1. Introduction
The coronavirus pandemic has had a huge impact on healthcare systems worldwide. The healthcare system has not only been burdened by the increase in the number of infections with the coronavirus-19 (COVID-19) but also had to continue to provide emergency and urgent care for non-COVID-19 patients [
1,
2]. Thus, the healthcare system has faced an enormous challenge. This particularly affects neurosurgery, as many diseases in this field have an emergency character. Neurosurgical diseases are characterized by enormous heterogeneity, complexity, rapid tendency to undergo neurological deterioration and urgent care character [
3]. A large number of neurosurgical operations have still been required during the pandemic [
4].
There has been an increased demand for ventilators and intensive care resources during the pandemic. These resources were taken away from non-COVID-19 patients. Thus, triaging and prioritization of patients in the non-COVID-19 area and deferral of elective procedures was required [
5].
An uncertainty resulted, therefore, regarding the impending undertreatment of non-COVID-19 cases in favor of the redistribution of COVID-19 patients under focus [
6]. Consequently, universal recommendations have been necessary. Numerous guidelines and recommendations for prioritizing, shifting, and structurally utilizing tightening resources during the pandemic were published [
7,
8,
9].
Accordingly, we looked at the period of the second wave of the pandemic in Saxony, Germany, compared to the pre-pandemic time regarding surgical procedures, complications, and readmissions in our neurosurgical department at a university hospital.
Unplanned readmissions consume potentially preventable resources, incur costs, and compromise patient satisfaction. Therefore, investigating the causes and predictors of unplanned readmissions is essential to achieve quality improvement. Unplanned readmissions represent a marker of quality, [
10,
11,
12] and also allow the estimation of patient care during the COVID-19 pandemic. To the best of our knowledge, we are the first to investigate the impact of the COVID-19 pandemic on the quality of neurosurgical care measured by surgical procedures, complications, and unplanned readmissions.
2. Materials and Methods
The internal review board of the Medical Faculty of the University Hospital Leipzig agreed to the retrospective data analysis (167/18-ek). All neurosurgical patients who underwent neurosurgical surgery during the period of the second wave of the COVID-19 pandemic in Saxony, Germany, from 1 October 2020 to 15 March 2021 (pandemic group) were included in this retrospective monocentric study. This patient group was compared to a comparison group of neurosurgical patients who had surgery from the period 1 October 2019 to 15 March 2020 (pre-pandemic group). Patient informed consent was not required according to the approval of the ethics committee. Patient criteria, hospital- and surgery-related factors, perioperative complications, and unplanned readmissions 30 days after discharge were analyzed. If multiple surgeries were performed, the index surgery, the main surgery in that inpatient stay, was listed. The first set of ‘index admission’ diagnoses contained all neurosurgical diseases according to the ICD-10 GM list. The patients were grouped into ‘neoplasm,’ ‘hydrocephalus,’ ‘traumatic head injury,’ ‘vascular,’ ‘functional disorder,’ ‘degenerative spine disease,’ and ‘others’ (e.g., abscess, trigeminus neuralgia). The patient clinical complexity level (PCCL) was defined via the effective assessment ratio of the German diagnosis-related groups’ coding level, which integrates the technical procedures and the patient’s secondary diagnoses. Causes for readmission were noted as: (1) surgical complications, (2) medical complications, (3) diagnosis-related complications (e.g., progression of tumor, hydrocephalus), (4) neurological decompensation (e.g., stroke, seizure, neurologic symptoms), (5) pain management, and (6) others (e.g., unrelated diagnoses, admissions due to missing home care). Categories of readmission were defined as: (1) preventable reasons (e.g., surgical site infection (SSI), cerebrospinal fluid (CSF) leak, postoperative hemorrhage, nosocomial infection, postoperative pain, falls), (2) reasons related to the natural progression of the disease (e.g., occlusive hydrocephalus, seizures), (3) reasons despite best practice (e.g., stroke), and (4) unrelated reasons according to the study by Shah et al. [
3].
Statistical analysis was performed with IBM SPSS Statistics 25.0 software (IBM, Armonk, New York, NY, USA). The associations between continuous variables were examined using the t-test for normal distribution and the Mann–Whitney U test for variables without normal distribution. Categorical variables were compared by employing the Fisher exact test. Continuous variables were described using mean and median values, while categorical variables were described with counts and frequencies. A two-tailed p value < 0.05 was considered to be statistically significant.
3. Results
3.1. Surgical Procedures
A total of 535 patients were included in the COVID-19 pandemic group, and a total of 602 operations were performed. By contrast, 602 patients were treated in the non-pandemic group, and a total of 717 operations were performed. Thus, there was a decrease of 67 patients (reduction to 88.87%), and a total of 115 fewer surgeries (reduction to 83.96%) were conducted in the COVID-19 pandemic group. In addition, the operating room capacity had been reduced to 88% due to higher intensive care unit resources necessary to take care of critically ill COVID-19 patients during the pandemic. Analysis stated that the two groups, pandemic and pre-pandemic, did not differ in the patient characteristics (see
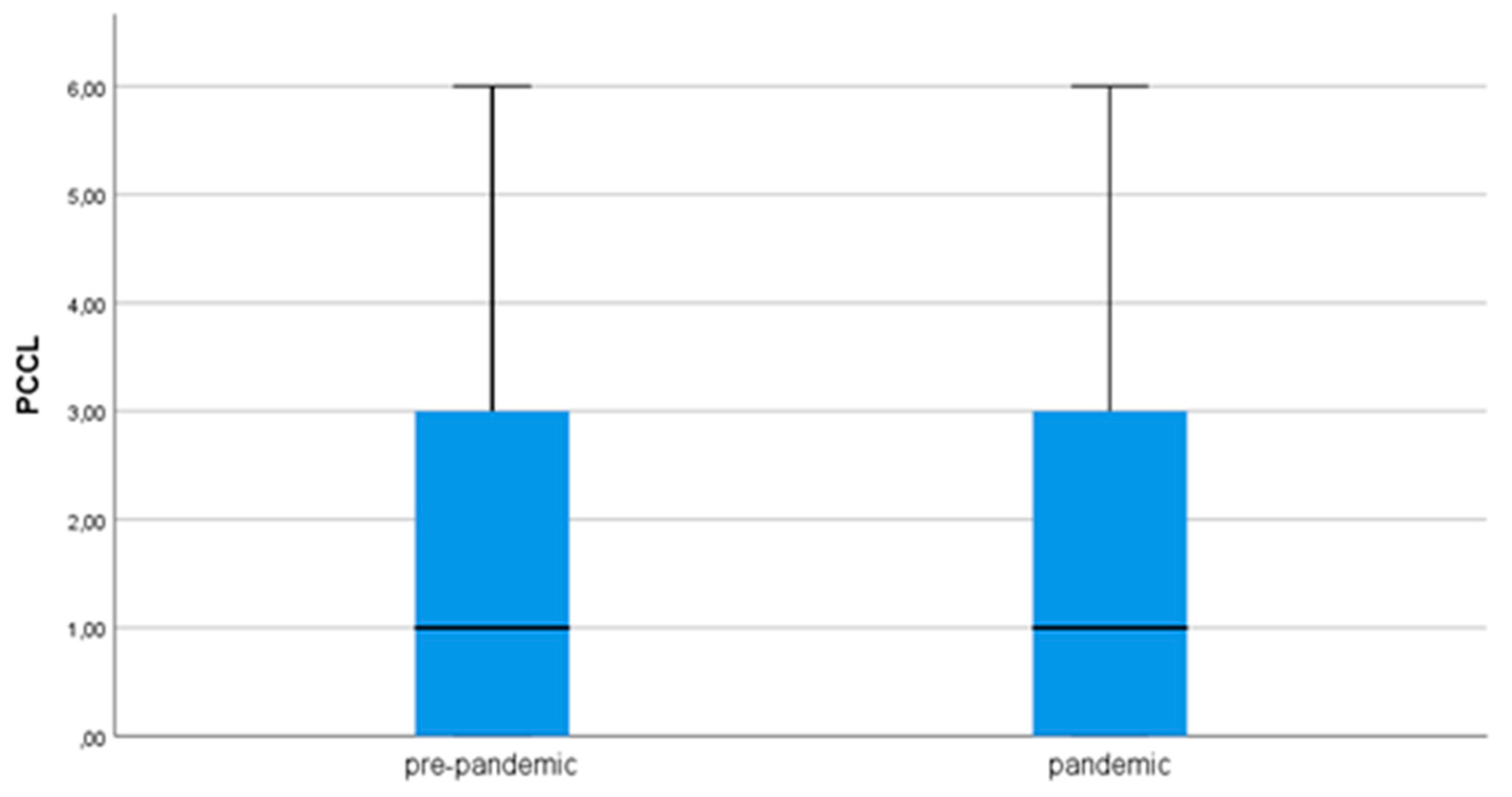
Table 1). The patient groups were similar in terms of age, gender, and index diagnosis groups. When we analyzed the admission modalities, we observed identical frequencies of elective and emergency admissions in the pandemic and the pre-pandemic period. Discharge modalities were also identical in both groups. When the operation-dependent factors were examined, a homogeneity was found between the two study groups. The number of operations, the length of surgery, and the timing were identical. The PCCL was identical during the pandemic and pre-pandemic, and the duration of ventilation did not change during the pandemic compared to the pre-pandemic (
Figure 1). With regard to the index diagnosis groups, a categorization of the neurosurgical diseases according to the ICD-10 GM list was performed. Fewer intracranial neurinomas, cervical spinal stenoses, and peripheral nerve injuries were treated surgically during the pandemic. By contrast, no diagnostic group was represented more frequently in the coronavirus group (see
Table 2).
3.2. Complications
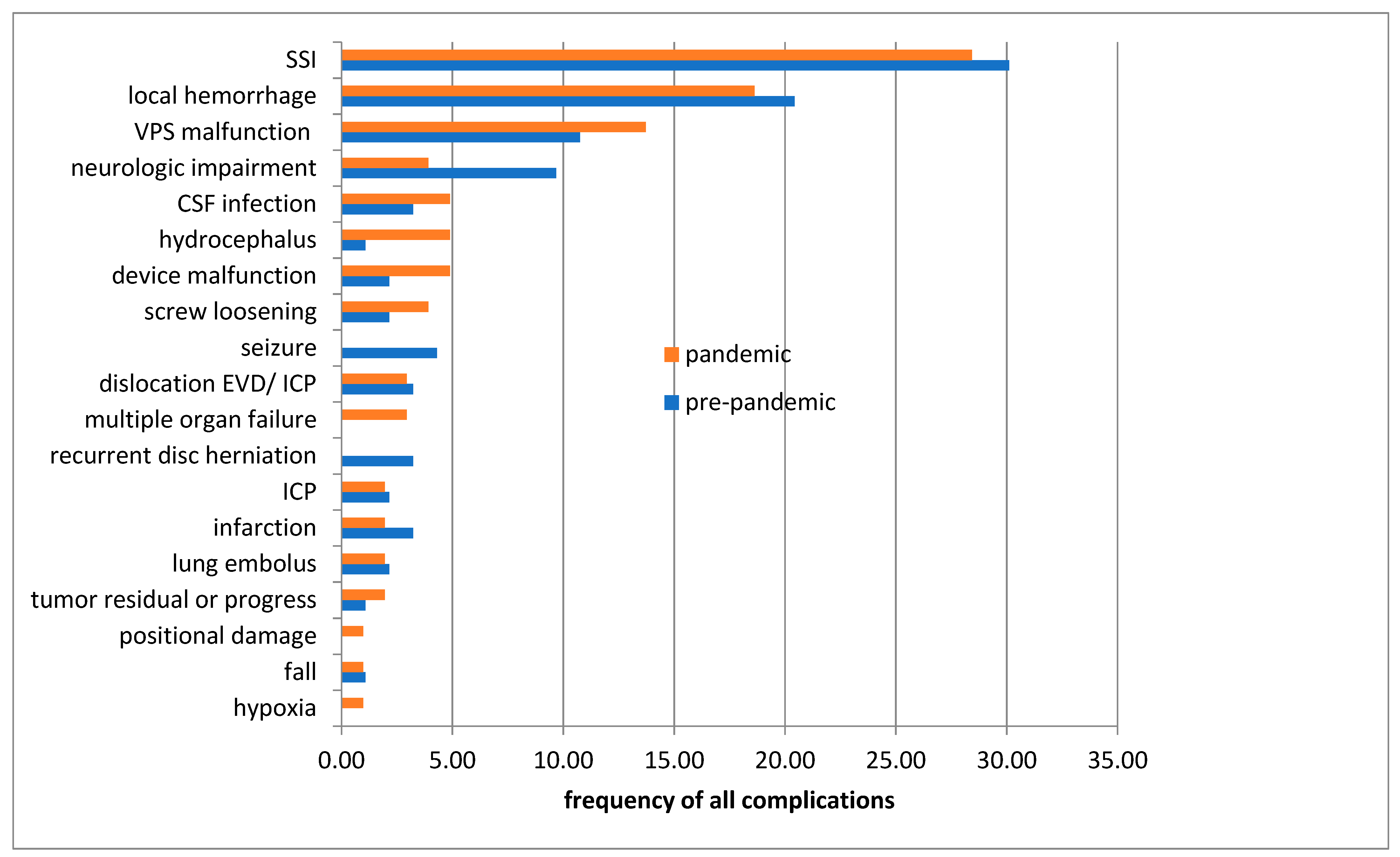
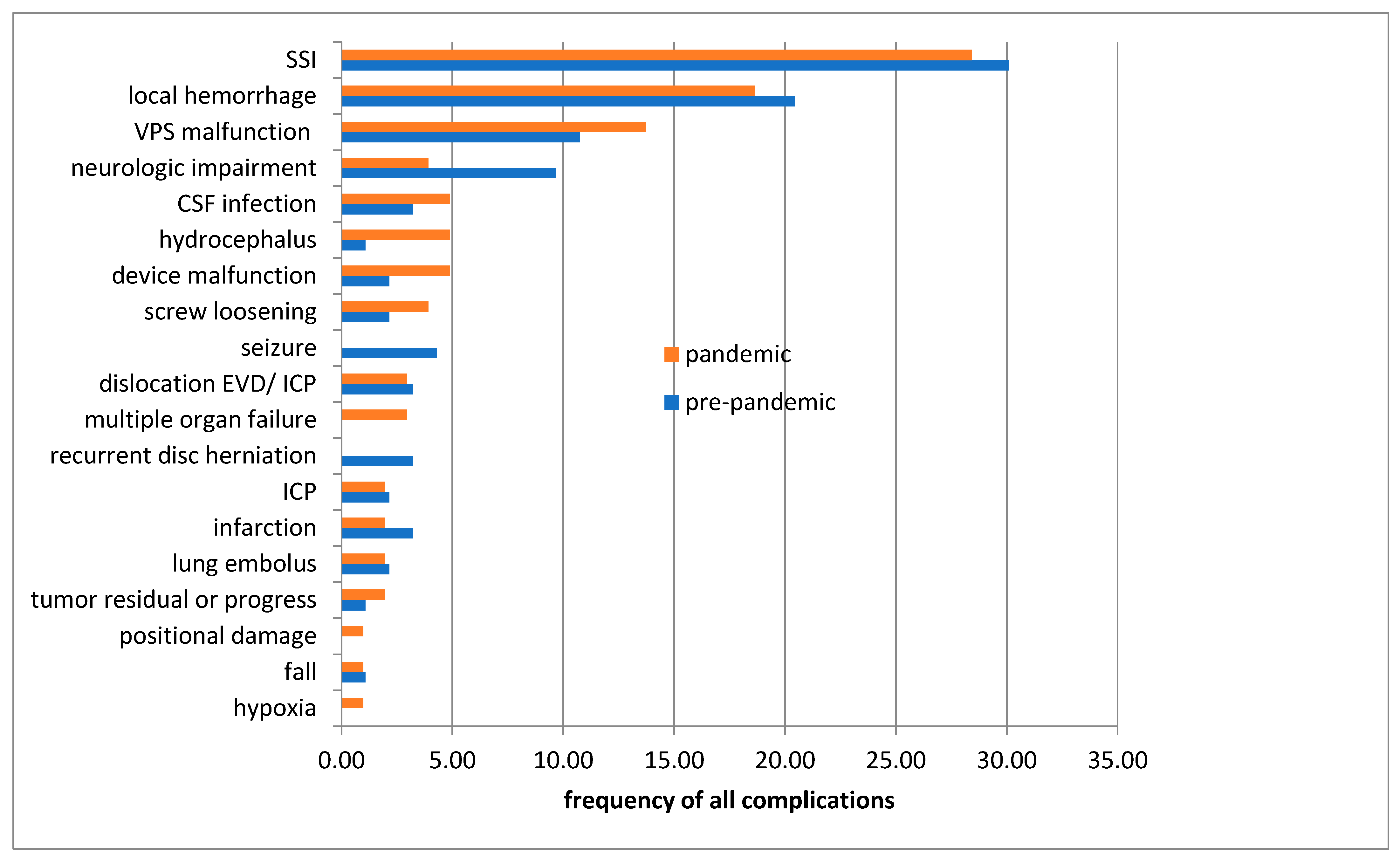
In the next step, we looked at the perioperative complications.
Figure 2 presents the different complications. There is a homogeneity of the two groups with no significant difference. The most frequent complications registered in both groups are SSIs followed by local postoperative bleeding.
3.3. Readmissions
Finally, we examined the unplanned readmissions in both groups. The unplanned readmission rate was 5.05% (27 cases) during the pandemic, while the pre-pandemic readmission rate was 5.81% (35 cases). The detailed reasons for readmissions were without statistical difference for both groups (see
Supplementary Table S1). A closer look at the detailed reasons for readmission indicated that SSIs were responsible for most of the unplanned readmissions. There is no significant difference (
p-value = 0.390), but there is a trend towards a reduction in the pandemic group (10 cases pre-pandemic vs. 5 cases pandemic). A significant difference between the reasons for readmission was not found. Further factors regarding the unplanned readmission group with patient-related and treatment-dependent factors are shown in
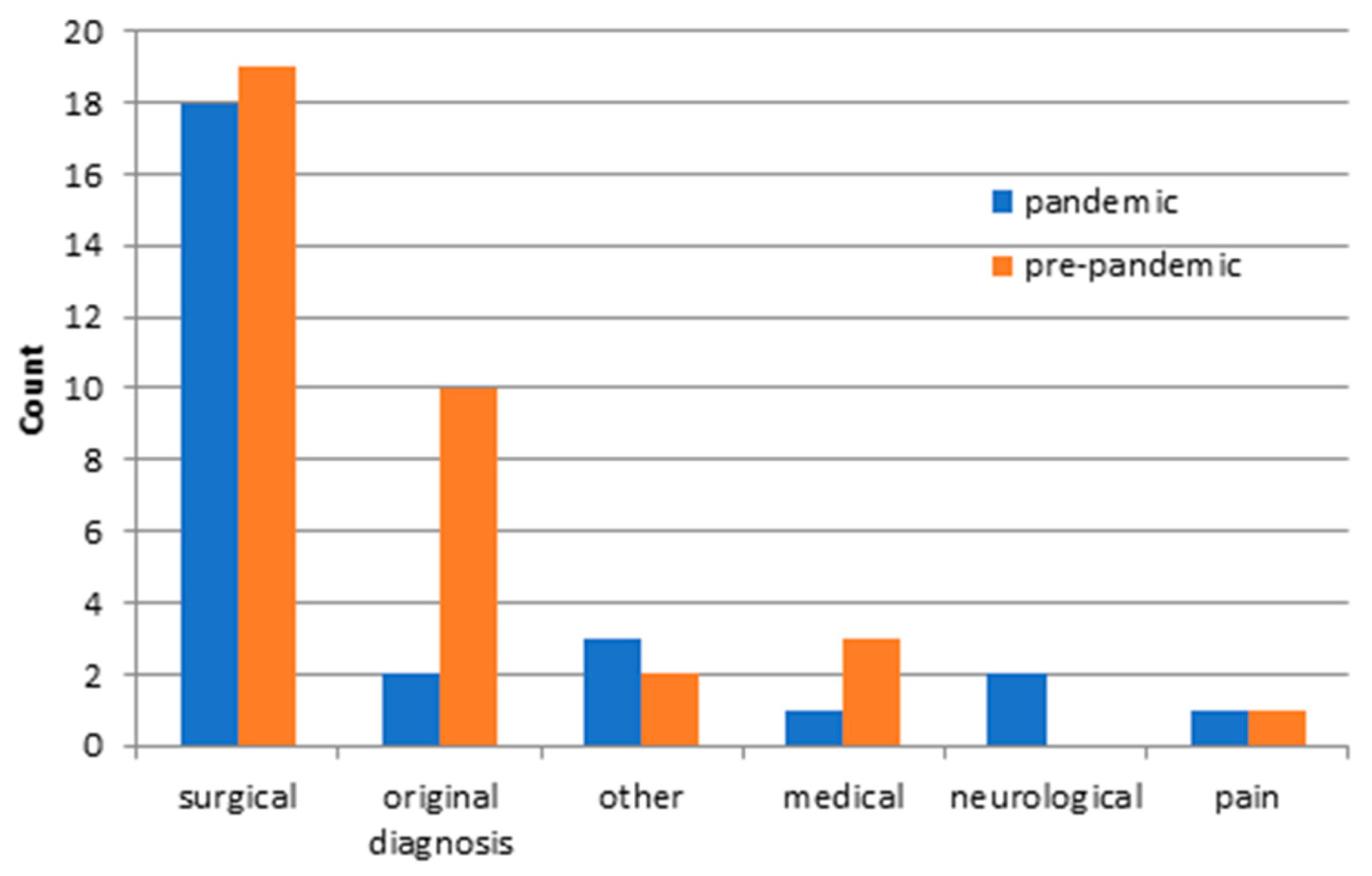
Table 3. There were no significant differences for either study group. Furthermore, there were similar frequencies for the pandemic and the pre-pandemic group regarding the causes for readmissions (
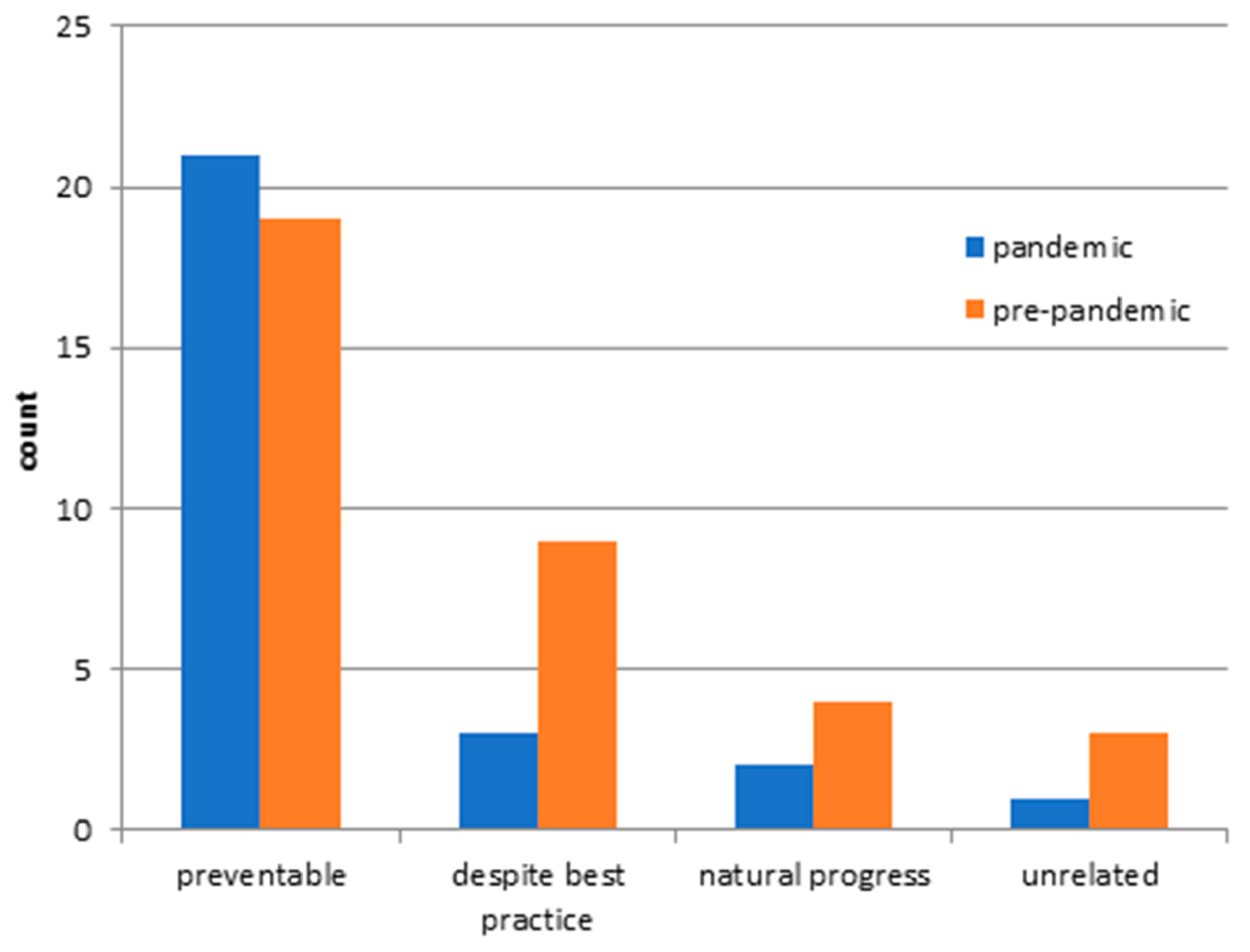
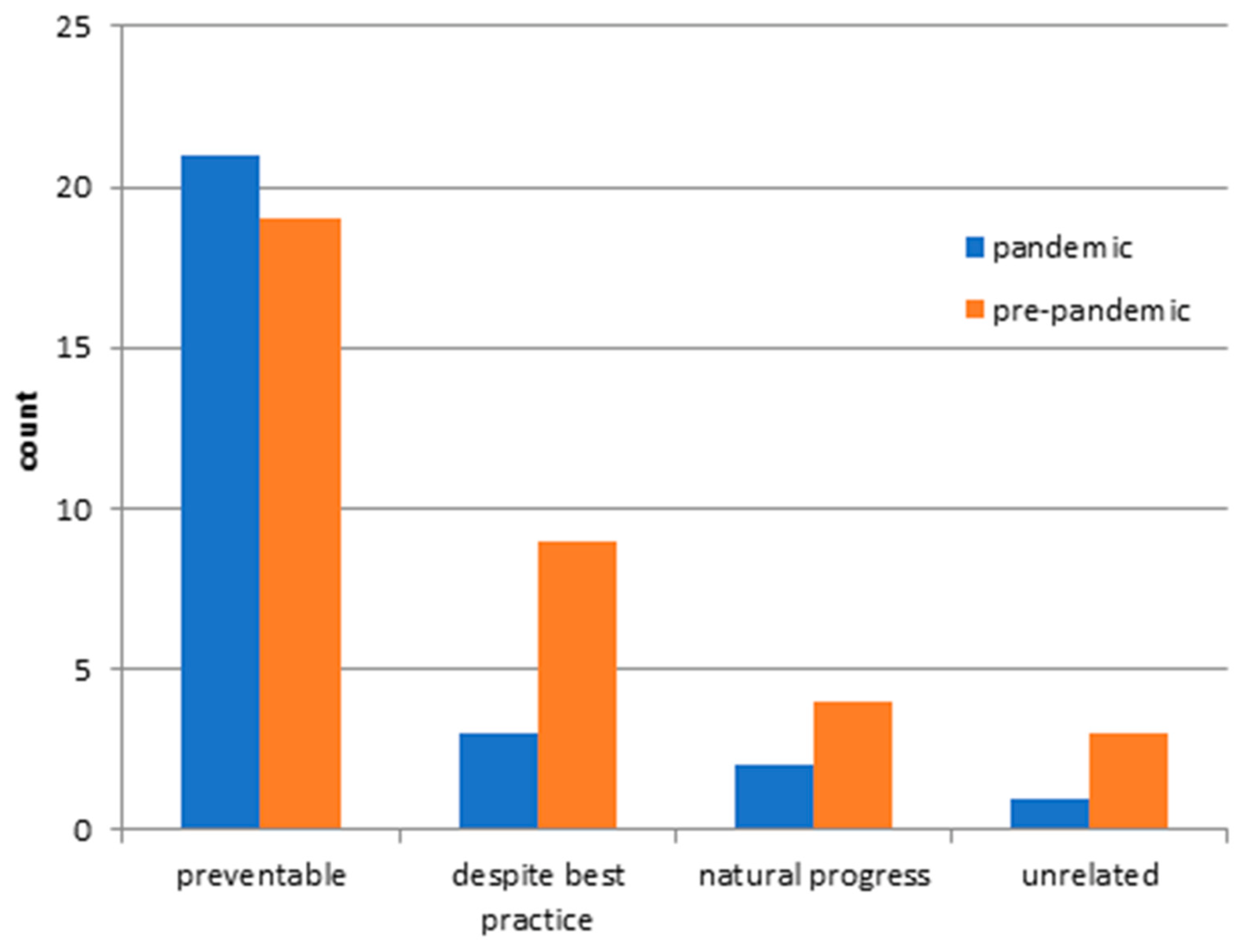
Figure 3). The surgical causes predominated in both groups. A progress of the underlying disease was responsible for the majority of pre-pandemic unplanned readmissions, whereas new medical complications caused the majority of unplanned readmissions in the pandemic group. In the following, the readmissions were divided into categories (
Figure 4). There was no significant difference in readmission categories for either study group. Most unplanned readmissions were for the pandemic and pre-pandemic study group classified as ‘preventable,’ followed by ‘despite best practice’.
4. Discussion
Our study demonstrated the differences and similarities of patients treated neurosurgically during the COVID-19 pandemic compared to pre-pandemic in a retrospective, monocentric study.
4.1. Surgical Procedures
Many similarities were found between the study groups in terms of patient characteristics and treatment-related factors. For instances, we revealed a statistically similar distribution in terms of age, sex, and index diagnosis groups of patients during the COVID-19 pandemic compared with the pre-pandemic period. However, there were also significant differences between the study groups. Significantly fewer intracranial neurinomas, peripheral nerve lesions, and cervical spinal stenosis were surgically treated and hospitalized during the pandemic. These three admission diagnoses are among the highly elective and postponable procedures. In a comprehensive survey of neurosurgical centers in Europe during the early part of the COVID-19 pandemic in March 2020, decreases in elective craniotomies and intermediate and regular neurosurgical beds were reported in the majority of centers. The decrease in elective procedures was necessary to ensure medical care for the increasing number of COVID-19 patients. Resources in the hospital such as intensive care beds and medical staff are limited. Therefore, the need for prioritization and triage of procedures and emergencies has emerged to adequately care for both COVID-19 patients and neurosurgical cases [
4]. For example, a recent study found a 40% decrease in neurosurgical operations, clinical visits, and inpatient consultations, and a significant decrease in spine and endovascular procedures during the pandemic compared with the pre-pandemic [
13]. Interestingly, there were also few European centers that reported no decreases in the quantity and quality of medical care of neurosurgical procedures, elective as well as emergency cases due to the pandemic [
4]. Another study of neurosurgical patients during the COVID-19 pandemic in Germany found a slight decrease in patients and (1278 cases pandemic versus 1379 pre-pandemic) and surgical procedures [
14].
Triaging of highly elective procedures is possible for patients who are not at risk of neurologic deficit due to the waiting time of postponed surgeries. In some cases, a stabilization and decrease of the initial symptoms during the waiting period was described for this patient collective. This brings the conservative therapy of these diseases back into the foreground [
15,
16]. In addition, the avoidance of patients with a low symptom burden before hospitalization or the initial favoring of conservative therapy could also explain the decrease in elective admissions causally. Differential prioritization and rationing in neurosurgical centers across Europe were demonstrated [
4]. Some centers were able to provide emergency care, depending on the region, whereas others also described an uninterrupted elective program. Here, the enormous difference in the volume of neurosurgical procedures performed was attributed to the varying severity of the COVID-19 burden and the resources available. Some centers had less bed capacity and a longer waiting list even in pre-pandemic times, which was exacerbated by the COVID-19 pandemic [
4]. The most pandemic constraints were reported in neurosurgical centers, where regions were particularly severely affected by the COVID-19 pandemic, had large catchment areas and low resources. In addition, the number of beds and longer waiting lists for neurosurgical procedures were already present in these centers before the pandemic. As a result, there was little flexibility in adjusting COVID-19 measures related to triage, rationing, and prioritization, leading to a high degree of change in indications and services [
4].
4.2. Emergency Admission
Some neurosurgical departments responded quickly and effectively to the redistribution of resources during the pandemic. In addition to reducing the surgical capacity, a change in indications, namely task shifting, is also an efficient way to adapt resources during the pandemic [
4]. There is a division of responsibilities among the centers, with different responsibilities for emergency surgeries, elective surgeries, and, of course, the care of COVID-19 patients regarding task shifting [
17]. Consequently, the catchment area of the neurosurgical departments changes during the pandemic and, therefore, the potential number of patients to treat. Interestingly, we could not register any changes in emergency cases, mortality, or night-shift surgery during the pandemic compared to the pre-pandemic time course. Despite this, a decrease in emergency neurosurgical cases, such as traumatic brain injuries, spine conditions, or chronic subdural hematomas, was noticed [
18]. However, no decrease in neurosurgical emergencies or night procedures was evident in our study. We cared for statistically equal numbers of emergencies, elective procedures, and night shift procedures before and during the pandemic. These variations in the different neurosurgical centers can be explained by differences in coronavirus burden within regions, differences in resources and bed distribution, and, of course, catchment area [
4]. Thus, an absolute reduction in neurosurgical emergencies per population can still be masked by an expanded catchment area, as was present in our neurosurgical center.
4.3. PCCL
Considering the severity of cases during the pandemic and pre-pandemic period, there was no difference. By contrast, an increase in PCCL during the pandemic was documented in the visceral surgery patient population at the University Hospital Leipzig, which was explained by the predominance of severely ill patients in the case mix [
19]. An increase in PCCL during the pandemic is attributable to the fact that primarily sicker patients with emergency indications were hospitalized. Treatments for healthier patients with elective indications were postponed or canceled according to prioritization and triage. Interestingly, no change in PCCL was evident in our study, which would have been expected from a shift in index diagnosis groups and triage. There are several possible explanations for this. First, we found no statistically significant change in the number of emergencies versus elective procedures for neurosurgical patients. Only for three index diagnosis groups, intracranial neurinomas, peripheral nerve lesions, and cervical spinal stenosis, a significant reduction of admissions during the pandemic compared to the pre-pandemic was evident. Moreover, it was striking that the neurosurgical patients already had a relatively high median PCCL. Therefore, the comparison of the different patient groups is per se difficult.
4.4. Complications
The type of complications and the complication rate of surgically treated patients did not change during the pandemic. The most common perioperative complications in both groups were SSIs and local hemorrhages. It should be emphasized, however, that a trend for less SSI among patients receiving neurosurgical care was evident during the pandemic, but this difference was not statistically significant. A recently published study in a large neurosurgical center in Germany described a drastic decrease in SSI after neurosurgical procedures due to the strict hygiene measures and limited visitors in the hospital [
14]. It should be underlined that in our study 29 cases (28.34% of all complications in the pandemic group) versus 28 cases (30.11% of all complications in the pre-pandemic group,
p-value 0.588) were identified. Therefore, a reliable conclusion or even confirmation of the above-cited study is not possible based on our data with the small number of cases.
4.5. Readmission
Finally, we examined the unplanned readmissions in the two study groups. No significant differences were found regarding the index diagnosis, the LOS, the occurrence of complications, or the PCCL of the index admission. Reasons, causes, and categories for readmission are also equally prevalent with predominantly surgical causes in both groups. We showed previously that readmission rates in neurosurgery ranged from 5.7 to 9.2%, depending on the index diagnosis [
19,
20]. We confirmed a similar readmission rate in this study population during the pandemic and pre-pandemic period. Furthermore, SSIs again emerged as the leading cause of readmissions. In the literature, SSIs were found repeatedly to be the most common reason for unplanned readmission [
1,
6,
18]. The majority of unplanned readmissions in neurosurgery belong to the group of preventable readmission categories. This fact has already been described by Sander et al. in cranial and spinal neurosurgical patients [
16,
17]. Interestingly, a lower incidence of SSIs during the COVID-19 pandemic period was striking as a preventable category of unplanned readmission. This correlation is not statistically significant and should, therefore, only be considered hypothetically. A significant decrease in SSIs during the pandemic was described in another neurosurgical collective. Intensified hygiene measures with an increased use of disinfectants in everyday life, the mandatory use of medical or FFP2 masks, and the stricter restriction of hospital visits may explain a tendency toward a decrease in the number of germs circulating [
4].
5. Conclusions
This study investigated the quality and quantity of medical care provided to neurosurgical patients during the COVID-19 pandemic. Ours was the first study to demonstrate only minor statistical differences among neurosurgical patients during the pandemic compared with pre-pandemic. Thus, in terms of patient characteristics such as age, sex, and PCCL, we showed that the study groups did not differ. In addition, most treatment-related factors such as type of admission and type of discharge, length of stay, certain index diagnoses, and surgical procedures were statistically the same. It is important to emphasize that there were no differences in perioperative complications, predominantly SSI and local hemorrhage, for both study groups. Furthermore, the COVID-19 pandemic did not affect the rate of unplanned readmissions (5.08% vs. 5.81%, pandemic vs. pre-pandemic), which is known to be a quality measure of medical care in health care services. Causes and reasons for readmission were statistically similar for both study groups. There are only minor statistical differences between the neurosurgical patients in the COVID-19 pandemic and pre-pandemic period. Some highly elective, postponable procedures, such as intracranial neurinomas, peripheral nerve lesions, and cervical spinal stenosis, were treated with fewer hospitalizations during the COVID-19 pandemic. The decrease in highly elective procedures can be explained by prioritization, rationing, and triage in favor of critically ill patients. Moreover, during the COVID-19 pandemic, a decrease in SSI as perioperative complications and as unplanned readmission cause in the corona was recorded. However, it should be emphasized that it was only apparent as a trend and did not become statistically significant.
The absence of massive limitations due to the COVID-19 pandemic in our neurosurgical center can be assumed due to a good resource distribution and structuring already existing before the pandemic with a simultaneous expansion of the catchment area.
In summary, we demonstrated that broad cross-diagnosis care of neurosurgery patients was provided at our hospital, even during the COVID-19 pandemic.
Author Contributions
Conceptualization, C.S. and F.A.; methodology, C.S., J.M., S.S. and D.W.; software, M.K.F. and T.W.; validation, F.A., J.M., S.S., N.v.D. and D.W.; writing—original draft preparation, C.S. and F.A.; writing—review and editing, F.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of university of Leipzig, medicine faculty (167/18-ek).
Informed Consent Statement
Not applicable for this study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
CNS: central nervous system; COVID-19: Corona-virus-19; CSF: cerebrospinal fluid; EDH: epidural hematoma; ICD-10-GM: Classification of Diseases and Related Health Problems, 10th Revision, German Modification; ICP: intracranial pressure; LOS: length of stay; NPH: normal pressure hydrocephalus; No.: number; PCCL: patient clinical complexity level; SSI: surgical site infection; SDH: subdural hematoma; SAH: subarachnoidal hemorrhage; TBI: traumatic brain injury.
References
- Dobran, M.; Paracino, R.; Iacoangeli, M. Neurosurgery during the COVID-19 pandemic: Update from Lombardy, northern Italy. Acta Neurochir. 2020, 162, 1223–1224. [Google Scholar]
- Galarza, M.; Gazzeri, R. Letter: Collateral Pandemic in Face of the Present COVID-19 Pandemic: A Neurosurgical Perspective. Neurosurgery 2020, 87, E186–E188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, M.N.; Stoev, I.T.; Sanford, D.E.; Gao, F.; Santiago, P.; Jaques, D.P.; Dacey, R.G. Are readmission rates on a neurosurgical service indi-cators of quality of care? J. Neurosurg. 2013, 119, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Mathiesen, T.; Arraez, M.; Asser, T.; Balak, N.; Barazi, S.; Bernucci, C.; Bolger, C.; Broekman, M.L.D.; Demetriades, A.K.; Feldman, Z.; et al. A snapshot of European neurosurgery December 2019 vs. March 2020: Just before and during the COVID-19 pandemic. Acta Neurochir. 2020, 162, 2221–2233. [Google Scholar] [CrossRef] [PubMed]
- Jean, W.C.; Ironside, N.T.; Sack, K.D.; Felbaum, D.R.; Syed, H.R. The impact of COVID-19 on neurosurgeons and the strategy for triaging non-emergent operations: A global neurosurgery study. Acta Neurochir. 2020, 162, 1229–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tartara, F.; Cofano, F.; Zenga, F.; Boeris, D.; Garbossa, D.; Cenzato, M. Are we forgetting non-COVID-19-related diseases during lockdown? Acta Neurochir. 2020, 162, 1501. [Google Scholar] [CrossRef] [PubMed]
- Castelnuovo, P.; Turri-Zanoni, M.; Karligkiotis, A.; Battaglia, P.; Pozzi, F.; Locatelli, D.; Bernucci, C.; Iacoangeli, M.; Krengli, M.; Marchetti, M.; et al. Skull-base surgery during the COVID-19 pandemic: The Italian Skull Base Society recommendations. Int. Forum Allergy Rhinol. 2020, 10, 963–967. [Google Scholar] [CrossRef] [PubMed]
- Gandía-González, M.L.; Sáez-Alegre, M.; Roda, J.M. Neurosurgeons on the frontline of COVID-19: No place for surgery? Acta Neurochir. 2020, 162, 1503–1504. [Google Scholar] [CrossRef] [PubMed]
- Sander, C.; Oppermann, H.; Nestler, U.; Sander, K.; von Dercks, N.; Meixensberger, J. Early unplanned readmission of neurosur-gical patients after treatment of intracranial lesions: A comparison between surgical and non-surgical intervention group. Acta Neurochir. 2020, 162, 2647–2658. [Google Scholar] [CrossRef] [PubMed]
- Bernatz, J.T.; Anderson, P.A. Thirty-day readmission rates in spine surgery: Systematic review and meta-analysis. Neurosurg. Focus 2015, 39, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, H.; Carico, C.; Nuño, M.; Mukherjee, D.; Ortega, A.; Black, K.L.; Patil, C.G. Unplanned readmissions and survival following brain tumor surgery. J. Neurosurg. 2015, 122, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Schipmann, S.; Varghese, J.; Brix, T.; Schwake, M.; Keurhorst, D.; Lohmann, S.; Molina, E.S.; Mauer, U.M.; Dugas, M.; Warneke, N.; et al. Establishing risk-adjusted quality indicators in surgery using administrative data—an example from neurosurgery. Acta Neurochir. 2019, 161, 1057–1065. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.D.; Kelly, K.A.; Reynolds, R.A.; Turer, R.W.; Salwi, S.; Rosenbloom, S.T.; Bonfield, C.M.; Naftel, R.P. Tracking the volume of neurosurgical care during the coronavirus sisease 2019 pandemic. World Neurosurg. 2020, 142, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Chacón-Quesada, T.; Rohde, V.; von der Brelie, C. Less surgical site infections in neurosurgery during COVID-19 times—one potential benefit of the pandemic? Neurosurg. Rev. 2021, 5, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Black, P.M. Benign brain tumors. Meningiomas, pituitary tumors, and acoustic neuromas. Neurol. Clin. 1995, 13, 927–952. [Google Scholar] [CrossRef]
- Hug, A.; Hähnel, S.; Weidner, N. Diagnostik und konservative Therapie zervikaler und lumbaler Spinalkanalstenosen. Der Nervenarzt 2018, 89, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Robertson, F.C.; Esene, I.N.; Kolias, A.G.; Khan, T.; Rosseau, G.; Gormley, W.B.; Park, K.B.; Broekman, M.L.; Rosenfeld, J.; Balak, N.; et al. Global Perspectives on Task Shifting and Task Sharing in Neurosurgery. World Neurosurg. X 2020, 6, 100060. [Google Scholar] [CrossRef] [PubMed]
- Grassner, L.; Petr, O.; Warner, F.M.; Dedeciusova, M.; Mathis, A.M.; Pinggera, D.; Gsellmann, S.; Meiners, L.C.; Freigang, S.; Mokry, M.; et al. Trends and outcomes for non-elective neu-rosurgical procedures in Central Europe during the COVID-19 pandemic. Sci. Rep. 2021, 11, 6171. [Google Scholar] [CrossRef] [PubMed]
- von Dercks, N.; Seehofer, D.; Steinert, M.; Krämer, S.; Branzan, D.; Dietrich, A.; Schürmann, O.; Gockel, I. Wie stark trifft die Corona-Pandemie die chi-rurgische Klinik eines universitären Maximalversorgers?: Eine Analyse der ersten 7 Wochen (How severe is the effect of the coronavirus pandemic on the department of surgery of a university hospital? An analysis of the first 7 weeks). Der Chir. Z. Fur Alle Geb. Der Oper. Medizen 2020, 91, 755–761. [Google Scholar]
- Sander, C.; Oppermann, H.; Nestler, U.; Sander, K.; von Dercks, N.; Meixensberger, J. Causes and predictors of unplanned read-mission in cranial neurosurgery. World Neurosurg. 2021, 149, 622–635. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}