
Applying Latent Profile Analysis to Identify Lifestyle Profiles and Their Association with Loneliness and Quality of Life among Community-Dwelling Middle- and Older-Aged Adults in South Korea

 ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Lifestyle Factors
2.2.2. Quality of Life
2.2.3. Loneliness
2.3. Data Analysis
3. Results
3.1. Characteristics of the Study Population
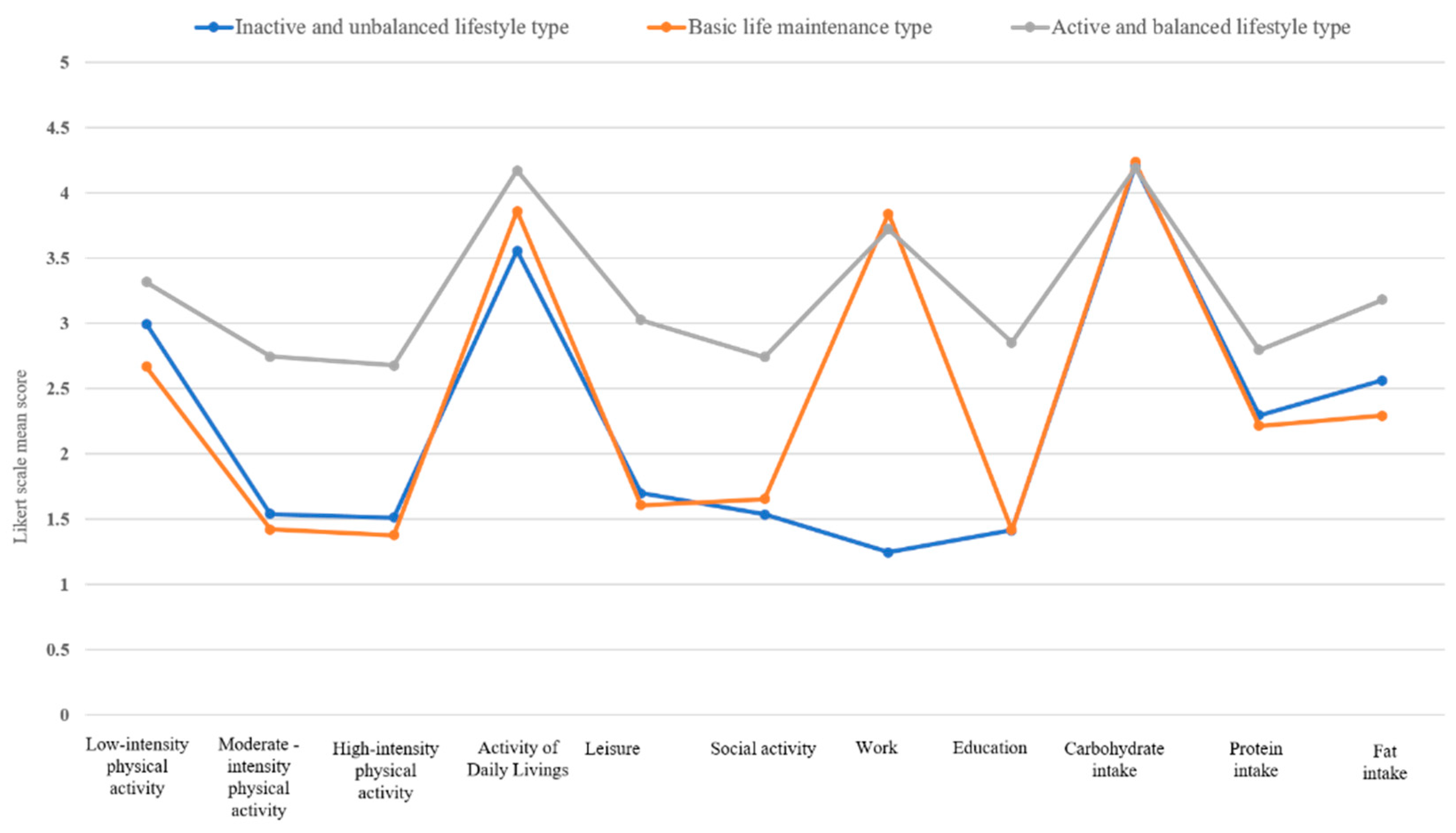
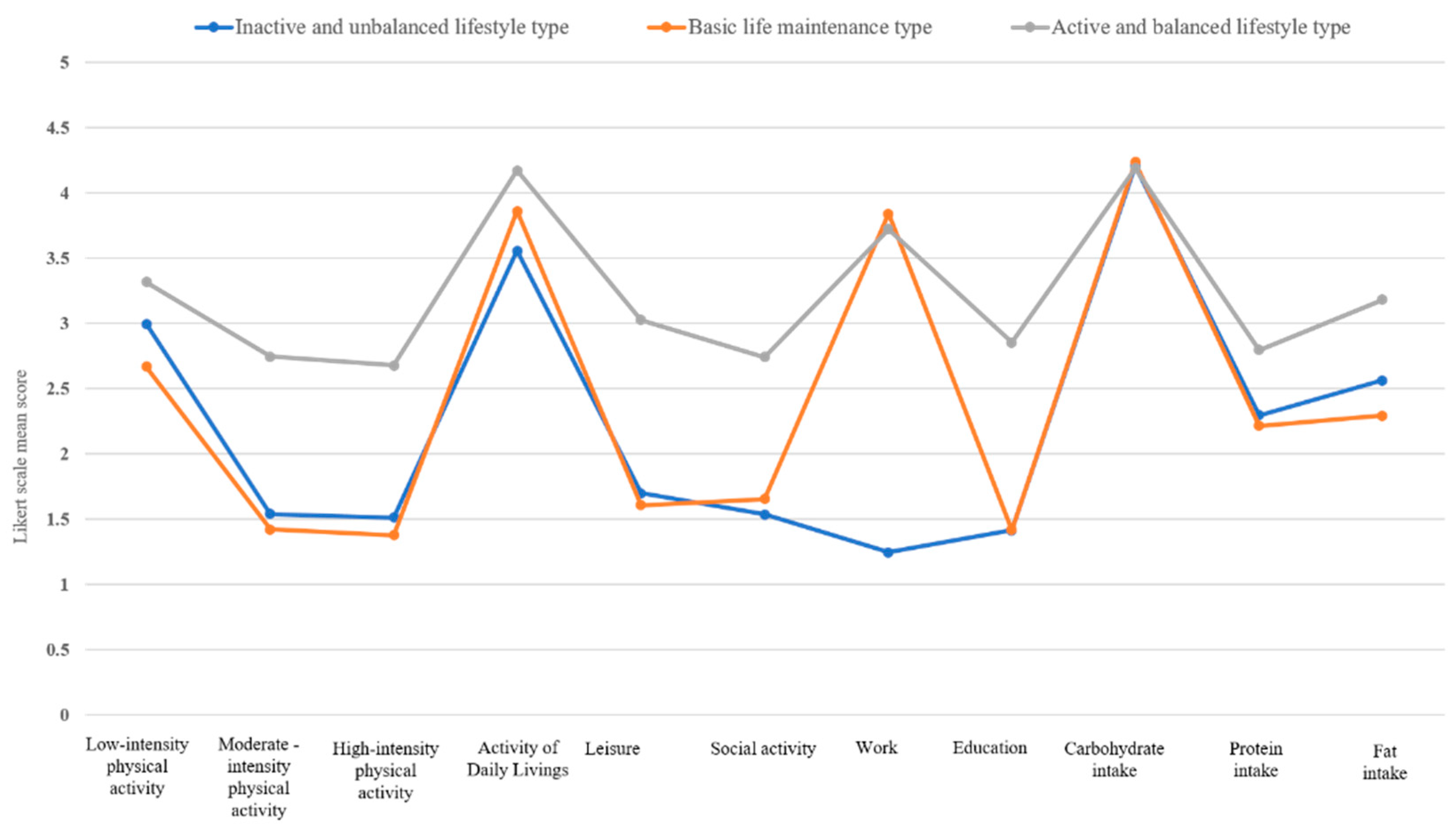
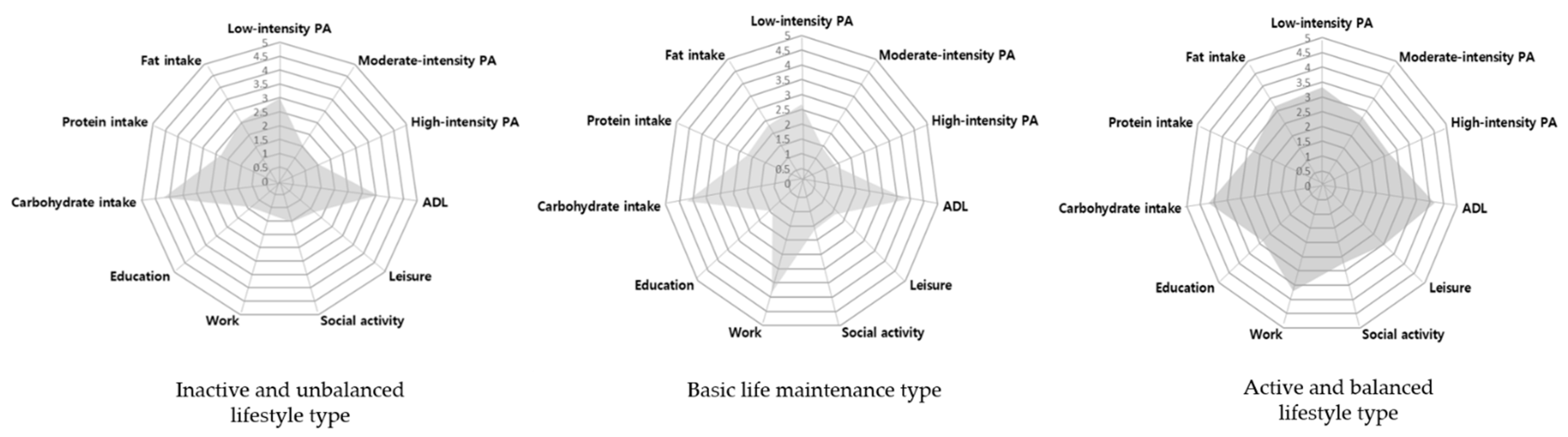
3.2. Lifestyle Profile Models by Latent Profile Analysis
3.3. Characteristics of the Identified Lifestyle Profiles
3.4. Association between Lifestyle Profiles and Quality of Life and Mental Health
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ministério da Saúde Brasília-DF. Plano de Ações Estratégicas Para o Enfrentamento das Doenças Crônicas não Transmissíveis (Dcnt) No Brasil 2011–2022; Ministério da Saúde: Brasília, Brazil, 2011. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf (accessed on 10 May 2014).
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf (accessed on 14 May 2016).
- Bauman, A.E. Updating the Evidence that Physical Activity is Good for Health: An Epidemiological Review 2000–2003. J. Sci. Med. Sport. 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Thorp, A.A.; Healy, G.N. Prolonged Sitting: Is It a Distinct Coronary Heart Disease Risk Factor? Curr. Opin. Cardiol. 2011, 26, 412–419. [Google Scholar] [CrossRef]
- Kurth, T.; Moore, S.; Gaziano, M.; Kase, C.; Stampfer, M.J.; Berger, K.; Buring, J.E. Healthy lifestyle and the risk of stroke in women. Arch. Intern. Med. 2006, 166, 1403–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Dam, R.M.; Li, T.; Spiegelman, D.; Franco, O.H.; Hu, F.B. Combined Impact of Lifestyle Factors on Mortality: Prospective Cohort Study in US Women. BMJ 2008, 337, 742–745. [Google Scholar]
- Anstey, K.J.; Bahar-Fuchs, A.; Herath, P.; Kim, S.; Burns, R.; Rebok, G.W.; Cherbuin, N. Body Brain Life: A Randomized Controlled Trial of an Online Dementia Risk Reduction Intervention in Middle-aged Adults at Risk of Alzheimer’s Disease. Alzheimer’s Dement. 2015, 1, 72–80. [Google Scholar] [CrossRef] [Green Version]
- McMaster, M.; Kim, S.; Clare, L.; Torres, S.J.; Cherbuin, N.; D’Este, C.; Anstey, K.J. Lifestyle Risk Factors and Cognitive Outcomes from the Multidomain Dementia Risk Reduction Randomized Controlled Trial, Body Brain Life for Cognitive Decline (BBL-CD). J. Am. Geriatr. Soc. 2020, 68, 2629–2637. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 Year Multidomain Intervention of Diet, Exercise, Cognitive Training, and Vascular Risk Monitoring versus Control to Prevent Cognitive Decline in At-Risk Elderly People (FINGER): A Randomised Controlled Trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Nho, J.; Yoo, S. Relationships among Lifestyle, Depression, Anxiety, and Reproductive Health in Female University Students. Korean J. Women Health Nurs. 2018, 24, 80–89. [Google Scholar] [CrossRef]
- Statistics Korea. Population Projections for Korea: 2017–2067; Statistics Korea: Seoul, Korea, 2019.
- Pan, W.C.; Ma, Q.; Sun, H.P.; Xu, Y.; Luo, N.; Wang, P. Tea Consumption and Health-Related Quality of Life in Older Adults. J. Nutr. Health Aging 2017, 21, 480–486. [Google Scholar] [CrossRef]
- World Health Organization. Active Ageing: A Policy Framework; World Health Organization: Geneva, Switzerland, 2002. Available online: www.who.int/hpr/ageing/ActiveAgeingPolicyFrame.pdf (accessed on 5 June 2016).
- The State Council Information Office, China. The Development of China’s Undertakings for the Aged. The State Council Information Office: Beijing, China, 2006. Available online: http://www.china.org.cn/english/China/191990.htm (accessed on 12 December 2006).
- Heroux, M.; Janssen, I.; Lee, D.C.; Sui, X.; Hebert, J.R.; Blair, S.N. Clustering of Unhealthy Behaviors in the Aerobics Center Longitudinal Study. Prev. Sci. 2011, 13, 183–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laaksonen, M.; Prattala, R.; Karisto, A. Patterns of Unhealthy Behaviour in Finland. Eur. J. Public Health 2001, 11, 294–300. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Morrison, J.A.; Wiecha, J.; Horton, M.; Hayman, L.L. Healthy Lifestyle Factors Associated with Reduced Cardio Metabolic Risk. Br. J. Nutr. 2011, 105, 747–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.; Park, J. Analysis of Convergent Influence of Functional Level, Environmental Factors and Lifestyle on Health and Quality of Life among Elderly Using Structural Equation Model. J. Korea Converg. Soc. 2019, 10, 377–386. [Google Scholar]
- Park, K.H.; Park, J.H. Development of an Elderly Lifestyle Profile: A Delphi Survey of Multidisciplinary Health-Care Experts. PLoS ONE 2020, 15, e0233565. [Google Scholar] [CrossRef]
- Lee, E.; Shin, J. A Study on Lifestyle-Based Market Segmentation of the Korean Mature Consumers. J. Korean Gerontol. Nurs. 2004, 24, 1–20. [Google Scholar]
- Park, Y.S.; Kim, H. Gender Differences in Healthy Lifestyle Cluster and Their Relationship with Depressive Symptoms among Middle-Aged and Older Adults in Korea. Korean J. Health Edu. Promot. 2016, 33, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Todd, M.; Adams, M.A.; Kurka, J.; Conway, T.L.; Cain, K.L.; Buman, M.P.; Frank, L.D.; Sallis, J.F.; King, A.C. Gis-Measured Walkability, Transit, and Recreation Environments in Relation to Older Adults’ Physical Activity: A Latent Profile Analysis. Prev. Med. 2016, 93, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Berlin, K.S.; Williams, N.A.; Parra, G.R. An Introduction to Latent Variable Mixture Modeling (Part 1): Overview and Cross-Sectional Latent Class and Latent Profile Analyses. J. Pediatr. Psychol. 2014, 39, 174–187. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Han, D.; Park, J. The Yonsei Lifestyle Profile (YLP) for adults and the older adults: Development and test-retest reliability. In Proceedings of the 2020 The Korean Gerontological Society Annual Conference, Seoul, Korea, 27 November 2020. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Williams & Wilkins: New York, NY, USA, 2014. [Google Scholar]
- Group WHOQOL. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF Quality of Life Assessment: Psychometric Properties and Results of the International Field Trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Min, S.K.; Kim, K.I.; Lee, C.I.; Jung, Y.C.; Suh, S.Y.; Kim, D.K. Development of the Korean Versions of WHO Quality of Life Scale and WHOQOL-Bref. Qual. Life Res. 2002, 11, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E. Development of the Korean Geriatric Loneliness Scale (KGLS). J. Korean Acad. Nurs. 2019, 49, 643–654. [Google Scholar] [CrossRef] [PubMed]
- Södergren, M.; Wang, W.C.; Salmon, J.; Ball, K.; Crawford, D.; McNaughton, S.A. Predicting Healthy Lifestyle Patterns among Retirement Age Older Adults in the Well Study: A Latent Class Analysis of Sex Differences. Maturitas 2014, 77, 41–46. [Google Scholar] [CrossRef]
- Vajdi, M.; Nikniaz, L.; Pour Asl, A.M.; Abbasalizad Farhangi, M. Lifestyle Patterns and Their Nutritional, Socio-Demographic and Psychological Determinants in a Community-Based Study: A Mixed Approach of Latent Class and Factor Analyses. PLoS ONE 2020, 15, e0236242. [Google Scholar] [CrossRef]
- Park, K.; Won, K.; Park, J. A Systematic Study on the Multifaceted Lifestyle Assessment Tools for Community-Dwelling Elderly: Trend and Application Prospect. Thera. Sci. Neurorehab. 2019, 8, 7–29. [Google Scholar] [CrossRef]
- Ferreira, L.K.; Meireles, J.F.F.; Ferreira, M.E.C. Evaluation of Lifestyle and Quality of Life in the Elderly: A Literature Review. Rev. Bras. Geriatr. Gerontol. 2018, 21, 616–627. [Google Scholar] [CrossRef]
- Footit, J.; Anderson, D. Associations between Perception of Wellness and Health-Related Quality of Life, Comorbidities, Modifiable Lifestyle Factors and Demographics in Older Australians. Australas. J. Ageing 2012, 31, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Denton, M.; Walters, V. Gender Differences in Structural and Behavioral Determinants of Health: An Analysis of the Social Production of Health. Soc. Sci. Med. 1999, 48, 1221–1235. [Google Scholar] [CrossRef]
- Uitenbroek, D.G.; Kerekovska, A.; Festchieva, N. Health Lifestyle Behaviour and Socio-Demographic Characteristics. A Study of Varna, Glasgow and Edinburgh. Soc. Sci. Med. 1996, 43, 367–377. [Google Scholar] [CrossRef]
- Vari, R.; Scazzocchio, B.; D’Amore, A.; Giovannini, C.; Gessani, S.; Masella, R. Gender-Related Differences in Lifestyle May Affect Health Status. Ann. Ist. Super. Sanita 2016, 52, 158–166. [Google Scholar]
- Syed-Abdul, M.M.; McClellan, C.L.; Parks, E.J.; Ball, S.D. Effects of a Resistance Training Community Programme in Older Adults. Ageing Soc. 2021, 23, 1–16. [Google Scholar] [CrossRef]
- Reid, K.J.; Baron, K.G.; Lu, B.; Naylor, E.; Wolfe, L.; Zee, P.C. Aerobic Exercise Improves Self-Reported Sleep and Quality of Life in Older Adults with Insomnia. Sleep Med. 2010, 11, 934–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, B.S.; Syed-Abdul, M.M.; Weitzel, K.J.; Ball, S.D. Acute Resistance Training May Have Lasting Benefit to Middle-Aged Adults. Gerontol. Geriatr. Med. 2021, 7, 23337214211022592. [Google Scholar] [CrossRef]
- Syed-Abdul, M.M. Benefits of Resistance Training in Older Adults. Curr. Aging Sci. 2021, 14, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kim, C.; Park, Y.S. The Effect of Nutrition Education Program in Physical Health, Nutritional Status and Health-Related Quality of Life of the Elderly in Seoul. J. Nutr. Health 2007, 40, 270–280. [Google Scholar]
- Hawkley, L.C.; Burleson, M.H.; Berntson, G.G.; Cacioppo, J.T. Loneliness in Everyday Life: Cardiovascular Activity, Psychosocial Context, and Health Behaviors. J. Pers. Soc. Psychol. 2003, 85, 105. [Google Scholar] [CrossRef] [PubMed]
- Richard, A.; Rohrmann, S.; Vandeleur, C.L.; Schmid, M.; Barth, J.; Eichholzer, M. Loneliness Is Adversely Associated with Physical and Mental Health and Lifestyle Factors: Results from a Swiss National Survey. PLoS ONE 2017, 12, e0181442. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | N | (%) | |
|---|---|---|---|
| Sex | Male | 287 | 50.4 |
| Female | 282 | 49.6 | |
| Age (Mean ± SD: 60.2 ± 4.3) | 55–64 | 482 | 84.7 |
| 65–74 | 85 | 14.9 | |
| >75 | 2 | 0.4 | |
| Educational attainment | Elementary school | 4 | 0.7 |
| Middle school | 9 | 1.6 | |
| High school | 161 | 28.3 | |
| College or university | 395 | 69.4 | |
| Residential area | Metropolitan | 304 | 53.4 |
| Provincial big city | 116 | 20.4 | |
| Small and medium-sized cities | 139 | 24.4 | |
| Countryside | 10 | 1.8 | |
| Regular medication intake | Yes | 291 | 51.1 |
| No | 278 | 48.9 |
| No. of Profiles | AIC | BIC | SS-ABIC | LMR-LRT | Entropy | Latent Profile Proportions (%) | |||
|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||||||
| 2 | 16,869.422 | 17,017.114 | 16,909.179 | 503.666 *** | 0.904 | 87.170 | 12.830 | ||
| 3 | 16,552.489 | 16,758.307 | 16,606.278 | 336.512 *** | 0.956 | 36.380 | 54.482 | 9.139 | |
| 4 | 16,404.205 | 16,656.150 | 16,472.026 | 170.050 | 0.940 | 30.053 | 8.436 | 54.657 | 6.854 |
| Variables | Latent Profile (N (%)) | χ2 | |||
|---|---|---|---|---|---|
| Profile 1 | Profile 2 | Profile 3 | |||
| Sex | Male | 76 (36.7) | 190 (61.3) | 21 (40.4) | 32.302 *** |
| Female | 131 (63.3) | 120 (38.7) | 31 (59.6) | ||
| Age | 55–64 | 150 (72.5) | 287 (92.6) | 45 (86.5) | 40.006 *** |
| 65–74 | 55 (26.5) | 23 (7.4) | 7 (13.5) | ||
| >75 | 2 (1.0) | - | - | ||
| Educational attainment | Elementary school | 2 (1.0) | 2 (0.6) | - | 6.593 |
| Middle school | 3 (1.4) | 5 (1.6) | 1 (1.9) | ||
| High school | 67 (32.4) | 77 (24.8) | 17 (32.7) | ||
| College or university | 134 (64.7) | 226 (72.9) | 34 (65.4) | ||
| No response | 1 (0.5) | - | - | ||
| Residential area | Metropolitan | 103 (49.8) | 177 (57.1) | 24 (46.2) | 11.501 |
| Provincial big city | 53 (25.6) | 52 (16.8) | 11 (21.2) | ||
| Medium-sized city | 45 (21.7) | 77 (24.8) | 17 (32.7) | ||
| Countryside | 6 (2.9) | 4 (1.3) | - | ||
| Regular medication intake | Yes | 122 (58.9) | 141 (45.5) | 28 (53.8) | 9.158 ** |
| No | 85 (41.1) | 169 (54.5) | 24 (46.2) | ||
| Variables | Latent Profile (M (SD)) | F | ||
|---|---|---|---|---|
| Profile 1 | Profile 2 | Profile 3 | ||
| Loneliness (KGLS) | 35.63 (3.83) | 35.53 (3.68) | 37.54 (4.94) | 6.14 ** |
| Quality of life (WHOQOL) | 82.17 (16.05) | 83.00 (15.78) | 92.50 (16.20) | 9.17 *** |
| Variables | B | SE | OR | 96% CI | |
|---|---|---|---|---|---|
| Profile 3 vs. | |||||
| Profile 1 | Sex | −0.155 | 0.317 | 0.856 | 0.460–1.595 |
| Age | 0.092 * | 0.038 | 1.096 | 1.017–1.180 | |
| Educational attainment | −0.035 | 0.271 | 0.966 | 0.568–1.644 | |
| Residential area | −0.106 | 0.170 | 0.899 | 0.645–1.254 | |
| Regular medication intake | 0.207 | 0.312 | 1.230 | 0.667–2.268 | |
| Loneliness (KGLS) | −0.073 ** | 0.026 | 0.929 | 0.883–0.978 | |
| Quality of life (WHOQOL) | −0.043 *** | 0.011 | 0.957 | 0.938–0.978 | |
| Profile 2 | Sex | 0.849 ** | 0.306 | 2.337 | 1.284–4.256 |
| Age | −0.074 | 0.038 | 0.929 | 0.862–1.002 | |
| Educational level | 0.221 | 0.267 | 1.247 | 0.739–2.105 | |
| Residential area | −0.202 | 0.165 | 0.817 | 0.592–1.128 | |
| Regular medication intake | −0.335 | 0.301 | 0.715 | 0.397–1.289 | |
| Loneliness (KGLS) | −0.064 * | 0.025 | 0.938 | 0.892–0.985 | |
| Quality of life (WHOQOL) | −0.040 *** | 0.010 | 0.961 | 0.941–0.980 | |
| Profile 2 vs. | |||||
| Profile 1 | Sex | −1.004 *** | 0.185 | 0.366 | 0.255–0.527 |
| Age | 0.165 *** | 0.024 | 1.180 | 1.126–1.236 | |
| Educational level | −0.255 | 0.163 | 0.775 | 0.562–1.067 | |
| Residential area | 0.096 | 0.101 | 1.100 | 0.902–1.342 | |
| Regular medication intake | 0.543 ** | 0.182 | 1.720 | 1.205–2.456 | |
| Loneliness (KGLS) | −0.009 | 0.014 | 0.991 | 0.964–1.019 | |
| Quality of life (WHOQOL) | −0.003 | 0.006 | 0.997 | 0.986–1.008 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.-H.; Yoo, E.-Y.; Kim, J.; Hong, I.; Lee, J.-S.; Park, J.-H. Applying Latent Profile Analysis to Identify Lifestyle Profiles and Their Association with Loneliness and Quality of Life among Community-Dwelling Middle- and Older-Aged Adults in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 12374. https://doi.org/10.3390/ijerph182312374
Park K-H, Yoo E-Y, Kim J, Hong I, Lee J-S, Park J-H. Applying Latent Profile Analysis to Identify Lifestyle Profiles and Their Association with Loneliness and Quality of Life among Community-Dwelling Middle- and Older-Aged Adults in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(23):12374. https://doi.org/10.3390/ijerph182312374
Chicago/Turabian StylePark, Kang-Hyun, Eun-Young Yoo, Jongbae Kim, Ickpyo Hong, Jae-Shin Lee, and Ji-Hyuk Park. 2021. "Applying Latent Profile Analysis to Identify Lifestyle Profiles and Their Association with Loneliness and Quality of Life among Community-Dwelling Middle- and Older-Aged Adults in South Korea" International Journal of Environmental Research and Public Health 18, no. 23: 12374. https://doi.org/10.3390/ijerph182312374
APA StylePark, K.-H., Yoo, E.-Y., Kim, J., Hong, I., Lee, J.-S., & Park, J.-H. (2021). Applying Latent Profile Analysis to Identify Lifestyle Profiles and Their Association with Loneliness and Quality of Life among Community-Dwelling Middle- and Older-Aged Adults in South Korea. International Journal of Environmental Research and Public Health, 18(23), 12374. https://doi.org/10.3390/ijerph182312374