
A Randomized Feasibility Trial of a Fundamental Motor Skill Parent-Mediated Intervention for Children with Autism Spectrum Disorders



Abstract
:1. Introduction
2. Materials and Methods
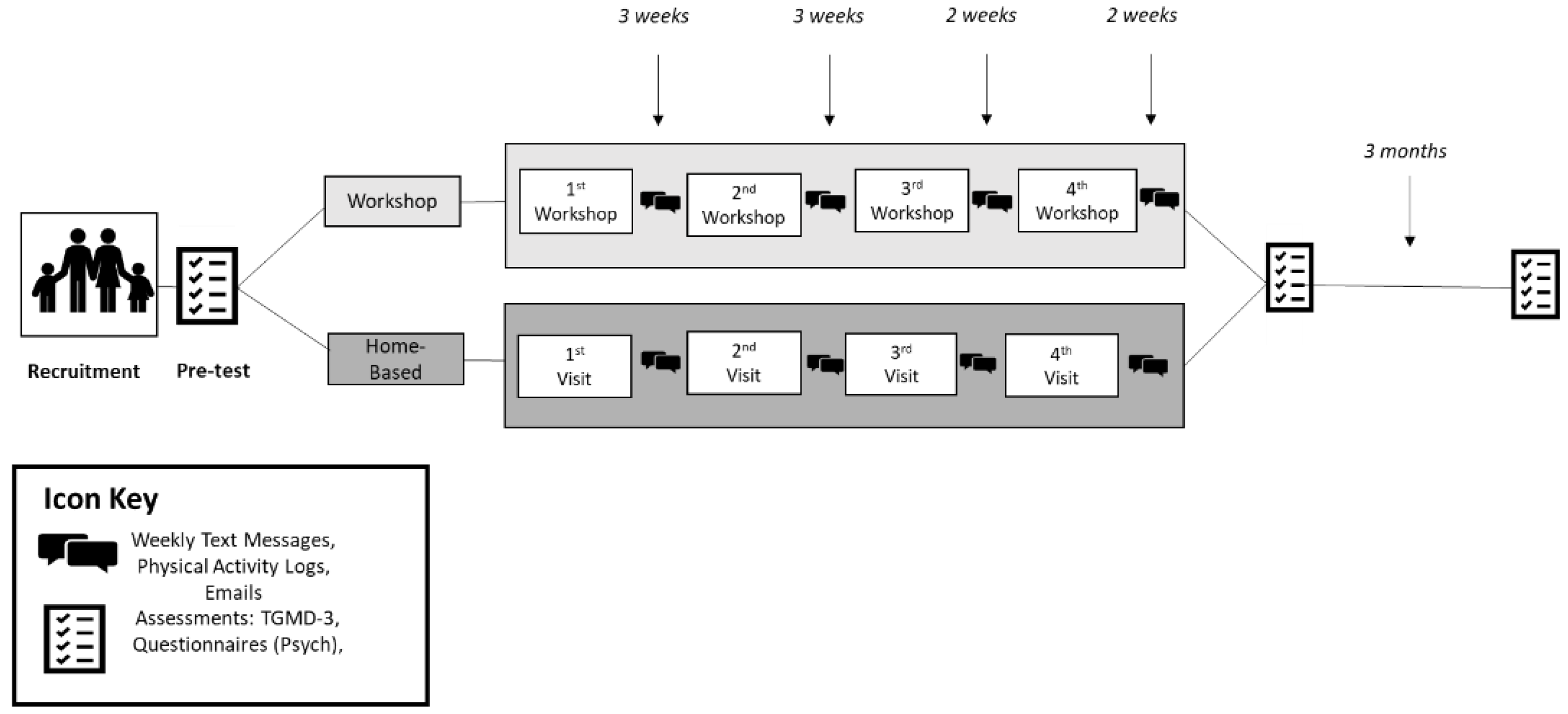
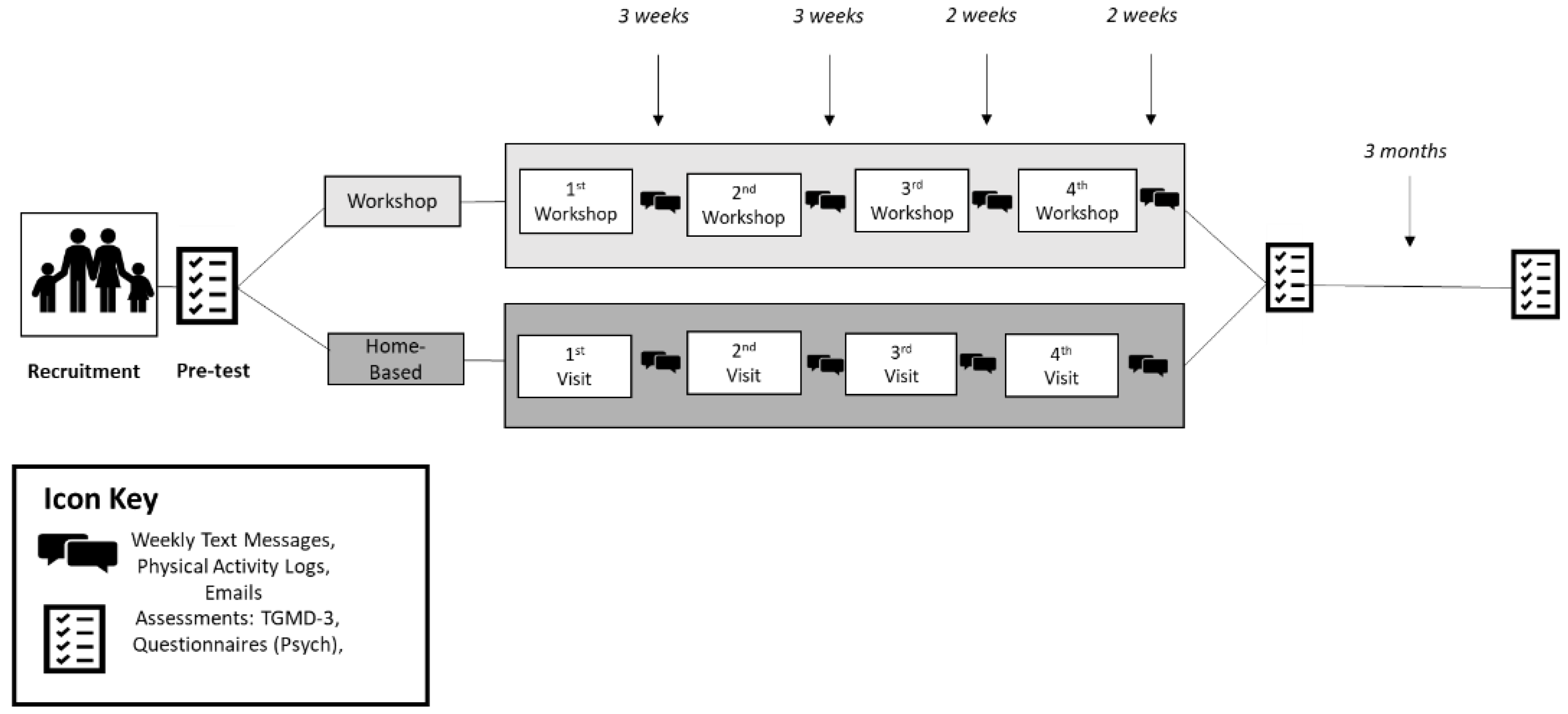
2.1. Trial Design
2.2. Participants
2.3. Intervention Description: Fit Families Program
2.4. Home-Based Group
2.5. Workshop Group
2.6. Trial Feasibility
2.7. Recruitment and Retention
2.8. Practicality of Group Division
2.9. Fundamental Motor Skills Data Collection
2.10. Intervention Feasibility
2.11. Attendance and Adherence
2.12. Acceptability
2.13. Statistical Methods
3. Results
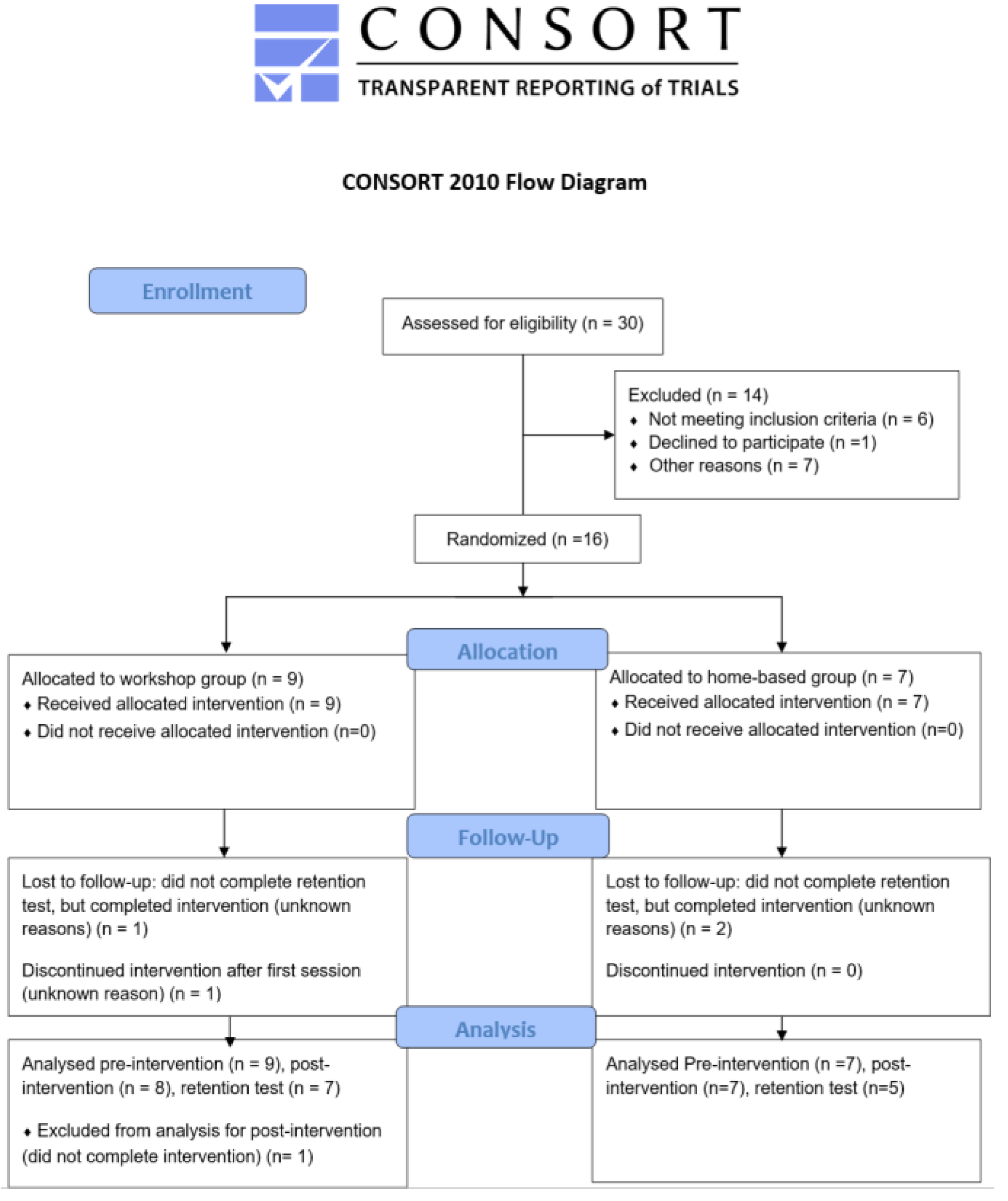
Recruitment and Retention
- Practicality of Group Division
- Intervention Attendance, Safety, and Adherence
- Intervention Acceptability
- 1.
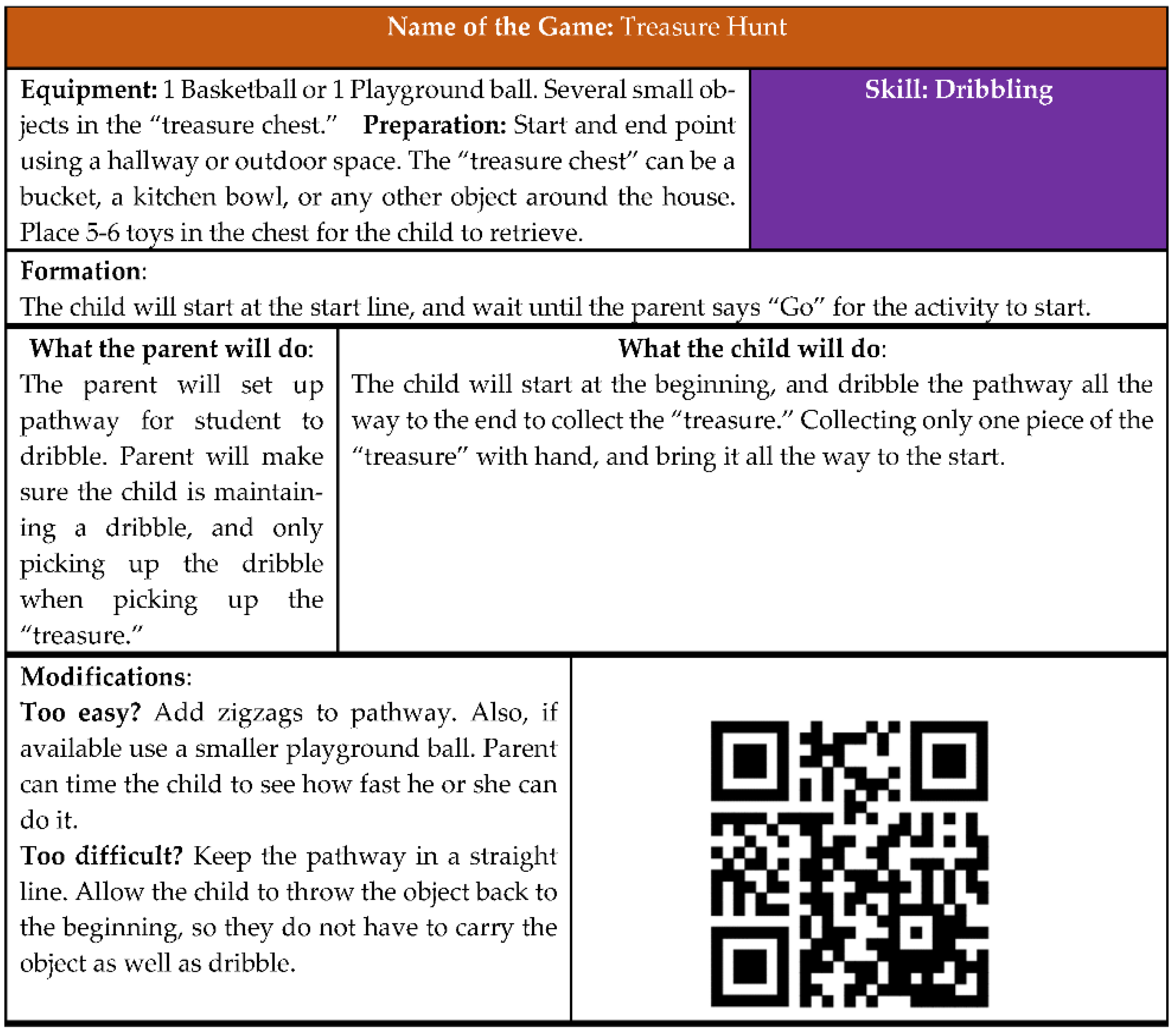
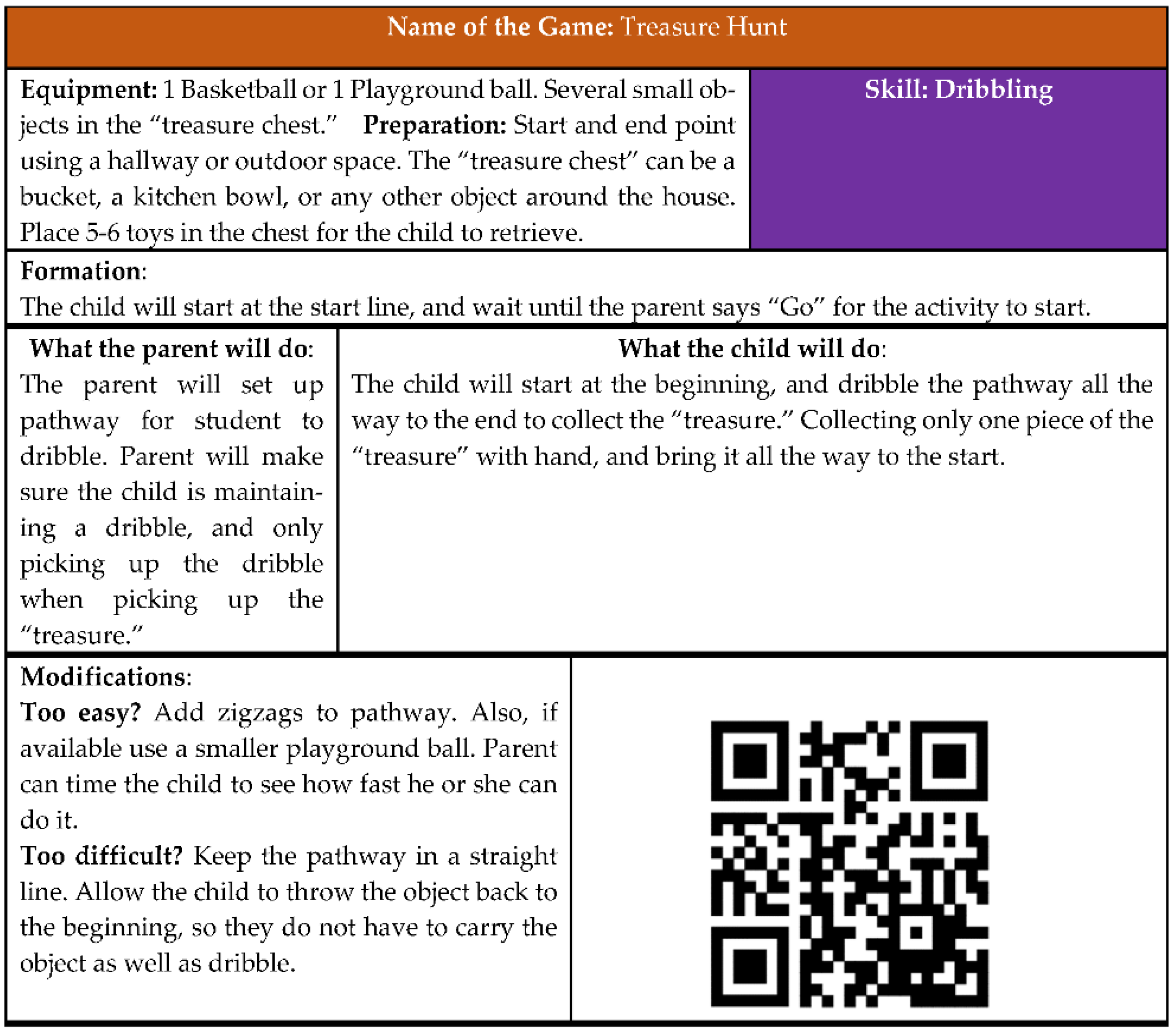
- Activity Booklet
- 2.
- Adapted Physical Education Equipment
- 3.
- Quality of Workshops
- 4.
- Text Message Acceptability
- Fundamental Motor Skills Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Staples, K.L.; Reid, G. Fundamental movement skills and autism spectrum disorders. J. Autism Dev. Disord. 2010, 40, 209–217. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, M.; Lord, C.; Ulrich, D.A. Motor skills and calibrated autism severity in young children with autism spectrum disorder. Adapt. Phys. Act. Q. 2014, 31, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.E.; Metcalfe, J.S. The mountain of motor development: A metaphor. Mot. Dev. Res. Rev. 2002, 2, 183–202. [Google Scholar]
- Colombo-Dougovito, A.M.; Block, M.E. Fundamental motor skill interventions for children and adolescents on the autism spectrum: A literature review. Rev. J. Autism Dev. Disord. 2019, 6, 159–171. [Google Scholar] [CrossRef]
- Haibach-Beach, P.S.; Reid, G.D.; Collier, D.H. Motor Learning and Development, 2nd ed.; Human Kinetics: Champaign, IL, USA, 2018. [Google Scholar]
- Berkeley, S.L.; Zittel, L.L.; Pitney, L.V.; Nichols, S.E. Locomotor and object control skills of children diagnosed with autism. Adapt. Phys. Act. Q. 2001, 18, 405–416. [Google Scholar] [CrossRef]
- Payne, G.; Issacs, L.D. Human Motor Development: A Lifespan Approach, 9th ed.; Mayfield: Mountain View, CA, USA, 2016. [Google Scholar]
- Bremer, E.; Balogh, R.; Lloyd, M. Effectiveness of a fundamental motor skill intervention for 4-year-old children with autism spectrum disorder: A pilot study. Autism 2015, 19, 980–991. [Google Scholar] [CrossRef]
- Bremer, E.; Lloyd, M. School-based fundamental-motor-skill intervention for children with autism-like characteristics: An exploratory study. Adapt. Phys. Act. Q. 2016, 33, 66–88. [Google Scholar] [CrossRef]
- Ketcheson, L.; Hauck, J.; Ulrich, D. The effects of an early motor skill intervention on motor skills, levels of physical activity, and socialization in young children with autism spectrum disorder: A pilot study. Autism 2017, 21, 481–492. [Google Scholar] [CrossRef]
- Elliott, L.K.; Weiss, J.A.; Lloyd, M. Beyond the motor domain: Exploring the secondary effects of a fundamental motor skill intervention for children with autism spectrum disorder. Adapt. Phys. Act. Q. 2021, 38, 195–214. [Google Scholar] [CrossRef]
- Kirby, A.V. Parent expectations mediate outcomes for young adults with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 1643–1655. [Google Scholar] [CrossRef]
- Hurley, K.S.; Burt, T.L. Development of physical competence through motor skill acquisition for children and youth with disabilities: Parental perceptions. Health Psychol. Rep. 2015, 3, 1–12. [Google Scholar] [CrossRef]
- Must, A.; Phillips, S.; Curtin, C.; Bandini, L.G. Barriers to physical activity in children with autism spectrum disorders: Relationship to physical activity and screen time. J. Phys. Act. Health 2015, 12, 529–534. [Google Scholar] [CrossRef] [Green Version]
- Chaapel, H.; Columna, L.; Lytle, R.; Bailey, J. Parental expectations about adapted physical education services. J. Spec. Educ. 2013, 47, 186–196. [Google Scholar] [CrossRef]
- Altunsöz, I.H.; Goodway, J.D. Skiping to motor competence: The influence of project successful kinesthetic instruction for preschoolers on motor competence of disadvantaged preschoolers. Phys. Educ. Sport Pedagog. 2016, 21, 366–385. [Google Scholar] [CrossRef]
- Hamilton, M.; Goodway, J.; Haubenstricker, J. Parent-assisted instruction in a motor skill program for at-risk preschool children. Adapt. Phys. Act. Q. 1999, 16, 415–426. [Google Scholar] [CrossRef]
- Healy, S.; Marchand, G. The feasibility of Project CHASE: A facebook-delivered, parent-mediated physical activity intervention for children with autism. Int. J. Disabil. Dev. Educ. 2020, 67, 225–242. [Google Scholar] [CrossRef]
- Cohen, L.; Manion, L.; Morrison, K. Research Methods in Education, 7th ed.; Routledge: New York, NY, USA, 2011. [Google Scholar]
- Rutter, M.; Bailey, A.; Lord, C. The Social Communication Questionnaire: Manual; Western Psychological Services: Torrance, CA, USA, 2003. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Rizzo, T.L.; Columna, L. Theory of planned behavior. In Routledge Handbook of Adapted Physical Education; Haegele, J.A., Hodge, S.R., Shapiro, D.R., Eds.; Routledge: London, UK, 2020; pp. 326–346. [Google Scholar]
- Lepore, M.; Columna, L.; Lizner, L.F. Assessments and Activities for Teaching Swimming; Human Kinetics: Champaign, IL, USA, 2015. [Google Scholar]
- Manohar, H.; Kandasamy, P.; Chandrasekaran, V.; Rajkumar, R.P. Brief parent-mediated intervention for children with autism spectrum disorder: A feasibility study from South India. J. Autism Dev. Disord. 2019, 49, 3146–3158. [Google Scholar] [CrossRef]
- Matheson, B.E.; Drahota, A.; Boutelle, K.N. A pilot study investigating the feasibility and acceptability of a parent-only behavioral weight-loss treatment for children with autism spectrum disorder. J. Autism Dev. Disord. 2019, 49, 4488–4497. [Google Scholar] [CrossRef] [PubMed]
- Seefeldt, V. Developmental motor patterns: Implications for elementary school physical education. Psychol. Mot. Behav. Sport 1980, 36, 314–323. [Google Scholar]
- Ulrich, D. Test of Gross Motor Development—3rd Edition (TGMD-3); University of Michigan: Ann Arbor, MI, USA, 2016. [Google Scholar]
- Case, L.; Yun, J. Video modeling and test of gross motor development-3 performance among children with autism spectrum disorder. Eur. J. Adapt. Phys. Act. 2018, 11, 1–10. [Google Scholar] [CrossRef]
- Marchand, G.; Healy, S. Implementation of project CHASE (children with autism supported to exercise): A facebook-delivered, parent-mediated physical activity intervention. Palaestra 2019, 33, 32–39. [Google Scholar]
- Breslin, C.M.; Rudisill, M.E. The effect of visual supports on performance of the TGMD-2 for children with autism spectrum disorder. Adapt. Phys. Act. Q. 2011, 28, 342–353. [Google Scholar] [CrossRef]
- MacDonald, R.; Dickson, C.A.; Martineau, M.; Ahearn, W.H. Prerequisite skills that support learning through video modeling. Educ. Treat. Child. 2015, 38, 33–47. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Group 1 (Workshop) N = 8 | Group 2 (Home-Based) N = 7 | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Age (years) | 7.25 ± 3.01 | 7.64 ± 2.56 |
| SCQ-C | 15.56 ± 4.80 | 13.29 ± 3.64 |
| SCQ-L | 21.11 ± 5.73 | 18.57 ± 6.13 |
| ABAS | 77.60 ± 15.33 | 84.5 ± 14.00 |
| GAC | 77.60 ± 15.33 | 84.5 ± 14.00 |
| Conceptual | 78.43 ± 15.90 | 86.67 ± 15.50 |
| Social | 79.14 ± 12.30 | 82.83 ± 10.90 |
| Practical | 80.00 ± 16.60 | 87.70 ± 14.10 |
| Activity Log (minutes) | 138 ± 60 | 99 ± 34 |
| TGMD 3 (GMQ) | ||
| Pre-test | 70.38 ± 17.10 | 75.86 ± 13.26 |
| Post-test | 74.50 ± 11.64 | 85.29 ± 12.54 |
| Retention Test | 71.14 ± 16.30 * | 86.40 ± 12.10 ** |
| Topic | Duration | Topic Description | Equipment Received | Skills Practiced |
|---|---|---|---|---|
| Sensorimotor | 3 weeks | To learn about activities that address sensory issues associated with ASD | Spooner board Soccer Balls Basketballs (playground balls) | Kick Slide Dribble Balance |
| Communication | 3 weeks | To learn strategies on how physical activity can be an opportunity to promote communication | Blue Disk Gator Balls Tennis Balls Hula Hoop Rackets Balloons | Underhand throw Overhand throw Catch One-hand strike Fitness: Strength and Flexibility |
| Aquatic | 2 weeks | To learn about water safety, basic aquatic skills, and have opportunities to engage in locomotor skills at home | Aquatic Book Pool noodles Goggles Kickboards Submergible toys | Aquatic Related Skills Skip Gallop Run |
| Physical Activity/ Sport | 2 weeks | To learn about strategies to promote physical activity and sport for their children at home and in the community | Stomp Rocket Slow-motion sand ball Batt with ball | Horizontal Jump Leap Hop Two-hand Strike |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Columna, L.; Prieto, L.A.; Beach, P.; Russo, N.; Foley, J.T. A Randomized Feasibility Trial of a Fundamental Motor Skill Parent-Mediated Intervention for Children with Autism Spectrum Disorders. Int. J. Environ. Res. Public Health 2021, 18, 12398. https://doi.org/10.3390/ijerph182312398
Columna L, Prieto LA, Beach P, Russo N, Foley JT. A Randomized Feasibility Trial of a Fundamental Motor Skill Parent-Mediated Intervention for Children with Autism Spectrum Disorders. International Journal of Environmental Research and Public Health. 2021; 18(23):12398. https://doi.org/10.3390/ijerph182312398
Chicago/Turabian StyleColumna, Luis, Laura A. Prieto, Pamela Beach, Natalie Russo, and John T. Foley. 2021. "A Randomized Feasibility Trial of a Fundamental Motor Skill Parent-Mediated Intervention for Children with Autism Spectrum Disorders" International Journal of Environmental Research and Public Health 18, no. 23: 12398. https://doi.org/10.3390/ijerph182312398
APA StyleColumna, L., Prieto, L. A., Beach, P., Russo, N., & Foley, J. T. (2021). A Randomized Feasibility Trial of a Fundamental Motor Skill Parent-Mediated Intervention for Children with Autism Spectrum Disorders. International Journal of Environmental Research and Public Health, 18(23), 12398. https://doi.org/10.3390/ijerph182312398