.58 | 0.03 | 0.33a | 0 | – | – | – | – | – | – | – |
| Disturbance of consciousness | 2 | 0.09 | 0.01 | 0.62 a | 0 | – | – | – | – | – | – | – | – | – | – | – |
| Symptoms unique to children | 7 | 11.57 | 0.09 | 0.00 | 1 | 0.19 | 0.02 | 0.55 a | 0 | – | – | – | – | – | – | – |
| Died or Missing | Injury of the Self | Injury of Family, Relative, Acquaintance | Collapse of House | Forced Displacement from Home | Loss of Property Other Than Home | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | Φ | p | n | χ2 | φ | p | |
| DIAGNOSIS | ||||||||||||||||||||||||
| Dementia | 1 | 2.53 | 0.05 | 0.08a | 1 | 0.74 | 0.03 | 0.34 a | 1 | 0.29 | 0.02 | 0.45 a | 30 | 2.33 | 0.05 | 0.13 | 17 * | 8.36 | 0.09 | 0.00 | 7 | 0.05 | 0.01 | 0.83 |
| Alcoholism | 0 | – | – | – | – | – | – | – | 1 | 0.47 | 0.02 | 0.41 a | 7 | 2.99 | 0.05 | 0.08 | 2 | 0.28 | 0.02 | 0.45 a | 0 | – | – | – |
| Schizophrenia | 6 | 1.33 | 0.04 | 0.25 | 2 | 2.36 | 0.05 | 0.12 | 2 | 1.07 | 0.03 | 0.24 a | 72 | 3.66 | 0.06 | 0.06 | 16 | 1.52 | 0.04 | 0.22 | 19 | 0.26 | 0.02 | 0.61 |
| Depression | 5 | 0.64 | 0.03 | 0.28 a | 3 | 0.56 | 0.02 | 0.32 a | 0 | – | – | – | 43 * | 4.81 | 0.07 | 0.03 | 3 | 4.02 | 0.06 | 0.05 | 4 | 1.39 | 0.04 | 0.24 |
| Manic depression | 1 | 0.06 | 0.01 | 0.63 a | 1 | 0.12 | 0.01 | 0.52 a | 0 | – | – | – | 13 | 0.16 | 0.01 | 0.69 | 3 | 0.00 | 0.00 | 0.58 | 1 | 0.94 | 0.03 | 0.29 |
| Acute Stress Disorders | 15 | 26.52 | 0.16 | <0.0001 a | 8 * | 12.71 | 0.11 | <0.0001 | 6 | 9.48 | 0.10 | 0.01 a | 56 * | 6.14 | 0.08 | 0.01 | 11 | 0.01 | 0.00 | 0.95 | 10 | 0.15 | 0.01 | 0.70 |
| PTSD | 1 * | 23.33 | 0.15 | 0.04 a | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – |
| Natural disaster phobia | 0 | – | – | – | 1 | 1.71 | 0.04 | 0.26 a | 0 | – | – | – | 3 | 1.32 | 0.04 | 0.25 | 1 | 0.05 | 0.01 | 0.65 a | 2 | 1.03 | 0.03 | 0.27 a |
| Adjustment Disorder | 6 | 0.49 | 0.02 | 0.31 a | 2 | 0.15 | 0.01 | 0.52 a | 5 * | 5.57 | 0.07 | 0.04 a | 56 * | 7.05 | 0.08 | 0.01 | 22 * | 15.13 | 0.12 | <0.0001 | 17 * | 9.33 | 0.09 | 0.00 |
| Other severe stress reactions | 2 | 3.00 | 0.05 | 0.08 | 4 | 0.21 | 0.01 | 0.41a | 2 | 0.09 | 0.01 | 0.55 a | 61 | 1.58 | 0.04 | 0.21 | 9 | 1.82 | 0.04 | 0.18 | 5 | 4.17 | 0.06 | 0.04 |
| Other anxiety disorders | 0 | – | – | – | 0 | – | – | – | 1 | 0.71 | 0.03 | 0.37 a | 8 | 0.67 | 0.03 | 0.41 | 2 | 0.01 | 0.01 | 0.27 a | 3 | 0.50 | 0.02 | 0.55 a |
| Somatoform disorder | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 3 | 0.10 | 0.01 | 0.52 a | 2 | 1.72 | 0.04 | 0.21 a | 1 | 0.13 | 0.01 | 0.52 a |
| Sleep Disorders | 3 | 0.01 | 0.00 | 0.62 a | 1 | 0.35 | 0.02 | 0.47 a | 0 | – | – | – | 27 | 0.30 | 0.02 | 0.58 | 9 | 0.54 | 0.02 | 0.46 | 11 * | 4.98 | 0.07 | 0.03 |
| Intellectual disability | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 7 | 1.84 | 0.04 | 0.18 | 1 | 1.08 | 0.03 | 0.26a | 1 | 0.66 | 0.03 | 0.36 a |
| Autistic spectrum disorders | 1 | 0.36 | 0.02 | 0.46 a | 0 | – | – | – | 0 | – | – | – | 11 | 3.15 | 0.06 | 0.08 | 0 | – | – | – | 0 | – | – | – |
| Other childhood mental disorders | 1 | 0.33 | 0.02 | 0.45 a | 1 | 1.49 | 0.04 | 0.28 a | 0 | – | – | – | 3 | 1.74 | 0.04 | 0.19 | 0 | – | – | – | 0 | – | – | – |
| Epilepsy | 1 | 2.41 | 0.05 | 0.22 a | 0 | – | – | – | – | – | – | – | 2 | 0.07 | 0.01 | 0.58a | 0 | – | – | – | 0 | – | – | – |
| Died or Missing | Injury of the Self | Injury of Family, Relative, Acquaintance | Collapse of House | Forced Displacement from Home | Loss of Property Other Than Home | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | n | χ2 | φ | p | |
| SYMPTOM | ||||||||||||||||||||||||
| Physical symptoms | 20 | 0.01 | 0.00 | 0.91 | 12 | 0.45 | 0.02 | 0.50 | 5 | 1.51 | 0.03 | 0.22 | 208 | 0.37 | 0.02 | 0.54 | 45 | 0.48 | 0.02 | 0.49 | 51 * | 6.56 | 0.06 | 0.01 |
| Sleep problems | 27 | 0.28 | 0.01 | 0.60 | 19 * | 5.43 | 0.06 | 0.02 | 11 | 0.31 | 0.01 | 0.58 | 291 * | 20.57 | 0.11 | <0.0001 | 68 * | 10.17 | 0.08 | 0.00 | 57 | 3.86 | 0.05 | 0.05 |
| Anxiety symptoms | 31 | 0.60 | 0.02 | 0.44 | 16 | 0.51 | 0.02 | 0.48 | 14 | 1.64 | 0.03 | 0.20 | 274 | 0.07 | 0.01 | 0.79 | 75 * | 10.85 | 0.08 | 0.00 | 73 * | 14.91 | 0.09 | <0.0001 |
| Symptoms related to mood and affect | 27 * | 7.12 | 0.07 | 0.01 | 9 | 0.01 | 0.00 | 0.93 | 5 | 0.62 | 0.02 | 0.43 | 201 * | 9.70 | 0.08 | 0.00 | 37 | 0.09 | 0.01 | 0.77 | 30 | 0.35 | 0.01 | 0.56 |
| Dissociation and conversion symptoms | 0 | – | – | – | 1 | 0.94 | 0.02 | 0.33 a | 1 | 1.61 | 0.03 | 0.27 a | 10 | 0.98 | 0.02 | 0.32 | 0 | – | – | – | 4 | 4.66 | 0.05 | 0.06a |
| Oppressive symptoms | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 11 | 3.82 | 0.05 | 0.05 | 1 | 0.15 | 0.01 | 0.57 a | 0 | – | – | – |
| Hallucinations and delusions | 3 | 0.44 | 0.02 | 0.36 a | 0 | – | – | – | 0 | – | – | – | – | 4.90 | 0.05 | 0.03 | 7 | 0.40 | 0.02 | 0.53 | 8 | 0.00 | 0.00 | 0.98 |
| Behavioral problems | 1 | 5.64 | 0.06 | 0.02 | 3 | 0.05 | 0.01 | 0.56 a | 0 | – | – | – | 51 | 7.06 | 0.07 | 0.01 | 11 | 0.63 | 0.02 | 0.43 | 13 | 0.02 | 0.00 | 0.90 |
| Epileptic and convulsive seizures | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 5 | 1.46 | 0.03 | 0.20a | 0 | – | – | – | 1 | 0.24 | 0.01 | 0.48 a |
| Drinking problems | 0 | – | – | – | 1 | 0.40 | 0.02 | 0.43 a | 1 | 0.83 | 0.02 | 0.35 a | 10 | 0.10 | 0.01 | 0.75 | 1 | 0.73 | 0.02 | 0.34 a | 1 | 0.58 | 0.02 | 0.38 a |
| Disturbance of consciousness | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 0 | – | – | – | 1 | 2.39 | 0.04 | 0.23 a | 0 | – | – | – |
| Symptoms unique to children | 4* | 7.25 | 0.07 | 0.03 a | 0 | – | – | – | 1 | 0.69 | 0.02 | 0.37 a | 9 | 1.02 | 0.03 | 0.31 | 2 | 0.07 | 0.01 | 0.57 a | 2 | 0.02 | 0.00 | 0.62 a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takagi, Y.; Takahashi, S.; Fukuo, Y.; Arai, T.; Tachikawa, H. Acute-Stage Mental Health Symptoms by Natural Disaster Type: Consultations of Disaster Psychiatric Assistance Teams (DPATs) in Japan. Int. J. Environ. Res. Public Health 2021, 18, 12409. https://doi.org/10.3390/ijerph182312409
Takagi Y, Takahashi S, Fukuo Y, Arai T, Tachikawa H. Acute-Stage Mental Health Symptoms by Natural Disaster Type: Consultations of Disaster Psychiatric Assistance Teams (DPATs) in Japan. International Journal of Environmental Research and Public Health. 2021; 18(23):12409. https://doi.org/10.3390/ijerph182312409
Chicago/Turabian StyleTakagi, Yoshifumi, Sho Takahashi, Yasuhisa Fukuo, Tetsuaki Arai, and Hirokazu Tachikawa. 2021. "Acute-Stage Mental Health Symptoms by Natural Disaster Type: Consultations of Disaster Psychiatric Assistance Teams (DPATs) in Japan" International Journal of Environmental Research and Public Health 18, no. 23: 12409. https://doi.org/10.3390/ijerph182312409
APA StyleTakagi, Y., Takahashi, S., Fukuo, Y., Arai, T., & Tachikawa, H. (2021). Acute-Stage Mental Health Symptoms by Natural Disaster Type: Consultations of Disaster Psychiatric Assistance Teams (DPATs) in Japan. International Journal of Environmental Research and Public Health, 18(23), 12409. https://doi.org/10.3390/ijerph182312409