
Feasibility of Delivering an on-Campus Food Distribution Program in a Community College Setting: A Mixed Methods Sequential Explanatory Investigation

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
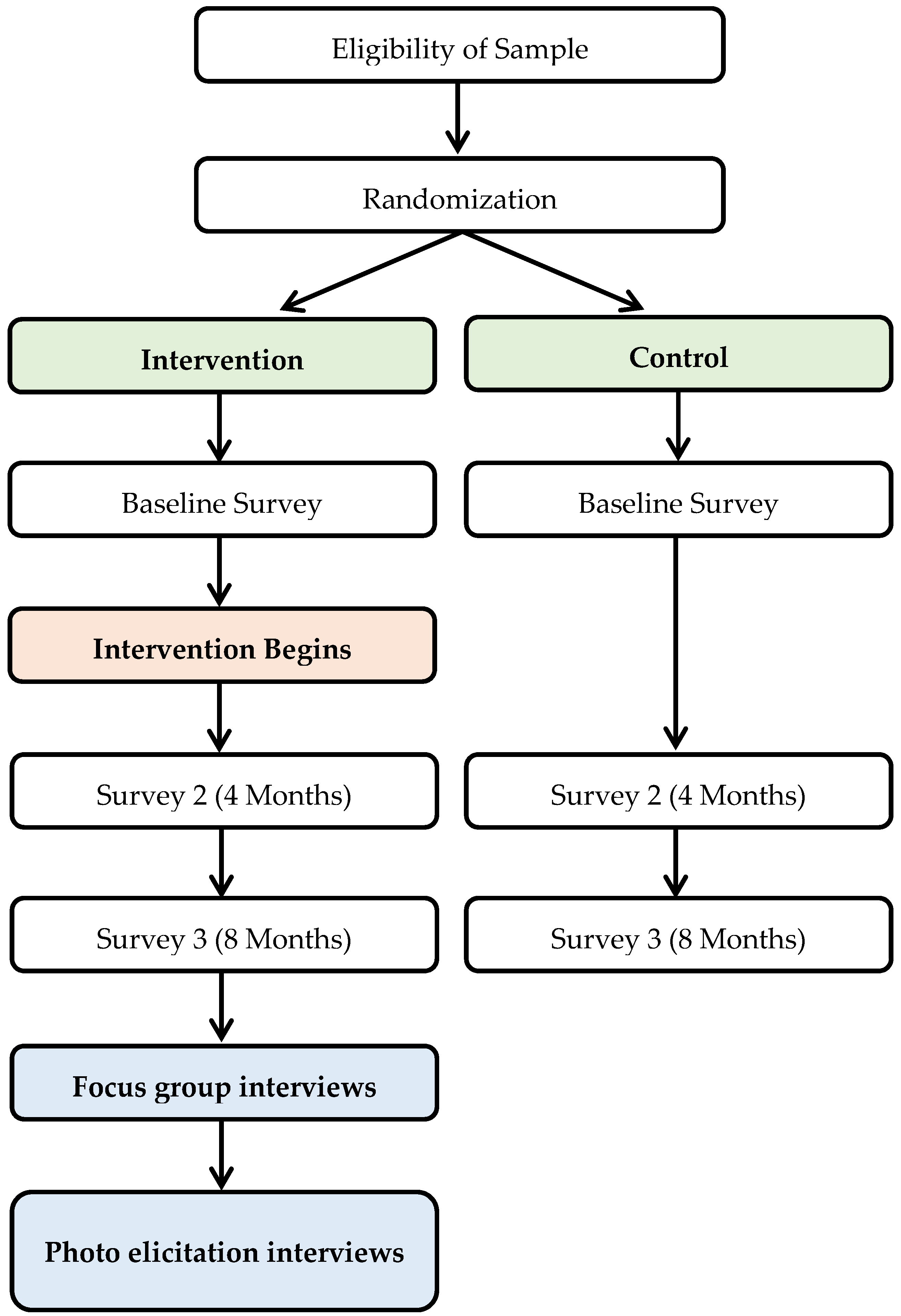
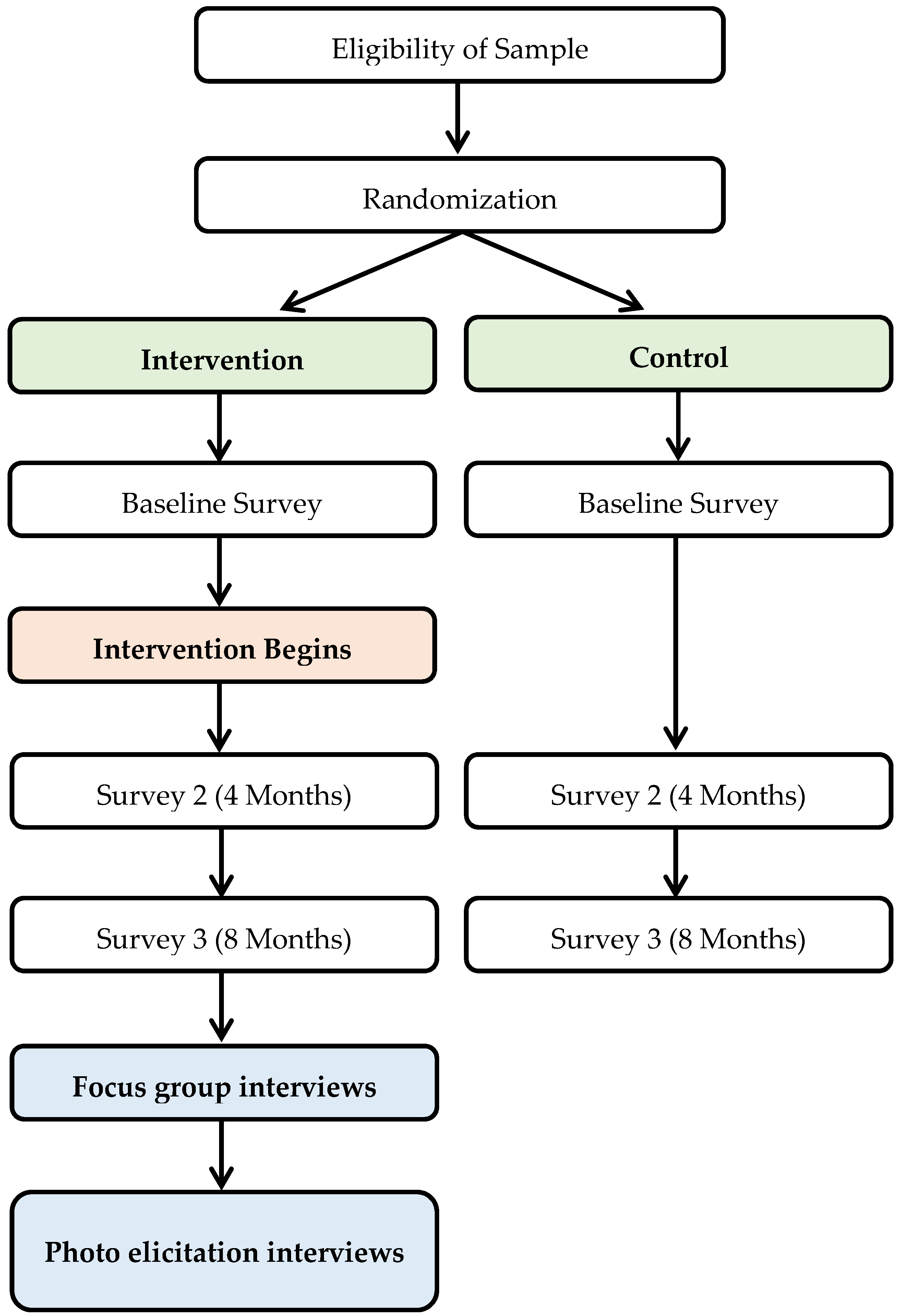
2.2. Study Design and Eligibility
2.3. Randomization
2.4. Recruitment for the Intervention
2.5. Survey
2.6. Intervention: Food Distribution Program
2.7. Focus Groups and Photo Elicitation Interviews
2.8. Measures
2.8.1. Recruitment Capability and Resulting Intervention Sample Characteristics
2.8.2. Data Collection Procedures and Outcome Measures
2.8.3. Participants’ Acceptability and Responses to the Intervention
2.9. Data Analysis
Trustworthiness and Credibility
3. Results
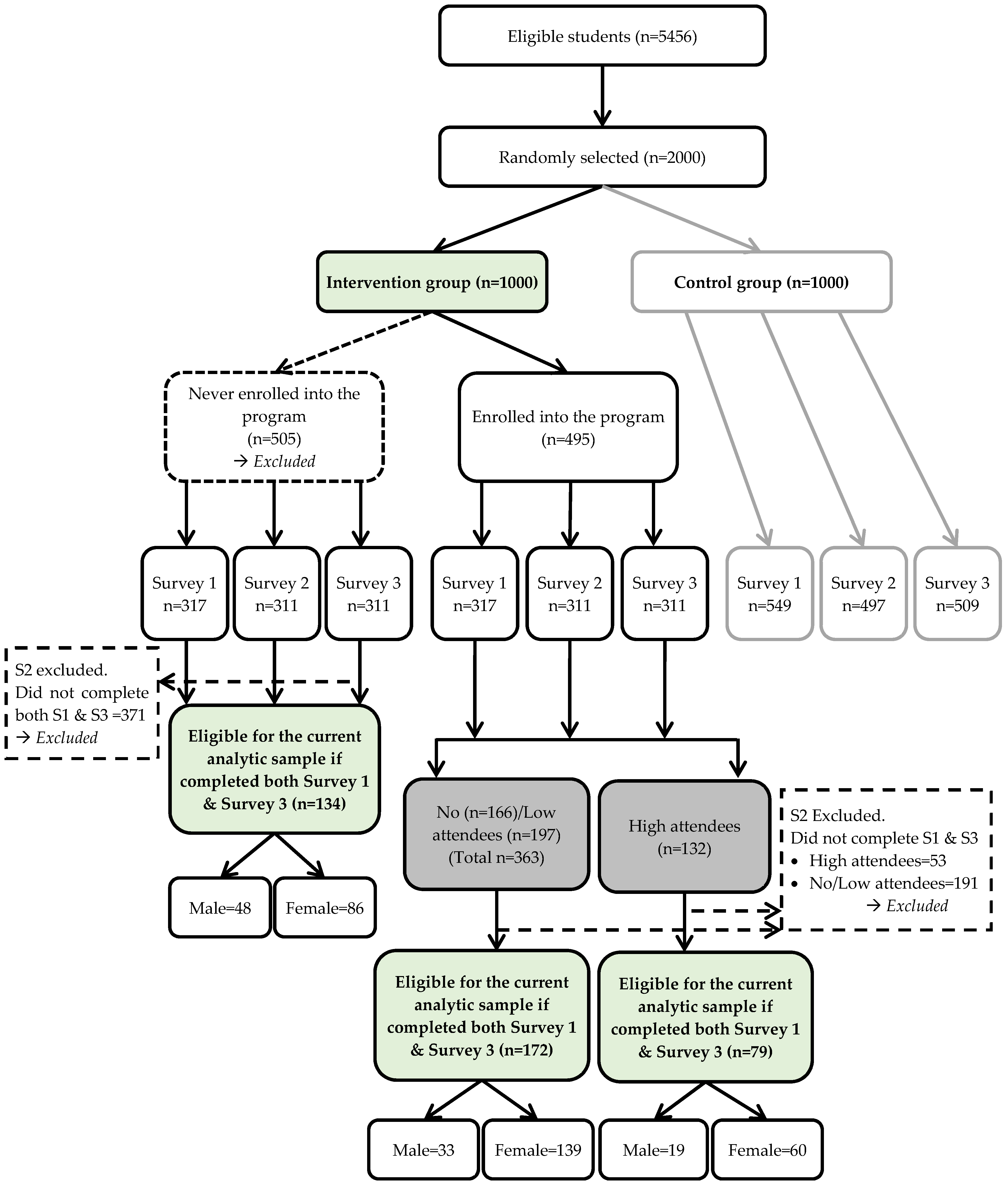
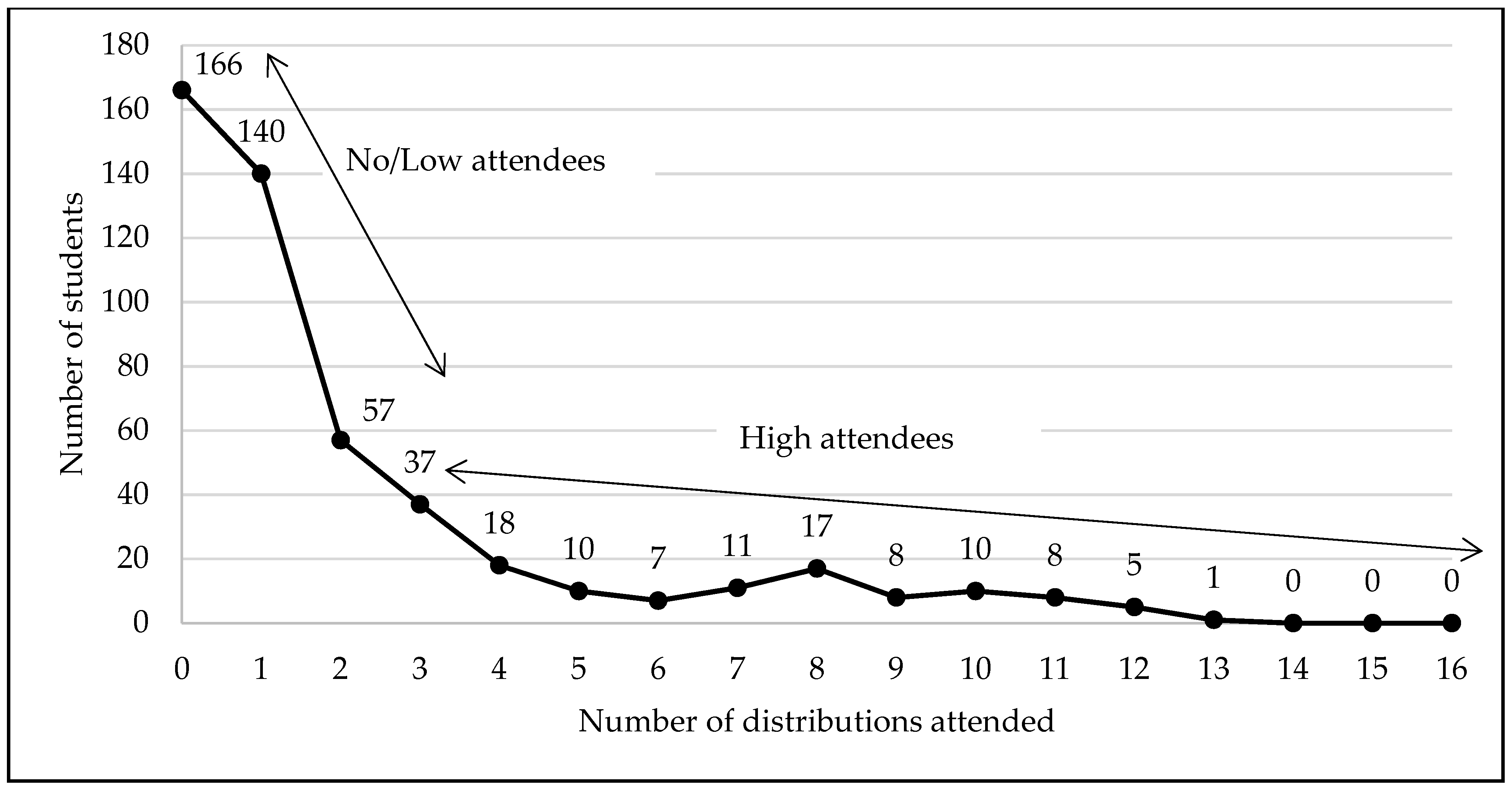
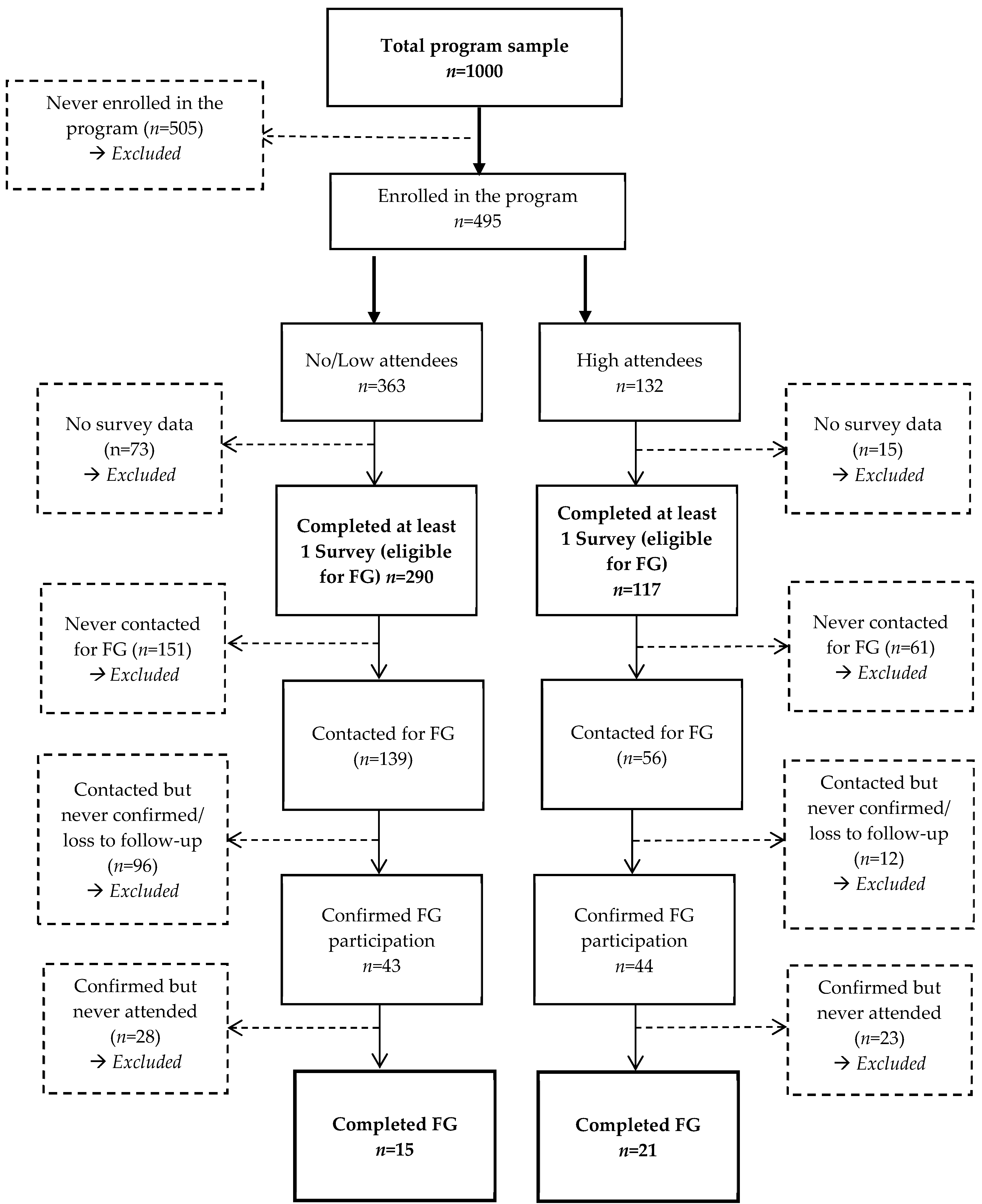
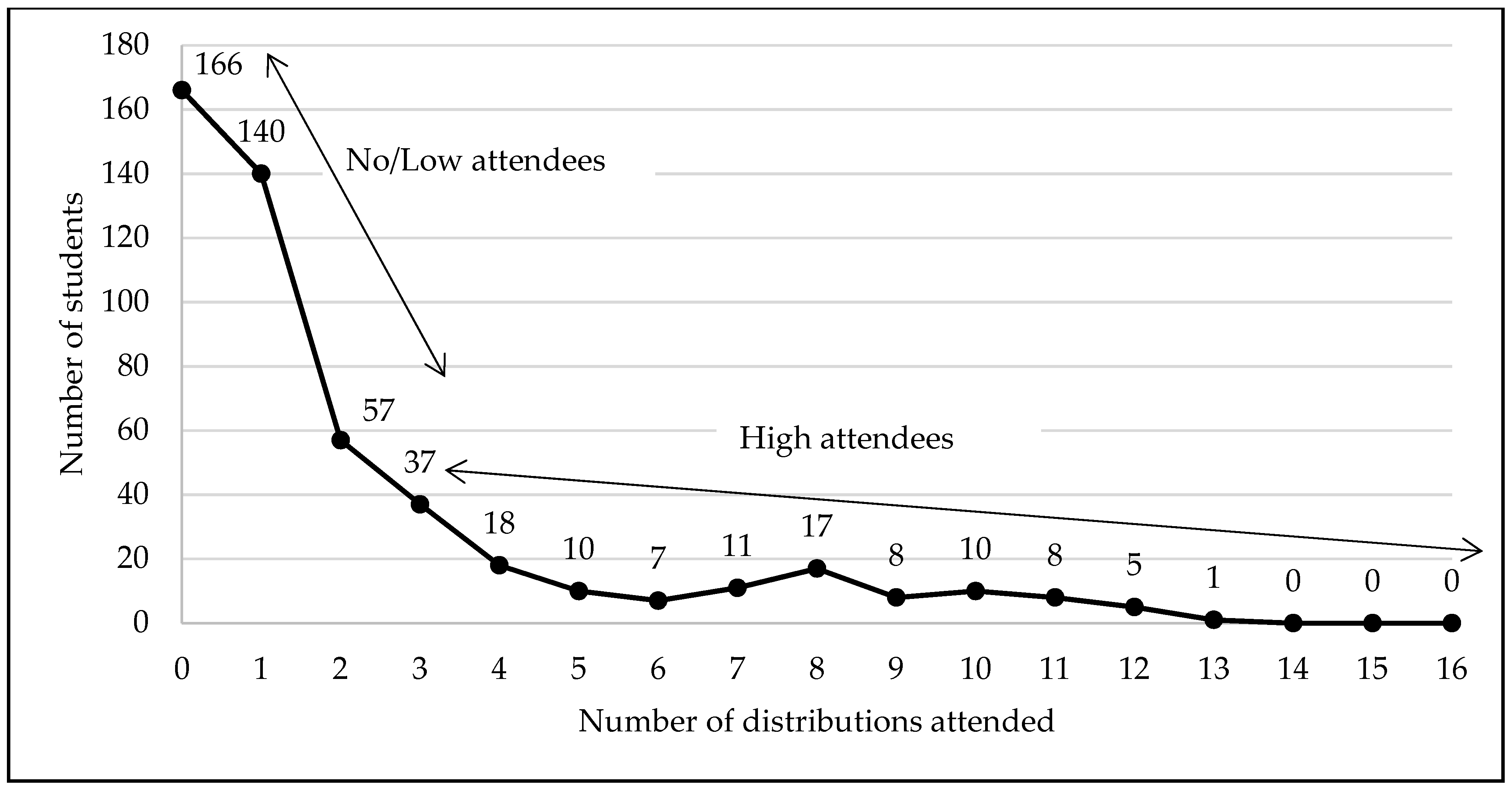
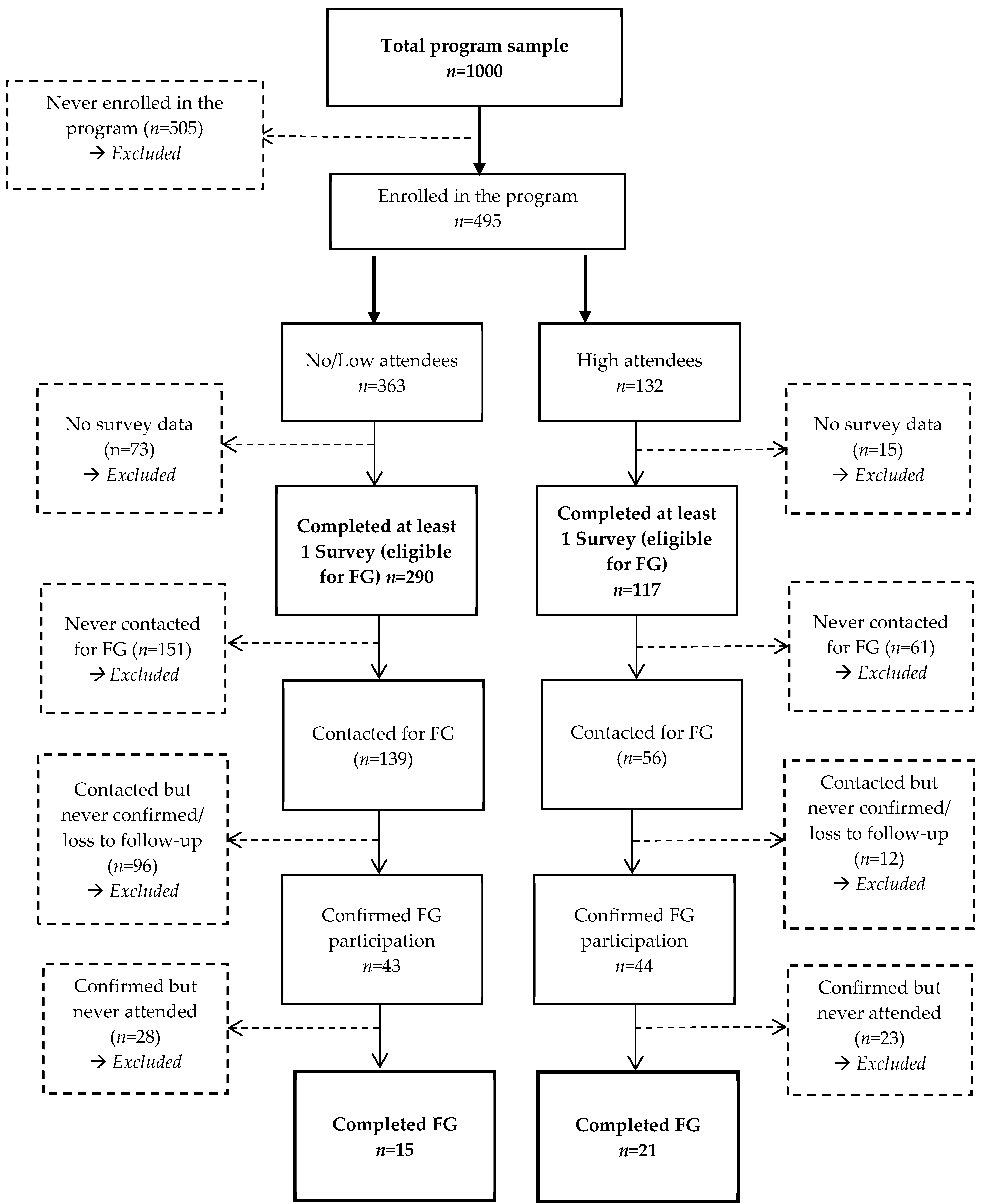
3.1. Recruitment Feasibility and Resulting Intervention Sample Characteristics
3.2. Evaluation of Data Collection Procedures and Sample Characteristics of the Students That Enrolled
3.3. Evaluation of Outcome Measures
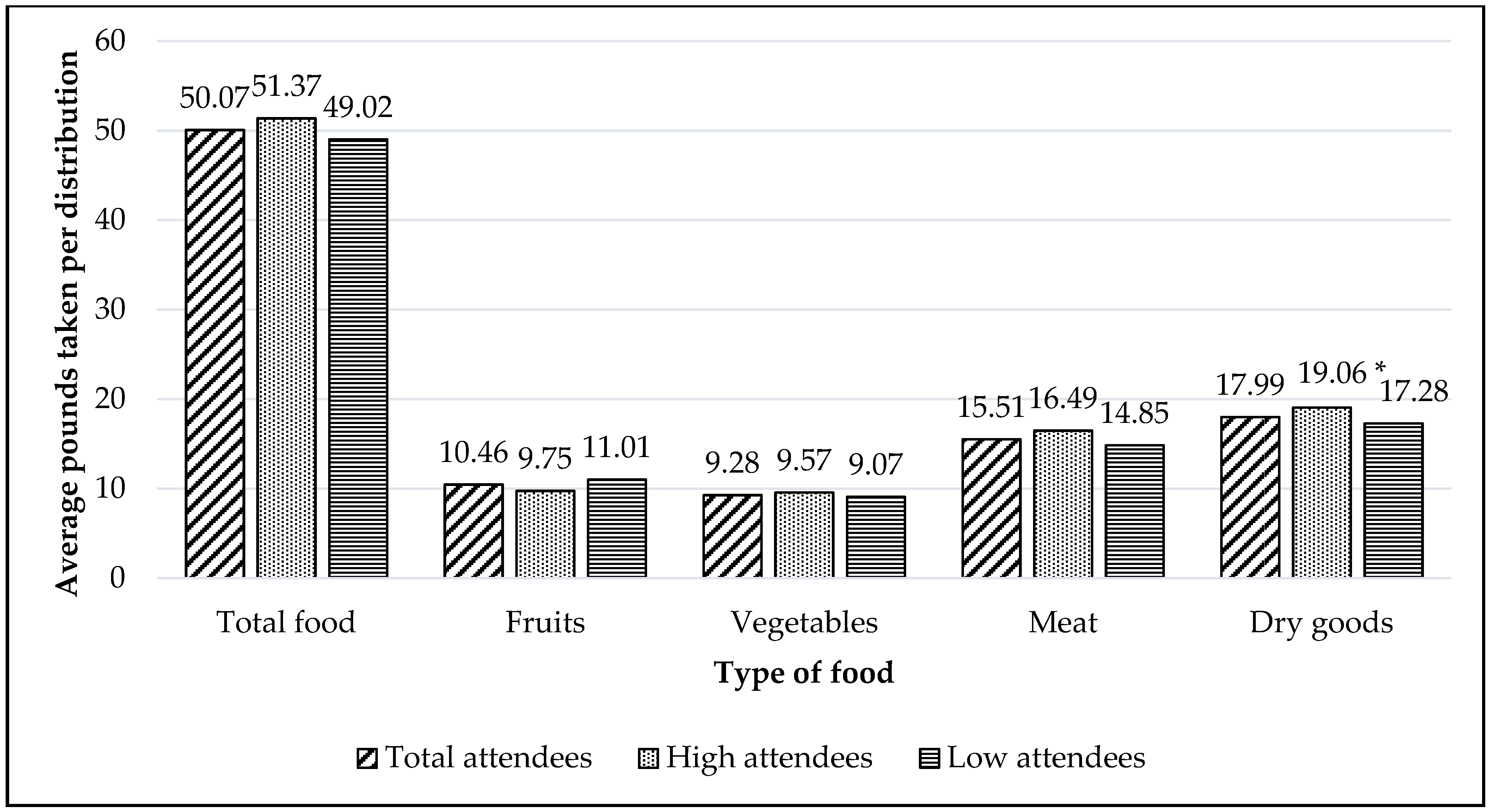
3.3.1. Poundage of Food
3.3.2. Dietary Intake
3.3.3. Food Insecurity
3.4. Evaluation of Participants’ Acceptability and Responses to the Intervention
3.5. Barriers Limiting FDP Utilization
3.5.1. The Program’s Design and Organization
3.5.2. Personal Schedule and Transportation
3.5.3. Program Abuse by Other Attendees
3.6. Facilitators for FDP Utilization
3.6.1. Type of Food Distributed and Welcoming Environment
3.6.2. Allowing a Substitute Shopper to Collect Food
4. Discussion
4.1. Recruitment Feasibility
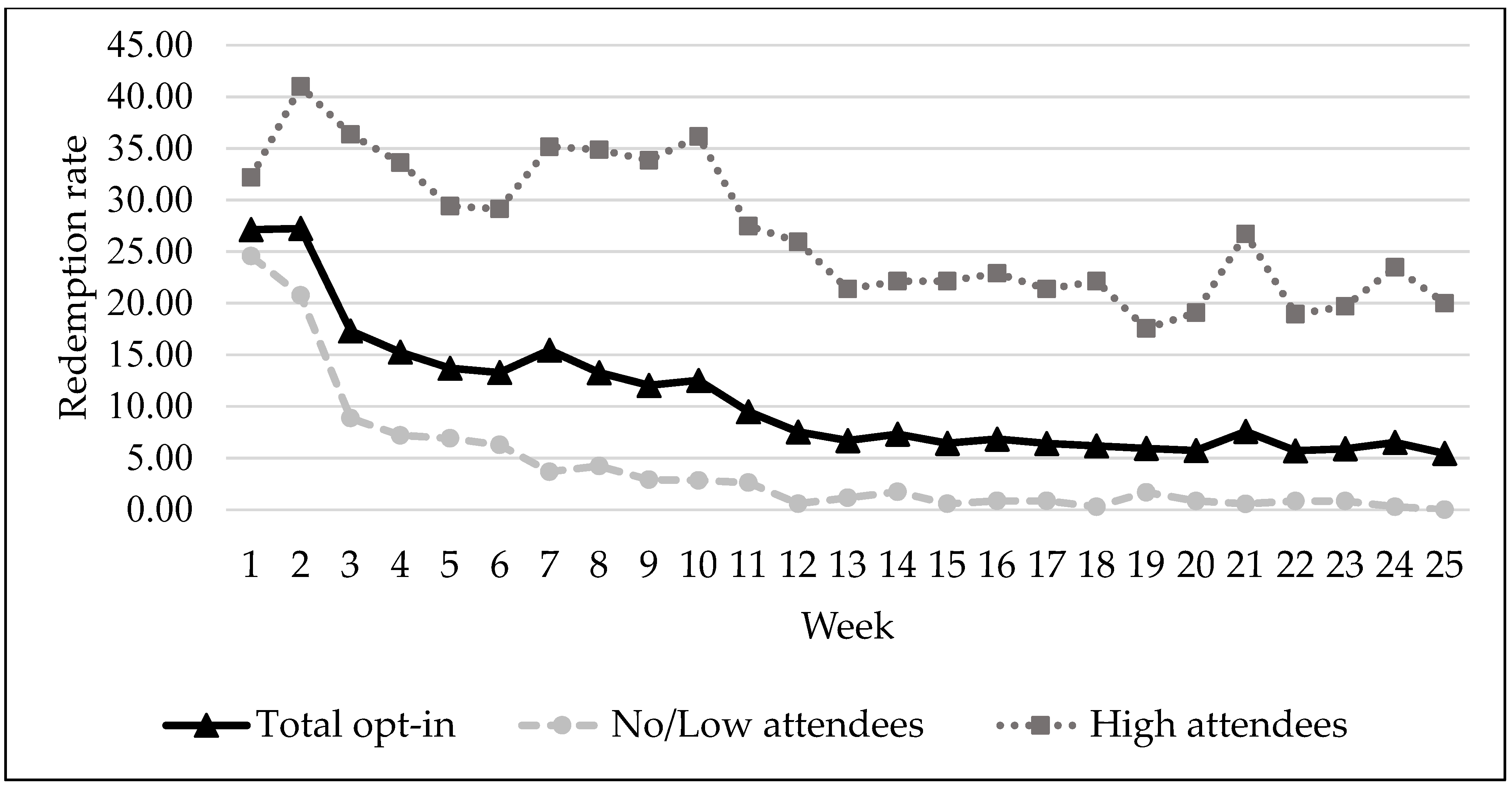
4.2. Utilization
4.3. Dietary Intake
4.4. Food Insecurity
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ma, J.; Baum, S. Trends in Community Colleges: Enrollment, Prices, Student Debt, and Completion; College Board: New York, NY, USA, 2016; Available online: https://research.collegeboard.org/pdf/trends-community-colleges-research-brief.pdf (accessed on 7 November 2011).
- Blagg, K.; Gundersen, C.; Schanzenbach, D.W.; Ziliak, J.P. Assessing Food Insecurity on Campus; The Urban Institute: Washington, DC, USA, 2017; Available online: http://www.urban.org/sites/default/files/publication/92331/assessing_food_insecurity_on_campus_0.pdf (accessed on 7 November 2021).
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2019, ERR-275; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2020.
- Maroto, M.E.; Snelling, A.; Linck, H. Food insecurity among community college students: Prevalence and association with grade point average. Comm. Coll. J. Res. Pract. 2015, 39, 515–526. [Google Scholar] [CrossRef]
- Martinez, S.M.; Frongillo, E.A.; Leung, C.; Ritchie, L. No food for thought: Food insecurity is related to poor mental health and lower academic performance among students in California’s public university system. J. Health Psychol. 2020, 25, 1930–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raskind, I.G.; Haardorfer, R.; Berg, C.J. Food insecurity, psychosocial health, and academic performance among college and university students in Georgia, USA. Public Health Nutr. 2019, 22, 476. [Google Scholar] [CrossRef]
- Davison, K.M.; Gondara, L.; Kaplan, B.J. Food insecurity, poor diet quality, and suboptimal intakes of folate and iron are independently associated with perceived mental health in Canadian adults. Nutrients 2017, 9, 274. [Google Scholar] [CrossRef] [Green Version]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in US adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robaina, K.A.; Martin, K.S. Food insecurity, poor diet quality, and obesity among food pantry participants in Hartford, CT. J. Nutr. Educ. Behav. 2013, 45, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Bruening, M.; MacLehose, R.; Loth, K.; Story, M.; Neumark-Sztainer, D. Feeding a family in a recession: Food insecurity among Minnesota parents. Am. J. Public Health 2012, 102, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Martinez, S.M.; Grandner, M.A.; Nazmi, A.; Canedo, E.R.; Ritchie, L.D. Pathways from food insecurity to health outcomes among California University Students. Nutrients 2019, 11, 1419. [Google Scholar] [CrossRef] [Green Version]
- Haapala, E.A.; Eloranta, A.M.; Venäläinen, T.; Jalkanen, H.; Poikkeus, A.M.; Ahonen, T.; Lindi, V.; Lakka, T.A. Diet quality and academic achievement: A prospective study among primary school children. Eur. J. Nutr. 2017, 56, 2299–2308. [Google Scholar] [CrossRef]
- Tapia-Serrano, M.A.; Esteban-Cornejo, I.; Rodriguez-Ayllon, M.; Vaquero-Solís, M.; Sánchez-Oliva, D.; Sánchez-Miguel, P.A. Adherence to the Mediterranean diet and academic performance in adolescents: Does BMI status moderate this association? Clin. Nutr. 2021. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Stinebrickner, R.; Stinebrickner, T. Academic performance and college dropout: Using longitudinal expectations data to estimate a learning model. J. Labor Econ. 2014, 32, 601–644. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M. Degreeless in Debt: What Happens to Borrowers Who Drop Out. Charts You Can Trust; Education Sector: Washington DC, USA, 2012. [Google Scholar]
- Itzkowitz, M. Want More Students to Pay Down Their Loans? Help Them Graduate; Third Way: Washington, DC, USA, 2018; Available online: http://thirdway.imgix.net/pdfs/want-more-students-to-pay-down-their-loans-help-them-graduate.pdf (accessed on 9 November 2021).
- El Zein, A.; Mathews, A.E.; House, L.; Shelnutt, K.P. Why are hungry college students not seeking help? Predictors of and barriers to using an on-campus food pantry. Nutrients 2018, 10, 1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McArthur, L.H.; Fasczewski, K.S.; Farris, A.R.; Petrone, M. Use and perceptions of a campus food pantry among food insecure college students: An exploratory study from Appalachia. J. Appalach. Health 2020, 2, 7–23. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Ivankova, N.V.; Creswell, J.W.; Stick, S.L. Using mixed-methods sequential explanatory design: From theory to practice. Field Methods 2006, 18, 3–20. [Google Scholar] [CrossRef]
- Orsmond, G.I.; Cohn, E.S. The distinctive features of a feasibility study: Objectives and guiding questions. OTJR 2015, 35, 169–177. [Google Scholar] [CrossRef] [PubMed]
- National Center for Education Statistics. College Navigator. 2015. Available online: https://nces.ed.gov/collegenavigator/ (accessed on 5 May 2021).
- Eigege, C.Y.; Daundasekara, S.S.; Gomez, M.L.; Walton, Q.L.; Hernandez, D.C. Conducting Research Six Feet Apart: The Feasibility of Transitioning Qualitative Research to Meet the Merging Resesarch Needs during a Pandemic. Int. J. Qual. Methods 2021, accepted. [Google Scholar]
- Hernandez, D.C.; Walton, Q.L.; Eigege, C.Y.; Daundasekara, S.S.; Marshall, A.N. Using Photo Elicitaiton Methods to Explore Food Insecurity and Material Hardship. 2021; manuscript in preparation, to be submitted. [Google Scholar]
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security, Revised 2000; Food and Nutrition Service: Alexandria, VA, USA, 2000.
- Block, G.; Gillespie, C.; Rosenbaum, E.H.; Jenson, C. A rapid food screener to asses fat and fruit and vegetable intake. Am. J. Prev. Med. 2000, 18, 284–288. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- National Institutes of Health. Nutrient Recomendations: Dietary Reference Intakes (DRI); US Department of Health and Human Services: Washington, DC, USA, 2021. Available online: https://ods.od.nih.gov/HealthInformation/Dietary_Reference_Intakes.aspx (accessed on 20 May 2021).
- Glaser, B.G.; Straus, A.L. The Discoverty of Grounded Theory: Strategies for Qualitative Research; Sociology Press: Mill Valley, CA, USA, 1967. [Google Scholar]
- Dedoose Version 8.3.43. In Web Application for Managing, Analyzing, and Presenting Qualitative and Mixed Method Research Data; SocioCultural Research Consultants, LLC: Los Angeles, CA, USA, 2020; Available online: www.dedoose.com (accessed on 9 November 2021).
- Kidd, P.S.; Parshall, M.B. Getting the focus and the group: Enhancing analytical rigor in focus group research. Qual. Health Res. 2000, 10, 293–308. [Google Scholar] [CrossRef]
- Onwuegbuzie, A.J.; Dickinson, W.B.; Leech, N.L.; Zoran, A.G. A qualitative framework for collecting and analyzing data in focus group research. Int. J. Qual. Methods 2009, 8, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, S. Focus groups in health research: Exploring the meanings of health and illness. J. Health Psychol. 1998, 3, 329–348. [Google Scholar] [CrossRef] [Green Version]
- Ilieva, R.T.; Ahmed, T.; Yan, A. Hungry minds: Investigating the food insecurity of minority community college students. J. Public Aff. 2019, 19, e1891. [Google Scholar] [CrossRef]
- Meier, C.; Ryan, G.; Askelson, N.; Pieper, F.; Greene, M.; Buckert, A.; Rasmusson, A. Meeting household food needs: A qualitative examination of food access among parenting community college students. Comm. Coll. J. Res. Pract. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Hill, C.E.; Thompson, B.J.; Williams, E.N. A guide to conducting consensual qualitative research. Couns. Psychol. 1997, 25, 517–572. [Google Scholar] [CrossRef] [Green Version]
- Aiyer, J.N.; Raber, M.; Bello, R.S.; Brewster, A.; Caballero, E.; Chennisi, C.; Durand, C.; Galindez, M.; Oestman, K.; Saifuddin, M.; et al. A pilot food prescription program promotes produce intake and decreases food insecurity. Transl. Behav. Med. 2019, 9, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Izumi, B.T.; Higgins, C.E.; Baron, A.; Ness, S.J.; Allan, B.; Barth, E.T.; Smith, T.M.; Pranian, K.; Frank, B. Feasibility of using a community-supported agriculture program to increase access to and intake of vegetables among federally qualified health center patients. J. Nutr. Educ. Behav. 2018, 50, 289–296.e1. [Google Scholar] [CrossRef]
- Chuang, R.J.; Cox, J.N.; Mincemoyer, C.C.; Sharma, S.V. A pilot randomized controlled trial of a nutrition and dietary intervention for early care and education providers. J. Sch. Health 2020, 90, 859–868. [Google Scholar] [CrossRef]
- Gans, K.M.; Risica, P.M.; Keita, A.D.; Dionne, L.; Mello, J.; Stowers, K.C.; Papandonatos, G.; Whittaker, S.; Gorham, G. Multilevel approaches to increase fruit and vegetable intake in low-income housing communities: Final results of the ‘Live Well, Viva Bien’ cluster-randomized trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, J. Perceived functional social support and self-rated health: The health promoting effects of instrumental support for the Irish community in London. J. Immigr. Minor. Health 2019, 21, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- O’Conor, R.; Benavente, J.Y.; Arvanitis, M.; Curtis, L.M.; Eldeirawi, K.; Hasnain-Wynia, R.; Federman, A.D.; Hebert-Beirne, J.; Wolf, M.S. Perceived adequacy of tangible social support and associations with health outcomes among older primary care patients. J. Gen. Intern. Med. 2019, 34, 2368–2373. [Google Scholar] [CrossRef] [PubMed]
- Oemichen, M.; Smith, C. Investigation of the food choice, promoters and barriers to food access issues, and food insecurity among low-income, free-living Minnesotan seniors. J. Nutr. Educ. Behav. 2016, 48, 397–404.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMartini, T.L.; Beck, A.F.; Kahn, R.S.; Klein, M.D. Food insecure families: Description of access and barriers to food from one pediatric primary care center. J. Comm. Health 2013, 38, 1182–1187. [Google Scholar] [CrossRef]
- Freedman, D.A.; Vaudrin, N.; Schneider, C.; Trapl, E.; Ohri-Vachaspati, P.; Taggart, M.; Ariel Cascio, M.; Walsh, C.; Flocke, S. Systematic review of factors influencing farmers’ market use overall and among low-income populations. J. Acad. Nutr. Diet. 2016, 116, 1136–1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritter, G.; Walkinshaw, L.P.; Quinn, E.L.; Ickes, S.; Johnson, D.B. An assessment of perceived barriers to farmers’ market access. J. Nutr. Educ. Behav. 2019, 51, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Haynes-Maslow, L.; Auvergne, L.; Mark, B.; Ammerman, A.; Weiner, B.J. Low-income individuals’ perceptions about fruit and vegetable access programs: A qualitative study. J. Nutr. Educ. Behav. 2015, 47, 317–324.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simmet, A.; Depa, J.; Tinnemann, P.; Stroebele-Benschop, N. The nutritional quality of food provided from food pantries: A systematic review of existing literature. J. Acad. Nutr. Diet. 2017, 117, 577–588. [Google Scholar] [CrossRef]
- Lee, C.Y.; Zhao, X.; Reesor-Oyer, L.; Cepni, A.B.; Hernandez, D.C. Bidirectional relationship between food insecurity and housing instability. J. Acad. Nutr. Diet. 2021, 121, 84–91. [Google Scholar] [CrossRef]
- Hernandez, D.C. The impact of cumulative family risks on various levels of food insecurity. Soc. Sci. Res. 2015, 50, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Fleischhacker, S.; Petsoulis, C.; Bruening, M.; Stebleton, M.J. Addressing college food insecurity: An assessment of federal legislation before and during Coronavirus disease-2019. J. Nutr. Educ. Behav. 2020, 52, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Fleischhacker, S.; Petsoulis, C.; Bruening, M.; Stebleton, M.J. Food insecurity among college students: An analysis of US state legislation through 2020. J. Nutr. Educ. Behav. 2021, 53, 261–266. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Program Sample (n = 1000) | Program Sample (n = 1000) | Enrolled into the Program (n = 495) | ||
|---|---|---|---|---|---|
| Never Enrolled into the Program (n = 505) | Enrolled into the Program (n = 495) | No/Low Attendees (n = 363) | High Attendees (n = 132) | ||
| Age | 29.65(10.35) | 27.71 (9.10) | 31.63 (11.15) a | 30.16 (10.40) | 35.66 (12.16) b |
| Gender | |||||
| Male | 331 (33.1%) | 209 (41.4%) | 122 (24.7%) a | 91 (25.1%) | 31 (23.5%) |
| Female | 669 (66.9%) | 296 (58.6%) | 373 (75.4%) | 272 (74.9%) | 101 (76.5%) |
| Race/ethnicity | |||||
| Non-Hispanic white | 79 (7.9%) | 37 (7.3%) | 42 (8.5%) | 34 (9.4%) | 8 (6.1%) |
| Non-Hispanic black | 544 (54.4%) | 263 (52.1%) | 281 (56.8%) | 200 (55.1%) | 81 (61.4%) |
| Hispanic | 289 (28.9%) | 156 (30.9%) | 133 (26.9%) | 94 (25.9%) | 39 (29.6%) |
| Other | 88 (8.8%) | 49 (9.7%) | 39 (7.9%) | 35 (9.6%) | 4 (3.1%) b |
| Marital status | |||||
| Married | 78 (7.8%) | 31 (6.2%) | 47 (9.5%) a | 35 (9.6%) | 12 (9.1%) |
| Divorced/separated | 77 (7.7%) | 31 (6.2%) | 46 (9.3%) | 32 (8.8%) | 14 (10.6%) |
| Single | 844 (84.4%) | 442 (87.7%) | 402 (81.2%) a | 296 (81.5%) | 106 (80.3%) |
| Academic level | |||||
| Freshman | 724 (72.4%) | 378 (74.9%) | 346 (69.9%) | 262 (72.2%) | 84 (63.6%) |
| Sophomore | 59 (5.9%) | 30 (5.9%) | 29 (5.9%) | 18 (5.0%) | 11 (8.3%) |
| Associate degree | 76 (7.6%) | 35 (6.9%) | 41 (8.3%) | 28 (7.7%) | 13 (9.9%) |
| Bachelor’s degree | 29 (2.9%) | 13 (2.6%) | 16 (3.2%) | 14 (3.9%) | 2 (1.5%) |
| Master’s degree | 5 (0.5%) | 3 (0.6%) | 2 (0.4%) | 1 (0.3%) | 1 (0.8%) |
| Unclassified/not available | 107 (10.7%) | 46 (9.1%) | 61 (12.3%) | 40 (11.0%) | 21 (15.9%) |
| Employment status | |||||
| Full-time employee | 114 (11.4%) | 59 (11.7%) | 55 (11.1%) | 39 (10.7%) | 16 (12.1%) |
| Part-time employee | 153 (15.3%) | 85 (16.8%) | 68 (13.7%) | 49 (13.5%) | 19 (14.4%) |
| Not employed | 733 (73.3%) | 361 (71.5%) | 372 (75.2%) | 275 (75.8%) | 97 (73.5%) |
| Female (n = 285) | |||||||
| Dietary Intake Variables | No/Low Attendees (n = 139) | High Attendees (n = 60) | Never Enrolled (n = 86) | Recommended Intakes a | |||
| S1 | S3 | S1 | S3 | S1 | S3 | ||
| Fruit/vegetable score | 11.44 (6.08) | 10.40 (6.03) | 9.95 (6.21) | 9.58 (7.08) | 11.93 (7.09) | 10.97 (6.29) | NA |
| Fruit/vegetable/bean score | 15.17 (8.43) | 13.80 (8.28) | 13.05 (7.54) f | 12.78 (8.55) | 16.16 (9.79) | 15.04 (8.73) | NA |
| Meat/snack score | 24.29 (11.72) | 24.12 (12.39) | 22.45 (11.28) | 20.63 (10.84) f | 25.73 (11.10) | 26.17 (11.50) | NA |
| Fruit and vegetable intake | |||||||
| Fruit and Vegetable servings (per day) | 3.47 (2.23) | 3.08 (2.22) | 2.92 (2.27) | 2.82 (2.55) | 3.64 (2.62) | 3.30 (2.29) | |
| Micronutrient intake | |||||||
| Vitamin C (mg) | 115.97 (55.86) | 106.67 (54.91) | 100.92 (49.15) f | 98.96 (56.89) | 124.05 (64.57) | 116.32 (57.99) | 75.0 |
| Magnesium (mg) | 302.94 (99.55) e | 286.10 (97.97) | 274.39 (86.29) f | 270.53 (101.93) f | 320.26 (113.92) | 306.07 (103.25) | 320.0 |
| Potassium (mg) | 2902.53 (979.63) | 2737.43 (963.67) | 2626.91 (852.92) f | 2590.09 (1001.16) | 3063.54 (1125.36) | 2925.07 (1016.76) | 2600.0 |
| Dietary fiber (g) | 14.20 (6.72) e | 13.06 (6.62) | 12.19 (5.78) f | 11.93 (6.89) f | 15.51(7.61) | 14.54 (6.95) | 25.0 |
| Fat intake | |||||||
| Total fat (f) | 102.19 (28.12) | 101.79 (29.74) | 97.78 (27.07) | 93.42 (26.03) f | 105.66 (26.64) | 106.72 (27.59) | NA b |
| Fat % | 36.67 (7.03) | 36.57 (7.44) | 35.57 (6.77) | 34.48 (6.51) f | 37.54 (6.66) | 37.81 (6.90) | 20–35% |
| Saturated fat (g) | 27.27 (10.31) | 27.13 (10.91) | 25.66 (9.93) | 24.06 (9.54) f | 28.54 (9.77) | 28.93 (10.12) | NA c |
| Dietary cholesterol (g) | 284.55 (92.58) | 283.26 (98.51) | 269.13 (90.20) | 254.96 (86.40) f | 295.86 (90.94) | 299.30 (93.71) | NA d |
| Male (n = 100) | |||||||
| Dietary Intake Variables | No/Low Attendees (n = 33) | High Attendees (n = 19) | Never Enrolled (n = 48) | Recommended Intakes a | |||
| S1 | S3 | S1 | S3 | S1 | S3 | ||
| Fruit/vegetable score | 9.64 (7.52) | 10.18 (7.24) | 10.21 (6.52) | 8.90 (4.74) | 10.65 (5.51) | 12.19 (6.93) | NA |
| Fruit/vegetable/bean score | 13.52 (10.36) | 15.18 (10.05) | 14.53 (8.15) | 13.37 (6.73) | 15.27 (7.54) | 17.46 (10.02) | NA |
| Meat/snack score | 24.76 (13.64) | 24.61 (9.91) | 22.79 (12.56) | 20.79 (11.33) | 24.40 (8.81) | 25.60 (9.52) | NA |
| Fruit and vegetable intake | |||||||
| Fruit and Vegetable servings (per day) | 3.34 (2.77) | 3.54 (2.68) | 3.56 (2.39) | 3.06 (1.75) | 3.71 (2.04) | 4.29 (2.55) | |
| Micronutrient intake | |||||||
| Vitamin C (mg) | 132.68 (68.43) | 143.45 (67.26) | 137.12 (54.96) | 129.36 (44.88) | 145.18 (49.85) | 159.36 (66.62) | 90.0 |
| Magnesium (mg) | 379.58 (121.17) | 398.04 (120.78) | 382.88 (100.26) | 369.01 (81.40) | 403.38 (88.55) | 427.80 (118.70) | 420.0 |
| Potassium (mg) | 3500.18 (1195.21) | 3684.40 (1185.90) | 3547.87 (978.58) | 3411.32 (795.34) | 3729.64 (872.31) | 3973.00 (1168.72) | 3400.0 |
| Dietary fiber (g) | 18.38 (8.13) | 19.58 (8.19) | 18.36 (6.90) | 17.43 (5.61) f | 20.05 (5.96) | 21.65 (7.99) | 38.0 |
| Fat intake | |||||||
| Total fat (g) | 92.12 (32.73) | 91.76 (23.77) | 87.40 (30.14) | 82.60 (27.18) | 91.25 (21.14) | 94.15 (22.85) | NA b |
| Fat % | 34.66 (8.18) | 34.56 (5.94) | 33.47 (7.54) | 32.27 (6.80) | 34.44 (5.29) | 35.16 (5.71) | 20–35% |
| Saturated fat (g) | 31.19 (12.00) | 31.05 (8.72) | 29.45 (11.05) | 27.69 (9.97) | 30.87 (7.75) | 31.93 (8.38) | NA c |
| Dietary cholesterol (g) | 336.40 (114.44) | 335.22 (84.35) | 332.43 (97.15) | 316.83 (87.26) | 332.40 (74.27) | 341.83 (82.07) | NA d |
| Characteristic | Analytic Sample (n = 385 a) | Analytic Sample (n = 385) | Enrolled into the Program (n = 251) | ||||
|---|---|---|---|---|---|---|---|
| Never Enrolled in the Program (n = 134) | Enrolled into the Program (n = 251) | Comparison Never Enrolled vs. Enrolled b | No/Low Attendees (n = 172) | High Attendees (n = 79) | Comparison No/Low vs. High Attendees b | ||
| Food insecurity at S1 (baseline) | |||||||
| Food secure | 150 (39.0%) | 60 (44.8%) | 90 (35.9%) | 63(36.6%) | 27 (34.2%) | ||
| Food insecure | 235 (61.0%) | 74 (55.2%) | 161 (64.1%) | z = −1.710 | 109 (63.4%) | 52 (65.8%) | z = −0.376 |
| Low food security | 117 (30.4%) | 41 (30.6%) | 76 (30.3%) | z = −0.065 | 54 (31.4%) | 22 (27.9%) | z = 0.568 |
| Very low food security | 118 (30.7%) | 33 (24.6%) | 85 (33.9%) | z = −1.873 | 55 (32.0%) | 30 (38.0%) | z = −0.933 |
| Food insecurity at S3 (final time point) | |||||||
| Food secure | 159 (41.3%) | 74 (55.2%) | 85 (33.9%) | 60 (34.9%) | 25 (31.7%) | ||
| Food insecure | 226 (58.7%) | 60 (44.8%) | 166 (66.1%) | z = −4.055 *** | 112 (65.1%) | 54 (68.4%) | z = −0.503 |
| Low food security | 89 (23.2%) | 25 (18.7%) c | 64 (25.5%) | z = −1.517 | 43 (25.0%) | 21 (26.6%) | z = −0.267 |
| Very low food security | 137 (35.6%) | 35 (26.1%) | 102 (40.6%) | z = −2.834 *** | 69 (40.1%) | 33 (41.8%) | z = −0.248 |
| Barriers | Facilitators |
|---|---|
“Yeah, I had medical issues. I had a couple surgeries. And I had to get a co-worker of mine to go up there with me. Because the check-in process was really long and I wasn’t supposed to be up just period. So just standing there in line waiting.” “I think they had more options in the beginning. Then as time progressed, the options changed, too.” “I think that’s slow, not—I mean I get it like once you check-in it’s find. But I shouldn’t have to check out I believe. I think that kind of slowed things down a little bit because you’re checking in, you go through the line, you get the end, you got to go through the same process.” “And because it was such slim pickings they were sending you through the line three and four times trying to get you to meet that quota on that weight amount.” |
“But in most cases, we brought our own bags to carry, a cart, or whatever to carry it, but they also had carts that you could put _____ _____ in and take it to your car, and unload it in your car and bring the cart back. So, that was helpful, too, yeah.” “Really, it was really convenient, because when you would get there, they would give you the option of having a bag that they had already packed with each food group. Or you can go through and get what you wanted off the tables from, you know, each food group.’ “Yeah, because there weren’t too many sweets. Like I didn’t see that as far as giving us cakes. So if you don’t have it, you’re not going to consume it, right? So yeah, I didn’t see cakes and stuff. Unhealthy.” “The selections were, the specials were I think good and excellent because we had a choice of everything on the pyramid, of meat, vegetables, different things.” “They treated us equally, they made us feel like we were welcome there, and that’s the biggest thing of it, when somebody’s doing something like this, you know, you want them to feel, like, accepted.” |
“I sometimes—most of the time, either I had class, I couldn’t leave class and go. And so, this lady that was picking it up for me and taking it home for me, she couldn’t do it no more, so that really knocked me out of the box, ‘cause she couldn’t do it no more. And when I wasn’t in class, that wasn’t the day they’d get it. The day that they’d bring it over there to the Newton, it was my class, I had class.” “And then I found out that it was over here at Newton. Highland didn’t have it, Pin Oak didn’t have it, Saddle Brook didn’t have it. So I had no other option but—and like I said because I work in the Hacienda it was kind of convenient when I was at work. But coming from home, I’m passing up two other campuses to get there.” “My location for sure. Only because I live in Wilcox and at the time, I didn’t have a car, which is why online classes was really easy for me but that would have been my only obstacle, actually getting to the food bank.” “Well, first of all, I work part time and I go to school part time, so the timing affects me, because I also ride Metro. I’m a seizure patient, so I don’t try to drive. My seizures are basically controlled, but I do have problems with stress, and pressure, and have seizures occasionally, so I ride Metro. So basically, my biggest I guess you can say problem would be timing.” “Transportation, yeah, _____ _____ challenge, ‘cause it’s kind of difficult, by the time you get home, the meat is thawed out and, you know, so you got to cook it ‘cause it’s already thawed out. So now you got to _____ _____ _____ cook it, you can’t put it back in the fridge, and…” “Yeah, they missed it, because I live in Katy; if I didn’t have a car, there’s no bus that comes in, where I live in Kollen, to over here. So, yeah, there’s a lot of people that may have classes here, but they live over here and there’s no public transportation to get you from Point A to Point B. And everybody can’t afford Uber or Lyft or going to pay somebody to take them somewhere, you know? They only have maybe the resources to get them to that specific class at that location at that time, yeah, so.” |
“I lived so close to campus, and I also had, like, housemates that, you know, one of my housemates was willing to go and stand in and pick up for me.” “And it was me and my daughter and my daughter would go for me because during that time I had surgery. Yeah, and I wasn’t supposed to be out.” “And so if you weren’t able to go, you could send someone to go for you, and I think it was usually two different locations” “Usually the challenges that I had was regarding time and I would just send my son in my place to go and get it. So when they were having it either I was at work or I was in class, so I would just let him go. If I didn’t have him, then it probably would have been more of a challenge, but he was able to compensate for where I couldn’t go.” “And also one thing other, they had a part of it if you weren’t able to make it you could send someone. So that was really good” |
“Because people were being greedy, getting too much. Then that became a problem.” “I can’t really say. No, it was a good variety of everything that time that I went. At the beginning, I was kind of in the middle of the line, so I noticed that a lot of people were trying to—I think the limit was 50 pounds or something, so a lot of people were just trying to get meat and that was not leaving a good selection for the people that were behind them if you only grabbed meat and nothing else.” “It came at a time where I really needed it and I don’t have anything negative to say about the program. It’s just some of the people, I think, were discourteous and they went in with an attitude like, “Hey, I’m going in with me and my daughter. I’m going to bring my daughter with me and me and my daughter’s going to get this.” And I’ve seen some people get eight, nine, ten packs of meat, and I was, wait. This is crazy.” “People on your back, people reaching over your shoulder, or you’re trying to get your products, and they see something they want, so they just go around you and grab it. That was my only kickback about it, and I’m the type of person, I’m going to let you go ahead and get what you want.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez, D.C.; Daundasekara, S.S.; Walton, Q.L.; Eigege, C.Y.; Marshall, A.N. Feasibility of Delivering an on-Campus Food Distribution Program in a Community College Setting: A Mixed Methods Sequential Explanatory Investigation. Int. J. Environ. Res. Public Health 2021, 18, 12106. https://doi.org/10.3390/ijerph182212106
Hernandez DC, Daundasekara SS, Walton QL, Eigege CY, Marshall AN. Feasibility of Delivering an on-Campus Food Distribution Program in a Community College Setting: A Mixed Methods Sequential Explanatory Investigation. International Journal of Environmental Research and Public Health. 2021; 18(22):12106. https://doi.org/10.3390/ijerph182212106
Chicago/Turabian StyleHernandez, Daphne C., Sajeevika S. Daundasekara, Quenette L. Walton, Chinyere Y. Eigege, and Allison N. Marshall. 2021. "Feasibility of Delivering an on-Campus Food Distribution Program in a Community College Setting: A Mixed Methods Sequential Explanatory Investigation" International Journal of Environmental Research and Public Health 18, no. 22: 12106. https://doi.org/10.3390/ijerph182212106
APA StyleHernandez, D. C., Daundasekara, S. S., Walton, Q. L., Eigege, C. Y., & Marshall, A. N. (2021). Feasibility of Delivering an on-Campus Food Distribution Program in a Community College Setting: A Mixed Methods Sequential Explanatory Investigation. International Journal of Environmental Research and Public Health, 18(22), 12106. https://doi.org/10.3390/ijerph182212106