

Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review

 ,
,  , and
, and 
Abstract
1. Introduction
2. Methods
3. Results
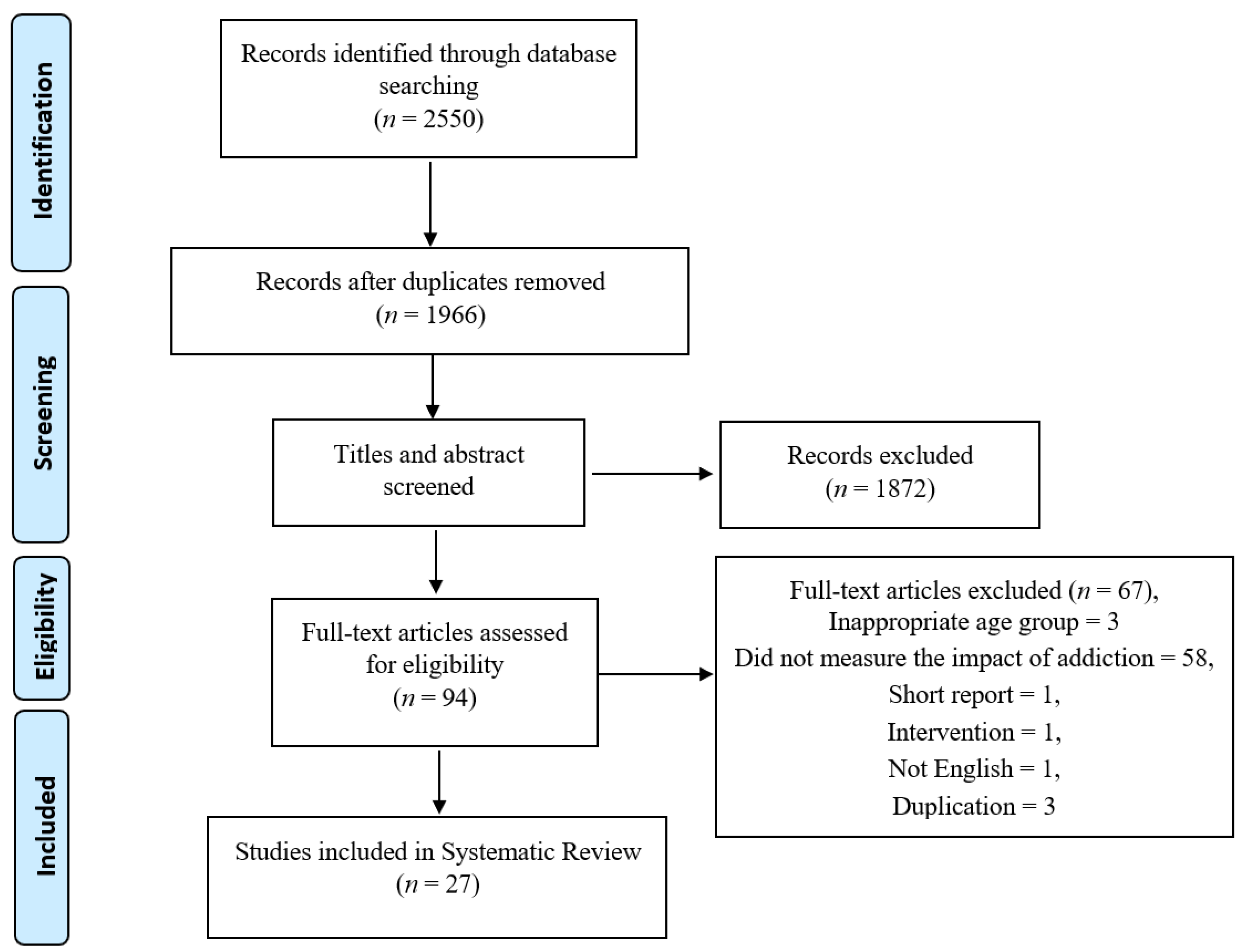
3.1. Overall Search Findings
3.2. Main Findings
3.2.1. Mental Health
3.2.2. Physical Health
Musculoskeletal Problems
Sleep Quality and Sedentary Lifestyle
Accidents
Neurological Problems
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wajcman, J. Life in the fast lane? Towards a sociology of technology and time. Br. J. Sociol. 2008, 59, 59–77. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Grant, D. Narrative, drama and charismatic leadership: The case of Apple’s Steve Jobs. Leadership 2011, 7, 3–26. [Google Scholar] [CrossRef]
- Ozdalga, E.; Ozdalga, A.; Ahuja, N. The Smartphone in Medicine: A Review of Current and Potential Use Among Physicians and Students. J. Med. Internet Res. 2012, 14, e128. [Google Scholar] [CrossRef]
- Zargaran, A.; Ash, J.; Kerry, G.; Rasasingam, D.; Gokani, S.; Mittal, A.; Zargaran, D. Ethics of Smartphone Usage for Medical Image Sharing. Indian J. Surg. 2018, 80, 300–301. [Google Scholar] [CrossRef]
- Karim, R.; Chaudhri, P. Behavioral Addictions: An Overview. J. Psychoact. Drugs 2012, 44, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.E.; Potenza, M.N.; Weinstein, A.; Gorelick, D.A. Introduction to behavioral addictions. Am. J. Drug Alcohol Abus. 2010, 36, 233–241. [Google Scholar] [CrossRef]
- Young, K.S. Internet Addiction: A New Clinical Phenomenon and Its Consequences. Am. Behav. Sci. 2004, 48, 402–415. [Google Scholar] [CrossRef]
- Kwon, M.; Lee, J.-Y.; Won, W.-Y.; Park, J.-W.; Min, J.-A.; Hahn, C.; Gu, X.; Choi, J.-H.; Kim, D.-J. Development and Validation of a Smartphone Addiction Scale (SAS). PLoS ONE 2013, 8, e56936. [Google Scholar] [CrossRef]
- Montag, C.; Wegmann, E.; Sariyska, R.; Demetrovics, Z.; Brand, M. How to overcome taxonomical problems in the study of Internet use disorders and what to do with “smartphone addiction”? J. Behav. Addict. 2021, 9, 908–914. [Google Scholar] [CrossRef]
- Watkins, S.C. The Young and The Digital: What the Migration to Social-Network Sites, Games, and Anytime, Anywhere Media Means for Our Future; Beacon Press: Boston, MA, USA, 2009. [Google Scholar]
- Vuori, T.O.; Huy, Q.N. Distributed Attention and Shared Emotions in the Innovation Process: How Nokia Lost the Smartphone Battle. Adm. Sci. Q. 2015, 61, 9–51. [Google Scholar] [CrossRef]
- Ellis, D.A. Are smartphones really that bad? Improving the psychological measurement of technology-related behaviors. Comput. Hum. Behav. 2019, 97, 60–66. [Google Scholar] [CrossRef]
- Alavi, S.S.; Ferdosi, M.; Jannatifard, F.; Eslami, M.; Alaghemandan, H.; Setare, M. Behavioral Addiction versus Substance Addiction: Correspondence of Psychiatric and Psychological Views. Int. J. Prev. Med. 2012, 3, 290–294. [Google Scholar] [PubMed]
- Van Rooij, A.J.; Prause, N. A critical review of “Internet addiction” criteria with suggestions for the future. J. Behav. Addict. 2014, 3, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.M.; Zajac, K.; Ginley, M.K. Behavioral Addictions as Mental Disorders: To Be or Not to Be? Annu. Rev. Clin. Psychol. 2018, 14, 399–423. [Google Scholar] [CrossRef]
- Al-Hadidi, F.; Bsisu, I.; Al Ryalat, S.A.; Al-Zu’Bi, B.; Bsisu, R.; Hamdan, M.; Kanaan, T.; Yasin, M.; Samarah, O. Association between mobile phone use and neck pain in university students: A cross-sectional study using numeric rating scale for evaluation of neck pain. PLoS ONE 2019, 14, e0217231. [Google Scholar] [CrossRef]
- Horvath, J.; Mundinger, C.; Schmitgen, M.M.; Wolf, N.D.; Sambataro, F.; Hirjak, D.; Kubera, K.M.; Koenig, J.; Wolf, R.C. Structural and functional correlates of smartphone addiction. Addict. Behav. 2020, 105, 106334. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Chang, L.-R.; Lee, Y.-H.; Tseng, H.-W.; Kuo, T.B.J.; Chen, S.-H. Development and Validation of the Smartphone Addiction Inventory (SPAI). PLoS ONE 2014, 9, e98312. [Google Scholar] [CrossRef]
- Panova, T.; Carbonell, X. Is smartphone addiction really an addiction? J. Behav. Addict. 2018, 7, 252–259. [Google Scholar] [CrossRef]
- NIH. Study Quality Assessment Tools. 2021. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 2 March 2021).
- Kim, H.J.; Min, J.-Y.; Kim, H.-J.; Min, K.-B. Accident risk associated with smartphone addiction: A study on university students in Korea. J. Behav. Addict. 2017, 6, 699–707. [Google Scholar] [CrossRef]
- Kim, Y.-J.; Jang, H.M.; Lee, Y.; Lee, D.; Kim, D.-J. Effects of Internet and Smartphone Addictions on Depression and Anxiety Based on Propensity Score Matching Analysis. Int. J. Environ. Res. Public Health 2018, 15, 859. [Google Scholar] [CrossRef]
- Lee, D.; Namkoong, K.; Lee, J.; Lee, B.O.; Jung, Y.-C. Lateral orbitofrontal gray matter abnormalities in subjects with problematic smartphone use. J. Behav. Addict. 2019, 8, 404–411. [Google Scholar] [CrossRef]
- Lee, J.; Seo, K. The Comparison of Cervical Repositioning Errors According to Smartphone Addiction Grades. J. Phys. Ther. Sci. 2014, 26, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Kim, S.-H.; Ha, T.-Y.; Yoo, Y.-M.; Han, J.-J.; Jung, J.-H.; Jang, J.-Y. Dependency on Smartphone Use and its Association with Anxiety in Korea. Public Health Rep. 2016, 131, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Yang, H.-S.; Jeong, C.-J.; Yoo, Y.-D.; Jeong, G.-Y.; Moon, J.-S.; Kang, M.-K.; Hong, S.-W. Changes in the Thickness of Median Nerves Due to Excessive Use of Smartphones. J. Phys. Ther. Sci. 2012, 24, 1259–1262. [Google Scholar] [CrossRef]
- Rho, M.J.; Park, J.; Na, E.; Jeong, J.-E.; Kim, J.K.; Kim, D.-J.; Choi, I.Y. Types of problematic smartphone use based on psychiatric symptoms. Psychiatry Res. 2019, 275, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Alhassan, A.A.; Alqadhib, E.M.; Taha, N.W.; Alahmari, R.A.; Salam, M.; Almutairi, A.F. The relationship between addiction to smartphone usage and depression among adults: A cross sectional study. BMC Psychiatry 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alosaimi, F.D.; Alyahya, H.; Alshahwan, H.; Al Mahyijari, N.; Shaik, S.A. Smartphone addiction among university students in Riyadh, Saudi Arabia. Saudi Med. J. 2016, 37, 675–683. [Google Scholar] [CrossRef]
- El-Sayed Desouky, D.; Abu-Zaid, H. Mobile phone use pattern and addiction in relation to depression and anxiety. East Mediterr. Health J. 2020, 26, 692–699. [Google Scholar] [CrossRef]
- Elhai, J.D.; Yang, H.; Fang, J.; Bai, X.; Hall, B. Depression and anxiety symptoms are related to problematic smartphone use severity in Chinese young adults: Fear of missing out as a mediator. Addict. Behav. 2019, 101, 105962. [Google Scholar] [CrossRef]
- Hu, Y.; Long, X.; Lyu, H.; Zhou, Y.; Chen, J. Alterations in White Matter Integrity in Young Adults with Smartphone Dependence. Front. Hum. Neurosci. 2017, 11, 532. [Google Scholar] [CrossRef]
- Elhai, J.D.; Yang, H.; McKay, D.; Asmundson, G.J. COVID-19 anxiety symptoms associated with problematic smartphone use severity in Chinese adults. J. Affect. Disord. 2020, 274, 576–582. [Google Scholar] [CrossRef]
- Zhuang, L.; Wang, L.; Xu, D.; Wang, Z.; Liang, R. Association between excessive smartphone use and cervical disc degeneration in young patients suffering from chronic neck pain. J. Orthop. Sci. 2021, 26, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Demir, Y.P.; Sümer, M.M. Effects of smartphone overuse on headache, sleep and quality of life in migraine patients. Neurosciences 2019, 24, 115–121. [Google Scholar] [CrossRef]
- Demirci, K.; Akgönül, M.; Akpinar, A. Relationship of smartphone use severity with sleep quality, depression, and anxiety in university students. J. Behav. Addict. 2015, 4, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Gokce, A.; Ozer, A. The relationship between problematic cell phone use, eating disorders and social anxiety among university students. Pak. J. Med. Sci. 2021, 37, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, B.; Acimis, N.M. Sleep Quality in Pamukkale University Students and its relationship with smartphone addiction. Pak. J. Med. Sci. 2020, 37, 206–211. [Google Scholar] [CrossRef]
- Haripriya, S.; Samuel, S.E.; Megha, M. Correlation between Smartphone Addiction, Sleep Quality and Physical Activity among Young Adults. J. Clin. Diagn. Res. 2019, 13, YC05–YC09. [Google Scholar] [CrossRef]
- Lane, H.-Y.; Chang, C.-J.; Huang, C.-L.; Chang, Y.-H. An Investigation into Smartphone Addiction with Personality and Sleep Quality among University Students. Int. J. Environ. Res. Public Health 2021, 18, 7588. [Google Scholar] [CrossRef]
- Annoni, A.; Petrocchi, S.; Camerini, A.-L.; Marciano, L. The Relationship between Social Anxiety, Smartphone Use, Dispositional Trust, and Problematic Smartphone Use: A Moderated Mediation Model. Int. J. Environ. Res. Public Health 2021, 18, 2452. [Google Scholar] [CrossRef]
- Elhai, J.D.; Rozgonjuk, D.; Yildirim, C.; Alghraibeh, A.M.; Alafnan, A.A. Worry and anger are associated with latent classes of problematic smartphone use severity among college students. J. Affect. Disord. 2019, 246, 209–216. [Google Scholar] [CrossRef]
- Megna, M.; Gisonni, P.; Napolitano, M.; Orabona, G.D.; Patruno, C.; Ayala, F.; Balato, N. The effect of smartphone addiction on hand joints in psoriatic patients: An ultrasound-based study. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 73–78. [Google Scholar] [CrossRef]
- Tangmunkongvorakul, A.; Musumari, P.M.; Thongpibul, K.; Srithanaviboonchai, K.; Techasrivichien, T.; Suguimoto, S.P.; Ono-Kihara, M.; Kihara, M. Association of excessive smartphone use with psychological well-being among university students in Chiang Mai, Thailand. PLoS ONE 2019, 14, e0210294. [Google Scholar] [CrossRef]
- Hussain, Z.; Griffiths, M.D.; Sheffield, D. An investigation into problematic smartphone use: The role of narcissism, anxiety, and personality factors. J. Behav. Addict. 2017, 6, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.; Hussain, Z.; Griffiths, M.D. Problematic smartphone use, nature connectedness, and anxiety. J. Behav. Addict. 2018, 7, 109–116. [Google Scholar] [CrossRef]
- Alageel, A.A.; Alyahya, R.A.; Bahatheq, Y.A.; Alzunaydi, N.A.; Alghamdi, R.A.; Alrahili, N.M.; McIntyre, R.S.; Iacobucci, M. Smartphone addiction and associated factors among postgraduate students in an Arabic sample: A cross-sectional study. BMC Psychiatry 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; McGeeney, K.; Duggan, M. US Smartphone Use in 2015; Report; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Ratan, Z.A.; Bin Zaman, S.; Islam, S.M.S.; Hosseinzadeh, H. Smartphone overuse: A hidden crisis in COVID-19. Health Policy Technol. 2021, 10, 21–22. [Google Scholar] [CrossRef] [PubMed]
- Billieux, J.; Maurage, P.; Lopez-Fernandez, O.; Kuss, D.J.; Griffiths, M.D. Can Disordered Mobile Phone Use Be Considered a Behavioral Addiction? An Update on Current Evidence and a Comprehensive Model for Future Research. Curr. Addict. Rep. 2015, 2, 156–162. [Google Scholar] [CrossRef]
- Wolniewicz, C.A.; Rozgonjuk, D.; Elhai, J.D. Boredom proneness and fear of missing out mediate relations between depression and anxiety with problematic smartphone use. Hum. Behav. Emerg. Technol. 2020, 2, 61–70. [Google Scholar] [CrossRef]
- Elserty, N.S.; Helmy, N.A.; Mounir, K.M. Smartphone addiction and its relation to musculoskeletal pain in Egyptian physical therapy students. Eur. J. Physiother. 2020, 22, 70–78. [Google Scholar] [CrossRef]
- Baabdullah, A.; Bokhary, D.; Kabli, Y.; Saggaf, O.; Daiwali, M.; Hamdi, A. The association between smartphone addiction and thumb/wrist pain: A cross-sectional study. Medicine 2020, 99, e19124. [Google Scholar] [CrossRef]
- Saito, K.; Saito, Y. Relationship between Information and Communication Device Usage and Development of Hand Disorders. Inq. J. Health Care Organ. Provis. Financ. 2021, 58, 00469580211029607. [Google Scholar] [CrossRef]
- Benites-Zapata, V.A.; Jiménez-Torres, V.E.; Ayala-Roldán, M.P. Problematic smartphone use is associated with de Quervain’s tenosynovitis symptomatology among young adults. Musculoskelet. Sci. Pract. 2021, 53, 102356. [Google Scholar] [CrossRef]
- Elhai, J.D.; Levine, J.C.; Dvorak, R.D.; Hall, B. Fear of missing out, need for touch, anxiety and depression are related to problematic smartphone use. Comput. Hum. Behav. 2016, 63, 509–516. [Google Scholar] [CrossRef]
- Zhang, M.X.; Wu, A.M.S. Effects of smartphone addiction on sleep quality among Chinese university students: The mediating role of self-regulation and bedtime procrastination. Addict. Behav. 2020, 111, 106552. [Google Scholar] [CrossRef] [PubMed]
- Sohn, S.Y.; Rees, P.; Wildridge, B.; Kalk, N.J.; Carter, B. Prevalence of problematic smartphone usage and associated mental health outcomes amongst children and young people: A systematic review, meta-analysis and GRADE of the evidence. BMC Psychiatry 2019, 19, 356. [Google Scholar]
- Alshobaili, F.A.; Alyousefi, N.A. The effect of smartphone usage at bedtime on sleep quality among Saudi non- medical staff at King Saud University Medical City. J. Fam. Med. Prim. Care 2019, 8, 1953–1957. [Google Scholar] [CrossRef]
- Li, L.; Griffiths, M.D.; Mei, S.; Niu, Z. Fear of Missing Out and Smartphone Addiction Mediates the Relationship Between Positive and Negative Affect and Sleep Quality Among Chinese University Students. Front. Psychiatry 2020, 11, 877. [Google Scholar] [CrossRef]
- Zhang, M.X.; Zhou, H.; Yang, H.M.; Wu, A.M.S. The prospective effect of problematic smartphone use and fear of missing out on sleep among Chinese adolescents. Curr. Psychol. 2021, 1–9. [Google Scholar] [CrossRef]
- Höhn, C.; Schmid, S.; Plamberger, C.; Bothe, K.; Angerer, M.; Gruber, G.; Pletzer, B.; Hoedlmoser, K. Preliminary Results: The Impact of Smartphone Use and Short-Wavelength Light during the Evening on Circadian Rhythm, Sleep and Alertness. Clocks Sleep 2021, 3, 66–86. [Google Scholar] [CrossRef]
- Bahji, A.; Brietzke, E.; Soares, C.; Stuart, H. Recent Advances in Biomarkers of Addiction: A Narrative Review. Can. J. Addict. 2021, 12, 6–12. [Google Scholar] [CrossRef]
- Hanlon, C.; Canterberry, M. The use of brain imaging to elucidate neural circuit changes in cocaine addiction. Subst. Abus. Rehabil. 2012, 3, 115–128. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yeh, P.-H.; Simpson, K.; Durazzo, T.C.; Gazdzinski, S.; Meyerhoff, D. Tract-based spatial statistics (TBSS) of diffusion tensor imaging data in alcohol dependence: Abnormalities of the motivational neurocircuitry. Psychiatry Res. Neuroimag. 2009, 173, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Qin, W.; Wang, G.; Zeng, F.; Zhao, L.; Yang, X.; Liu, P.; Liu, J.; Sun, J.; Von Deneen, K.M.; et al. Microstructure Abnormalities in Adolescents with Internet Addiction Disorder. PLoS ONE 2011, 6, e20708. [Google Scholar] [CrossRef]
- Zhou, Y.; Lin, F.-C.; Du, Y.-S.; Qin, L.-D.; Zhao, Z.-M.; Xu, J.-R.; Lei, H. Gray matter abnormalities in Internet addiction: A voxel-based morphometry study. Eur. J. Radiol. 2011, 79, 92–95. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors, Country, Year | Sample Size | Type of Population | Age/Age Range | Gender | Type of Study | Outcome Measurement Tool | Pattern of Survey | Assessment Tool (SA) |
|---|---|---|---|---|---|---|---|---|
| Hye-Jin Kim [21,47], South Korea, 2017 | 608 | University/college students | Control:23.01 ± 2.32, SA: 22.54 ± 2.05 | Male = 183, Female = 425 | Cross-sectional | Self-reported experience of accidents was assessed | Online questionnaire-based survey | SAPS |
| Yeon-Jin Kim [22], South Korea, 2015 | 4854 | General | Age range 19–49 | Male = 2573, Female = 2281 | Cross-sectional | The Symptom Checklist-90-Revised-SCL-90-R | Online survey | K-scale |
| Deokjong Lee [23], South Korea, 2019 | 94 | General | 22.6 ± 2.4 (Age range 16–27) | Male = 61, Female = 27 | Cross-sectional | Magnetic resonance imaging (MRI) scan | Online advertisements, MRI | SAPS |
| JeonHyeong Lee [24], South Korea, 2014 | 30 | University students | N = 22.6 ± 1.3, Moderate Addiction Group (MAG) = 21.5 ± 1.9, Severe Addiction Group (SAG) = 22.4 ± 2.0 | Male = 12, Female = 18 | Cross-sectional | Motion meter (Performance Attainment Associates, West Germany) | Survey, the range of motion (ROM), a range of motion meter (Performance Attainment Associates, West Germany) | SAPS |
| Kyung Eun Lee [25], South Korea, 2016 | 1261 | University/ college students | M 23.6 ± 2.7, F 21.5 ± 2.7 | Male = 725, Femle = 511 | Cross-sectional study | Zung’s Self-Rating Anxiety Scale | Face-to-face interview | Young’s Internet Addiction Test |
| Yeon-Seop Lee [26], South Korea, 2012 | 125 | General | 21.4 ± 2.0 | Male = 32, Female = 93 | Cross-sectional | Phalen’s tests, Reverse Phalen’s tests, Ultrasonography | Structured questionnaires | Structured questionnaires |
| Mi Jung Rho [27] South Korea, 2019 | 5372 | General | 26.43 ± 5.954 (Age range 19–39) | Male = 2443, Female = 2929 | Cross-sectional | Brief Self-Control Scale (BSCS), Generalized Anxiety Disorder (GAD)-7, Patient Health Questionnaire-9 (PHQ-9), and Dickman Impulsivity Inventory-Short Version (DII). | Web survey | S-Scale |
| Aljohara A. Alhassan [28], Saudi Arabia, 2018 | 935 | General public | 31.7 ± 10.98 younger age group (18–35 years), middle-age group (36–54 years), and older age group (≥55 years) | Male = 316 (33.8%), Female = 619 (66.2%) | Cross-sectional | The Beck’s Depression Inventory second edition | Web-based | SAS-SV |
| Alosaimi, F. D. [29], Saudi Arabia, 2016 | 2367 | University students | not mentioned | Male = 43.6% | Cross-sectional | Not mentioned | An electronic self-administered questionnaire | PUMP |
| Dalia El-Sayed [30], Saudi Arabia, 2020 | 1513 | University students | M = 20.58 (1.71) | Male = 825 (54.5%) Female = 688 (45.5%) | Cross-sectional | Taylor Manifest Anxiety Scale and Beck Depression Inventory | Not reported | The Problematic Use of Mobile Phones (PUMP) scale |
| Jon D. Elhai [31], China, 2019 | 1034 | Young adults | 19.34 ± 1.61 | Male = 359, Female = 675 | Cross-sectional | Depression anxiety stress scale-21 (DASS-21), Fear of missing out (FOMO) scale | Web survey | SAS-SV |
| Yuanming Hu [32], China, 2017 | 49 | Young adults | Control: 23.07 ± 2.01, SPD: 22.11 ± 1.78 | Male = 26, Female = 23 | Cross-sectional | Tract-based spatial statistics (TBSS) analysis | Survey questionnaire | MPATS |
| Jon D. Elhai [33], China, 2020 | 908 | General | Age averaged 40.37 years (SD = 9.27) | Male = 156, Female = 752, | Cross-sectional | Depression anxiety stress scale-21 (DASS-21) Generalized anxiety disorder scale-7 (GAD-7) for COVID-19 anxiety | Web-based survey | Smartphone addiction scale-short version (SAS-SV) |
| Linbo Zhuang [34], China, 2021 | 2438 | Young patients | Age, 18–44 years | Male = 1085, Female = 1353 | Cross-sectional study | Magnetic Resonance Imaging (MRI) examination, Cervical Disc Degeneration Scale (CDDS) | Not reported | Smartphone Addiction Scale (SAS) |
| Yasemin P. Demir [35], Turkey, 2019 | 123 | Patients who had Migraine | >18 years and <65 years | Male = 69, Female = 54 | Cross-sectional comparative | Migraine disability assessment (MIDAS) questionnaire, The Visual Analogue Scale (VAS), Migraine Quality of Life Questionnaire) 24-h MQoLQ, Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS) | Written survey questionnaire | PUMP |
| Kadir Demirci [36], Turkey, 2015 | 319 | University students | Mean age = 20.5 ± 2.45 years
| Male = 116, Female = 203 | Cross-sectional | Pittsburgh Sleep Quality Index (PSQI), Beck Depression Inventory (BDI), Beck Anxiety Inventory (BAI) | Not reported | PUMP |
| Ayse Gokce [37], Turkey, 2021 | 319 | University Students | 18–33, 21.03 ± 2.05 | Male = 104, Female = 215 | Cross-sectional study | The Liebowitz Social Anxiety Scale (LSAS); Eating Attitudes Test (EAT). | Face-to-face survey | Problematic Mobile Phone Use Scale |
| Betul Ozcan [38], Turkey, 2021 | 1545 | 21.39 ± 2.21 years | Male = 43.2%, Female = 56.8% | Cross-sectional study | Pittsburgh Sleep Quality Index (PSQI) | Not reported | Smartphone Addiction Scale-Short Version (SAS-SV) | |
| S HariPriya [39], India, 2019 | 113 | College students | 22.15 ± 1.69 (Age range 19–25) | Male = 63, Female = 50 | Cross-sectional study | Pittsburgh Sleep Quality Index (PSQI), International Physical Activity Questionnaire-Short Form (IPAQSF) | Written survey questionnaire | Self-reported questionnaire |
| Hsien-Yuan Lane [40], Taiwan, 2021 | 422 | University students | 20.22 (SD = 2.34 years) | Male = 79, Female = 343 | Cross-sectional study | Tri-Dimensional Personality Questionnaire (TPQ), Chinese Version of the Pittsburgh Sleep Quality Index (CPSQI), Beck Depression Inventory (BDI), Beck Anxiety Inventory (BAI) | Online | Chen’s Smartphone Addiction Inventory |
| Anna Maria [41] Switzerland, 2021 | 240 | Young adults | 18–35 years old, Mean age = 23.33, | Male = 120, Female = 120 | Cross-sectional | 12-item Social Anxiety Scale, a question on the daily duration of smartphone use, a single-item measure of dispositional truth | Online | Smartphone Addiction Scale Short Version |
| Jon D. Elhai [42], USA, 2018 | 300 | College students | 19.87 ± 3.79 | Male = 24.3%, Female = 75.7% | Cross-sectional | Penn State Worry Questionnaire-Abbreviated Version (PSWQ-A), Dimensions of Anger Reactions-5 (DAR-5) Scale | Web survey | SAS-SV |
| Matteo Megna [43], Italy, 2018 | 52 | Psoriatic patients | 26.9 ± 7.8 (age range 18–35) | Male = 24, Female = 28 | Cross-sectional | Nail Psoriasis Severity Index (NAPSI), Early psoriatic arthritis screening questionnaire (EARP), ultrasound score | Face-to-face interview | SAS-SV |
| Arunrat TangmunkongvorakulI [44], Thailand, 2019 | 800 | University students | 18–24 (Age range 18–24) | Male = 395, Female = 405 | Cross-sectional | Flourishing Scale (FS) | Face-to-face | Young’s Internet Addiction Test |
| Zaheer Hussain [45], Global (majority in the UK, 86%), 2017 | 640 | General | 24.89 ± 8.54 (Age range 13–69) | Male = 214, Female = 420 | Cross-sectional | Spielberger State-Trait Anxiety Inventory (STAI) Short-Form | Online survey | Independent questionnaire (Problematic smartphone use scale) |
| Miles Richardson [46], 2018, Global (majority UK, 82.8%) | 244 | General | 29.72 ± 12.16 | Male = 90, Female = 149 | Cross-sectional | Spielberger State-Trait Anxiety Inventory (STAI), Nature Relatedness Scale | Web survey | PSUS |
| Asem A. Alageel [47], worldwide, 2021 | 506 | Postgraduate students | Age 21 years and above (21–24 = 9.41%, 25–29 = 35.88% 30–39 = 44.51%, >=40 = 10.20%) | Male = 158 Female = 348 | Cross-sectional | Patient Health Questionnaire (PHQ9) for depression, Athens Insomnia Scale (AIS), the Fagerström Test for Cigarette Dependence Questionnaire (FTCd),The adult ADHD Self-Report Scale (ASRS-v1.1) | Online | Smartphone Addiction Scale (SAS) |
| Author and Reference | Outcomes | Specific Outcome | Quality |
|---|---|---|---|
| HYE-JIN KIM [21] |
| Accident | Fair |
| Yeon-Jin Kim [22] |
| Depression and anxiety | Fair |
| DEOKJONG LEE [23] |
| Gray matter abnormalities | Fair |
| JeonHyeong Lee [24] |
| Musculoskeletal problems | Fair |
| Kyung Eun Lee [25] |
| Anxiety | Fair |
| Yeon-Seop Lee [26] |
| Carpal tunnel syndrome | Poor |
| Mi Jung Rho [27] | Mental health problems were related to problematic smartphone use: (1) self-control (66%), (2) anxiety (25%), (3) depression (7%), and (4) dysfunctional impulsivities (3%) | Psychiatric symptoms | Fair |
| Aljohara A. Alhassan [28] |
| Depression | Fair |
| Alosaimi, F. D. [29] |
| Risk of sedentary behavior | Fair |
| Dalia El-Sayed [30] |
| Depression and trait anxiety | Good |
| Jon D. Elhai [31] |
| Anxiety | Good |
| Yuanming Hu [32] |
| Lower white matter integrity | Fair |
| Jon D. Elhai [33] |
| COVID-19 anxiety | Good |
| Linbo Zhuang [34] |
| cervical disc degeneration | Good |
| Yasemin P. Demir [35] |
| Increased headache duration, poor sleep quality | Fair |
| KADİR DEMİRCİ [36] |
| Depression, anxiety, and daytime dysfunction | Fair |
| Ayse Gokce [37] |
| Increased smoking | Fair |
| Betul Ozcan [38] |
| Poor sleep quality | Good |
| S HariPriya [39] |
| Poor sleep quality, less physical activity | Good |
| Hsien-Yuan Lane [40] |
| Psychological distress, poor sleep quality | Good |
| Anna Maria [41] |
| Social anxiety | Fair |
| Jon D. Elhai [42] |
| Worry and anger | Good |
| Matteo Megna [43] |
| Psoriatic arthritis | Fair |
| Arunrat TangmunkongvorakulI [44] |
| Psychological well-being | Fair |
| Zaheer Hussain [45] |
| Anxiety | Good |
| MILES RICHARDSON [46] |
| Connectedness with nature and anxiety | Fair |
| Asem A. Alageel [47] |
| Insomnia, depression, adult ADHD | Fair |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratan, Z.A.; Parrish, A.-M.; Zaman, S.B.; Alotaibi, M.S.; Hosseinzadeh, H. Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12257. https://doi.org/10.3390/ijerph182212257
Ratan ZA, Parrish A-M, Zaman SB, Alotaibi MS, Hosseinzadeh H. Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(22):12257. https://doi.org/10.3390/ijerph182212257
Chicago/Turabian StyleRatan, Zubair Ahmed, Anne-Maree Parrish, Sojib Bin Zaman, Mohammad Saud Alotaibi, and Hassan Hosseinzadeh. 2021. "Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 22: 12257. https://doi.org/10.3390/ijerph182212257
APA StyleRatan, Z. A., Parrish, A.-M., Zaman, S. B., Alotaibi, M. S., & Hosseinzadeh, H. (2021). Smartphone Addiction and Associated Health Outcomes in Adult Populations: A Systematic Review. International Journal of Environmental Research and Public Health, 18(22), 12257. https://doi.org/10.3390/ijerph182212257